
Abstract
Background:
Service user participation in direct service provision and evaluation has been developing in the western world in the past 20 years. However, this recovery-based care model is relatively new in Asia.
Aim:
To understand the views and perceptions of the service users and of psychiatric nurses about the recruitment of peer specialists in a regional psychiatric unit in Hong Kong.
Method:
A qualitative study using probe questions to understand the above issues in the form of focus group discussion. A total of 13 psychiatric nurses and 16 mental health service users were recruited from a regional psychiatric unit for the study.
Results:
Content analysis based loosely on grounded theory has identified several important themes. While service users are generally enthusiastic about the potential contribution of peer specialists in a service setting, they are much concerned about rejection and discrimination by the psychiatric staff. Psychiatric nurses are also sceptical about the involvement of peer specialists in the delivery of service, although for an entirely different set of reasons. In view of the divergent views of the service users and the psychiatric nurses, a second round of focus group discussion was conducted seven months later to understand whether the themes distilled were consistent with their views expressed in the first round of focus group discussion.
Conclusion:
It is encouraging is that, for those psychiatric nurses who worked with volunteer service users in the pilot scheme of ‘expert user participation’, there was a change in view towards positive acceptance about peer specialist involvement in service delivery. The study provides some insight into the potential obstacles to and opportunities in the implementation of peer specialist services in routine psychiatric services in Hong Kong.
Introduction
Expert users are central to the notion of person-centred recovery from mental illness, defined as a process of gaining and regaining goals and targets in life. This is a dynamic process where hope and aspiration play a pivotal role in shaping the functional outcome of rehabilitation (Corrigan, Mueser, Bond, Drake, & Soloman, 2008). Such an approach to recovery is radically different from the more medically oriented goal of achieving a semblance of normality through cure with the assistance of potentially lifelong medication. While the achievement of cure is more desirable, the former is more achievable and allows greater therapeutic optimism. A recovery-oriented service cannot be realized without the involvement of service users (in ways that are more than token) in two key areas: professional education and mental health service delivery. The study described in this paper was undertaken in Hong Kong using qualitative enquiry methods. The aim was to explore the views of service users and mental health nurses concerning expert user participation in psychiatric rehabilitation programmes in both inpatient and outpatient settings, as well as in professional staff education. The cultural context of service provision and professional education is somewhat more paternalistic and hierarchical than that currently prevailing in non-Asian countries. It was anticipated that these expectations would influence the acceptability of expert user involvement at both policy and practice level.
International experience
A central tenet of the recovery model is that empowerment of service users is conducive to positive outcomes. Studies have found that those who accept their mental illness and have a sense of mastery over it, and their lives, have a better outcome than those who passively accept their illness with resignation and internalized stigma (Lysaker, Davis, Warman, Strasburger, & Beattie, 2007; Vauth, Kleim, Wirtz, & Corrigan, 2007). Studies have found that service users expressed greater hope, sense of empowerment and satisfaction with services when peer support workers or peer specialists were involved in their clinical programmes (Corrigan, 2006; Davidson, Chinman, Sells, & Rowe, 2006; Resnick & Rosenheck, 2008; Warner, 2010). Randomized controlled trials comparing services with and without peer support workers have found no difference in hospital admission rates or length of stay (O’Donnell, Parker, & Roberts, 1999; Solomon & Draine, 1995). They did find a longer duration of maintenance in the community before first psychiatric hospitalization in services with peer support workers (Clarke et al., 2000) and better engagement with services (Sells, Davidson, Jewell, Falzer, & Rowe, 2006; see a comprehensive review by Repper & Carter, 2010). Peer support workers’ ability to foster an effective and stable alliance with patients at an early stage of treatment seems to be the key ingredient in the superior efficacy of services involving peer support workers (Sells et al., 2006; Solomon & Draine, 1995). Furthermore, benefits including increased self-esteem and enhanced interpersonal competence were observed in the peer support workers (Bracke, Christiaens, & Verhaeghe, 2008; Salzer & Shear, 2002). There is, therefore, ample evidence that involving service users as peer support workers or specialists in providing mental health services has significant benefits for both service users and peer support workers alike.
Transforming a traditional professional-led service into a recovery-based service demands change in organizational culture and care philosophy (Shepherd, Boardman, & Slade, 2008). Research into the effects of involving peer specialists in staff training suggests that medical and nursing trainees became more positive and empathic towards people suffering from mental illness, and showed greater awareness of personal factors relating to mental illness and stigma (Simmons et al., 2007; Wood & Wilson-Barnett, 1999). Gates and Akabas (2007) interviewed leaders of 27 organizations that employed peer support workers and found that a lack of understanding of recovery among existing staff and role confusion among peer specialists and existing staff were two of the major obstacles in integrating peer support workers into the service team.
Policy contexts
Increasing acceptance of this user-oriented service viewpoint is reflected by a growing emphasis on service user participation in government policies (Department of Health, 2001a). The National Service Framework for Mental Health in England stipulated that service users and carers should be involved in planning, delivering and evaluating all service programmes (Department of Health, 1999). Increasing numbers of mental health service plans have stipulated that local health authorities should ensure that service users are directly involved in the delivery of services. The guiding premise is that experts by experience may be more effective and acceptable coaches to service users (Department of Health, 2001b). Joint statements from professional bodies and community organizations have provided important guidelines on developing recovery-based practice and involving service users as peer specialists in services (Care Services Improvement Partnership, Royal College of Psychiatrists, & Social Care Institute for Excellence, 2006; Shepherd et al., 2008).
The Hong Kong Hospital Authority is the major government-funded health care service provider in Hong Kong. In its Mental Health Service Plan (2010–2015), one of the main objectives of mental health reform is to provide recovery-oriented mental health services (Hospital Authority of Hong Kong, 2010). This is a new perspective and presents an exciting challenge in relation to existing structures and staff. In 2011, a new Mental Health Service User group will be formed as one of the three working groups under the Implementation Task Force of the Mental Health Service Plan (2010–2015). The User Group consists of nominated service user and carer representatives from various patients’ and carers’ rights groups, representatives from the Hospital Authority (in which the first author is the convener) as well as from non-government organizations (NGOs) serving people with mental health problems. The major focus is to obtain users’ and carers’ views and opinions on future service design, service implementation and evaluation strategies and methods. The group will utilize opinions obtained for informing the Central Coordinating Committee (Psychiatry) of the Hospital Authority, the top advisory body for mental health services in the Authority, for future service planning. This is the first consultation group initiated by the Hospital Authority of Hong Kong that specifically targets mental health service users and their carers to solicit their feedback and opinions to inform mental health service planning. Each regional health cluster is also required to set up its own cluster-based service users’ and carers’ forum to collect their feedback and to report this to the Central Coordinating Committee (Psychiatry). In order to facilitate face-to-face discussion between top managers and service users and carers, it is intended to set up a regular open public forum in the head office of the Authority to facilitate direct dialogue.
The above initiatives appear to take important strides away from traditional medical paternalism. Yet there are no specific details of how recovery-based practice could be implemented and audited in the Mental Health Service Plan and the policy itself is ‘top-down’. Recent qualitative studies conducted among nurses, psychiatrists and service users revealed that their views about recovery were not conducive to the adoption of social recovery as a guiding care principle in Hong Kong (Ng, Pearson, & Chen, 2008; Ng, Pearson, Lam et al., 2008). Nor, so far, has there been a study of how staff and service users view expert user participation in psychiatric services in Hong Kong, a key ingredient in recovery-based practice. The study reported represents an initial attempt to answer the questions, how acceptable is the inclusion of expert users and what are the potential obstacles to their inclusion?
Method
The study used a cross-sectional design in the form of four focus group discussions. Members of the two staff focus groups were mental health nurses (one group of six nurses and the other of seven) from a local psychiatric department in Hong Kong. The other two focus groups were composed of service users suffering from severe mental illness (one focus group of eight service users from a rehabilitation ward and the other of eight service users participating in a clubhouse programme). Each focus group lasted about three hours, with a 15-minute tea break at the end of two hours of discussion. The facilitator of the service user groups’ discussion (the first author, RMKN) is an experienced local psychiatrist specializing in psychiatric rehabilitation. Facilitators of staff focus groups’ discussion (the fourth author, SNW, and the fifth author, SCW) are experienced mental health nurses with extensive experience in psychiatric rehabilitation. All four focus groups were audio-taped and verbatim transcription of the recordings was undertaken by the third author (YWP) and her associates who were not directly involved in conducting these focus groups. In the second stage the main categories and themes distilled from thematic analysis of the transcripts were used as feedback topics for further discussion in four additional staff focus groups (n = 13, 100% of the original participants) and two additional service user focus groups (n = 10, comprising 62.5% of the original participants). Three service users were hospitalized and two refused to give informed consent at the time of invitation to join the second round. This second stage was considered necessary to establish the validity of the content analysis, to ensure the full contribution of the participants in the research by providing an opportunity for them to add, subtract or qualify views previously expressed, and to offer criticism of the results. The time lapse between the initial and follow-up focus groups was seven months. The resulting discussion in all additional focus groups was subjected to the same kind of literal transcription and thematic analysis as the content of the original groups.
Participant recruitment
The third author invited a group of service users from the psychiatric rehabilitation ward and a group of service users attending the clubhouse to participate in the service user focus groups (U groups: eight male and eight female service users). Both facilities are run by the Department of Psychiatry of Kowloon Hospital. Participants were informed about the purpose of the focus group – i.e. that it was an attempt to understand service users’ views about the possibility of service user participation in running intervention programmes for other service users and in training mental health professional staff and students, with the possibility of introducing a new model that would involve service users in rehabilitation programmes and in staff education/training. Staff focus groups were conducted with mental health nurses (known collectively as S groups). The mental health nurses from all wards of the department were sent invitations to participate in this research project via internal email correspondence distributed by the third author. They were informed that the study was an attempt to understand personal views about service user participation in professional staff training and in conducting intervention programmes for other service users. Thirteen mental health nurses (five male and eight female) working in various wards consented to participate. All participants were fluent in Cantonese. Details of the participants in the service user focus groups have been provided in Table 1. Details of participants in the staff focus groups have not been given in view of the sensitivity of the personal data and request for anonymity by the participants. The study was approved by the ethics committee of the Kowloon Central Cluster of the Hospital Authority of Hong Kong. All participants gave written informed consent to their participation in this study. No financial incentive was offered. Light refreshments were provided during the tea break in the focus group discussions.
Users’ characteristics.

Discussion guideline
A discussion guideline was devised by the first and third authors, both having more than 20 years of experience in the care and rehabilitation of people suffering from severe mental illness. The guideline was intended to be used to probe focus group members’ views and to encourage open and free-flowing interaction. The guideline contained questions that were thought to be pertinent to the concept of service user participation in mental health service training:
Have you come across the idea of involving service users in the provision of rehabilitation programmes for patients?
If there were such service user participation, do you think it would help patients’ rehabilitation and re-integration into community life?
Do you find the idea of such participation acceptable? (question to patients)
Do you find the idea of such participation by expert users in programmes conducted by yourself acceptable? (question to staff)
What kind of rehabilitation programmes do you think we could invite expert users to conduct together with staff?
If you received such an invitation, would you accept? (question to patients only)
If you were invited as an expert user to participate in training programmes for staff would you accept? (question to staff only)
Do you think expert users would encounter difficulties if they were recruited to help run rehabilitation programmes for patients and training programmes for staff?
What do you think would be the risks and benefits associated with expert user participation in rehabilitation programmes for patients and training programmes for staff?
Special care was taken not to impose any concepts or personal values concerning expert user participation on the participants. The participants were told that they could stop the focus group at any time if they felt distressed by the discussion. None of them expressed either dissatisfaction or distress.
Data coding
A verbatim transcription of the audio-taped recording was made as described above. The data generated were analysed using a thematic content analysis approach, based loosely on grounded theory (Strauss & Corbin, 1998). Fine-grained consideration and coding of small units was used to build higher-order categories and main themes. This process led to the development of a central thematic framework to describe the data. The transcribed scripts were sorted into small units, each consisting of a single idea.
Inter-rater reliability
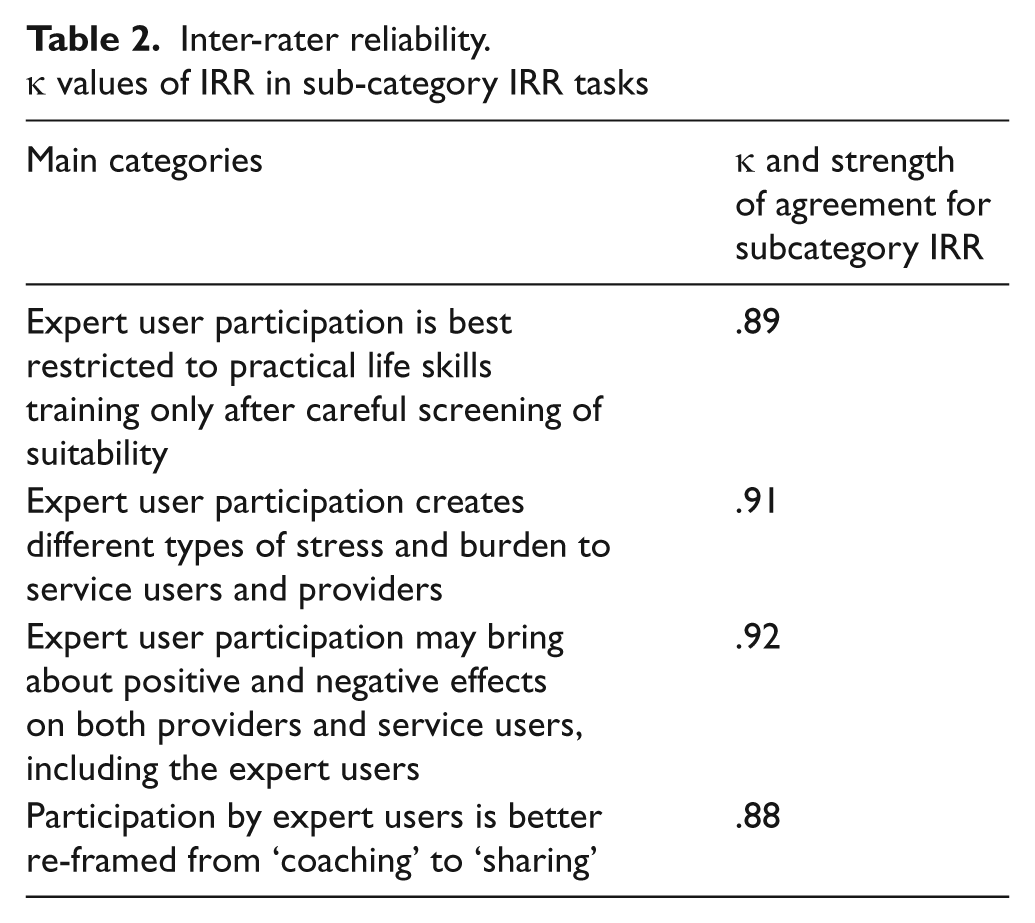
An independent rater (a postgraduate nurse research assistant unrelated to the current service unit) was asked to classify 30 sample quotations into four categories – assigned by the chief author (main category inter-rate reliability (IRR)) – without prior knowledge of those categories. The rater was asked to classify a body of 90 quotations into the sub-categories used in the analysis that follows, again without prior knowledge (sub-category IRR). IRR was calculated using Cohen’s kappa (ĸ). Values were interpreted according to the classification of the strength of agreement provided by Landis and Koch (1977). The ĸ value for the main category IRR task was .87 (equalling substantial agreement). The ĸ values for the sub-category IRR task are shown in Table 2. As can be seen, ĸ values ranged from substantial to almost perfect.
Inter-rater reliability. k values of IRR in sub-category IRR tasks
Methodological quality controls
Articles addressing this area (Elliott, Fischer, & Rennie, 1999) have suggested that verifying the reliability of observations and the validity of interpretations are of central importance in conducting rigorous qualitative research. The present study employed a number of recognized measures to control subjectivity and enhance transparency in these areas. These included the grounding of ideas in a fine-grained analysis of the data; tests of IRR with an independent researcher; the illustrative quotations reproduced below; and validity checking by reconvening the participants for further focus group discussion of the initial findings.
Results
Category 1: Differing expectations between users and staff as to the appropriate contributions of expert users
Staff tended to view service users as only capable of providing programmes focusing on simple procedural skills like cooking or cleaning.
Computer, chess, cooking classes can be considered.
A smarter patient can lead other patients, monitor them to improve self-care skills.
This is in contrast with the service users’ views about their possible contribution towards providing psychological support.
We can talk to other patients hospitalized in the ward and listen to their hearts.
And delivering mental health interventions with other service users.
We can take care of long-stay patients in wards to reduce the workload of the staff and contribute back to the staff.
Service users considered that they could offer special insights into the experience of illness and the effects of taking psychotropic medication.
We can remind other patients to take medication during home visits in the community and to encourage them to go back to normal life.
We can show other patients in structured programs how stopping medication can lead to devastating effects on ourselves and on our relatives.
They also considered themselves as having a ‘microscopic’ view about mental illness, which was of complementary value to the ‘macroscopic’ view held by the staff.
Staff are undeniably professionals but they look at things from a more global view… but patients have real-life war experiences.
Staff must keep abreast of new knowledge… learning directly from patients helps to supplement theories with real-life stories.
I am more “professional” than a young doctor in medication, as I have been taking different medications for the past 20 years…. Young doctors have little knowledge in this area.
Staff groups were extremely sceptical about the suitability and ability of service users to deliver effective training for patients and staff. The following statement is the most extreme example of this view.
If you ask an acute patient to teach in a cheese cake baking class, what if he takes out a piece of faeces for baking?
They were concerned about their lack of training and dissemination skills and thought that input from service users, if it were to be considered at all, should be confined to sharing their personal experiences with, for example, physical restraint and symptoms. The need for the careful clinical assessment of service users’ mental states by staff was raised in the staff focus groups, for fear of ineffective or inappropriate dissemination of information.
We must do quality assurance here: we need to see if these patients have adequate knowledge, if they are of sufficient calibre, if they need some kind of enrichment.
However, such worries appear unwarranted as the service users expressed similar concerns and were obviously aware of the potential pitfalls.
We must assess whether we are mentally stable enough to talk to other patients… I do not want to give wrong messages to fellow patients.
If the patient is not well himself while he is leading a group, this is a disaster as the staff will have to take care of an additional ill patient.
Patients can help to train staff and patients only if we have attended adequate courses in training skills.
Category 2: Differences between service users and staff in predicted sources of stress for expert users participating in rehabilitation and training
Both service users and staff expected that expert user participation in staff training and rehabilitation programmes for other service users would lead to increased stress for the expert users. However, the sources of stress identified by each group were radically different. Service users were worried about being dismissed as incompetent by the staff audience.
Staff will look down on us and view our teaching with scepticism.
Some staff who do not accept us may consider us as obstructing their work. Such differences may cause chaos in the ward.
You [user] try your best to influence them [staff], the question is whether they can take the message home.
Staff are professionals but we are not. They might think we are repeating the same thing and they think we are wasting their time and dismiss us as meaningless.
This was a valid concern as verified by the negative views expressed by staff about service user participation in this category and in category three below.
If I am so unfortunate that I have to recruit patients as teachers (giggles)… unless the caregivers are doctors or nurses, I would not accept patients teaching me professional stuff.
Staff worried that the stress of public speaking, learning the training material and preparing such training would lead to a psychotic breakdown. They also had doubts that users would be able to be independent teachers.
Assessing the suitability of the patients for teaching and preparing teaching stuff for them are stressful for staff… We are used to preparing stuff to teach patients.
Asking patients to prepare the teaching material is too stressful for them… they will have more self-muttering.
If they do not perform well in the teaching session, they will have a sense of failure and worsen their feelings. This would lead to unpredictable consequences.
To speak in front of a group of professionals who know these things well and yet the speaker knows less than the audience this would create stress for the patients… they will not be able to cope and will be sent back to the admission ward.
None of the service users mentioned stress arising from preparation procedures. Another prominent concern raised almost exclusively by the staff was that service user participation could upset the balance of power and challenge the ‘old wisdom’.
I cannot imagine that a patient can teach a group of nurses, no matter what rank, even including our Director of Operations! How come we can be taught by this other way round? (sighing and shaking his head)
Users showed rather more understanding of the staff’s likely reactions and the barriers that would have to be overcome to change the old ways.
This is a new way of working and needs a lot of courage, resource and dedication from staff… a determined and influential figure must be willing to come out and stand up for this [movement].
Category 3: The impact of expert users’ participation on other service users
Both service users and staff shared the view that expert users would be useful to engage with other service users in rehabilitation programmes. They also thought that involving expert users in ward activities would enhance the empathy of staff and have a direct emotional impact on patients. The staff mentioned that if service users shared with staff their distress about being physically restrained, this might enhance staff empathy so that they sought to reduce resorting to such restrictive methods.
However, none of the staff participants shared the view of the service users that expert users could serve as positive role models, fostering hope and higher levels of responsibility in other patients, for instance in relation to medication compliance.
I once disclosed to other patients in the training group that I occasionally omitted medication. They then also shared these secrets. We then discussed how we were different persons while we were in relapse and how medication helped all of us.
We must monitor what they [users] will say as they may encourage others to not take medication.
Service users expressed very clearly that it was important to them that they were able to contribute and to give something back, to help others whose situation they understood only too well.
I feel I am helping patients and staff. I am useful.
I am not just sucking resources from the community. I can contribute to society.
And, rather more poetically:
I am now a piece of unpolished gem stone. If I am given the opportunity to help other patients, I can help others and give myself opportunities to polish and transform myself into a piece of jade.
Only one nurse identified benefits for service users concomitant on involving expert users in rehabilitation programmes, and that was to do with medication compliance. Most of the nurses failed to see beyond the potential risks (real or imagined) of the involvement of expert users in rehabilitation programmes and staff training, and tended to focus on the nursing staff’s concomitant loss of control and authority.
I guess that patients sometimes cannot control what they say and give wrong information.
A user might have constipation due to inadequate fruit intake and he erroneously associates this as side effect of medication and this will misguide our staff to think that the medication will cause constipation.
I have encountered occasions when the patients delivered the opposite message and this was readily endorsed by other patients in the group. This would affect our teaching to patients.
They seemed to have little sense of the benefits that might accrue from expert user involvement to the expert users themselves, to current service users and to the staff. Service users were very much more aware of the possibilities for hope and optimism in relation to recovery.
The user coach can serve as a role-model for other patients so that they can be like the user coach one day.
This is a project of hope. Although it is still a twig now… with water and sunlight, it will stand up and grow.
Maybe I do not have the ability to lead today, but we have the opportunities [to become expert users] and we can all move one step forward.
I can tell other patients how I got back to the community and they will know that every one can do that. It is just a matter of time. It is okay. It is absolutely possible.
There were no equivalent comments from staff.
Category 4: Is it more appropriate for expert users to be seen as ‘sharing their experience’ rather than as ‘teaching’?
Both service users and providers in the focus groups concurred that referring to expert user participation as ‘teaching’ or ‘coaching’ might be ‘too heavy’. Traditionally, among the Chinese, a person’s teacher is second only to parents in importance and must be treated with deference and respect. A teacher is expected to be morally upright, wise and knowledgeable, and the act of teaching is assumed to involve a one-way communication that takes place in a classroom and involves many students in passive roles.
It is better for staff to lead the group as they are more positive and structured in approach. User coach will not know how to control the chaotic situations in [that can arise in a] group.
We took so many years to learn nursing and to train others, how can patients teach in the absence of the same number of years of education and training? They can only share their personal experiences… not expert knowledge.
I am not smart so I cannot lead. I would rather share my experiences when called upon by staff.
Both service users and staff preferred the term ‘sharing’. In the eyes of the service user it demotes the expert users’ knowledge and input, thus reducing the service users’ fear of scepticism from staff, a form of expectation management. From the staff viewpoint, it reduces the chances of disturbing the existing power balance that favours the staff. Such a hypothesis explains why in category 1 service users thought of themselves as experts in their own mental illness, yet in category 4 claimed that it would be better to see them as ‘sharing their experience’ rather than as ‘teaching staff and other patients’. This suggests that while they saw themselves as ‘experts by experience’, they had serious reservations about staff responses to them portraying themselves as such. This interpretation is consistent with the concerns expressed by staff about the possibility of upsetting the balance of power in mental health services by incorporating expert user participation. This demotion of the importance of expert users is further reflected in the opinion of most service users that a salary would not be required for their services.
I do not want money as payment implies a certain standard expected from me. This would create stress to me.
I do not want to fight for fame and profit with staff. I just want to help other patients.
However, at least some staff thought expert users should be paid for their efforts, if only to encourage commitment and reliability.
The users have to think about their future and they need to earn money. If users or caregivers are not paid for their service, it is difficult.
If you want to make sure that they will turn up for the training work you have to pay them [users and caregivers].
Diverging views: Are they valid?
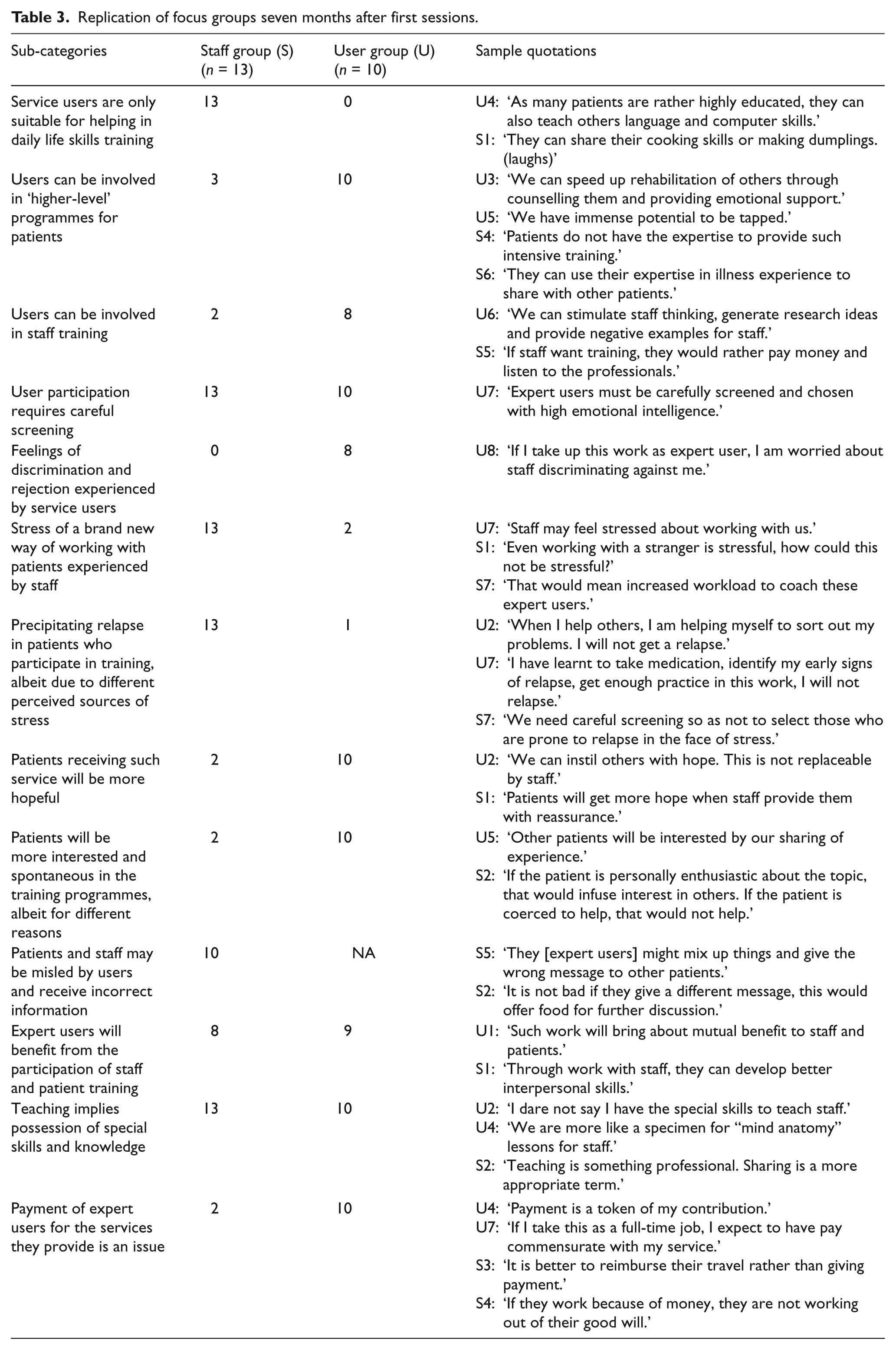
In view of the divergent views of the service users and staff on various aspects of expert user participation in rehabilitation programmes for service users and staff education programmes, participants were invited to take part in a review of the themes and categories distilled from thematic analyses. The consistency of the differences between the staff and service user groups after a lapse of seven months confirms that the themes obtained from previous groups were not transitory. Two changes emerged from the second series of focus groups. Staff who worked in the rehabilitation ward had been exposed to some pilot work in expert user participation and their views were observed to have become more tolerant, exemplified by the following statement.
Even if expert users express a different view [from that of the staff] about medication to our patients, it is also an opportunity to stimulate more discussion among the patients.
More staff endorsed the view that expert user participation would be of benefit to the expert users themselves, mainly because participation in these programmes was an opportunity to improve interpersonal skills.
Such work will bring about mutual benefit to staff and patients.
Through work with staff, they can develop better interpersonal skills.
Further examples of responses are given in Table 3.
Replication of focus groups seven months after first sessions.
Discussion
The goal of Hong Kong’s Mental Health Service Plan is rolling out recovery-based services. Is this a case of ‘ready or not, here we come’? Our research group previously found that both service users and staff were still heavily biased towards medical recovery as the only way (Ng, Pearson, Lam et al., 2008). Such narrow views of recovery were rooted among psychiatrists well before their graduation from medical school or from their psychiatric training institutions (Ng, Pearson, & Chen, 2008; Ng et al., 2010). Our research group has found that such a pessimistic view of recovery was a gradual process of ‘acculturation’, as they were more optimistic about their recovery at their early stage of illness (Lam et al., 2009).
The current study extends such findings into the area of expert user participation, an important step towards recovery-based practice. Our research indicates major differences between service users and nursing staff about recruitment and involvement of expert users in service delivery. Staff in this study adopted a rather authoritarian and pessimistic view about the capacity of expert users to work alongside staff in delivering service programmes and in ‘teaching’ mental health staff. These views reflect the conventional medical view of schizophrenia as a progressively deteriorating brain disease with predictable decline in social and vocational functioning (Edwards, Maude, McGorry, Harrigan, & Cocks, 1998; Robinson et al., 2004). Thus, among both service users and staff in Hong Kong, recovery equates to cure (Ng, Pearson, & Chen, 2008; Ng et al., 2010). Although widely accepted, this has been challenged by international evidence (Repper & Carter, 2010; Shepherd et al., 2008).
There is also a fear that expert users might ‘indoctrinate’ other service users with concepts and attitudes aversive to positive mental health in the eyes of the staff, especially promoting non-adherence to medication (Felton & Stickley, 2004). Yet it was evident from the focus group discussions that service users’ views on medication and its pros and cons were nuanced and informed. There was no suggestion that their default position was anti-medication.
Existing international evidence is clear: service users can contribute positively to mental health services by acting as case managers, trainers and researchers (Simpson & House, 2002) and to the promotion of the self-management of mental health problems (Sells et al., 2006). This is supported by results from cohort studies and randomized controlled trials comparing services with and without peer specialist involvement (see Repper & Carter, 2010 for a comprehensive review of current evidence).
Service users may hold views about conventional treatment approaches that are different from those espoused by staff. This is hardly news, particularly in relation to medication compliance. Involving expert users in service delivery should encourage an honest and open dialogue between staff and service users to address these issues, thus providing opportunities that are currently lacking for reflection and the improvement of our existing mental health service provision model (Crawford et al., 2002). There is no reason why Hong Kong should not be part of this trend (Ng, Pearson, Lam et al., 2008). Open dialogue would foster better trust and rapport between service providers and service users, with expert users acting as the catalyst for user empowerment (Warner, 2010).
Underlying staff reluctance to incorporate expert user participation is the fear of change, which calls for the acquisition of additional skills and acceptance of new ideas, plus the willingness to give up old ones. This raises issues of loyalty and questions the validity of past professional practice and can lead to profound psychological discomfort. Yet this is what is necessary if staff are to train expert users in the skills that will allow them to fulfil their potential, such as presentation, assertiveness and effective negotiation. Staff will need to negotiate with expert users who hold different views about illness and care provisions and to translate these different views into intriguing agendas for discussion and exploration. All this must be achieved in a context of maintaining a delicate balance between respecting expert users as collaborating partners and helping to maximize their potential and fulfil their aspirations in the face of the real limitations imposed by severe mental illness.
This is a difficult and challenging task, yet eminently worthwhile. However, change should not be one sided and Ahuja and Williams (2005) have rightly pointed out that effective partnership between service users and professionals should involve changes in attitudes on both sides. Listening to service users’ anger about service provisions could be unsettling and lead to defensiveness. Expert users can be encouraged to present their perspectives and views in a constructive fashion, addressing the fear expressed by staff in the focus groups about possible ‘indoctrination’ of other service users by the expert users.
Even more challenging for staff is the need for a fundamental change in their philosophy of care. It is hard to see how the nurse who imagined an expert user producing faeces as an ingredient for cheesecake in a cookery demonstration could make the conceptual leap to mutual trust and respect. Such a shift from medical paternalism to collaborative partnership understandably arouses anxiety and concern in staff afraid of losing service users’ respect, relinquishing their power and losing control. Recognizing that service users having knowledge about their own illnesses is of equal importance to recovery poses a threat to some professionals who fear giving up their roles as experts on health matters (Hanson & Mitchell, 2001). A survey of psychiatrists showed that some found it difficult to accept service users as appropriate teachers of staff. They feared that such a reversal of roles would have an adverse impact on their relationships with their patients and entail a loss of respect and status (Ahuja & Williams, 2005; Alison, 2003). This view was also strongly held by many of the nursing staff in our focus groups. Yet rigid adherence to a care provision model not conducive to the recovery of the very people that service providers are expected to serve only invites antagonism, rejection and non-adherence. There is ample evidence that non-adherence to medication is related to intentional discontinuation (Wroe, 2002). Why then are patients reluctant to mention that they have stopped medication? Strong evidence links the quality of the doctor–patient relationship with patients’ compliance with medical advice (Stevenson, Cox, & Britten, 2004). The clinical professionals’ ability to influence service users involves communication, trust and confidence (Trachtenberg, Dugan, & Hall, 2005). Greater service user participation in health care decision-making, the delivery of mental health training for staff and the delivery of mental health services would enhance trust between service providers and service users as well as foster stronger therapeutic alliances between staff and service users. This should translate into more effective health care benefits for patients, carers and mental health professionals, as well as society as a whole.
Other unresolved issues of expert user participation found in the literature include setting ethical boundaries between expert users and service users; service provision to expert users in the face of their possible deterioration in mental health; and provision of peer supervision and mentoring to expert users during their service delivery. There are also issues around convincing human resource departments of the necessity to recruit staff by experience rather than by educational qualification or previous work profile (Chinman et al., 2008; Gates & Akabas, 2007). These experiences may provide some insight to service providers on how to troubleshoot these problems, but solutions acceptable in Hong Kong require hands-on experience of recruiting and working with expert users.
A pilot project involving expert users’ participation is now being conducted in Hong Kong, with expert users involved in rehabilitation programmes involving daily living skills and the education of medical and allied health students about the personal journey of recovery. In addition, a Rehabilitation Department-wide opinion survey concerning the structure and content of patient education programmes has been conducted. In the second round of staff focus groups reported in this article, those working in the rehabilitation team evidenced a significant change in their views about expert user participation, suggesting that actual experience of working with expert users is a key method of transforming staff attitudes and organizational culture. As time is needed to convince policy makers about the value of the inclusion of expert users in mental health teams, the research group is now planning to apply for research funds to pilot test an expert user employment programme. This will involve the collection of prospective data on levels of satisfaction among expert users, staff and service users, plus measuring the sense of recovery and hopefulness among service users participating in the pilot project.
However, without due care, service user involvement can be open to criticism by the public and mass media in Hong Kong on the grounds that it exploits vulnerable people. Clearly, patients should be offered a genuine choice about becoming involved in training. There is some evidence that choice of this kind rarely exists and that service users are being exploited to educate health professionals (Livingston & Cooper, 2004) and that some expert users have been recruited for clerical jobs to relieve staff shortages rather than contributing their experience of illness (Chinman et al., 2008). The reluctance among some participants in staff focus groups to accept that expert users should be paid for their time in anything other than a token way suggests such a risk could exist in Hong Kong. It also suggests a devaluing of what an expert user can offer. As mental health professionals, we tread a fine line between being criticized for tokenism in user involvement in order to satisfy political initiatives and of exploiting our service users to advance our health care initiatives and policies. It demands advanced ‘acrobatic skills’ to turn expert user participation into something both meaningful and beneficial for our service users, our carers and our colleagues.
Conclusion
Changes at the policy level that are about to see the introduction of the Mental Health Service User Group into the formal management structure of mental health services in Hong Kong make the findings in our study of particular relevance. Without at least some level of acceptance of the involvement of expert users in treatment and training by professional staff, it will be all too easy for them to subvert the intentions to open up service provision to user influence. It is far from obvious that such levels of acceptance currently exist among nursing staff.
It appears that service users in Hong Kong are ready to contribute their time and effort in taking up the expert user role. They value such expert user participation as an opportunity to learn new skills and to assist other service users and staff, even in the absence of monetary incentives. However, it is apparent that service providers, namely our mental health nurses in the study, focus more on the risks associated with service user participation (precipitating relapse in the expert users, service users ‘being led astray’ by expert users’ divergent views, etc). The risk-averse attitude of the mental health professionals is translated into stringent selection criteria for expert users (possession of a good knowledge base about mental health care, competencies in training and dissemination of skills and knowledge, etc). This makes an interesting contrast with the relatively tolerant attitude that staff display in recruiting novice staff without prior experience. They argue that such novices can be trained and become mature and experienced with clinical exposure and mentoring from senior clinical staff. Clearly, different paradigms are being applied to the two groups of human beings. The pertinent question here is whether we, as mental health professionals, are prepared to apply a similar mindset and offer a similar level of support towards the training of expert users. A logical extension of this pertinent question is the key issue of whether mental health staff are prepared to share their power with their service users and to value their unique insights and experiences (the ‘microscopic view’/‘local knowledge’) as being of equal importance as the expertise of staff (the ‘macroscopic view’/’cosmopolitan knowledge’). Users are prepared to accept the challenge of change, but are we?