
Abstract
Introduction
Patients with schizophrenia and other psychotic disorders represent a large portion of American state hospital populations, both currently and historically. Delusions are a common component of psychotic disorders. According to the Diagnostic and Statistical Manual-IV-TR (American Psychiatric Association, 2000), persecutory delusions are the most common. Indeed, analysis of delusion content across cultures reflects a prominence of delusions of persecution, including samples from Australia (Brakoulias and Starcevic, 2008), Austria (Gutiérrez-Lobos et al., 2001; Stompe et al., 1999; Tateyama et al., 1998), Germany (Tateyama et al., 1998), the UK (Renvoize and Beveridge, 1989), Japan (Tateyama et al., 1998), Pakistan (Ahmed, 1978; Stompe et al., 1999) and Spain (de Portugal et al., 2008).
Delusion type in schizophrenia has been associated with patient characteristics and response to treatment. In a study of 61 Polish patients diagnosed with schizophrenia-paranoid type (Debowska et al., 1998), patients with thought-broadcasting delusions had a lower acceptance of treatment and a lack of judgement and insight, as compared to patients with other types of delusions. In addition, patients in this study with delusions of grandeur and sexual delusions were also found to be more likely to have lower treatment acceptance rates. This lower acceptance of treatment may be caused by the patient’s denial of treatment efficacy based upon their feelings of importance and power (Debowska et al., 1998).
Type of delusion has also been related to its persistence. Repeat assessment of 1,136 American patients every 10 weeks across one year found patients with delusions of thought broadcasting or body/mind control to be more likely to have persistence of their delusions across time (Appelbaum et al., 2004). Greater intensity of belief in the delusion (e.g. preoccupation, impact on behaviour, pervasiveness) was also related to the likelihood of persistence (Appelbaum et al., 2004).
One of the earliest accounts of delusions in schizophrenia can be found in Gogol’s 1834 publication of Diary of a Madman (Altschuler, 2001). The main character, Poprishchin, has a grandiose delusion that he is the King of Spain. Although such psychosis may be associated with mania, the accompanying behavioural deterioration and disorganization in the absence of manic energy is suggestive of schizophrenia, with psychosis stemming from substance use or dementia ruled out (Altschuler, 2001).
In the early 1900s, Southard published efforts to evaluate the content of delusions. Southard (1912–13) believed that there existed a parallel between underlying true organic disease and delusional content, advising physicians to take cues from their patients’ delusional content when assessing for physical illness. Southard and Stearns (1913) sought to determine the influence of the environment on the patient’s delusional content. They explored the nature of such ‘allopsychic’ delusions among 31 patients at Danvers State Hospital in Massachusetts, US, after excluding cases with brain lesions evident at autopsy. These case study analyses, however, did not reveal a consistent effect. Southard (1915) continued to analyse delusional content, focusing next on personalized delusions, so called ‘autopsychic’, from the perspective of being of a pleasant or unpleasant nature. Southard (1915) hypothesized a relationship between kidney disease and unpleasant delusional content, and tubercular disease (‘phthisis’) and pleasant content, citing anecdotal data to support his contentions.
In an effort to continue exploration of the evolution, if any, of delusions, the present study sought to explore the content of delusions across the 20th century.
Methods
Records of delusional patients who were admitted to a state psychiatric hospital in Pennsylvania, US, were randomly sampled by decade (N = 102), to approximate equal cases across the century. Descriptions of the patients’ delusional beliefs were recorded and coded for category (persecutory, religious, somatic and grandiose) and bizarre or non-bizarre content. Discharge diagnosis was noted.
Discharge dates ranged from 1913 to 1999, with approximately 11–17 cases from each decade from 1940 onwards, with complete data available for only 15 cases from 1913 to 1939. Paranoid schizophrenia (or ‘dementia praecox-paranoid type’) was the most common diagnosis, comprising 42% of the sample. An additional 6% had a ‘paranoid condition’, with one case having a diagnosis of ‘paranoid state’. Chronic undifferentiated schizophrenia and catatonic schizophrenia were the next most frequent diagnoses (each 10%), with 9% diagnosed as manic, 6% hebephrenic, and the remaining 16% falling into various other psychotic categories (e.g. syphilitic psychosis, simple psychosis, delusional disorder, schizoaffective disorder, etc.). Mean age at admission was 38.7 years (SD = 14.9), with an almost equal representation of men and women (47% men, 52% women).
Results
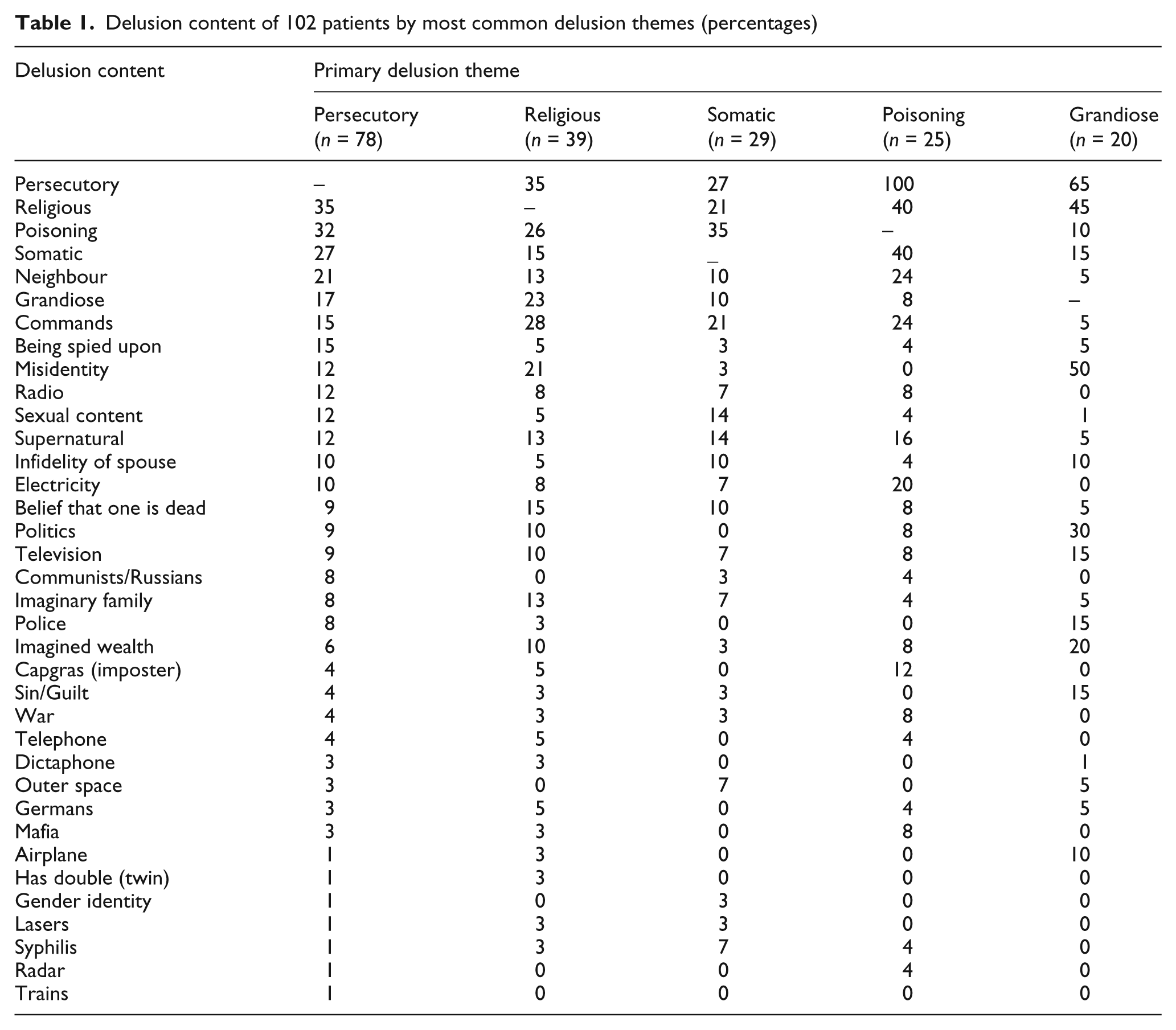
Analysis of delusional content reveals persecutory to be the most common theme (76%). Religious focus was the next most frequent at 38%, followed by somatic delusions (28%). Poisoning was the focus of 25% of the delusions. Grandiosity was exhibited by 20% of the sample.
When comparing those cases discharged prior to 1950 (n = 51) with those discharged after 1950 (n = 51), χ2 analyses reveal a greater frequency of general persecutory delusions after 1950, χ2(1, N = 24) = 4.17, p < 0.05. More specifically, cases of delusions involving one being spied upon occurred after 1950, χ2(1, N = 12) = 5.33, p < 0.05. The first half of the century did not differ from the second half in any other delusional content area. Frequencies of all delusional content are reported in Table 1.
Delusion content of 102 patients by most common delusion themes (percentages)
Twenty-two percent (22%) of the sample had bizarre delusions. Patients with non-bizarre delusions were less likely to have delusions with somatic content, χ2(1, N = 80) = 33.8, p < 0.001. Bizarre delusions did not occur more frequently in either half of the century.
Length of stay differed significantly for admissions pre- and post-1950, with the earlier group staying an average of 149.6 months (SD = 188.7) and the post-1950 group having an average stay of 30.2 months (SD = 69.9), t(94) = 4.01, p < 0.0001. No doubt the introduction of neuroleptic medications, the discharge of many chronic psychiatric patients in the early 1980s, and the more recent impact of managed care have contributed to these shorter stays. The most frequently used treatment approaches prior to 1950 were: hydrotherapy (18%), electroconvulsive therapy (14%) and ‘routine care’ (14%). After 1950, haloperidol was most frequently prescribed (20%), followed by chlorpromazine (18%), electroconvulsive therapy (18%) and loxapine (8%).
Discussion
The results are consistent with reports in the literature, with persecutory content being the most common delusional category. The other main categories of somatic, religious and grandiose also are well represented, with a large number of patients also reporting more specific persecutory beliefs of being poisoned. That more patients after 1950 believe they are being spied upon is consistent with the development of related technology and the advent of the Cold War. Delusional content tended to reflect the culture at the time, with focus on syphilis in the early 1900s, on Germans during World War II, on Communists during the Cold War, and on technology in recent years. Indeed, delusions now are being reported relating to computers (Stompe et al., 2003), the internet (Bell et al., 2005) and computer games (Forsyth et al., 2001).
In a study of delusional content among the records of Slovenian schizophrenic patients between 1881 and 2000, changes in delusional content were also correlated with historical events (Škodlar et al., 2008). The spread of radio and television was found to correlate with an increase in delusions of control. An increase in persecutory content was also found in this sample in the latter half of the 20th century, leading the authors to conclude: ‘This trend is primarily ascribed to urbanization, industrialization and technical developments with much new information and communication transfer, exerting considerable “cultural pressure” on an individual’ (Škodlar et al., 2008: 107).
Historical sociocultural influence on delusional content is also reflected in a review of 141 case histories of patients admitted to mental asylums in York, England, between 1880 and 1884 (Renvoize and Beveridge, 1989). Records indicate that 72.9% experienced delusions, with only 23.7% reported to have hallucinations. Delusions of persecution, grandeur and guilt occurred most frequently. Additional categories, in descending order of frequency, included: love, ill health, nihilistic, demonic possession, poverty, pregnancy, mis-identification, sexual interference, reference, infestation and infidelity of spouse (Renvoize and Beveridge, 1989). Religious delusions were found in 34.9% of Quaker patients and 17.4% of the non-Quaker patients. Renvoize and Beveridge attributed this frequency of religious content to the ‘considerable influence which organized religion still had at this time’ (Renvoize and Beveridge, 1989: 25).
Further support for the influence of sociocultural factors on delusional content comes from an examination of delusional content in different cultures. Consistent with the current study, persecutory delusions were the most common type found in a sample of 200 patients in India (82%), followed by delusions of reference (60%; Kala and Wig, 1982). Of interest was the finding that delusions of bodily control were the third most frequent, occurring in 31% of the sample. The authors suggest that this variation from delusional content in other cultures reflects the influence of practised religion in India, which engenders passivity and a lack of control by perceiving events as resulting from destiny (Kala and Wig, 1982). Although religious delusional content was reported in 21% of this sample, this theme is more common in other cultures, as in the current study. Rao (1966) addressed this phenomenon, stating:
Certain behaviour deemed as abnormal in the Western sense is culturally accepted in the Indian context, unless it becomes altogether intolerable. A person professing to have visions of God may be venerated unless he presents aggressive behaviour. Hence admission to a mental hospital may reflect only the incidence of mental illness transgressing the tolerance level of the immediate members of the family (Rao, 1966: 142).
Tateyama et al. (1998) compared samples from Japan, Austria and Germany and found differences in delusional content. Although persecutory delusions were the most common type in patient samples from all three countries, the specific content of the delusion varied (Tateyama et al., 1998). Patients in the Western European countries were more likely to have individually orientated persecutory delusions, such as being poisoned, while patients in Japan had greater occurrence of group-orientated delusions of reference, such as ‘being slandered by others’ (Tateyama et al., 1998: 66).
Similarly, Stompe et al. (1999) compared schizophrenic samples from Austria and Pakistan. Pakistani patients were found to be significantly less likely to have delusions related to guilt. Sharing the conclusion reached by Tateyama et al. (1998) regarding their Japanese sample, Stompe et al. cited the ‘shame culture’ of Asia as reducing the incidence of guilt-related delusions, while the ‘guilt culture’ of Europe influences the greater incidence of these delusions among European patients (Stompe et al., 1999: 231). It appears to be the broader cultural influences in Pakistan that influence delusional content, as no correlations were found between delusional content and the beliefs of a patient’s head of family (Ahmed, 1978).
Conclusions
In conclusion, it is apparent that both historical and cultural factors influence delusional content. Persecutory beliefs are consistently the most common type across time periods and cultures. The specific delusional content of such beliefs, however, may reflect either historical or cultural influences. An increase in persecutory delusion content appears to have occurred since the middle of the 20th century. Although limited by the incompleteness of early psychiatric hospital records, the present report provides further exploration of delusion content from both a historical and cultural perspective.
Footnotes
Acknowledgements
The authors wish to express their gratitude to Victoria Stewart, PsyD, for her assistance in the preparation of this manuscript.