
Abstract
Background:
During the past decade, the mental health consumer movement has drawn the attention of mental health providers, researchers and policy makers to the concept of recovery. Traditionally, recovery primarily refers to the remission of symptoms. Nowadays, recovery is also regarded in a sense that all individuals, even those with severe psychiatric disabilities, can improve. Accordingly, recovery for people with severe mental illness refers to hope and optimism, empowerment, regained control and increased self-esteem, illness self-management and engagement in meaningful daily activities (Corrigan, Giffort, Rashid, Leary & Okeke, 1999; Jacobson & Greenley, 2001; Leamy, Bird, le Boutillier, Williams & Slade, 2011; van Gestel-Timmermans, Brouwers, van Assen, Bongers & van Nieuwenhuizen, 2012). Little empirical research, however, has been done and instruments to measure recovery are scarce.
Aims:
In the current study, the psychometric properties of the Dutch version of the Mental Health Recovery Measure (MHRM) are explored. Convergent and divergent validity of the MHRM was assessed using standardized measures of hope (Hope Herth Index (HHI)), recovery-promoting professional competence (Recovery Promoting Relationships Scale (RPRS)) and general physical health and well-being (RAND Measure of Health-Related Quality of Life (RAND-36)).
Methods:
A factor analysis was conducted and Cronbach’s α of the MHRM scales was assessed. The construct validity was assessed by computing the intercorrelations of the MHRM, HHI, RPRS and RAND-36.
Results:
Data were available for 212 patients: 70 patients completed the MHRM, HHI and RAND 36 and 142 filled out the MHRM and RPRS. Exploratory factor analysis resulted in an interpretable three-factor solution. Cronbach’s α ranged from 0.86 to 0.94. The convergent validity of the instrument was satisfactory; the divergent validity was less clear.
Conclusions:
This study offers evidence to suggest that the Dutch version of the MHRM is a reliable measure (in terms of internal consistency) with a generally acceptable convergent and divergent validity. Further research is needed to clarify the extent to which the MHRM is sensitive enough to capture the individual recovery process of patients.
Introduction
During the past decade, the mental health consumer movement has drawn the attention of mental health providers, researchers and policy makers to the concept of recovery. Traditionally, recovery primarily referred to the remission of symptoms (Fava, Ruini & Belaise, 2007; Lysaker & Buck, 2008). Nowadays, recovery is also regarded in a sense that all individuals, even those with severe psychiatric disabilities, can improve. This means that recovery is more than the remission of symptoms and can be achieved despite the existence of these symptoms (Anthony, 1993a, 1993b; Lloyd, King & Moore, 2010; Mead & Copeland, 2000; Roberts & Wolfson, 2004). Accordingly, recovery for people with severe mental illness refers to hope and optimism, empowerment, regained control and increased self-esteem, illness self-management and engagement in meaningful daily activities (Corrigan et al., 1999; Jacobson & Greenley, 2001; Leamy et al., 2011; van Gestel-Timmermans, Brouwers, van Assen, Bongers et al., 2012). Recovery-orientated services work collaboratively with service users to agree and facilitate their individualized goals.
The consumer movement has urged that mental health services should be more recovery-orientated and this notion is gradually being incorporated internationally into mental health policy (Allott, Loganathan & Fulford, 2002; Andresen, Caputi & Oades, 2006; Marshall, Crowe, Oades, Deane & Kavanagh, 2007; Ramon, Healy & Renouf, 2007). Moreover, the demand to demonstrate effectiveness of mental health services is increasing (Srebnik et al., 2002). One way to demonstrate effectiveness is through assessment and monitoring of change and by reviewing outcome. Although mental health care is embracing recovery as an important and essential concept in the effective treatment of patients, little empirical research has been done and instruments to measure recovery are scarce (Corrigan et al., 1999; Drapalski et al., 2012; Schön, Denhov & Topor, 2009; van Gestel-Timmermans, Brouwers, van Assen & van Nieuwenhuizen, 2012; Weeks, Slade & Hayward, 2011). There are at least two reasons why measuring the recovery concept is warranted. First, monitoring of the individual recovery process can provide the client and professional with information that can be used during treatment and rehabilitation interventions. Second, results from recovery instruments can stimulate policy makers to develop and improve recovery-based care and mental health policy (Burgess, Prikis, Coombs & Rosen, 2011; Marshall et al., 2007). In order to do justice to the aspects of monitoring and recovery-based care, reliable instruments are needed. To this end, the psychometric properties of the Mental Health Recovery Measure (MHRM; Young & Bullock, 2003) are explored in the current study.
Methods
Participants
In this study, patients receiving long-term ambulatory or residential psychiatric care participated. Of these patients, 70 took part in a psychometric evaluation study of the MHRM and 142 participated in a study pertaining to the evaluation of recovery-oriented care in which the MHRM was used. Prior to participation, all patients were verbally informed by their personal mental health professional and/or researcher, received written information about the study they were enrolled in and provided written informed consent. Prior to the start, the regional Medical Ethics Approval Committee for Mental Health Care Institutions (METIGG) was approached. According to the Medical Research Involving Human Subjects Act (WMO), ethical approval was not required.
Instruments
The MHRM was chosen after (1) an extensive search of available instruments to measure recovery and (2) asking patients about their preference. Our search led to two potential appropriate instruments: the MHRM and the Recovery Assessment Scale (RAS; Corrigan & Phelan, 2004). Forty-five patients were asked to judge – on face value – both the MHRM and the RAS. Participants were recruited through experts by experience. In an interview with the researcher, each patient expressed his or her thoughts about the two instruments and their comments were registered. Of these patients, 63% reported that they preferred the MHRM over the RAS and we therefore decided to further explore the psychometric properties of the MHRM.
Mental Health Recovery Measure
The MHRM is a self-report instrument designed to assess the recovery process of persons with severe mental illness. The level of each respondent’s recovery is assessed without relying on the measurement of symptoms or symptom management. The MHRM was developed for two reasons: (1) to provide an individual self-report change measurement for the level of recovery; and (2) to be used as a programme evaluation tool. The items and domains of the MHRM were developed from a qualitatively derived grounded theory model of recovery and based upon the recovery experience of individuals with psychiatric disability (Young & Bullock, 2003; Young & Ensing, 1999). Subsequent development of the MHRM was based on the data of 279 mental health consumers in a variety of inpatient, forensic and community mental health settings. Reliability analysis and Rasch modelling resulted in a series of revisions to the original instrument, which eventually resulted in its current 30-item version. The original instrument comprises seven sub-scales, each of four items: ‘overcoming stuckness’ (α = 0.60); ‘self-empowerment’ (α = 0.82); ‘learning and self-redefinition’ (α = 0.79); ‘basic functioning’ (α = 0.62); ‘overall well-being’ (α = 0.86); ‘new potentials’ (α = 0.62) and ‘advocacy/enrichment’ (α = 0.66); there are two separate items that measure ‘spirituality’ (α = 0.89). All items are rated using a five-point Likert scale that ranges from ‘strongly disagree’ to ‘strongly agree’ (Young & Bullock, 2005).
Hope Herth Index
The Herth Hope Index (HHI) is a self-report questionnaire that measures hope. The HHI has 12 Likert-scale items, with scores ranging from 1 (‘strongly disagree’) to 4 (‘strongly agree’). The Dutch version of the HHI comprises two factors, each of six items: ‘view on life and future’ and ‘self-confidence and inner strength’ (van Gestel-Timmermans, van den Bogaard, Brouwers, Herth & van Nieuwenhuizen, 2010).
RAND-36
The RAND-36 comprises 36 items that assess eight health concepts: physical functioning; role limitations caused by physical health problems; role limitations caused by emotional problems; social functioning; emotional well-being; energy/fatigue; pain; and general health perceptions. Six sub-scales have items on three- to six-point Likert scales and the other two have items that can be answered with ‘yes’ or ‘no’. It also includes a single item that provides an indication of perceived change in health (van der Zee, Sanderman, Heyink & de Haes, 1996).
Recovery Promoting Relationship Scale
The Recovery Promoting Relationship Scale (RPRS; Russinova, Rogers & Ellison, 2006) is a self-report questionnaire for patients and measures the generic components of mental health providers’ recovery-promoting professional competence as seen by patients. In this study, the Dutch version of the RPRS was used (Wilrycx, Croon, van den Broek & van Nieuwenhuizen, 2012). This version consists of 22 items and has two scales; items are scored on a five-point Likert scale (‘do not agree’/‘agree’). The first scale (consisting of 17 items) is called ‘hopefulness and empowerment’ and represents the more recovery-related strategies, whereas the second scale, ‘self-acceptance’ (comprising five items), represents the provider’s skills to enhance clients’ self-acceptance.
Procedure
Seventy patients filled out the MHRM, HHI and RAND-36 and 142 patients filled out the MHRM and RPRS. Data were collected in two separate studies, one specifically aiming at looking at the psychometric properties of the MHRM (70 patients; data collected until beginning of 2008) and one as part of a larger study in which a recovery-oriented training was evaluated (142 patients; data collected until mid-2008). Since no Dutch version of the MHRM and RPRS existed, they were prepared in Dutch by using the backward-forward translation procedure (Cull et al., 2002; Wilrycx et al., 2012). First, five English/Dutch bilinguals made translations into Dutch. Any obvious differences between the English and Dutch versions were then discussed with a native English speaker. This process produced a consensus version of Dutch items that was subsequently translated back into English by two other native speakers. A fourth English native speaker discussed differences between this English version and the original. Final versions were thus constructed maintaining essentially the same format and meaning as the original instruments.
Statistical analysis
Factor analysis
Because four of the seven sub-scales of the MHRM of Young and Bullock (2003) had an α lower than 0.70, an exploratory factor analysis (EFA) using SPSS 17 was conducted on the Dutch version. The number of factors to retain in a principal axes factor solution was based on visual inspection of Cattell’s scree plot and on the results of a parallel analysis, as recommended by Fabrigar, Wegener, MacCallum and Strahan (1999). All principal axes solutions were obliquely rotated by means of the oblimin rotation procedure. Factor loadings with an absolute value larger than 0.30 were considered salient.
Reliablity analysis
On the basis of the factor analysis, sub-scales were formed for the MHRM and the reliability (in terms of Cronbach’s α) was assessed. An α value of 0.70 was considered the minimum for each scale. In addition, the reliability (in terms of Cronbach’s alpha) of all other scales used in the current study was assessed.
Construct validity
The construct validity of the MHRM was assessed by computing the correlations between the scales of the MHRM, HHI, RAND-36 and RPRS. Convergent validity was assumed if correlations were medium to high between the MHRM scales and the two scales of the HHI and the RAND-36 scales of social functioning, emotional well-being and energy/fatigue. Divergent validity was assumed if correlations were low (i.e. < 0.30) between the MHRM scales and the two scales of RPRS and the RAND-36 scales of ‘physical functioning’, ‘role limitations’ (physical health problems and emotional problems), ‘pain’ and ‘general health perceptions’. Note: according to Cohen (1998), a medium correlation ranges from 0.30 to 0.49 and a high correlation is r > 0.50.
Results
Sample characteristics
The mean age of the patients was 47.2 (SD = 13.1) and 64% of the group were female. General demographic and psychiatric characteristics are given in Table 1.
Demographic and psychiatric characteristics of the participants.
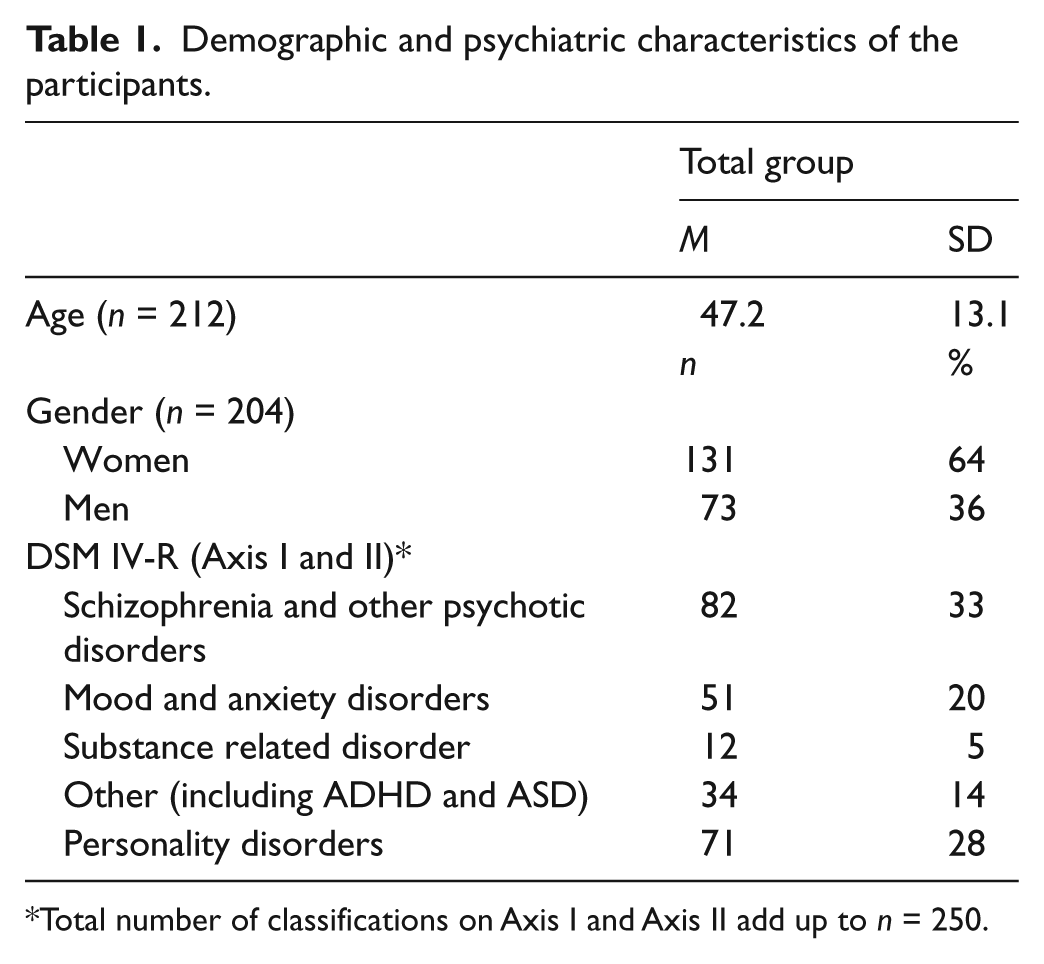
Total number of classifications on Axis I and Axis II add up to n = 250.
Exploratory factor analysis
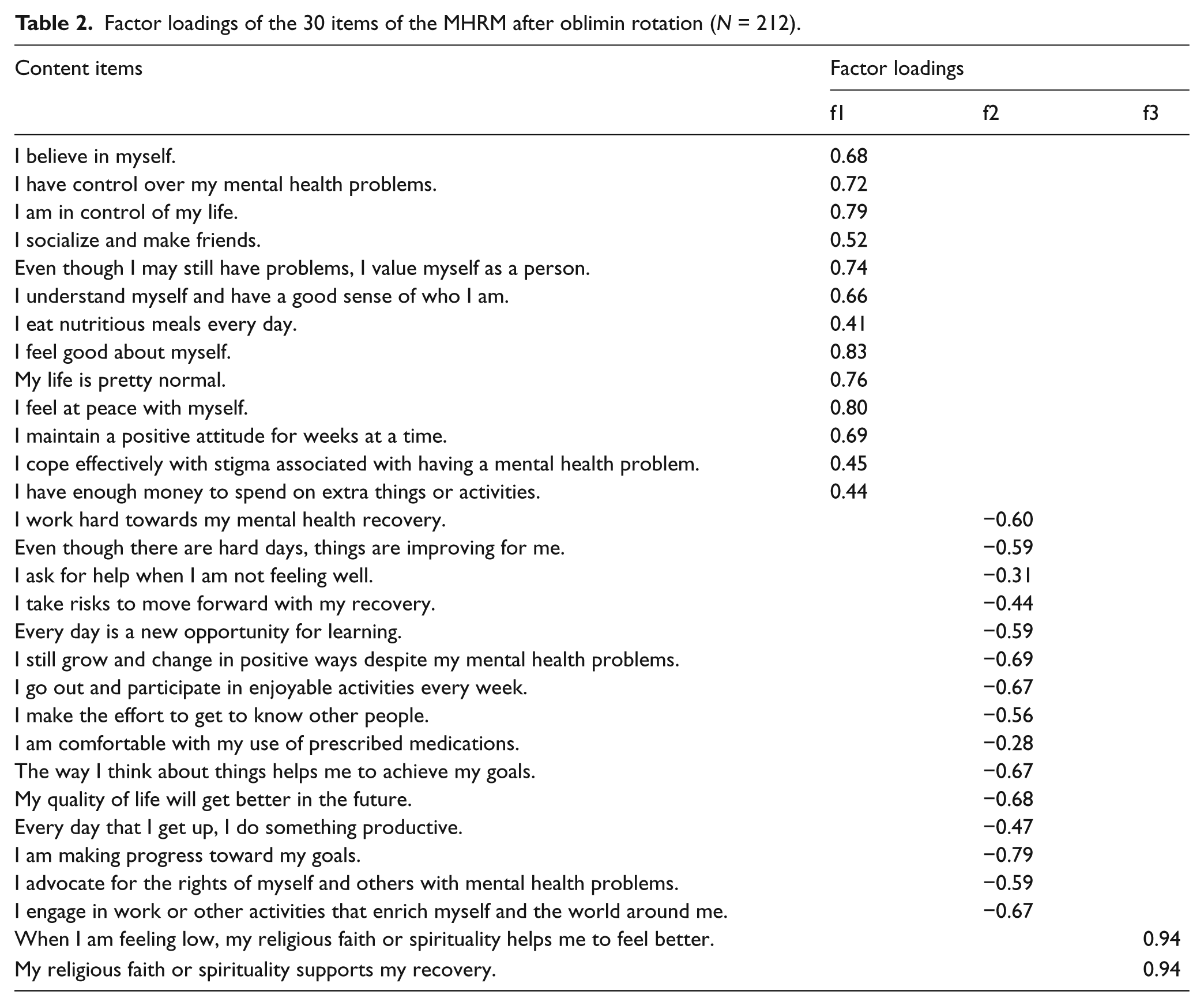
EFA on the 30 items of the MHRM resulted in seven components with an eigenvalue > 1.0. Together they explained 62% of the variance. Visual inspection of Cattell’s scree plot, however, showed that a three-factor solution was a far better option than a seven-factor solution. Moreover, some components comprised only a few items and one component consisted of just one item. Therefore, the analysis was repeated with a forced three-factor solution that explained 46% of the variance. After oblimin rotation, a good interpretable factor structure emerged (Table 2). All items but one loaded > 0.30 on at least one factor, with the majority of the items (77%) loading > 0.50.
Factor loadings of the 30 items of the MHRM after oblimin rotation (N = 212).
Reliability and scale labelling (MHRM)
Cronbach’s α coefficients for the three scales after EFA were 0.90, 0.86 and 0.94. Items of the first scale pertained to understanding oneself and feeling in control and the scale was therefore labelled ‘self-empowerment’. The second scale encompassed items that deal with learning new things, personal growth and the advocacy of rights of people with mental illness and was therefore labelled ‘learning and new potentials’. The last scale consisted of two items specifically focused on religion/spirituality, labelled ‘spirituality’.
In the current study, the Cronbach’s α coefficients for the two scales of the HHI were 0.85 and 0.75. The α coefficients of the RAND-36 current study ranged from 0.63 to 0.93; six of the eight scales had an α of 0.76 and higher and the αs for the two scales of the RPRS were 0.93 and 0.87.
Convergent and divergent validity
Table 3 shows the correlations between MHRM scales and the scales of the HHI, RAND-36 and RPRS. According to expectations, a significant medium to high correlation was found between the scales of the MHRM and HHI. A non-significant and low correlation, however, was found between the MHRM scale ‘spirituality’ and the HHI scale ‘view on life and future’. Significant medium to high correlations were also found between two of the three MHRM scales and the RAND-36 scales ‘social functioning’, ‘emotional well-being’ and ‘energy/fatigue’. As can be seen, the MHRM scale ‘learning and new potentials’ had an unexpected low and non-significant correlation with the social functioning scale of the RAND-36 and the MHRM scale ‘spirituality’ correlated low and non-significantly with all the aforementioned RAND-36 scales.
Correlations between scales of the MHRM, HHI, RAND-36 and RPRS.
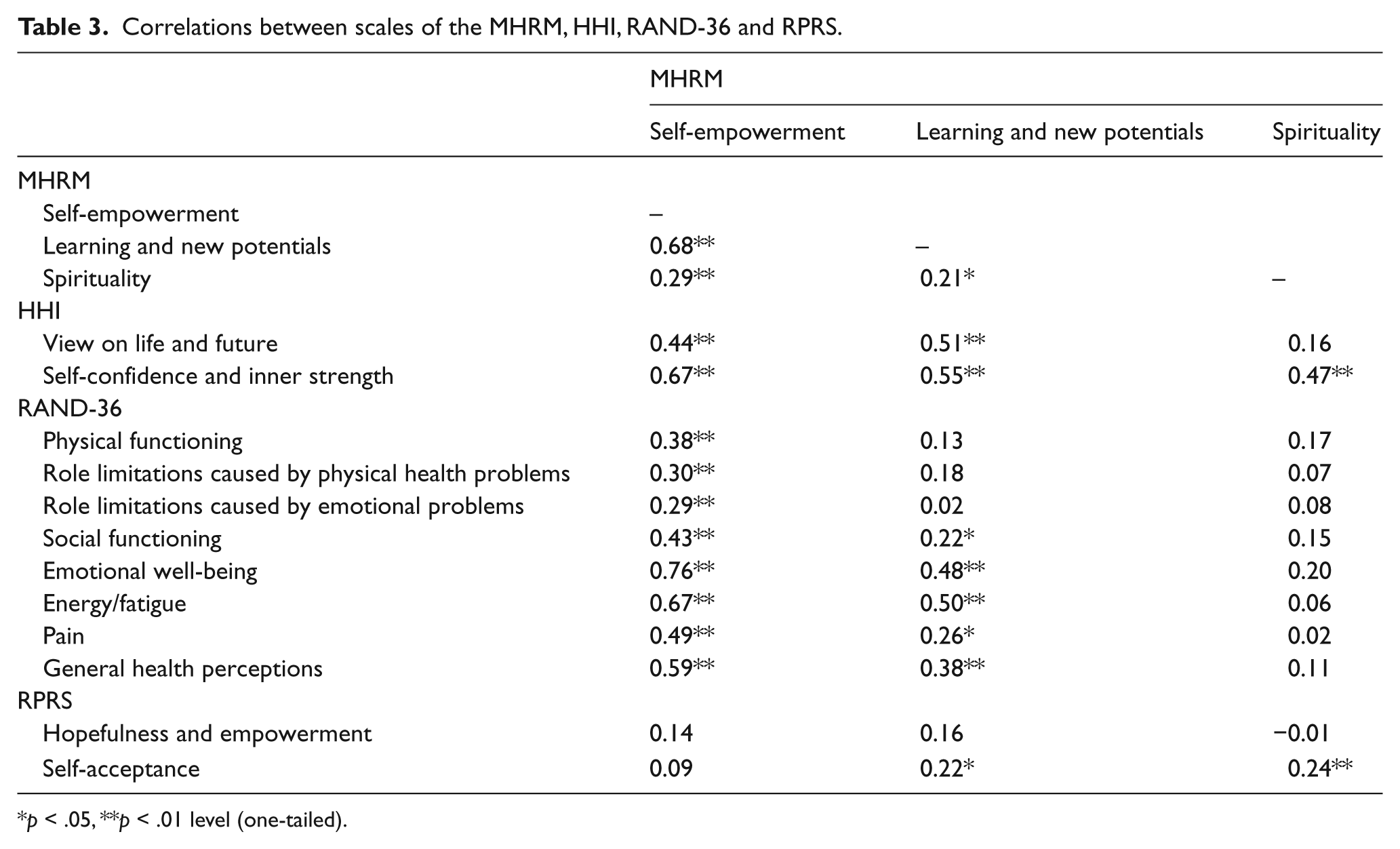
p < .05, **p < .01 level (one-tailed).
As for the divergent validity, low and non-significant correlations were found between all the scales of the MHRM and RPRS. The correlations between the MHRM scales and RAND-36 scales ’physical functioning’, ‘role limitations’ (physical health problems and emotional problems), ‘pain’ and ‘general health perceptions’ were less clear. As expected, low correlations with ‘learning and new potentials’ and ‘spirituality’ were found – except for a medium correlation between ‘learning and new potentials’ and ‘general health perceptions’ (r = 0.38). Medium to high correlations, however, were found with the MHRM scale ‘self-empowerment’, with correlations ranging between 0.30 and 0.59.
Conclusions
This study offers evidence to suggest that the Dutch version of the MHRM is a reliable measure (in terms of internal consistency), with a generally acceptable convergent and divergent validity. When considering the original MHRM as a suitable instrument to measure the individual recovery process, we noticed that not much information in scientific journals was available on the psychometric properties of the scale. Moreover, the composition of the sub-scales was not derived from a factor analysis carried out on a large pool of items, but was primarily based on substantive grounds (Cavelti, Kvrgic, Beck, Kossowsky & Vauth, 2012; Young, Ensing & Bullock, 2000). Recently, Drapalski et al. (2012) have mentioned this as two major criticism points on the MHRM. Instead of developing a new scale as Drapalski and colleagues have done, we have chosen to conduct an EFA on the MHRM on a substantial data set. The EFA resulted in an interpretable three-factor solution and the internal consistency of these three scales was good to excellent.
As for the validity of the modified MHRM, there are some interesting results that need further exploration. The MHRM scale ‘spirituality’, for instance, has a low and non-significant correlation with the vast majority of the other scales used in this study and also correlates low (although significantly) with other the two scales of the MHRM. These two items pertaining to religion/spirituality are probably too constricting in what people understand or feel as ‘belief’. Since respondents in the Netherlands in general experience religion in a different way than for instance the USA, this might explain why this factor stands on its own (e.g. van Nieuwenhuizen, Schene, Koeter & Huxley, 2001).
Results also show that the MHRM scale ‘self-empowerment’ correlates medium to high with nearly all scales of the RAND, whereas no relationship was expected with the more health-related aspects of the RAND (e.g. physical functioning and general health perceptions). It seems that feeling in control and good about oneselves – which are key elements of the scale ‘self-empowerment’ – has a positive effect on other areas of life (Corrigan & Penn, 1999), while this is not the case for ‘learning and new potentials’. The correlations of the MHRM with the RAND and RPRS suggest that the MHRM is measuring something different than, for example, role limitations and is not related to the recovery-promoting skills of professionals per se. This underlines the importance of differentiating between service-based recovery definitions and user-based recovery definitions (Schrank & Slade, 2007).
To conclude, the factors of the MHRM correspond with the consumer literature on recovery. The Dutch version of the MHRM is potentially a suitable instrument for evaluation studies and can play a role in stimulating policy makers to improve recovery-based care and mental health policy. Further research is needed, however, on the test-retest reliability and on the extent to which the MHRM is sensitive enough to capture the individual recovery process of patients so that it can become more than just an end point outcome measure (cf. Resnick, Fontana, Lehman & Rosenheck, 2005).
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.