
Abstract
Aim:
The study explored the socio-demographic, clinical and legal profile of forensic psychiatric inpatients in an attempt to improve the existing mental health services for prisoners within the prison and in psychiatric hospitals.
Methodology:
A chart review of 135 forensic psychiatric inpatients admitted between January 2005 and December 2009 was done. A structured data-extraction tool was used for data collection and a descriptive approach for analyses.
Results:
Subjects were referred either directly from prison (62.2%) or from court (37.8%) for diagnosis, treatment or certification. References to the Mental Health Act 1987, charges and inclusion of first investigation report and behavioural observation report was lacking in most. The majority of prisoners (85.7%) were under trial, murder being the most common charge. Psychiatric diagnosis was made in 90.3%, the most common being psychosis. Substance use (nicotine, alcohol, cannabis) and high-risk behaviours were also common.
Conclusion:
There is a need to streamline the procedure of referral and to sensitize the referral authorities about the Mental Health Act and mental illnesses, and the need to enclose first investigation reports and behavioural observation reports. De-addiction services and facilities need to be established within prison premises so that the inmates get the benefit of treatment at the earliest opportunity.
Keywords
Introduction
India has relatively low imprisonment rates. Worldwide, imprisonment per 10,000 population ranges from as low as 30 in India to as high as 750 in the USA (Wilper et al., 2009). Internationally, psychiatric morbidity is substantially higher in prison inmates than in the general population (Coid et al., 2003; Kjelsberg et al., 2006). Therefore, it is reasonable to assume that psychiatric morbidity in Indian prisons is much greater than that seen in the general population where the prevalence rate ranges from 9.5 to 370 per 1,000 population (Math, Chandrashekar, & Bhugra, 2007). It is largely unclear how well prison services are addressing these problems (Fazel & Danesh, 2002) given that treatment facilities, availability of psychiatrists (Coid, et al., 2003) and knowledge among prison officials about mental illness are often inadequate in developing countries (Math, Murthy, Parthasarathy, Kumar, & Madhusudhan, 2011).
There were 1,336 prisons with a capacity of 263,911 inmates in India as of 2006, but the existing total number of inmates on 31 December 2006 was 373,271 (National Crime Records Bureau, 2006). The most common factors that have negative effects on the mental health of prisoners are overcrowding, various forms of violence, enforced solitude or lack of privacy, lack of meaningful activity, isolation from social networks, insecurity about future prospects (work, relationships, etc.), and inadequate health services, especially mental health services, in prisons (Math, Murthy, Parthasarathy, Kumar, & Madhusudhan, 2011). The increased risk of suicide in prisons (often related to depression and adjustment disorder) is, unfortunately, one common manifestation of the cumulative effects of these factors. However, not all these prisoners are admitted to hospital. Reasons for transferring prisoners to psychiatric hospitals include diagnosis and treatment of behavioural problems including violence and suicidality, substance use, certification regarding fitness to stand trial, observation to assess presence or absence of psychiatric illness, review of existing psychiatric medications and insanity defence (Math, Murthy, Parthasarathy, Kumar, & Madhusudhan, 2011; World Health Organization, 2005).
Of the many laws enacted in relation to mental health in India, the most important legal provision is the Mental Health Act (MHA) 1987. This is the most modern version of the Indian Lunacy Act (ILA) of 1912. Its section 27 provides provision for admission, detention and treatment of mentally ill prisoners. Apart from treatment, courts may also request for various certifications. This includes: (1) certifying the presence or absence of psychiatric illness if the defendant claims for an insanity plea; (2) assessment of fitness to stand trial in cases where mental illness incapacitates cognitive, emotional and behavioural faculties of an individual causing serious impact on the ability to defend the case. If deemed unfit, the trial is usually postponed and the person is again sent for treatment to regain competence.
The Indian Penal Code (section 84, 1860) is a prototype of its British equivalent, the McNaughton’s Rule. This section has formulated the legal test for insanity defence, which states: Nothing is an offence, which is done by a person, who at the time of doing it by reason of unsoundness of mind, is incapable of knowing the nature of the act or that, what he is doing is either wrong or contrary to the law.
The basic difference is that unlike in McNaughton’s Rule where guilt is admitted but the accused is exonerated for reason of unsoundness of mind, here no offence is admitted if the offender is of unsound mind.
In western countries, several retrospective studies have been conducted on forensic psychiatric inpatients. The clinical and forensic profiles of these patients were studied and it was found that the main psychiatric diagnoses included: schizophrenia and other functional psychoses; affective disorders including depression and mania; personality disorders; substance use and mental handicap. The type of offences ranged from murder, sexual offences and arson, to driving under the influence of alcohol (MacCall, White, & Smith, 2005; O’Connor & O’Neill, 1990).
The only Indian study was done in 1970 by Kishore et al. and was an analysis of the case records of 380 criminal mental patients admitted to a mental hospital at Amritsar (Kishore, Verma, & Shah, 1970). The current study undertaken over four decades later attempts to probe into the current profile of forensic psychiatric inpatients including socio-demographic, psychiatric, medical and legal characteristics and high-risk behaviours, with an attempt to improve the existing mental health services for prisoners in psychiatric hospitals.
Methodology
A retrospective study design was employed by reviewing inpatient charts. A structured data-extraction tool was used for data collection from the chart and a descriptive approach was used towards analyses. Forensic psychiatric inpatients were operationally defined as patients admitted to the forensic psychiatric ward of the institution for treatment, observation, certification to stand for trial and insanity defence.
The study was carried out at the National Institute of Mental Health and Neurosciences (NIMHANS), Bangalore, India. This is a tertiary care centre with research, academic and training facilities. The male forensic psychiatric ward in NIMHANS is a part of the male closed ward. There is no forensic psychiatry ward for women in the institute. The forensic psychiatric inpatients receive care from a multidisciplinary team consisting of forensic psychiatrists, nurses, clinical psychologists and psychiatric social workers. Each patient is evaluated by a postgraduate junior resident using the structured NIMHANS Detailed Workup Proforma for Forensic Psychiatry Patients (NDPFPP) (see Chart-1), following which the case is discussed with the senior resident (lecturer) and findings are documented. In addition, ward behaviour of each patient is documented every day using the NIMHANS Behavioural Observation Report (NBOR) (see Chart-2). Finally, the case is presented in a multidisciplinary grand round, held once every week, consisting of two forensic psychiatry consultants, and consultants from clinical psychology, psychiatric social work, psychiatric nursing and students from the respective departments. This multidisciplinary team is responsible for assessment, diagnosis, management and providing legal opinion to the judiciary. Ward observation reporting (see Chart-2) and serial mental status examinations are done on a daily basis. The documentation of the forensic psychiatric chart is meticulous and monitored by a senior resident and two forensic psychiatry consultants.

Charts of all patients admitted in NIMHANS from January 2005 to December 2009 in the male forensic psychiatric ward were reviewed for the current study. A year-wise list of names and inpatient numbers of patients who were admitted to the forensic psychiatric ward was made as per the admission register maintained in the forensic ward. This was counter-checked with the psychiatric inpatients admission register maintained in the Medical Records Department.
During the five-year study period, there were a total of 20,887 psychiatry admissions, out of which 138 were in the forensic psychiatry ward, 135 of whose files could be retrieved. (Three files were submitted to the court and could not be retrieved owing to the complexity of the case involved.) An average of 60 to 90 minutes was needed to extract data from each case file. In case of doubt, consensus of the consultants was sought.
Development of research tool
In the absence of a standardized tool for the extraction of the necessary details from the case files, it was decided to develop one. The tool was developed on the basis of a review of relevant literature (books, journal articles and other published studies) and suggestions obtained from experts in forensic psychiatry, adult psychiatry, clinical psychology, psychiatric nursing and psychiatric social work. The research tool included a socio-demographic data schedule and a forensic data-extraction schedule. The items in the schedules were finalized after a pilot study that was also conducted in NIMHANS using 20 case files of forensic psychiatric inpatients admitted before 2005. The files were selected by simple random sampling, for which permission was obtained from the Medical Records Division officer. Content validity was tested by eight experts in the field of psychiatry, psychiatric social work, psychiatric nursing and biostatistics, prior to the pilot study.
The socio-demographic data schedule was used to extract socio-demographic details including age, marital status, religion, state, residence, educational status and occupation.
The forensic data extraction schedule covered four dimensions: legal variables; mental health clinical variables; general medical condition clinical variables; and high-risk behaviour variables. There were a total of 55 variables: 10 under legal issues; 17 under mental health; 21 under general medical condition; and 7 under high-risk behaviour.
To describe the characteristics of forensic psychiatric inpatients, the data were used to derive descriptive statistics including parametric statistics such as mean and standard deviation where appropriate.
The study was approved by the ethical committee of NIMHANS. Personal information related to patients available in the case files has not been shared with anyone. All the obtained information has been used solely for the purpose of research.
Results
Socio-demographic characteristics
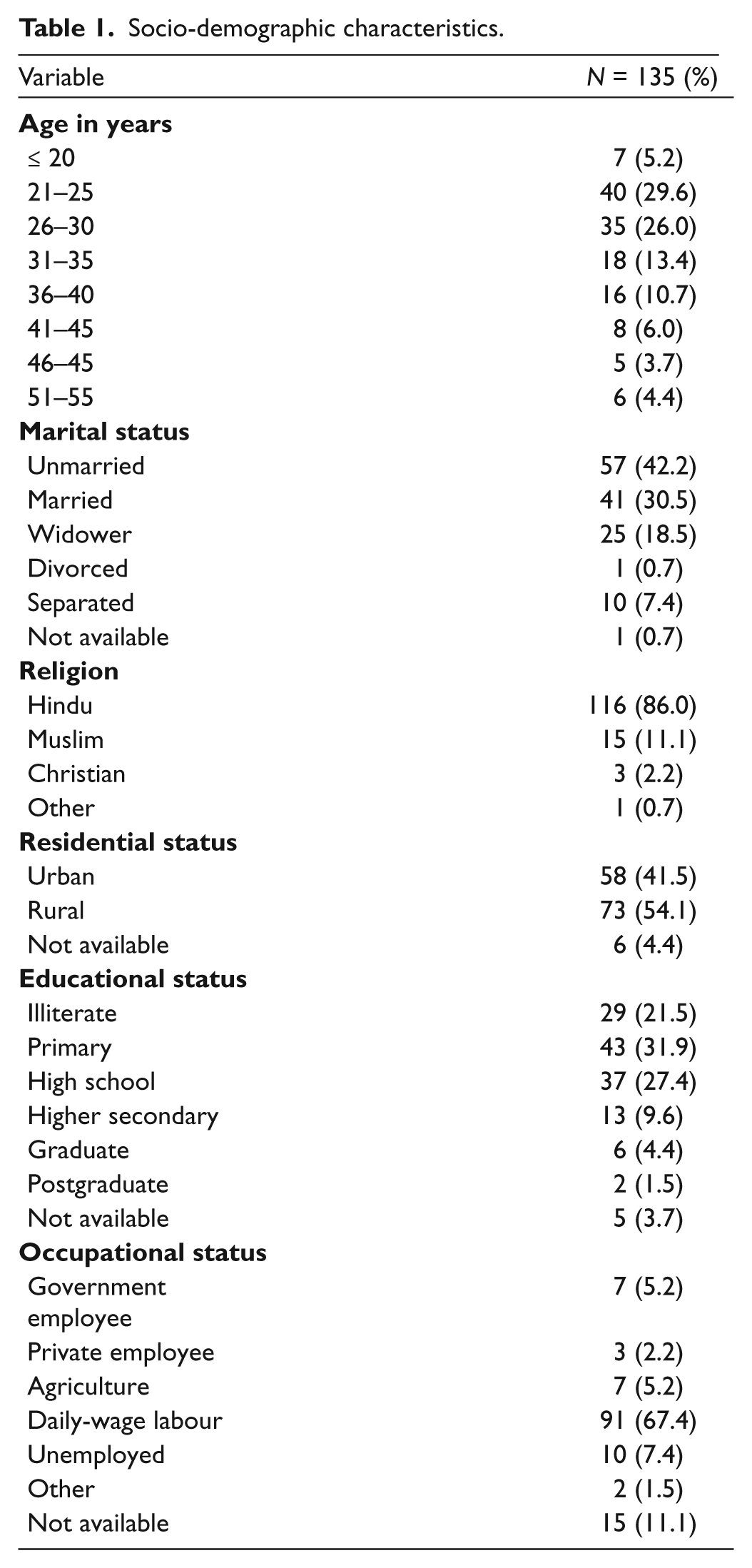
The total sample size was 135 with a mean age of 31.00 (SD = 8.74). Fifty-seven (42.2%) were unmarried, 41 (30.5%) married, 25 (18.5%) widowed, 10 (7.4%) separated and 1 (0.7%) divorced. Marital status was not available for one case file. The majority belonged to the Hindu religion (116, 86%), followed by Muslims (15, 11.1%), Christians (3, 2.2%) and other (1, 0.7%). Seventy-three (54.1%) were from a rural background and 58 (41.5%) from urban. Residential status was unavailable for one case file.
With respect to educational status, 29 (21.5%) had not had any formal education, 43 (31.9%) had primary education, 37 (27.4%) high-school education, 13 (9.6%) had completed higher secondary, 6 (4.4%) had completed graduation and 2 (1.5%) were postgraduates. No information about educational status was available in 5 (3.7%). Daily-wage labourers constituted the majority at 91 (67.4%) followed by 10 (7.4%) who were unemployed, 7 (5.2%) were agriculturists, 7 (5.2%) government employees, 3 (2.2%) private employees and 2 (1.5%) belonged to other categories (Table 1).This information was unavailable for 15 subjects.
Socio-demographic characteristics.
Referral status
All the subjects had been referred for diagnosis and treatment while in 25 (18.5%) certification had also been asked for. Eighty-four (62.2%) had been directly referred from prison by prison officials (medical officer of prison / superintendent of prison), while the remaining 51 (37.8%) had been referred from court via prison officials. The court referrals mentioned the Mental Health Act 1987 in only 5 (3.7%) cases, while in 1 (0.7%) of the subjects, the Indian Lunacy Act 1912 was mentioned. A behavioural observation report from the prison was available in 53 (39.2%) files only. A huge majority (130, 96.4%) had not had any previous admissions. However, during the study period, 14 had two admissions, four had three admissions and one was admitted six times.
Legal issues
A copy of the first information report (FIR), a written document prepared by the police when they first receive information about the commission of a cognizable offence, was unavailable in all 135 subjects (100%). Trial status of the subject was not mentioned in the referral letter in 2 (1.5%) cases. Among the remaining 133, 114 (85.7%) were under trial prisoners (UTP) and 19 (14.3%) were convicted prisoners (CTP). The most common charge was murder (40.7%), followed by severe assault/quarreling (13.3%), theft/robbery (11.9%), public nuisance (9.6%), abetment of suicide/dowry death (6%), dowry related (3%), kidnapping (2.2%), rape (2.2%) and others (0.7%). The information about charges against the patients was obtained by writing letters to the judicial authorities/prison officers. In spite of these efforts, this information was unavailable in 14 (10.4%) records. The duration of imprisonment before admission ranged from 1 to 3,652 days and the mean duration was 432.04 days (SD = 728.83). Lesser durations were mostly deliberate self-harm attempts and suspected psychiatric illness during the initial days of imprisonment.
Certificates were issued in 49 (36.3%) cases. Twenty subjects received a fitness to stand trial certificate (i.e. they were mentally fit or unfit to defend their case in court), 21 received a certificate of illness (i.e. they suffered from mental illness) and 8 received both certificates. Out of the 28 fitness to stand trial certificates issued, 16 (57.1%) were certified fit and the remaining unfit to stand trial.
Clinical characteristics
Total number of days of admission during the study period was computed, inclusive of all admissions in the case of multiple admissions. Mean inpatient stay was 42.25 days (SD = 33.85, range: 4–211). Shorter stays were due to subjects obtaining bail from the court and being discharged during the study period.
Psychiatric diagnoses were made in 122 (90.3%) patients. The distribution of the various psychiatric diagnoses is shown in Figure 1. The most common diagnoses were psychosis, including schizophrenia (28.2%), cannabis dependence syndrome, depression, adjustment disorder, alcohol dependence syndrome and antisocial personality disorder. Recent use of cannabis was confirmed using the cannabis urine testing in 38 patients (28.2%), of which 24 (63.1%) recorded positive.

Distribution of psychiatric diagnoses.
Twenty-two (16.3%) subjects had available and known past history of psychiatric illness: psychosis/schizophrenia (n = 4), mania (n = 4), depression (n = 4), neurotic disorders (n = 3) and others (n = 7). The majority (60%) of subjects had a past history of substance use, 43% had nicotine and alcohol use, 17% had nicotine, alcohol, cannabis and other substance use. In about 11.9% of subjects, the past history of substance use was not available.
Family members were available at the time of admission in only 51 (37.8%) subjects. Among the remaining, family members came to see the patients after admission of their own accord in about a third (34.8%) of cases, while in the remaining, attempts had to be made by the treating team to contact them. Of the 31 (41.9%) subjects with an available family history of illness, 8 had psychosis, 14 had alcohol dependence, 8 had suicide, 5 had depression and 1 had mental retardation.
Most patients (83%) had no past history of major physical illness, whereas the 17% who did had epilepsy/seizures, infections, fractures or head injury. In some subjects (14.1%) physical illnesses was diagnosed during inpatient stay, and were again infections, fractures or head injury and epilepsy/seizures.
Sixty (44.4%) subjects showed high-risk behaviour during the hospital stay, with suicidal risk in 29 (21.5%), deliberate self-harm in 25 (18.5%) and physical violence towards others in 6 (4.4%) (other inmates: 3; nurses: 2; ward assistant: 1).
High-risk behaviour precautions included anti-suicidal measures alone in 39 (63.9%) subjects, parenteral sedative plus antipsychotic in 7 (11.4%) and a combination of the two in 15 (24.5%) cases.
During inpatient stay, restraints were used only in 13 (17%) subjects; physical restraints were never used, although some required chemical restraints multiple times.
Drug therapy was given to the majority (96.3%); the highest use was for sedative hypnotics (82.2%) followed by antipsychotics – atypical (52.6%) and typical (25.2%). The distribution of drugs is shown in Figure 2.
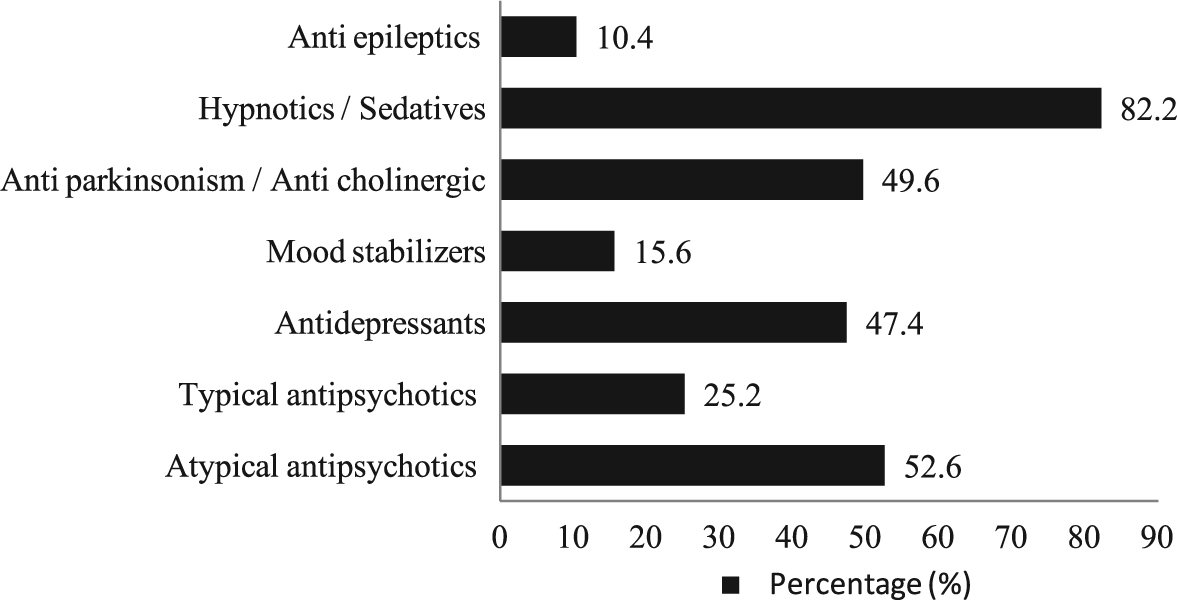
Distribution of types of drugs used for treatment.
Electroconvulsive therapy (ECT) was given in 35 (25.9%) subjects; the mean number of ECTs was 9.57 (SD = 8.33). Consent for ECT was given by the patient himself in 4, taken from doctors and the resident medical officer in 29 and from family members in the remaining 2.
Discussion
Most of the subjects were in their 20s and 30s, consistent with the previous Indian study as well as international studies (Kishore, et al., 1970; O’Connor & O’Neill, 1990). The majority of the subjects belonged to the Hindu religion, reflecting general population demographics. Most were from rural areas, and were poorly educated daily-wage labourers belonging to the lower socio-economic strata.
The majority of patients were referred by prison officials (medical officer of prison / superintendent of prison) and not by the court; the prime reason for referral was diagnosis and treatment, not certification. Hence, it appears that prison officials play a significant role in mental health care and that prisoners’ mental health is deemed more important than certification of fitness to stand trial or an insanity plea. Arguably, prison officials may also be keener to have disturbed prisoners removed from their care than attempt to address the mental health concerns raised by the prisoners themselves. Very few court referrals mentioned the Mental Health Act 1987, which is surprising. Although the Mental Health Act 1987 clearly states not to use derogatory and offensive terms such as ‘insane’, ‘lunatic’, ‘asylum’ and so forth, the majority of the referral letters contained such terms. This reflects the lack of knowledge and sensitivity among the referral authorities.
The first investigation report was not available for any patient and details about charges had to be collected post-admission by contacting judicial/prison authorities. A behavioural observation report from prison was also not available in the majority of cases, possibly reflecting lack of understanding of their importance among prison officials. Absence of these vital documents delays making a clear psychiatric diagnosis and treatment, and the formulation of a legal certificate where required.
The profile of alleged charges with the most common charges being assault and murder is supported by former studies (Cochrane, Grisso, & Frederick, 2001; Friel & White, 2006; MacCall, et al., 2005). The findings on duration of inpatient stay are consistent with previous studies that showed similar ranges (Kishore, et al., 1970; O’Connor & O’Neill, 1990; Simpson, Jones, Evans, & McKenna, 2006).
That more than 90% of patients received a psychiatric diagnosis indicates the high psychiatric morbidity within prisons. After psychosis, the next common diagnosis was cannabis dependence syndrome, with recent cannabis use established in many patients, pointing towards easy availability of cannabis in the prison population, and exacerbation of psychosis. The high rates of substance use is corroborative of former studies (MacCall, et al., 2005), although a high prevalence of neurosis/personality disorder as in some studies (Friel & White, 2006) was not replicated. The predominant use of pharmacotherapy, mainly sedative hypnotics and atypical antipsychotics, is also similar to earlier findings (Simpson, et al., 2006)
High-risk behaviour was recorded in the files of nearly half the subjects during the hospital stay, the most common being suicidal risk, which mainly required close monitoring. However, only a minority had received chemical restraints and none were physically restrained. Reasons for this could include a low percentage of prisoners exhibiting physical violence towards others; the presence of round-the-clock police personnel inside the forensic ward; and the usual practice in the hospital of using chemical restraint judiciously before resorting to physical restraints, indicating respect and protection of human rights.
Certificates were issued in about one-third of subjects and the majority were certified fit rather than unfit to stand trial in accordance with former studies, both Indian (Kishore, et al., 1970) and others (MacCall, et al., 2005; Rogers, Gillis, McMain, & Dickens, 1988).
Strengths and limitations
This is the first comprehensive report on the profile of forensic psychiatric patients in an Indian setting, covering an entire admission cohort over five years – thus reducing selection bias. The major drawback of the study was that it is a retrospective chart review. However, forensic case records at the institute are documented meticulously in view of it being a legal document. Documentation in each case record is monitored by two consultants in forensic psychiatry and one senior resident. In addition, data extraction was done using a structured data-extraction tool systematically and meticulously. Another limitation of the study is that there were no female patients, because of the absence of a female forensic psychiatric ward in the institute. Gender differences in psychiatric morbidity needs to be evaluated further.
Conclusion
Concluding, the current profile of male forensic psychiatric inpatients is in accordance with past studies from India and outside. However, there is a need to streamline the procedure of referral and to sensitize the referral authorities about the Mental Health Act and people with mental illness, along with the need to attach the first investigation report and behavioural observation report to enable a better understanding of the context of referral and avoid undue delays in diagnosis, treatment and certification on the side of the treating team. In view of the high rates of substance abuse, trafficking of these substances within the prison needs to be more stringently monitored, and de-addiction services and facilities need to be established on prison premises so that inmates get the benefit of treatment at the earliest opportunity.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.