
Abstract
Objectives:
To identify demographic or clinical factors associated with frequent admissions in a sample of patients admitted to an acute psychiatric hospitalization unit, controlling for potentially confounding factors.
Methods:
Socio-demographic variables, diagnosis, and the legal status, date and length of admission were collected for 1,722 consecutively admitted psychiatric patients during a period of up to eight years (1998–2005). Frequently admitted patients were defined as undergoing one or more admissions per year on average.
Results:
After controlling for potential confounding factors, logistic regression showed that being a frequently admitted patient was significantly associated with diagnoses of schizoaffective disorder, personality disorder or schizophrenia; an involuntary commitment at first admission; and younger age.
Conclusions:
Factors associated with frequently admitted patients should be identified in order to establish more effective strategies for preventing relapse.
Introduction
Frequently admitted patients (sometimes referred to as the ‘revolving door’ phenomenon) have been associated with a number of socio-demographic and clinical factors including diagnoses such as schizophrenia or schizoaffective disorder (Kastrup, 1987; Vogel & Huguelet, 1997), affective disorders (Vogel & Huguelet, 1997), substance-related disorders (Botha et al., 2010; Mellesdal, Mehlum, Wentzel-Larsen, Kroken, & Jørgensen, 2010; Vogel & Huguelet, 1987) and personality disorders (Kastrup, 1987; Mellesdal et al., 2010). In addition, results are frequently contradictory across studies, mostly due to the studies’ limited sample and/or follow-up, or the existence of confounding factors.
The purpose of this study was to identify demographic or clinical factors associated with frequent admissions (FA) in a sample of patients admitted to an acute psychiatric hospitalization unit, controlling for potentially confounding factors.
Methods
We analysed all patients (N = 1,722) consecutively admitted over a period of up to eight years (1998–2005) into one of the two general hospitals in Granada, southern Spain, which serves a catchment area of about 440,000 people. Data collected included socio-demographic variables (gender, age at first admission, marital status and residence location), diagnosis, and the legal status, date and length of admission. Diagnoses were taken from the discharge summaries made by treating clinicians, who followed the 10th version of the International Classification of Diseases (ICD-10). When diagnosis varied from one admission to another, we used the most recent. Following the criterion used by Mahendran, Mythil, Chong, & Chan (2005), patients who had an average of one or more admissions per year were considered frequently admitted (FA) patients. In order to allow for a follow-up time of at least one year, patients admitted for the first time in 2005 were followed up in 2006. Thus, no patient was followed up for less than one year.
Continuous variables and frequencies were respectively compared through student t or χ2 tests in univariate analyses. To identify an FA patient, we divided the patient’s number of hospitalizations by his/her follow-up time (measured in weeks). Since one admission divided by 52 weeks equals 0.019, any patient scoring ≥ 0.019 was considered an FA patient. A logistic regression model was built through a backward-selection procedure. The model’s dependent variable was being an FA subject, and socio-demographic variables, diagnosis, legal status at first admission and length of first admission were used as potential independent variables. The strength and direction of the associations were expressed by odds ratios (ORs) and their 95% confidence intervals (CI). The final logistic regression model fit well according to the Hosmer–Lemeshow goodness-of-fit test (Hosmer & Lemeshow, 2000).
Results
FA patients represented 10% of the sample (169/1,722). The mean age at first admission was significantly younger in FA patients than non-FA patients (37.3 vs 41.1 years, p = 0.002). Univariate analysis showed that FA patients were (1) not significantly more frequent among men than women (10% vs 9%, p = 0.3) and (2) borderline-significantly more frequent among non-married than married patients (10.5% vs 7%, p = 0.050). A first admission under involuntary commitment was more frequent among FA patients than non-FA patients (13% vs 2%, respectively, OR = 6.56, 95% CI = 3.61–11.92, p < 0.001). The mean lengths of first hospitalization for FA and non-FA patients were not significantly different (19.2 vs 16.0 days, p = 0.061). However, these lengths were significantly longer among men than women (19.1 vs 14.8 days, p = 0.021). Among FA subjects, the mean total length of stay combining all admissions was significantly greater in patients with schizophrenia than in the rest of the patients (23.5 vs 18.3, respectively, p = 0.005). According to the logistic regression (Table 1), after controlling for potential confounders, older age at first admission was significantly associated with lower odds of being an FA patient, and an involuntary commitment at first admission was significantly associated with increased odds of being an FA patient. Moreover, patients with schizophrenia, schizoaffective disorder or personality disorder had increased odds of being FA patients than did patients with neurotic disorders. Among FA subjects, (1) patients with schizophrenia were more frequently male than female (46% vs 17%, OR = 4.19, 95% CI = 1.97–8.92, p < 0.001) and (2) patients with personality disorder were more frequently female than male (21% vs 8%, OR = 1.77, 95% CI = 1.01–3.12, p = 0.011) and were younger than the rest of the patients (31.7 vs 38.1 years, p = 0.036).
Variables associated with being admitted one or more times per year in a sample of 1,722 patients who were admitted to a psychiatric unit between 1998 and 2005, according to a logistic regression model a
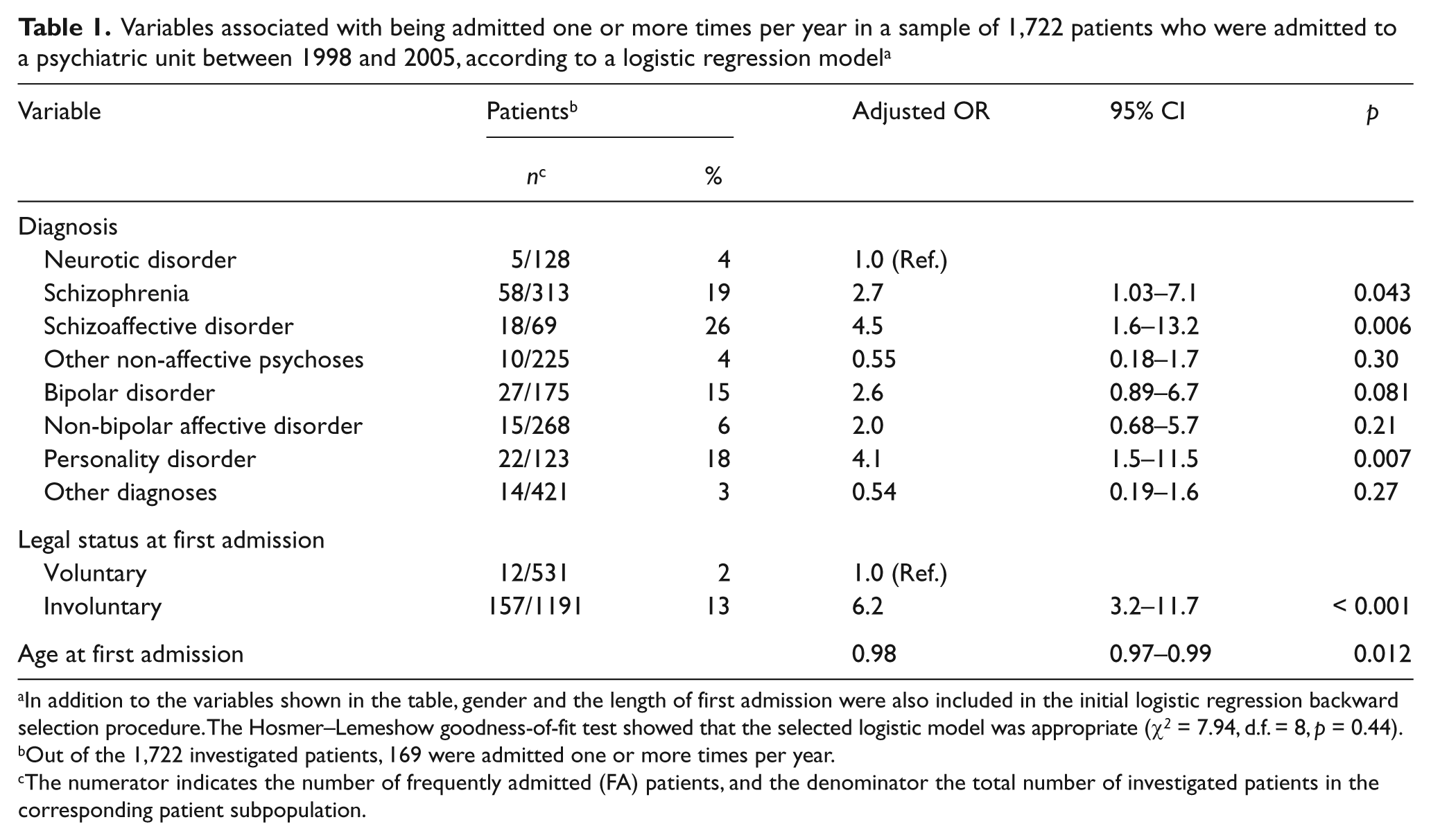
In addition to the variables shown in the table, gender and the length of first admission were also included in the initial logistic regression backward selection procedure. The Hosmer–Lemeshow goodness-of-fit test showed that the selected logistic model was appropriate (χ2 = 7.94, d.f. = 8, p = 0.44).
Out of the 1,722 investigated patients, 169 were admitted one or more times per year.
The numerator indicates the number of frequently admitted (FA) patients, and the denominator the total number of investigated patients in the corresponding patient subpopulation.
Discussion
The diagnoses most strongly associated with FA patients in this study were schizoaffective disorder, personality disorder and schizophrenia. A recent study (Botha et al., 2010) found that among patients with schizophrenia or schizoaffective disorder, (1) being an FA patient was associated both with higher PANSS scores and treatment with mood stabilizers, and with not being on depot antipsychotics, and (2) the admissions are often simultaneously precipitated by non-compliance and substance abuse. In the present study, among patients with schizophrenia, FA patients were significantly younger than non-FA (34.6 vs 38.1 years, p = 0.03); this was not the case for those with schizoaffective disorder. One related factor may be the abuse of substances, particularly cannabis, which may hasten schizophrenia pathogenesis and subsequent hospitalization. Patients with cannabis-induced psychosis developed schizophrenia at a significantly younger age than those with psychosis not associated with cannabis use (Arendt, Rosenberg, Foldager, Perto, & Munk-Jørgensen, 2005). On the other hand, we found that personality disorder was associated with FA, especially among young female patients. A poor adherence to treatment, a social support deficit, affective instability or substance abuse may contribute to increased admissions in patients with personality disorder. In a prospective study (Mellesdal et al., 2010), patients with both personality and substance use disorders had an increased likelihood of being readmitted because of suicide risk.
Regarding legal status, a study conducted in Israel (Rosca et al., 2006) found that patients who were involuntarily committed had a significantly greater number and longer duration of re-hospitalizations than those who were voluntarily committed. Lack of treatment compliance after discharge from the hospital or lack of insight among involuntarily committed patients may explain their increased odds of FA. An involuntarily committed patient study (Priebe et al., 2009) found that low levels of initial treatment satisfaction reported by the patients were associated with high readmission rates during the following year.
Finally, in this sample, after controlling for diagnosis, FA was significantly associated with younger age. Similarly, previous studies (Kastrup, 1987; Oiesvold et al., 2000) found that revolving-door patients are associated with younger age, although few of them controlled for the potentially confounding effect of diagnosis.
Strengths and limitations
Some strengths of this study are the large sample size and the characteristics of the sample, which was obtained from the mental health services of a catchment area, and is therefore representative of the usual clinical practice. The main limitations are that diagnoses were taken from charts recorded by different treating clinicians whose inter-rater reliability was not assessed, and that some variables related to patient’s social, clinical or functional status, such as treatment and outpatient care, were not established in this cohort.
Conclusions
FA patients may suffer from a more severe form of illness with disruptive behaviour, or perhaps may have more rapid access to inpatient units. A better understanding of these patients’ characteristics may help to establish more-effective strategies to prevent relapse. Social factors such as family or housing problems, which are non-psychiatric in nature and were not assessed in this study, may increase the likelihood of readmissions. These socioeconomic variables may be more important determinants of readmissions than of first admission (Haywood et al., 1995). Prospective longitudinal studies of patients with mental disorders that examine the relationship between clinical variables (including inpatient treatment), social factors and legal status must be considered.