
Abstract
Background:
Physical comorbidities and substance use are commonly reported in patients with mental disorders.
Aim:
To examine somatic comorbidity in patients with substance use disorders (SUD) compared to patients with mental disorders but no SUD.
Methods:
Lifetime prevalence data on mental and physical health status were collected from inpatients in 12 mental health care facilities in five different countries. Differences in somatic comorbidity were examined by means of logistic regression analysis controlling for age and gender.
Results:
Of 2,338 patients, 447 (19%) had a primary or secondary SUD diagnosis. In comparison to patients with other mental disorders, patients with SUD had a higher prevalence of infectious and digestive diseases but a lower prevalence of endocrine, nutritional and metabolic disorders. Patterns of physical comorbidities differed according to type of substance used (alcohol use – cardiovascular; tobacco use – respiratory, neoplasms; cannabinoid use – injuries; opioid use – infectious, digestive; benzodiazepine use – endocrine, nutritional, metabolic; stimulants – urogenital).
Conclusions:
SUD are related to specific somatic health risks while some of our findings point to potentially protective effects. The widespread prescription of benzodiazepines requires research on physical health effects. Early detection of SUD and their integration into programmes targeting physical comorbidity should be a priority in organizing mental health care.
Keywords
Introduction
In patients using addictive substances, physical comorbidity is a common issue. Three types of problems – drug use, comorbid mental disorders and physical illness – interact unfavourably, thus requiring comprehensive health care programmes (Phelan, Stradins & Morrison, 2001). While many studies of comorbid physical conditions among people with mental illness have focused on schizophrenia (Leucht, Burkard, Henderson, Maj & Sartorius, 2007), excess physical morbidity and mortality have also been identified in other types of mental disorder, such as mental retardation, eating disorders, affective disorders and, in particular, substance use disorders (SUD) (Harris & Barraclough, 1998; Kilian, Becker, Krüger, Schmid & Frasch, 2006; Osborn, 2001).
In a meta-analysis of eight papers based on a total patient population of over 50,000, deaths from natural causes in people with psychiatric illness were reported to be twice as high as in the general population (Harris & Barraclough, 1998). Factors such as self-medication with psychotropic agents (e.g. increased smoking rates, insufficient physical health care and adverse effects of psychotropic medication) are considered to contribute to excess somatic morbidity and mortality (Kilian et al., 2006; Osborn, 2001).
Many research reports have dealt with the use of legal drugs (i.e. alcohol and tobacco), but much less has been published on patterns of physical comorbidity in people using illicit drugs, especially with regard to patients with mental disorders in inpatient psychiatric services. One review reported incidence rates for pneumonia, obstructive lung disease, hypertension, diabetes, chronic liver disease, peptic ulcer, stroke and sexually transmitted diseases including HIV to be more than doubled in persons with addiction problems as compared to matched controls (DeAlba, Samet & Saitz, 2004). Another study reported increased rates for heart disease, asthma, gastrointestinal disorders, skin infections and acute respiratory disorders among patients with SUD, and this finding was found to hold also in the absence of comorbid psychotic disorders (Dickey, Normand, Weiss, Drake & Azeni, 2002).
Alcohol consumption has been linked to injuries and diabetes, hypertension and coronary heart disease (Puddey, Rakic, Dimmitt & Beilin, 1999; Wadland & Ferenchick, 2004), and it is also related to cardiomyopathy and liver cirrhosis (Wadland & Ferenchick, 2004). Studies of the association of alcohol consumption with the metabolic syndrome have reported both protective and detrimental effects (Fan et al., 2008; Yoon, Oh, Baik, Park & Kim, 2004). Alcohol use increases the risk of cancer of the mouth, pharynx, larynx, oesophagus and liver as well as other cancers, liver cirrhosis, injuries and poisoning (Gutjahr, Gmel & Rehm, 2001; Longnecker & Enger, 1996). Review papers have concluded that tobacco smoking is associated with many chronic diseases (e.g. lung and other cancers, cardiovascular and chronic respiratory diseases, duodenal and gastric ulcers) with a high mortality risk (Wadland & Ferenchick, 2004). Cannabis use is associated with respiratory and cardiovascular health problems similar to those experienced by tobacco smokers (Ashton, 2001). Associations of marijuana use with sexually transmitted diseases, bronchitis and lung cancer, of cocaine use with pancreatitis, of hallucinogen use with tinnitus/sexually transmitted diseases and of inhalant use with tinnitus, sexually transmitted and infectious diseases were reported by the National Survey on Drug Use and Health in the US adult population (Han, Gfroerer & Colliver, 2010).
Skin and soft tissue infections as well as infectious diseases such as tuberculosis and viral hepatitis (Deiss, Rodwell & Garfein, 2009; Reimer et al., 2007) and cirrhosis (Wadland & Ferenchick, 2004) and HIV (Fischer et al., 2005; Rehm, Taylor & Room, 2006) are common among injection drug users, especially women (Brown & Ebright, 2002). There is little evidence on the somatic consequences of tranquilizer use. Luderer, Schulz & Mayer (1995) reported comorbid SUD (mostly alcohol) in 70% of tranquilizer users but did not investigate somatic conditions.
In patients with cocaine use, myocardial infarction, cardiomyopathy and other complications have been reported (Wadland & Ferenchick, 2004). Amphetamine users experience an excess incidence of acute coronary syndrome and cardiac arrhythmias, as well as (haemorrhagic and ischaemic) stroke, hyperthermia, rhabdomyolysis with acute renal failure and other complications due to vasoconstriction. Amphetamine inhalation can result in noncardiogenic edema (Wadland & Ferenchick, 2004).
Aim of the study
This study aims to examine the relationships between substance use and lifetime somatic comorbidity in inpatients of mental health care facilities in five countries.
Subjects and methods
Study sample
The study was part of a multi-site international collaboration to examine physical comorbidities. For this purpose, data on physical health status were collected from all patients consecutively admitted to inpatient care in 12 mental health care facilities in five countries (Denmark, Germany, Japan, Nigeria and Switzerland) over a period of one year (March 2004 to February 2005) who consented to participate in the study. All eligible patients admitted to psychiatric acute hospital care were assessed at admission and discharge according to the current WHO (2003) International Classification of Diseases (ICD-10). If hospitalized for periods longer than three months, the follow-up assessment was performed at three months post-admission.
Local ethics committee approval was obtained as appropriate in the respective study centres.
Assessment
Lifetime and current physical and mental health status of study participants were assessed on the basis of medical records and a physical examination according to a screening questionnaire that was developed for the study (Kilian et al., 2006). Detailed information about patients’ drug use habits regarding tobacco, alcohol, cannabis, opioids, central nervous system (CNS) stimulants and benzodiazepines was obtained from medical records and patient interviews. Laboratory tests and other medical procedures (clinical diagnostics, referrals to other medical disciplines) were performed according to routine clinical practice. All available sources of medical information (patient records, outpatient consultations, inpatient care episodes, conditions diagnosed during the current psychiatric treatment episode) were considered. Somatic diagnoses were established according to the current WHO International Classification of Diseases (ICD-10):
A00–A99 Certain infectious and parasitic diseases; C00–C48 Neoplasms; E00–E90 Endocrine, metabolic and nutritional diseases; G00–G99 Diseases of the nervous system; H00–H95 Diseases of the eye and the ear; I00–I99 Diseases of the circulatory system; J00–J99 Diseases of the respiratory system; K00–K93 Diseases of the digestive system; L00–L99 Diseases of the skin and subcutaneous tissue; M00–M99 Diseases of the musculoskeletal system and connective tissue; N00–N99 Diseases of the genitourinary system; S00–T98 Injury, poisoning and certain other consequences of external causes. (WHO, 2003)
Statistical analysis
Since the occurrence of a physical disorder is a binary outcome, the effects of SUD on the prevalence of physical comorbidity were examined by means of logistic regression analysis. In patients with SUD, the effects of the type of substance use on the prevalence of comorbid somatic conditions were examined by means of logistic regression analysis, including type of substance use, age, gender, country, psychiatric diagnosis and psychotropic drugs as explanatory variables. Robust variance estimation using the study centre as the cluster variable was applied to correct for bias due to the cluster structure of the sample. Logistic regression analysis was conducted with STATA 10 (Stata Corporation, 2007).
Results
In total, 2,338 patients were included in the study; 447 patients (19%) had a primary or secondary diagnosis of SUD (Table 1).
Patient sample, by country and diagnostic group.
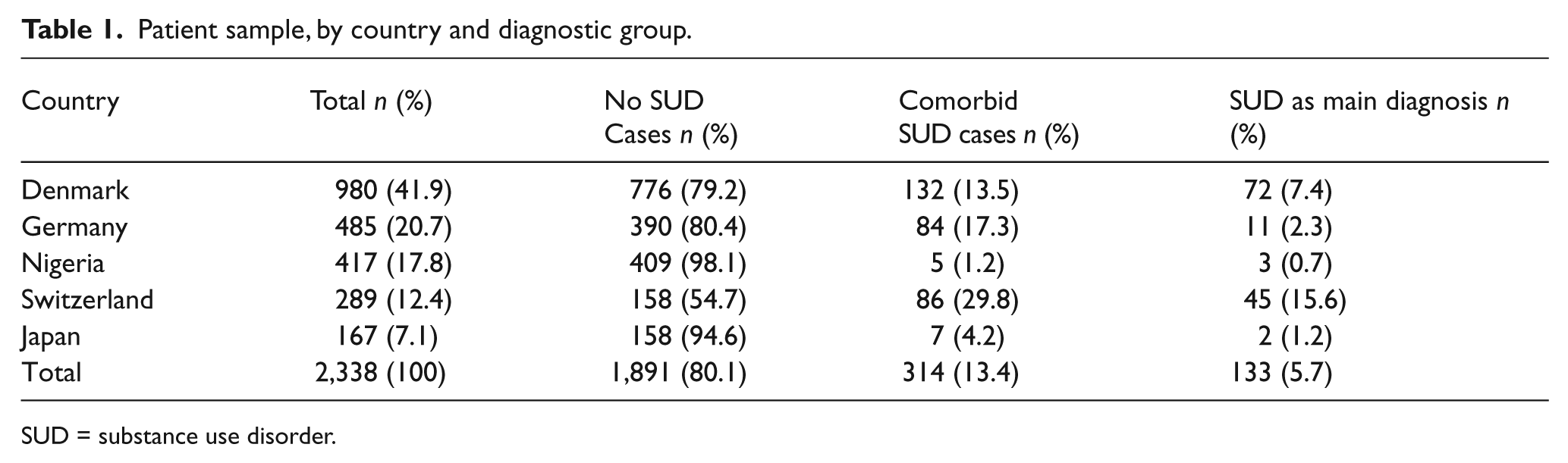
SUD = substance use disorder.
Table 2 shows prevalence rates of somatic disorders in patients with a SUD compared to those without SUD during the index episode.
Physical comorbidity in psychiatric patients with and without SUD.
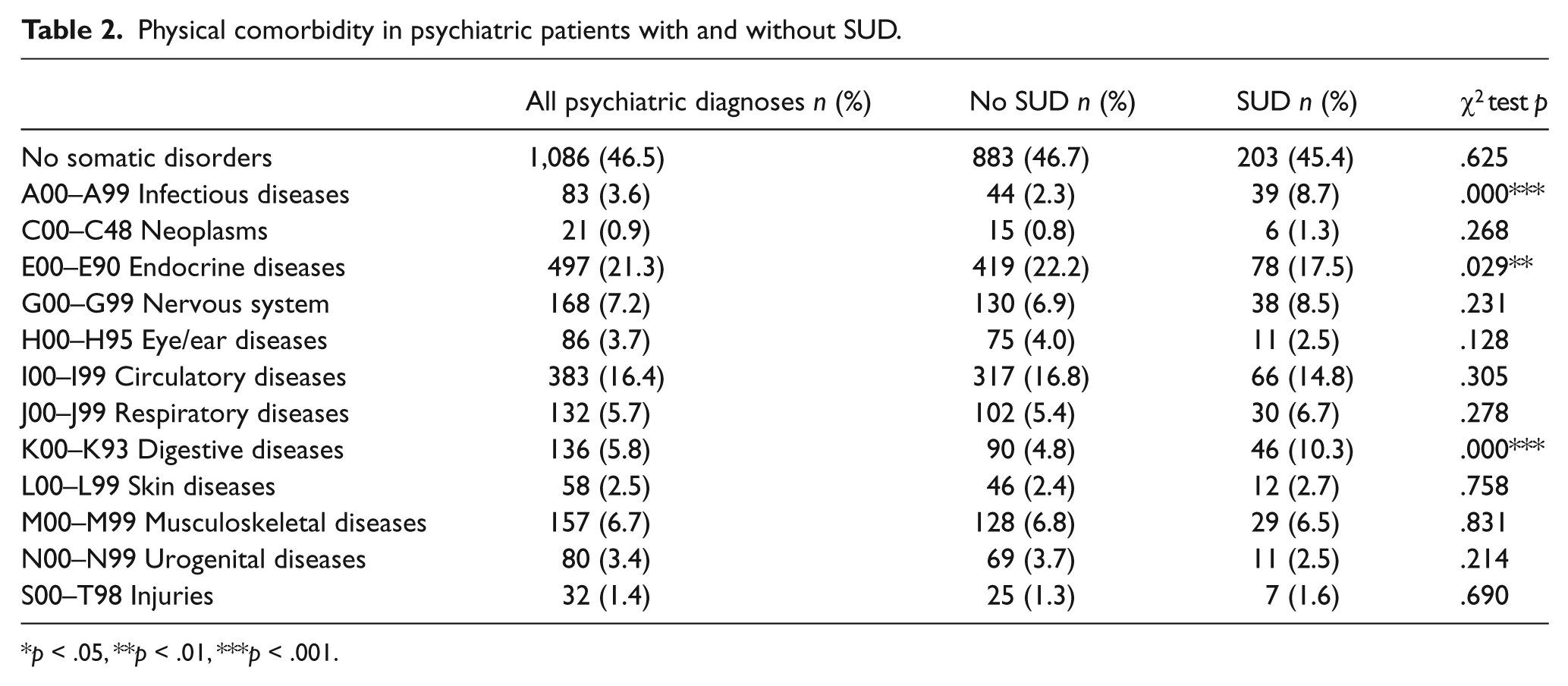
p < .05, **p < .01, ***p < .001.
In comparison with patients with other mental disorders (and no SUD), patients with SUD had a higher prevalence of infectious (p < .001) and digestive (p < .001) diseases, but a lower prevalence of endocrine, nutritional and metabolic disorders (p = .029).
Figure 1 shows that 370 (82.8%) of the study participants with SUD (N = 447) had a lifetime diagnosis of harmful alcohol use, 351 (78.5%) had a lifetime diagnosis of harmful tobacco use, 171 (38.3%) reported lifetime harmful use of cannabis, 105 (23.5%) had lifetime harmful opioid use, 165 (36.9%) reported benzodiazepine use, and 102 (22.8%) reported lifetime use of CNS-stimulant drugs.
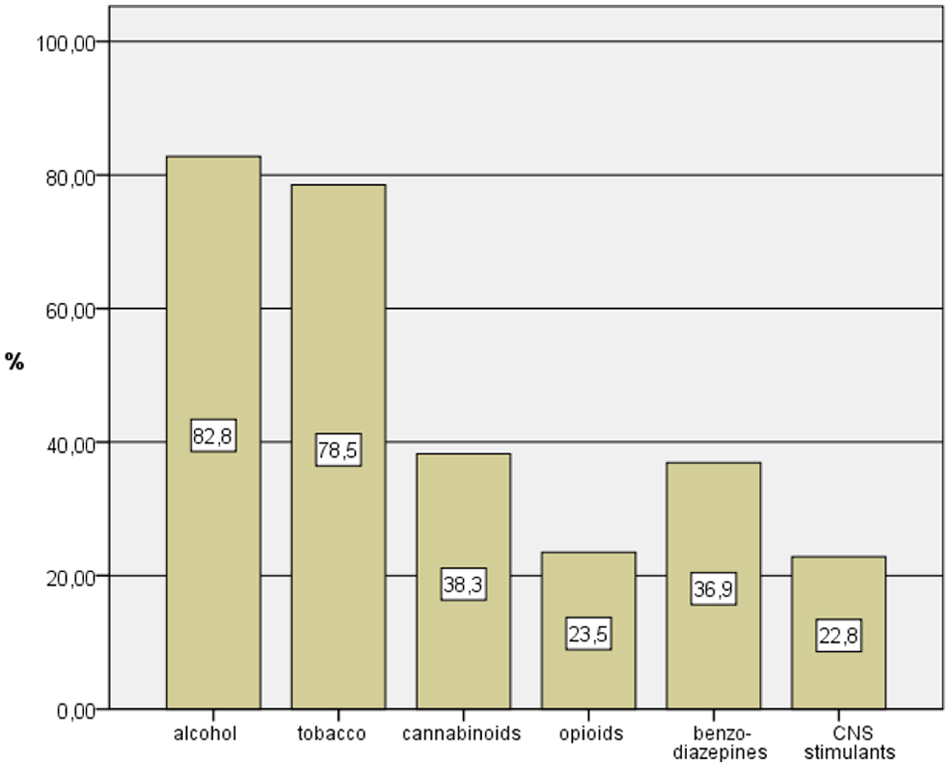
Psychoactive substance use by patients with substance use disorders (%); multiple answers permitted.
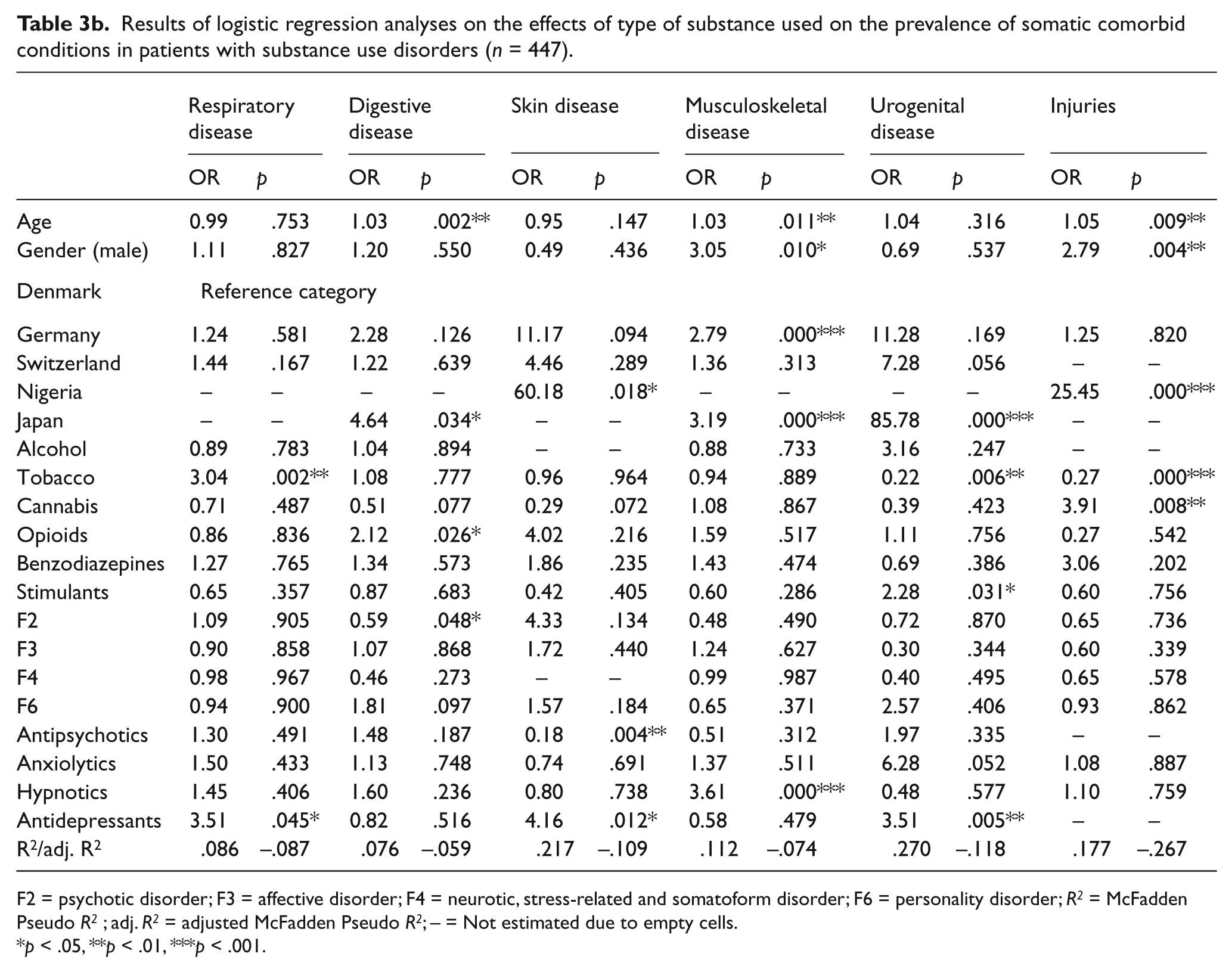
Table 3 shows the results of logistic regression analyses for the effects of type of substance used on the prevalence of a range of comorbid somatic disorders.
Results of logistic regression analyses on the effects of type of substance used on the prevalence of somatic comorbid conditions in patients with substance use disorders (n = 447).
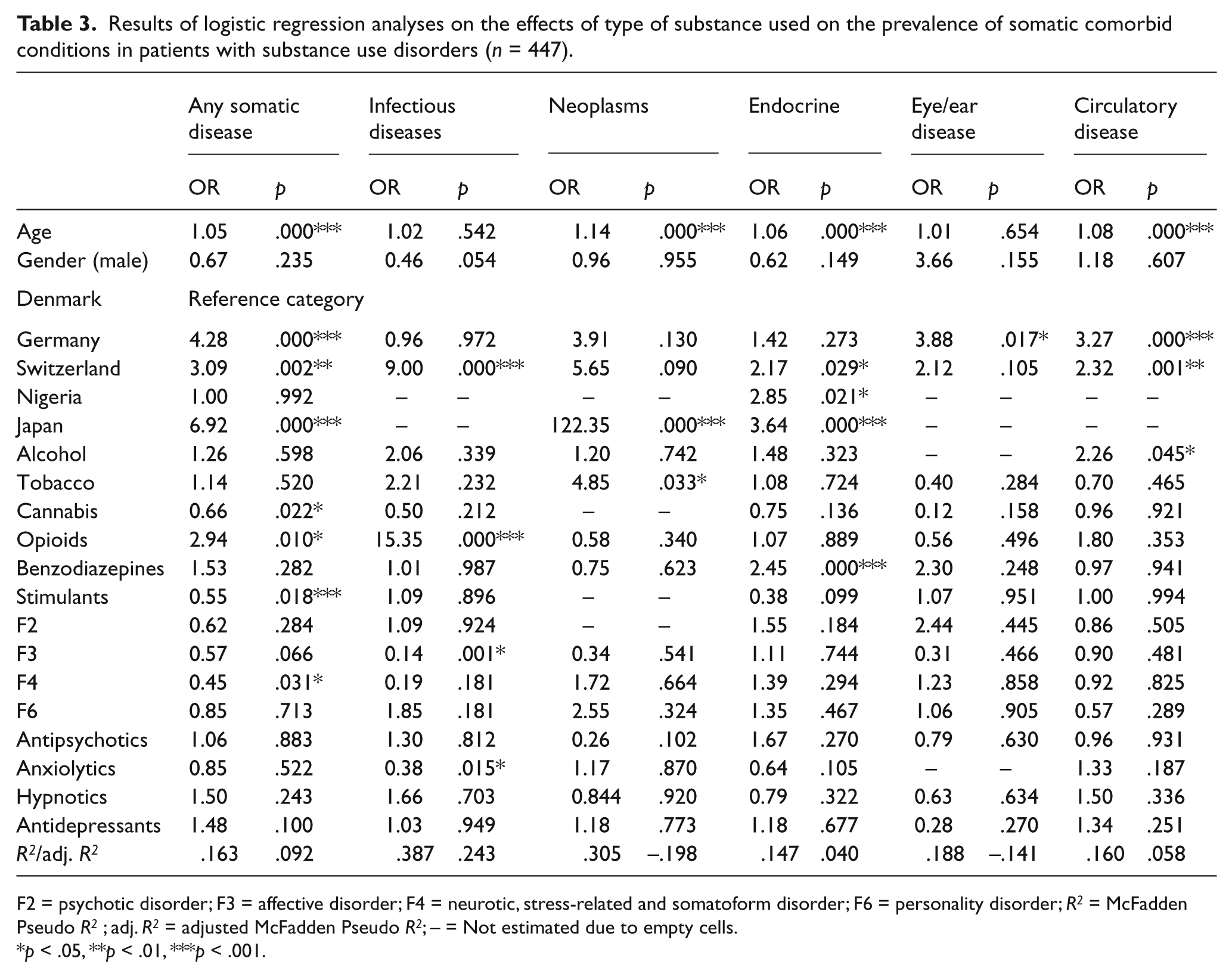
F2 = psychotic disorder; F3 = affective disorder; F4 = neurotic, stress-related and somatoform disorder; F6 = personality disorder; R 2 = McFadden Pseudo R 2 ; adj. R 2 = adjusted McFadden Pseudo R 2 ; – = Not estimated due to empty cells.
p < .05, **p < .01, ***p < .001.
Results of logistic regression analyses on the effects of type of substance used on the prevalence of somatic comorbid conditions in patients with substance use disorders (n = 447).
F2 = psychotic disorder; F3 = affective disorder; F4 = neurotic, stress-related and somatoform disorder; F6 = personality disorder; R 2 = McFadden Pseudo R 2 ; adj. R 2 = adjusted McFadden Pseudo R 2 ; – = Not estimated due to empty cells.
p < .05, **p < .01, ***p < .001.
The risk of any type of somatic comorbidity increased with increasing age (OR = 1.05, p = .000) and was higher for patients from Germany (OR = 4.28, p = .000), Switzerland (OR = 3.09, p = .002) and Japan (OR = 6.92, p = .000) in comparison to those from Denmark. The risk of having at least one somatic disease was higher for patients who reported opioid use (OR = 2.94, p = .010) but lower for those who reported cannabis use (OR = 0.66, p = .022) or the use of CNS-stimulant drugs (OR = 0.55, p = .018). The risk of having any somatic disease was also lower in patients with an ICD-10 F4 diagnosis (OR = 0.45, p = .031). While the pseudo R 2 for the model indicates that about 16% of the variance in risk of having any physical disorder could be explained by the model, the adjusted pseudo R 2 of 0.920 points to the fact that most of the variance is explained by non-significant effects.
The risk of infectious diseases was higher for patients from Switzerland in comparison to those from Denmark (OR = 9.00, p = .000). Patients who reported opioid use had a 15-fold higher risk of having an infectious disease than those who did not report opioid use (OR = 15.35, p = .000). Patients with a diagnosis of an affective disorder (OR = 0.14, p = .001) and patients who were treated with anxiolytic drugs (OR = 0.38, p = .015) had a lower risk in comparison to patients without these characteristics. Again, the pseudo R 2 of 0.387 suggests a very good model fit, but after adjustment it drops to 0.243.
The prevalence of cancer increased with increasing age (OR = 1.14, p =.000). In comparison to patients from Denmark, patients from Japan had a 122-fold higher risk of having cancer (OR = 122.35, p = .000). People who reported tobacco use had a fivefold risk of having cancer (OR = 4.85, p = .033) than those who did not report tobacco use. The pseudo R 2 of 0.305 suggests a good model fit, but, after adjustment, it decreases to -0.198, indicating that most of the model variables contribute nothing to the explanation of the variance in cancer prevalence.
With increasing age, patients had a higher risk of endocrine disease (OR = 1.06, p = .000). Patients from Switzerland (OR = 2.17, p = .029), Nigeria (OR = 2.85, p = .021) and Japan (OR = 3.64, p = .000) had a higher risk of having an endocrine disease than those from Denmark. Patients who reported benzodiazepine use had a higher risk of endocrine, metabolic and nutritional diseases (OR = 2.45, p = .000). As indicated by the adjusted pseudo R 2 , the model explains about 4% of the variance in the risk of having an endocrine disease.
In comparison to patients from Denmark, patients from Germany had a higher risk of having an eye or ear disease (OR = 3.88, p = .17). No other significant effects of model variables on the prevalence of eye/ear diseases were identified. Again, the negative adjusted pseudo R 2 indicates that the model variables do not contribute to explaining the variance in eye/ear disease prevalence.
The risk of cardiovascular disease increased with age (OR = 1.08, p = .000) and patients from Germany (OR = 3.27, p = .000) and Switzerland (OR = 2.32, p = .001) were at higher risk of cardiovascular disease than patients from Denmark. Alcohol use was related to an increased risk of cardiovascular disease (OR = 2.26, p = .045). The pseudo R 2 indicates that 16% of the variance in the risk of having a cardiovascular disorder was explained by the model but again, the decrease of the adjusted pseudo R 2 to 0.058 suggests that only a few of the model variables make a substantial contribution to the explanation of the variance.
The risk of respiratory diseases was found to be increased in patients who reported tobacco use (OR = 3.04, p = .002) and for patients who were treated with antidepressants (OR = 3.51, p = .045). The negative adjusted pseudo R 2 indicates that the model does not fit the data well.
The risk of having a digestive system disease increased with age (OR = 1.03, p = .002). In comparison to patients from Denmark, diseases of the digestive system were more prevalent in patients from Japan (OR = 4.64, p = .034). Patients who reported the use of opioids had a higher risk (OR = 2.12, p = .026) of digestive disease, while patients with a diagnosis of schizophrenia had a decreased risk (OR = 0.59, p = .048). The model accounts for about 8% of the variance in digestive system disease prevalence, but the negative adjusted pseudo R 2 indicates that the model does not fit the data well.
Patients from Nigeria, compared to Danish patients, had a 60-fold risk of skin disease (OR = 60.18, p = .018). While the prevalence of skin disease was decreased in patients who were treated with antipsychotics (OR = 0.018, p = .004), it was higher in patients who were treated with antidepressants (OR = 4.16, p = .012). About 22% of the variance in the prevalence of skin diseases could be explained by the model; however, the fact that most of the model variables have no significant effect is reflected by the negative adjusted pseudo R 2 .
The prevalence of musculoskeletal diseases increased with age (OR = 1.03, p = .011) and was higher in male patients (OR = 3.05, p = .020) than in females. In comparison to patients from Denmark, German (OR = 2.79, p = .000) and Japanese (OR = 3.19, p = .000) patients had a higher risk of having a musculoskeletal disease. The risk of having a musculoskeletal disease was increased in patients who were treated with hypnotic drugs (OR 3.61, p = .000). Due to the fact that most of the model variables have no significant effect, the adjusted pseudo R 2 is negative.
In Japanese patients, compared to Danish, urogenital diseases were more prevalent (OR = 85.78, p = .000). While the use of tobacco was related to a lower risk of urogenital disease (OR = 0.22, p = .006), the risk was increased in patients who reported use of CNS-stimulant drugs (OR = 2.228, p = .031). Patients who were treated with antidepressants had a higher risk of having a urogenital disease than those who did not receive antidepressant medication (OR = 3.51, p = .005). As indicated by the pseudo R 2 , the model explains about 27% of the variance in the risk of urogenital diseases but again, the pseudo R 2 is negative, reflecting the fact that most model variables have no significant effect.
The prevalence of injuries increased with age (OR = 1.05, p = .009), and injuries were more frequent among male patients (OR = 2.79, p = .004). Patients from Nigeria had a higher risk of having an injury than those from Denmark (OR = 25.45, p = .000). While patients who reported use of cannabis had a higher risk of injury (OR = 3.91, p = .008), this risk was lower in those with tobacco use (OR = 0.27, p = .000). About 18% of the variance in the prevalence of injuries was explained by the model but, again, the pseudo R 2 is negative, reflecting the fact that most model variables have no significant effect.
Discussion
This study included 2,338 patients admitted to inpatient psychiatric services in five countries.
A subgroup of 19% of all patients (n = 447) had a primary or secondary diagnosis of SUD. In the overall SUD group there was a higher likelihood of infectious diseases than in the non-SUD group that was attributable to opioid users, most likely due to injection use (Brown & Ebright, 2002). Furthermore, there was a higher risk of SUD patients suffering from digestive disorders, which could be due to unhealthy dietary behaviour among people with SUD (Kilian et al., 2006). Prevalence of endocrine, nutritional and metabolic disorders was higher in the non-SUD patient group. As expected, age was associated with a higher risk of several types of somatic disorder. Male patients had more injuries and musculoskeletal problems, which may be related to risk-taking lifestyles.
Numbers of SUD patients showed substantial variance between study centres, and only small patient numbers were included in the Japanese and Nigerian study site. Nevertheless, the effects of country dummy variables indicate that, in comparison to Danish patients, the prevalence of most physical diseases was higher in patients from Germany, Switzerland and Japan. As physical comorbidity was ascertained on the basis of medical records, we do not know whether differences in physical disease prevalence data reflect true differences or variation in the quality of physical examination or diagnostic routine procedures. In addition, patient selection might have differed across the sites. That is why site differences could reflect differences in setting and not necessarily causal effects.
In concordance with findings from other studies (e.g. Puddey et al., 1999; Wadland & Ferenchick, 2004), alcohol-related disorders were associated with cardiovascular diseases, tobacco smoking was linked to respiratory disorders and neoplasms (Wadland & Ferenchick, 2004), and opioid users had a higher risk of being diagnosed with infectious and digestive diseases (Deiss et al., 2009; Reimer et al., 2007). Tobacco smokers were at a lower risk of being diagnosed with urological disorders and injuries, which could point to potentially protective effects regarding some medical comorbidities. Cannabinoid users had a significantly higher risk of injury, which is in line with findings from a French study (Mura et al., 2003). In contrast, Gmel, Kuendig, Rehm, Schreyer and Daeppen (2009) found an inverse relation of cannabis use with risk of injury. Interestingly, cannabinoid users were less frequently diagnosed with any type of somatic disorder. This could be related to a lower BMI in this patient group. Reduced relative risk has been reported for cannabinoid users with regard to multiple sclerosis and neurodegenerative disorders (Malfitano, Matarese & Bifulco, 2005; Sarne & Mechuolam, 2005). However, unknown confounders and low case numbers need to be borne in mind.
Benzodiazepine users were more frequently diagnosed with endocrine, nutritional and metabolic disorders, which to the best of our knowledge is a new finding. These associations could have been due to confounding variables not considered in this study (e.g. patient factors, comorbid diseases, health behaviour, other medication, dietary and exercise habits). In view of the widespread prescription of benzodiazepines, there is an urgent need for studies on the effects of tranquilizer use on physical health status. The association of CNS-stimulant use with urological disorders should be considered with similar caution (e.g. potential urotoxicity of psychoactive drugs or their metabolites and potential sexual behaviour risk factors need to be considered). Antidepressant medication was associated with respiratory, skin and urogenital diseases, and hypnotic drug intake with musculoskeletal diseases. Since these associations are not easily accounted for by established side-effect profiles, they might be due to selection processes.
Limitations
Limitations result from large differences in sample sizes and in rates of patients with SUD across the study sites. Also, there was a lack of information on the frequency and intensity of past and current substance use. Since the prevalence of cancer was low in the total sample, the effects of substance use could not be estimated for all substances due to empty cells in the analysis. Assuming that SUD patients admitted to inpatient psychiatric care are a subgroup in current crisis with an unfavourable course of disease, somatic comorbidity findings in this study may not be representative of all SUD patients, and somatic comorbidity could have been overestimated. As indicated by pseudo R 2 values, the proportion of explained variance varies from 8% for digestive diseases to 39% for infectious diseases. However, in all models, the number of significant effects is small, as reflected by small adjusted pseudo R 2 values. A substantial proportion of variance might be explained by non-significant effects. Thus, there is evidence that case numbers, in this study, were too small to identify relevant effects. Further studies with larger samples are required in order to improve our understanding of variations in the physical comorbidity of SUD patients.
Conclusion
In summary, the current study found SUD to be related to an increased risk of infectious and digestive system disorders (such as diseases of the oral cavity, oesophagus, stomach and bowel, liver and pancreas). In addition, the use of particular psychoactive substances was found to be related to specific somatic health risks. This suggests that SUD patients need both differentiated somatic follow-up procedures and adequate treatment, for example smoking-cessation group therapy with or without nicotine replacement, which has proven efficacy (Osborn, 2001). Also, high mental health care dropout rates of SUD patients call for the implementation of intelligent follow-up systems to ensure that continuous outpatient care is provided (Masaki & Toyomaso, 2010; Phelan, Stradins & Morrison, 2001). Integrating SUD components in programmes targeting physical comorbidity is a priority issue in organizing mental health care (Dickey et al., 2002).
Footnotes
Acknowledgements
Thanks to all the patients and data collectors for supporting our research. We also would like to thank Eli Lilly for an unconditional grant for this study. Karel Frasch has received travel payments/speaker honoraria from AstraZeneca (presentation of results from this study), Janssen, Bristol-Myers Squibb, Pfizer and Lilly. He furthermore holds shares in the pharmaceutical company Stada. Jens Ivar Larsen reports consultant work for Bristol-Myers Squibb, AstraZeneca and Eli Lilly (none related to this study), as well as travel expenses from Wyeth Pharmaceuticals to present results from this study. Christoph Lauber received unrestricted grants from Eli Lilly, Janssen and AstraZeneca (none related to this study). Povl Munk-Jørgensen receives unconditional educational grants from Servier, Janssen-Cilag, Bristol-Myers Squibb and AstraZeneca (none related to this study). Thomas Becker reports research funding to the department (unrestricted research grants) from AstraZeneca (Wedel, Germany), GlaxoSmithKline (Munich, Germany), Pfizer (Karlsruhe) and Affectis Pharmaceuticals AG (Martinsried, Germany) for clinical trials and investigator-initiated trials (none related to this study). All other authors declare that they do not have any conflict of interest.