
Abstract
Background and aims:
There is a dearth of studies investigating the prevalence and factors associated with unmet needs in people with schizophrenia from low- and middle-income countries. We aimed to study prevalence and risk factors for unmet need.
Method:
A case-control study design was employed. One hundred and one (101) consecutive patients attending a psychiatric hospital were assessed using Camberwell Assessment of Need Short version (CANSAS) and Positive and Negative Syndrome Scale (PANSS). Multivariate analysis was employed to adjust for confounders.
Results:
The majority of patients had many unmet needs. These unmet needs were significantly associated with lower education, poverty and persistent psychopathology on multivariate analysis.
Conclusion:
Unmet needs are associated with poverty, lower education and persistent psychopathology. There is a need to manage unmet needs, in addition to addressing psychopathology and poverty.
Introduction
People with schizophrenia, with its chronicity and disability, are among the most socially and economically marginalized groups in the population. They have a complex mixture of clinical and social needs (Arvidsson, 2003; Holloway, 1994; Joska & Flisher, 2005; van der Krieke, Sytema, Wiersma, Tielen & van Hemert, 2011; Wiersma et al., 2009). Their needs can range from physical, psychological health, safety, an intimate relationship, family support, education, employment to good housing. These needs have to be met in order to enable the individual to achieve, maintain or restore an acceptable level of social independence and quality of life.
The assessment of need among people with mental illness is complex. It includes diverse areas of life including accommodation, food, looking after the home, self-care, daytime activities, physical health, psychotic symptoms, information, psychological distress, safety to self, safety to others, alcohol and substance use, company, an intimate relationship, sexual expression, childcare, education, telephone communication, transport, money and benefits. These needs are not specific to those with mental illness and also reflect the needs of the general population. Many people have multiple needs, which are satisfied to variable extents. The assessment of need is a crucial part of mental health assessment and should be routinely carried out in clinical practice. The Camberwell Assessment of Need (CAN), a family of questionnaires, systematically assesses a wide range of problems commonly experienced by people with severe mental illness (Phelan et al., 1995; Slade, Beck, Bindman, Thornicroft & Wright, 1999; Slade, Phelan, Thornicroft & Parkman, 1996; Slade, Thornicroft, Loftus, Phelan & Wykes, 1999; Slade, Loftus, Phelan, Thornicroft & Wykes, 1999). They can be used to assess the perceptions of the people with mental illness, their carers and mental health professionals. Many versions of the instrument are available including a clinical version (CAN-C), a research version (CAN-R), a short version (CANSAS), a version for use among older people (CANE) and among people with Developmental and Intellectual Disability (CANDID). Different aspects of these instruments have been evaluated in different populations (Andresen, Caputi & Oades, 2000; Kelly & Deane, 2011; McColl & Johnson, 2006; MacPherson, Gregory, Slade & Foy, 2007; MacPherson, Haynes, Summerfield, Foy & Slade, 2003; MacPherson, Varah, Summerfield, Foy & Slade, 2003; Salvi, Leese & Slade, 2005; Slade, Leese, Cahill, Thornicroft & Kuipers, 2005; Trauer, Tobias & Slade, 2008; van Vugt et al., 2011; van Vugt, Kroon, Delespaul & Mulder, 2012).
There is a dearth of studies on the needs of people with mental illness living in India (Kulhara et al., 2010). The assessment of need of people with mental illness is the essential first step in planning, developing and implementing mental health services that are sensitive to the local context and conditions. We aimed to study the needs of people with schizophrenia attending the Department of Psychiatry at the Christian Medical College, Vellore, India.
Method
Setting
The Department of Psychiatry, Christian Medical College, Vellore, is a tertiary referral centre, which treats people with a variety of mental and behavioural disorders. It employs a multidisciplinary and eclectic approach to management.
Participants
Consecutive patients, attending the hospital and meeting the following criteria were invited to participate in the study: (1) diagnosis of schizophrenia (WHO, 1992); (2) aged between 18 and 60 years; and (3) patients speaking Tamil, the local language. The exclusion criteria were: (1) florid nature of the psychosis precluding interview; (2) the presence of intellectual disability; and (3) severe hearing, visual and sensory impairment.
Assessments
The following instruments were employed:
Camberwell Assessment of Need Short Appraisal Schedule (CANSAS; Slade, Loftus et al., 1999; Slade, Phelan et al., 1996; Slade, Thornicroft et al., 1999). This instrument is considered the standard for the assessment of need in patients with mental illness. It has been used across regions and cultures. The instrument was translated and back-translated by bilingual health professionals into Tamil, the local language. A consensus version, keeping in mind conceptual, semantic and technical equivalence, was used for this study.
Positive and Negative Syndrome Scale (PANSS; Kay, Fiszbein & Opler, 1987). This scale assesses psychopathology in patients with schizophrenia and psychosis. It has also been employed in diverse regions and cultures.
Socio-demographic and clinical details. A specific pro forma was developed to collect this information.
Procedure
Consecutive patients were invited to take part in the study. Informed consent was obtained. The protocol was approved by the Institutional Review Board of the Christian Medical College, Vellore.
Analysis
Descriptive statistics, mean and standard deviation were calculated for continuous variables, while frequency distributions were obtained for categorical variables. The student t test and the χ 2 test were used to assess the significance of association for continuous and categorical variables, respectively. The median value was used to divide continuous variables into two groups. Multiple logistic regression was employed to adjust for confounders: age, gender and education. SPSS version 16 was used for analysis.
The Epi Info program version 6.1 was used to calculate the sample size. A sample size of 96 patients was required using the following assumptions: unmet needs in 50% of sample with an error of 10% and a confidence interval (CI) of 95%.
Results
Table 1 documents the socio-demographic and clinical characteristics of the sample. The majority were young, female, married, unemployed, literate, living in rural areas and in debt. The majority of subjects did not return to pre-morbid level of functioning and were not fully compliant with medication over the course of their illness. The median number of unmet needs was four, with a range of zero to 17.
Socio-demographic and clinical profile of the sample (N = 101).
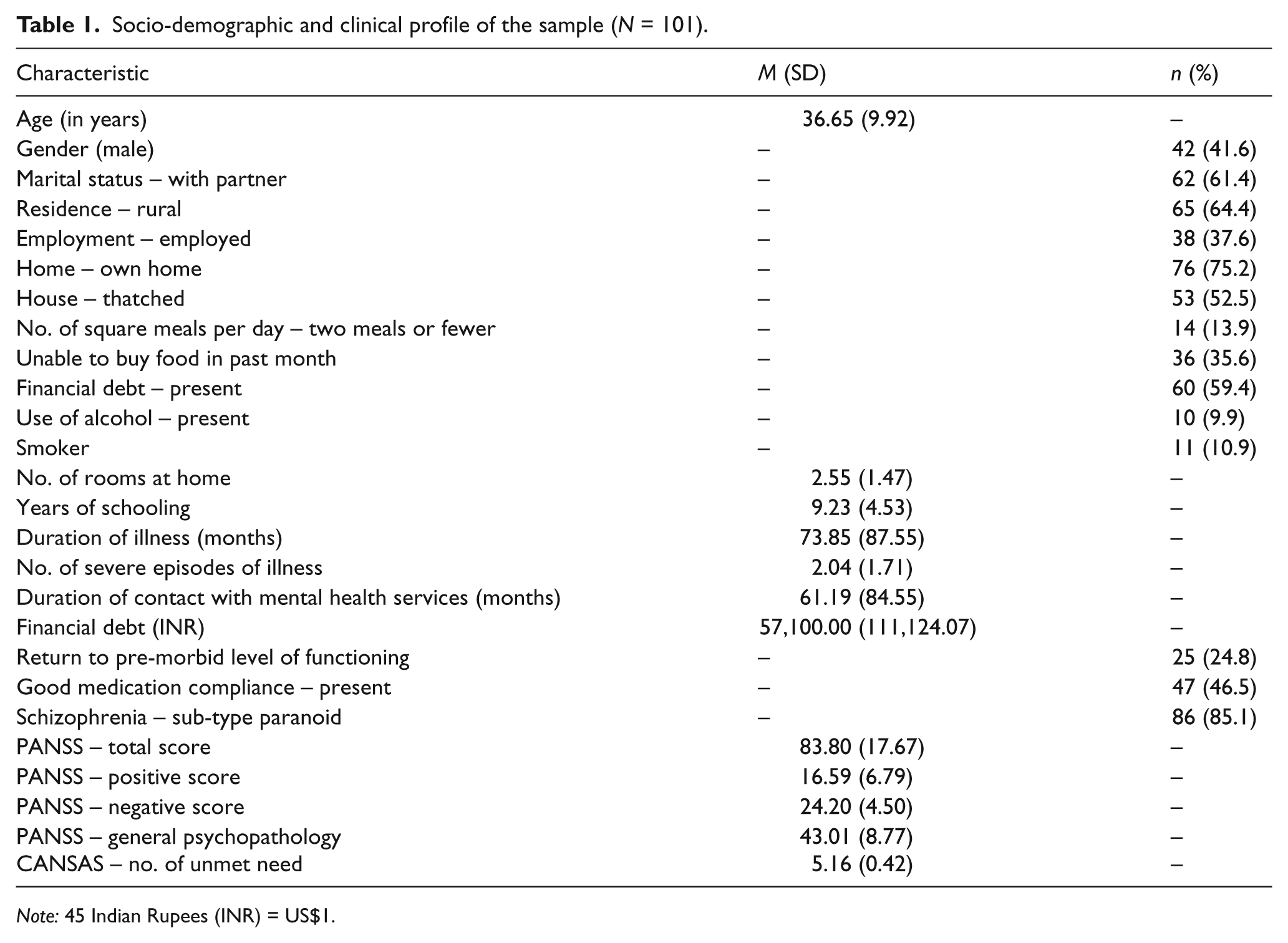
Note: 45 Indian Rupees (INR) = US$1.
Table 2 shows the comparison of subjects with high and low unmet needs on the different socio-demographic and clinical variables. Patients with high unmet needs were older, less educated and poorer (smaller house with thatched roofs and unable to buy food). Those with high unmet needs also had significantly higher scores on the total PANSS score and its subscales, had more number of episodes of illness, did not return to a pre-morbid level of functioning and had a non-paranoid psychosis.
Comparison of subjects with high and low unmet needs.
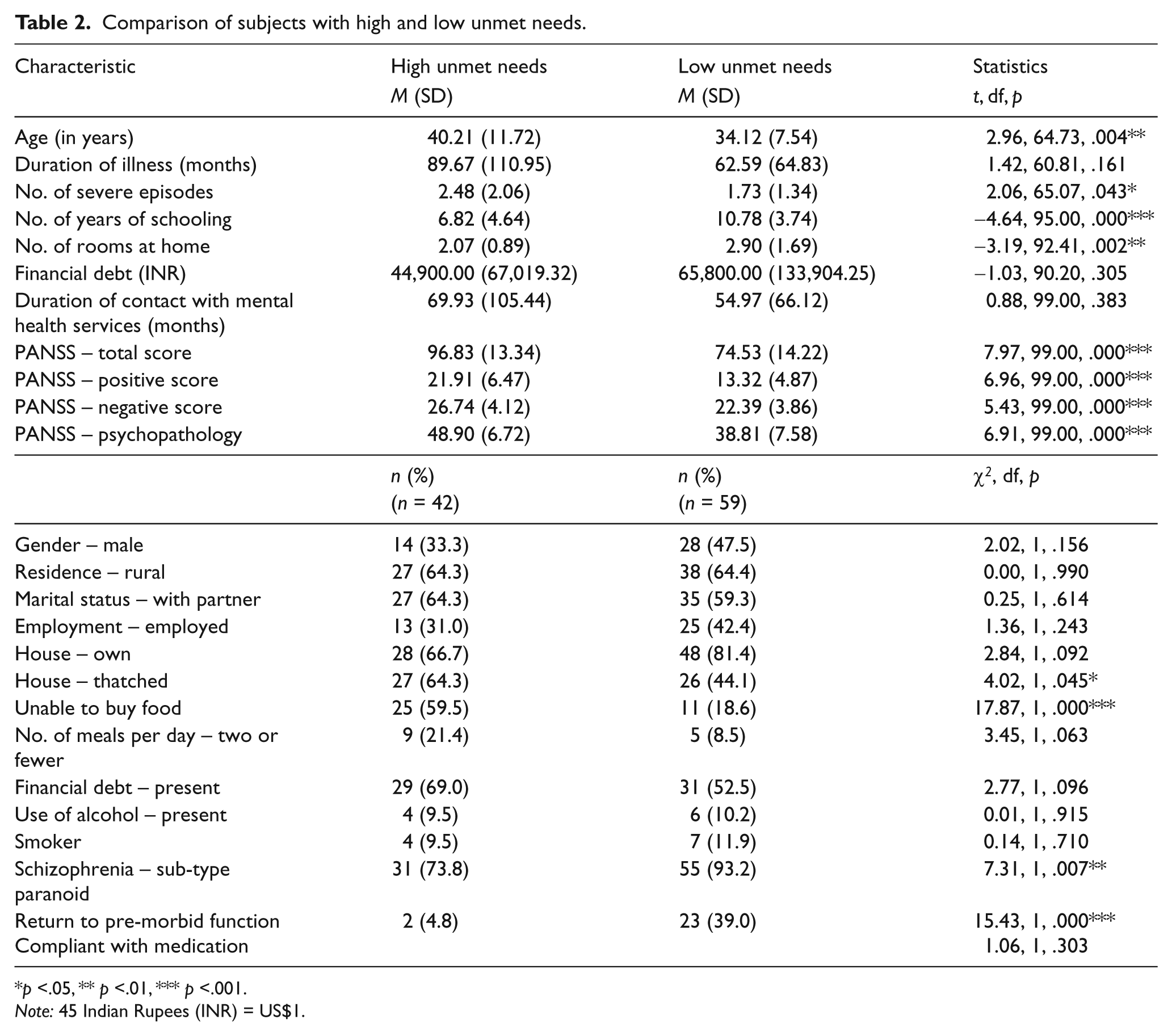
p <.05, ** p <.01, *** p <.001.
Note: 45 Indian Rupees (INR) = US$1.
The variables significantly associated with high unmet needs on bivariate analysis were adjusted for age, gender and education using logistic regression (Table 3). Unmet needs were significantly associated with lower education, measures of poverty and persistent psychopathology.
Factors associated with unmet need on multivariate analysis using logistic regression to adjust for age, gender and education.
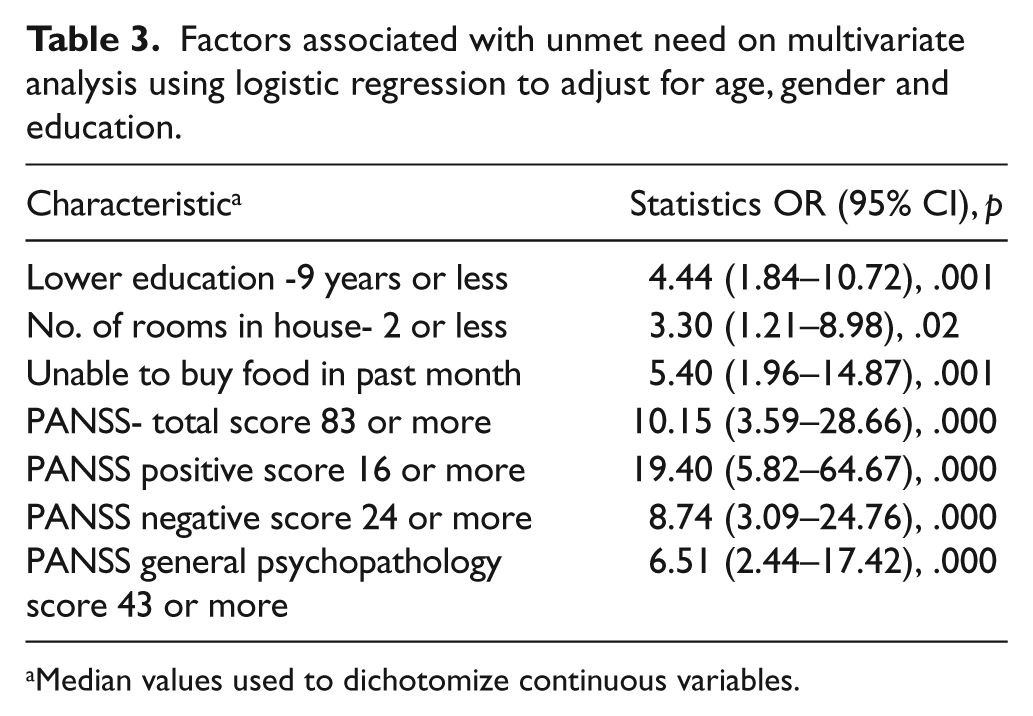
Median values used to dichotomize continuous variables.
The average met needs score was 6.70 (SD = 3.16). Bivariate analysis showed a statistically significant negative association with the following variables: PANSS total score (Pearson’s r = -0.53, p = .000); PANSS positive score (Pearson’s r = -0.42, p = .000); PANSS negative score (Pearson’s r = -0.42, p = .000); PANSS general psychopathology score (Pearson’s r = -0.53, p = .000); inability to buy food (t = -4.90, df = 99, p = .000); and debt (t = -2.23, df = 99, p = .028). There was a positive association with: return to a premorbid level of function (t = 3.75, df = 99, p = .000); living in a concrete house (t = 4.08, df = 99, p = .000); number of rooms at home (Pearson’s r = 0.35, p = .000); and years of schooling (Pearson’s r = 0.36, p = .000). Multiple linear regression analysis, using variables significant on bivariate procedures, documented a significant negative relationship between PANSS total score and met needs (B = -0.01, SE = 0.003, t = -3.83, p = .000), low education (B = -0.17, SE = 0.08, t = -2.14, p = .035) and small house (B = -0.28, SE = 0.088, t = -3.13, p = .002).
Discussion
This study systematically examined need in people with schizophrenia. Its strengths include the recruitment of consecutive patients, a relatively large sample and standard assessments. Its limitations include the fact that its case-control design precludes the evaluation of causality. The relationship between unmet needs and psychopathology is complex as unmet needs can be secondary to the illness and also impact the disease process. It would require a longitudinal cohort design to sort out the relationship between psychopathology and unmet needs in order to argue for the direction of causation.
The major findings of the study are that unmet needs are associated with lower education, measures of poverty and persistent psychopathology. Lower education and poverty are strongly associated with lower incomes in India and often result in many unmet needs. On the other hand, the direction of the relationship between persistent psychopathology and unmet needs will be difficult to disentangle in this study in view of the cross-sectional assessments involved. Poverty and persistent psychopathology have a bidirectional relationship in people with major mental illness. Persistent psychosis is often associated with unemployment and lowered income, resulting in unmet needs. Poverty results in unmet needs in addition to lowered access to treatment, poorer medication compliance and a worsening of the psychosis. Longitudinal studies using cohort designs will be required to establish the causal direction of such relationships.
The findings of the study are consistent with investigations done in other parts of the world. Persistent unmet needs are major lacunae in the management of people with schizophrenia. Physical and psychological health, safety, an intimate relationship, family support, education, employment, good housing, nutrition and education are basic human needs and consequently human rights. There is an urgent requirement to meet these needs so that people with major mental illnesses can achieve their full potential. The mental health delivery system, while focusing on medication and psychosocial management, should also facilitate the meeting of the basic needs of patients. Coordination with local government and rehabilitation schemes and personnel is crucial to empowering people with severe mental illness. The association between unmet need and persistent psychopathology demands a renewed focus on the needs of people with schizophrenia. There is a need to replicate the finding of this study using longitudinal designs in diverse populations in India and in other low- and middle-income countries. The identification of factors associated with unmet needs in people with schizophrenia and mental illness will allow for specific interventions targeting unmet needs and persistent psychopathology.
Footnotes
Funding
This study was funded by a grant from the Christian Medical College, Vellore.
Declaration of conflicting interest
The authors have no conflicts of interest to declare.