
Abstract
Aims:
Many patients have stigma about depression, which may inhibit treatment seeking. However, most previous research in this area has been conducted in outpatient samples. The current study investigated self-stigma and its relationship with treatment beliefs in depressed patients receiving psychiatric hospital treatment.
Method:
The sample consisted of 55 hospitalized patients with depressive disorders who completed measures of self-stigma, medication beliefs, psychotherapy beliefs and depression.
Results:
Multiple regression analyses controlling for demographic variables demonstrated that higher depression severity was associated with increased self-stigma related to treatment and having depression. Higher self-stigma about treatment was associated with more negative beliefs about psychiatric medications, but more positive beliefs about psychotherapy. In contrast, self-stigma about depression was associated with negative beliefs about medications, but not psychotherapy.
Conclusions:
Psychiatric hospital treatment, particularly in the USA, emphasizes medication treatment while de-emphasizing evidence-based psychosocial interventions. Individuals with negative views about psychiatric medications and positive views about the value of psychotherapy have higher treatment self-stigma, which may discourage them from seeking hospital treatment when needed or negatively affect their treatment response.
Introduction
Stigma refers to the various negative attitudes that people may have about mental illnesses and their treatment (Corrigan, 2005). Researchers often differentiate between two main types of stigma: public stigma, which involves attitudes held by the general public towards those with mental illnesses; and self-stigma, which represents internalized attitudes held by those with mental illnesses. Stigma in its various forms is recognized to be an important public health concern (President’s New Freedom Commission on Mental Health, 2003). Studies have shown that increased self-stigma is associated with reduced treatment seeking and engagement (Kelly & Jorm, 2007; Rusch, Angermeyer, & Corrigan, 2005). A recent meta-analysis of 127 studies demonstrated that higher self-stigma is correlated with a number of variables, including lower levels of hopefulness, self-esteem, self-efficacy, quality of life and social support, as well as higher psychiatric symptom severity and treatment non-adherence (Livingston & Boyd, 2010). Research suggests that self-stigma typically is a more powerful predictor of help seeking compared to public stigma (Barney, Griffiths, Jorm, & Christensen, 2006). Although most of the research on stigma has focused on patients with schizophrenia or other forms of chronic mental illness, studies also have found similar effects of stigma in depressed samples (Kanter, Rusch, & Brondino, 2008).
Furthermore, research suggests that public and self-stigma are interrelated, indicating that public stigma increases self-stigma, which in turn leads to various treatment barriers (Manos, Rusch, Kanter, & Clifford, 2009). Stigma theory posits that negative societal views about mental illness become a barrier to affected individuals seeking treatment for their condition. This public stigma becomes internalized by the individual and produces shame and guilt as these negative stereotypes become personally adopted (Corrigan, 1998).
In addition to self-stigma, a large body of research suggests that patients’ attitudes towards treatment affect outcomes and adherence. For example, findings from the National Institute of Mental Health’s Treatment of Depression Collaborative Research Program study demonstrated that treatment expectancies predicted response across both the psychotherapy and pharmacotherapy conditions (Sotsky et al., 1991). In addition, Aikens, Nease, Nau, Klinkman and Schwenk (2005) found that antidepressant adherence was lowest when depressed patients believed that the harm exceeded the need for medications in a primary care sample during maintenance treatment. In a clinical trial of antidepressants, Krell, Leuchter, Morgan, Cook and Abrams (2004) found that 90% of depressed patients who reported high expectancies for improvement at the start of the study responded to treatment, compared with only 33% of those who expected the medications to be ‘somewhat effective’.
Most previous studies on stigma and treatment attitudes have focused on depressed outpatients. Although some research on stigma in patients during psychiatric hospitalization is available (Chee, Ng, & Kua, 2005; Verhaeghe, Bracke, & Bruynooghe, 2007), we are not aware of recent studies conducted in an inpatient sample in the USA that specifically focus on self-stigma and its relationship with attitudes towards treatment. Previous research suggests that negative views about treatment predict increased self-stigma in outpatient samples (Prins, Verhaak, Bensing, & van der Meer, 2008). However, it is important to study the relationship between stigma and treatment in hospitalized samples as they may have different attitudes and unique barriers to treatment. Thus, we investigated the relationship between patients’ treatment beliefs and self-stigma in an inpatient sample with depression. We hypothesized that negative beliefs about medications and psychotherapy would predict higher self-stigma about depression and its treatment.
Method
Sample
Participants were 55 patients treated at a 160-bed, acute care psychiatric hospital in the USA. Average length of stay was approximately one to two weeks. Although pharmacotherapy was the primary treatment modality, interventions were delivered by a multidisciplinary team and included adjunctive group psychotherapy, occupational therapy and aftercare planning services, as is typical of similar psychiatric facilities in the USA. Inclusion criteria were: (1) a chart diagnosis of a depressive disorder, including major depressive disorder, dysthymia or depressive disorder not otherwise specified (NOS); (2) being over the age of 18; and (3) the ability to speak and read English sufficiently to complete study procedures. Exclusion criteria were: (1) the following chart diagnoses: bipolar disorder, schizophrenia or other psychotic disorder, mental retardation or a cognitive disorder (e.g. dementia); or (2) involuntary hospitalization.
The mean age of the sample was 40.1 (SD = 13.7) and mean years of education completed was 13.0 years (SD = 3.2). A total of 56.4% of the sample were women, 92.2% were white, 3.6% were Hispanic, 29.6% were currently married, 46.6% earned an annual income of less than $30,000, and 66.6% identified themselves as Christian. Their mean BDI-II score was 29.4 (SD = 14.2), which is in the severe range. The study participation rate (number consented/approached) was 75.6%.
Measures
Depression Self-Stigma Scale (DSSS)
The DSSS is a 32-item self-report scale that measures patients’ self-stigma related to depression (Kanter et al., 2008). The general self-stigma about depression (nine items) and self-stigma related to treatment (four items) subscales were administered to the current sample as they were most relevant to the study aims. The general depression self-stigma scale assesses negative attitudes held by respondents about their own depression (e.g. ‘When people learned I was depressed, they looked for flaws in my character’). The treatment self-stigma scale represents stigmatizing attitudes about receiving treatment for depression (e.g. ‘It is advisable for a person to hide from people that he/she has been treated for depression’). Items are rated from 1 = ‘completely disagree’ to 7 = ‘completely agree’. Items were summed for each subscale, and higher scores indicate higher self-stigma. Kanter et al. (2008) reported a good factor structure, internal consistency and construct validity for the DSSS. Internal consistency according to Cronbach’s α in the current sample was 0.74 for the treatment subscale and 0.90 for the general subscale.
Beliefs about Medicines Questionnaire (BMQ)
The BMQ is a widely used, 18-item self-report measure that assesses people’s beliefs about taking prescribed medications for controlling their illness and concerns about potential side effects (Horne & Weinman, 1999). Respondents rate their agreement on a Likert-type scale, ranging from 1 = ‘strongly agree’ to 5 = ‘strongly disagree’. The mean of the individual items was calculated to derive a total score, with higher scores indicating more negative beliefs about medications. Research has shown the scale to be predictive of outcomes associated with antidepressant treatment (Aikens et al., 2005). Internal consistency according to Cronbach’s α in the current sample was 0.87.
Beliefs about Psychotherapy Scale (BPS)
The BPS is an eight-item self-report measure assessing patients’ beliefs about psychotherapy (Bystritsky et al., 2005). Respondents rate their agreement to items on a Likert-type scale, ranging from 1 = ‘strongly disagree’ to 5 = ‘strongly agree’. Items were summed to derive a total score, with higher scores indicating more positive beliefs about psychotherapy. Previous research in a sample with emotional disorders showed that the scale has good internal consistency and concurrent validity (Bystritsky et al., 2005). Internal consistency according to Cronbach’s α in the current sample was 0.72.
Beck Depression Inventory-II (BDI-II)
The BDI-II is a 21-item self-report instrument that assesses cognitive and somatic symptoms of depression (Steer, Ball, Ranieri, & Beck, 1999). The psychometric properties of the BDI are well established (Beck, Steer, & Garbin, 1988). Internal consistency in the current sample according to Cronbach’s α was 0.89.
Procedure
Medical charts were screened by a research assistant (RA) to identify patients meeting the study inclusion/exclusion criteria. After identifying a potential participant, the RA asked the treating physician for his/her permission to approach the patient about study participation. If permission was granted, the RA provided a brief explanation of the study according to procedures approved by the Institutional Review Board. After signing the consent form, the patient was given an assessment pack to complete. The RA collected the completed assessment pack from the patient. Patients also completed measures of expectancies related to participation in hypothetical clinical trials, which is reported elsewhere (Gaudiano, Hughes, & Miller, under review). Patients were paid for completing the study.
Statistical analyses
First, simple correlations were conducted to examine the uncontrolled relationships among relevant demographic variables and study measures. Next, hierarchical multiple regression analyses were conducted to examine predictors of self-stigma. Hierarchical multiple regression was used to examine the unique variance explained by the variables (i.e. treatment beliefs) of interest after controlling for background variables.
Results
Simple correlations
Inter-correlations and descriptive statistics are presented in Table 1. Greater depression severity was associated with greater general self-stigma and female gender. Higher treatment self-stigma was associated with higher general self-stigma. Negative medication beliefs were associated with increased treatment self-stigma, increased general self-stigma, negative psychotherapy beliefs, younger age and lower educational attainment. Negative psychotherapy beliefs were also associated with lower educational attainment.
Correlations and descriptive statistics for study variables.
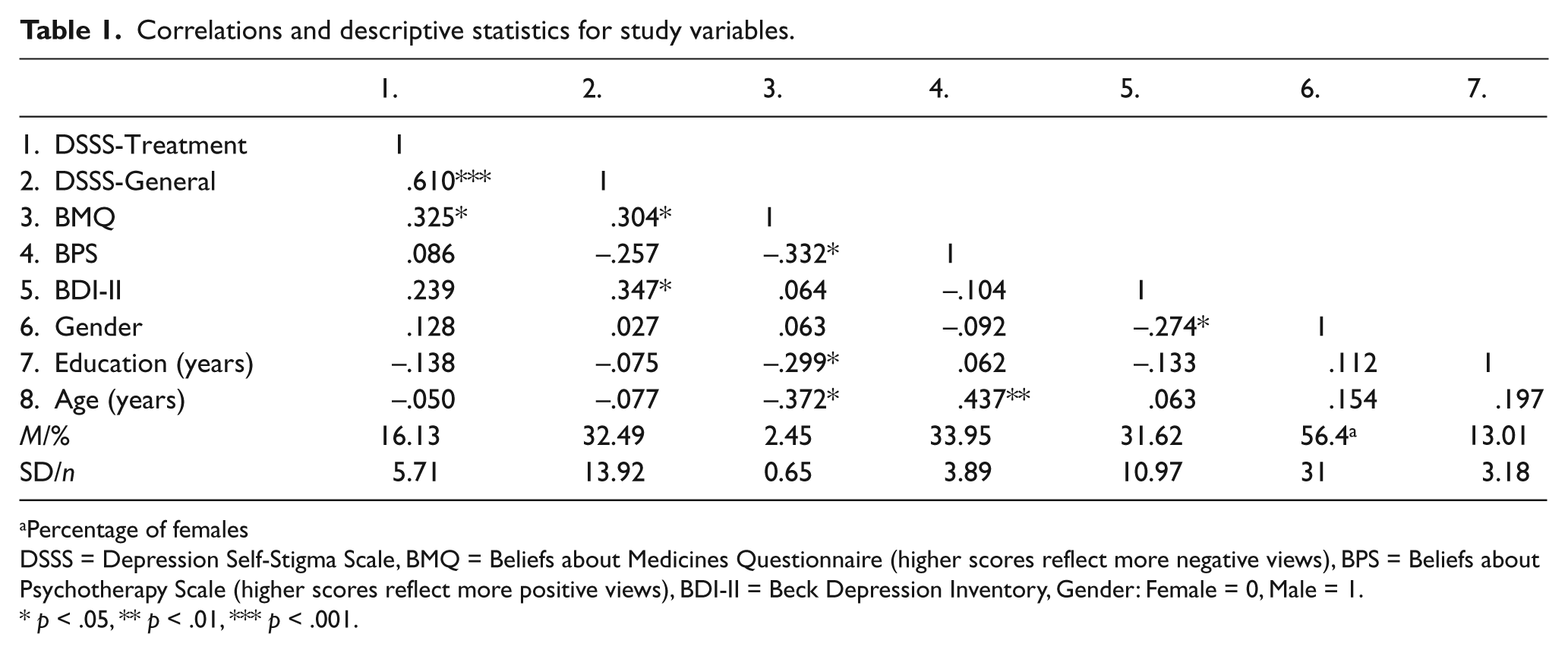
Percentage of females
DSSS = Depression Self-Stigma Scale, BMQ = Beliefs about Medicines Questionnaire (higher scores reflect more negative views), BPS = Beliefs about Psychotherapy Scale (higher scores reflect more positive views), BDI-II = Beck Depression Inventory, Gender: Female = 0, Male = 1.
p < .05, ** p < .01, *** p < .001.
Multiple regression analyses
Gender, education and age were entered in the first step of the regression. Depression severity, medication beliefs and psychotherapy beliefs were entered in the second step of the regression (Table 2). The second step of the regression analysis predicting treatment self-stigma was significant (FΔ = 4.67, d.f. = 3, 42, p = .007). Higher treatment self-stigma was predicted by more positive views about psychotherapy, more negative beliefs about medications and greater depression severity. A total of 28.1% of variance in treatment stigma was explained by the variables. In addition, the second step of the regression analysis predicting general self-stigma about depression was significant (FΔ = 4.10, d.f. = 3, 41, p = .012). Higher general self-stigma was predicted by more negative beliefs about medications and greater depression severity. Psychotherapy beliefs did not significantly predict general self-stigma. A total of 24.3% of the variance in general stigma was explained by the variables.
Hierarchical multiple regression analyses predicting self-stigma.
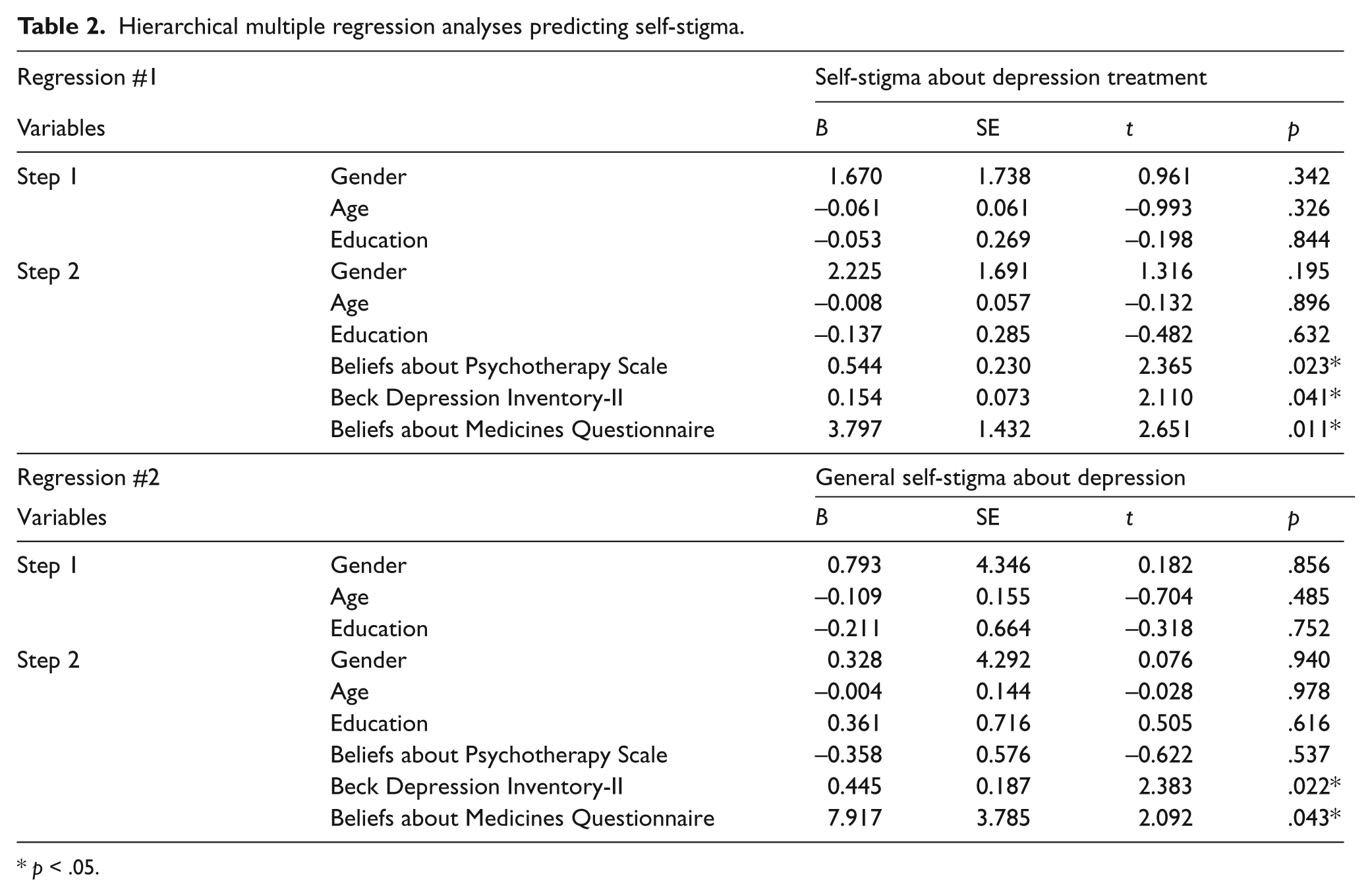
p < .05.
Discussion
Our results showed that more negative beliefs about psychiatric medications and more positive views about psychotherapy were associated with increased treatment self-stigma in our inpatient hospital sample. We expected more negative beliefs about medications to be related to increased stigma, but the association between psychotherapy beliefs and self-stigma was the opposite of what we had hypothesized. To explain this one must consider that psychiatric hospitals in the USA typically emphasize pharmacotherapy while de-emphasizing the provision of evidence-based psychotherapeutic interventions (Glick, Sharfstein, & Schwartz, 2011; Mullen, 2009; Sharfstein, 2009; Walsh & Boyle, 2009). Thus, we interpret these findings as suggesting that inpatient treatment may be more stigmatizing for patients who already are apprehensive about medications, and who also believe in the value of psychotherapy for treating their depression. Alternatively, patients with more positive views about medications and less positive views about psychotherapy appear to have less stigmatization related to receiving hospital treatment. Furthermore, we found that negative views about medications, but not psychotherapy, predicted self-stigma about having depression. This suggests that beliefs about medication may be more important than beliefs about psychotherapy per se when attempting to understand and predict general self-stigma. Finally, depression severity predicted increased self-stigma about both receiving treatment and having depression in the current sample, which is consistent with previous research (Kanter et al., 2008; Pyne et al., 2004).
Overall, our results are consistent with the literature on self-stigma. For example, researchers have previously found that negative attitudes towards medications are associated with increased public and self-stigma (Conner et al., 2010; Wang, Fick, Adair, & Lai, 2007). Using the same measure of self-stigma as in the current study, Kanter et al. (2008) reported an association between prior antidepressant treatment but not psychotherapy and increased self-stigma. In addition, Pyne et al. (2004) found that being in treatment was associated with increased self-stigma. Previous studies conducted in non-US hospital patients show that individuals in psychiatric hospitals endorse more stigma than those in general hospitals (Chee et al., 2005; Verhaeghe et al., 2007); full hospitalization is more stigmatizing than partial hospitalization (Verhaeghe, Bracke, & Christiaens, 2008), and more personalized treatment on hospital units is associated with lower levels of stigma (Verhaeghe & Bracke, 2008). In addition, Rusch et al. (2009) found that increased self-stigma predicted psychiatric hospitalization.
Surveys show that depressed patients tend to prefer psychotherapy over medications for managing their depression (Prins et al., 2008; van Schaik et al., 2004). Research also demonstrates that treatment beliefs and preferences predict adherence and improvement in pharmacotherapy and psychotherapy (Gaudiano & Miller, 2006; Prins et al., 2008; Sotsky et al., 1991), as well as decreased treatment seeking (Barney et al., 2006; Prins et al., 2008; Rusch et al., 2009; Schomerus, Matschinger, & Angermeyer, 2009). Thus, the current findings suggest that patients with negative medication beliefs and an interest in psychotherapy for depression may be less inclined to seek current hospital treatment when needed. Alternatively, if patients in psychiatric hospitals were offered a more comprehensive approach in which they could receive medications and/or evidence-based psychotherapies based on their needs and preferences, this may help to reduce stigma for such patients and promote increased treatment seeking.
Limitations
Limitations to the current study should be considered. First, data were cross-sectional and thus cause/effect relationships cannot be clearly established. Also, the sample was predominantly white and non-Hispanic and results may not generalize to ethnic/minority patients. In fact, research suggests that ethnic/minority patients have increased stigma (Rusch, Kanter, Manos, & Weeks, 2008). Furthermore, our results may not generalize to outpatients with depression or patients who are not seeking treatment, or to hospitals outside the USA or hospitals where psychosocial interventions are emphasized more compared to medications. It also is important to consider that we utilized a newly validated self-stigma measure because it was specifically developed for patients with depression. Thus, results should be replicated using other established stigma measures.
An alternative explanation that we considered was that patients who held positive beliefs about psychotherapy had increased treatment self-stigma because they believed that they had more control over their condition but failed to change it, which resulted in hospitalization. However, we also found that negative medication beliefs were related to increased general self-stigma about depression, but psychotherapy beliefs were not. Also, previous research has shown that prior use of antidepressant medications is related to self-stigma whereas psychotherapy is not (Kanter et al., 2008). Future research should be conducted in other samples receiving various forms of treatment to investigate whether patients differ in their attitudes based on treatment type and setting.
Conclusion
The Institute of Medicine (2001) stresses the importance of taking patients’ needs and preferences into account when delivering care. Many patients are not being offered the best evidence-based psychotherapeutic treatment options in psychiatric hospitals today. The implications from the current study are that offering more comprehensive and evidence-based hospital programmes that include psychotherapy may help reduce self-stigma about treatment and encourage more patients to seek acute hospital care when indicated.
Footnotes
Acknowledgements
The authors have no conflicts of interest to declare. Preparation of this manuscript was supported in part by a grant (MH076937) from the National Institutes of Health awarded to Dr Gaudiano.