
Abstract
Background:
Latin Americans represent one of the fastest-growing immigrant populations in Canada. But very little is known about their mental health.
Aims:
This paper reviews the literature on the mental health of Latin American immigrants to Canada. The paper also identifies potential areas to expand the research agenda.
Method:
Twenty-five papers were identified by a comprehensive electronic search undertaken in medical- and humanities-related databases.
Results:
Results are reported in three sections: (1) the rates of mental illness; (2) the risk factors that affect mental health; and (3) the access and barriers to care and services. Findings indicate that despite the diversity of immigration from Latin America to Canada, much of the information on mental health focuses on Central American refugees. The most frequently examined risk factor is displacement as a consequence of political persecution and torture in the home country. Access to mental health services in this population seems to be limited by cultural differences and language barriers.
Conclusion:
New research on this topic should reflect the growing diversity and heterogeneity of the Latin American population in Canada.
Introduction
According to government figures, there are 305,000 people of Latin American origin in Canada. Twenty-eight per cent arrived between 2001 and 2006, making this one of the fastest-growing immigrant populations. The Latin American population in Canada is active and vibrant, contributing in many aspects of public life, particularly in the largest cities of the country such as Toronto, Montreal and Vancouver (Statistics Canada, 2008, 2009a, 2009b, 2009c).
The interaction of Latin Americans with the host society has attracted the attention of scholars working in the fields of political participation, education and transnational families (Bernhard, Landolt & Goldring, 2009; Ginieniewicz, 2007, 2008). However, less is known about the health of this group in Canada, particularly their mental health.
This paper is a review of the literature on the mental health of Latin American immigrants to Canada. It uses the international literature on Latin American immigration and mental health to highlight what is known and what is missing in our knowledge of this population in Canada. The aim of this study is to review the literature on the mental health of the Latin American population in Canada. It is the first of its kind and identifies gaps in our knowledge that could be the subject of future research.
Background
Demography of the population of Latin American origin in Canada
Diverse migratory statuses, difficulty in determining the ‘Latin Americanness’ of an array of generations and self-categorization have made it difficult for scholars, government agencies and community organizations to reach an agreement on ‘who qualifies as a Latin American’. Because of this, the figure of 305,000 people of Latin American origin in Canada has been questioned (Ginieniewicz, 2010; Schugurensky & Ginieniewicz, 2007a).
When defining the size and composition of this population, one of the main sources of disagreement is related to the use of the terms ‘Latin American’ and ‘Hispanic’. Latin Americans are those who have origins in a country of the Americas that was colonized and influenced by a Latin power in the past (Spain or Portugal). However, in Canada, this definition is not widely accepted and part of the community prefers the word ‘Hispanic’. The term Hispanic includes people from Europe as well as immigrants from the Americas. However, people from Brazil are not included because they speak Portuguese (Ginieniewicz, 2010).
The dual categorization ultimately refers to issues of language, self-identification and differences between first- and second-generation immigrants. These circumstances have led to confusion in the calculation of the size of the population. It is therefore important to be aware of the fact that selecting either ‘Latin American’ or ‘Hispanic’ as categories of analysis may influence the demographic assessment (for a detailed discussion on this topic, see Ginieniewicz, 2010; Schugurensky & Ginieniewicz, 2007b).
Despite the difficulties surrounding the definition of groups of ‘Hispanic’ or ‘Latin American’ origin, data suggest that this population has increased significantly (Statistics Canada, 2008, 2009a, 2009b, 2009c). Similar to other groups, Latin American immigrants have tended to settle in the major Canadian cities. In Canada, more than 30 per cent of the population of Latin American origin lives in Toronto (Statistics Canada, 2007).
According to Statistics Canada, 17 per cent of immigrants from Latin America aged 15 and over hold a university degree, compared to 15 per cent in the adult Canadian population. However, Latin American immigrants have an average income 25 per cent lower than their peers (Statistics Canada, 2007). The educational situation is complex. Despite the high educational attainment of parts of the community, the Toronto District School Board reports that school dropout among youth of Latin American origin has now reached 40 per cent, which is twice the average of Toronto public schools (Schugurensky, 2009).
Recently, the Latin American population in Canada has been receiving increasing scholarly attention. So far, the literature has mostly focused on the civic and political engagement of the community (Ginieniewicz, 2007, 2010; Landolt & Goldring, 2009) and the situation of transnational families (Bernhard, Landolt & Goldring, 2005; Bernhard et al., 2009).
The mental health of Latin American populations: International research
Research has detailed the impacts that immigration can have on mental health. Circumstances that occur before, during and after migration may have effects on the mental well-being of immigrants. Pre-migration circumstances that increase risk of mental health problems and illness include war, famine, rape, torture, internment and economic crises. Factors during the migration process such as moving from country to country, losing touch with family and lost possessions are also important. In addition to this, poverty, discrimination, unemployment, acculturation, lack of language skills and separation from family represent some of the post-migration factors that can jeopardize immigrants’ mental health (Beiser, 1999; Fenta, Hyman & Noh, 2004; Fitinger & Schwartz, 1981; Handlin, 1951). There is some evidence that newcomers to Canada are less likely to have mental health problems than the native-born population, which is usually described as ‘the healthy immigrant effect’. The reasons for this are unclear but there is evidence that the health of immigrants, particularly their mental health, tends to decline over time (Ali, 2002; Lou & Beaujot, 2005; Ng & Rasugu Omariba, 2010).
One way of approaching the literature on the linkages between mental health and immigration is by focusing on three different, although related, dimensions: (1) the rates of mental illness among immigrants; (2) social risk factors that affect the mental health of immigrants; and (3) access and barriers to care that immigrants face (Hansson, Tuck, Lurie & McKenzie, 2010).
The mental health of ‘Latinos’ has been investigated most thoroughly in the USA, where this population represents the largest minority group. (We employ the term ‘Latinos’ as it is usually used to refer to both Latin American immigrants and Latin American descendants in the USA.) Most studies on the mental health of Latinos in the USA analyse the situation of Latin American economic immigrants and their descendants, although some focus on refugees (De Jesús-Rentas, Boehnlein & Sparr, 2012; Eisenman, Gelberg, Liu & Shapiro, 2003). Recent studies indicate that, in general, the rates for most mental disorders among Latino populations are similar to that of the overall population (APA, 2010). However, studies have also demonstrated that demographic variables are critical to interpret these rates, as the category of ‘Latino’ is composed of very diverse subgroups. Therefore, rates can vary considerably according to the specific subgroups. For example, using the National Latino and Asian American Study (NLAAS), Alegría, Norah Mulvaney-Day, Polo, Cao and Canino (2007) demonstrated that increased rates of psychiatric disorders can be found among US-born, English-language-proficient and third-generation Latinos. Moreover, Puerto Ricans have the highest overall prevalence rates among the different Latino ethnic subgroups assessed (Alegría et al., 2007; Alegría, et al., 2008; Lewis-Fernández, Das, Alfonso, Weissman & Olfson, 2005).
Risk factors such as unemployment, poverty (including lack of insurance and impossibility to afford transportation), language proficiency and cultural isolation also have an impact on the mental health of Latinos in the USA. Studies have shown that stress experienced as a consequence of getting used to a new culture or environment (acculturative stress) is a risk factor for anxiety disorders, depression and suicidal ideation (Crockett et al., 2007; Hovey, 2000a, 2000b).
Most of the aforementioned risk factors have also been linked to the difficulties in accessing mental health care in this population. Latinos tend to seek help for mental health problems from primary care providers rather than from mental health specialists. Only one out of 11 Latinos with a mental disorder contact a mental health specialist, while one in five contact general health care providers (Lewis-Fernández et al., 2005; USDHHS, 2001). Studies have pointed to poverty (Crowley, 2003), stigma (Brennan, Vega, Garcia, Abad & Friedman, 2005; Brown et al., 2004), traditional forms of healing (Brennan et al., 2005) and the language in which treatment is received (APA, 2010; Lewis-Fernández et al., 2005) as crucial variables to understand the barriers to care among Latinos.
In general, all these studies caution against over-generalizing the rates and social factors that affect the mental health of Latinos in the USA. They consider it prudent to analyse Latinos in different subgroups because of the range of ethnic groups, nationalities, generations, cultural backgrounds, socio-economic conditions and migratory statuses.
Methods
There were three inclusion criteria for this literature review: (1) research studies that analysed the psychosocial aspects of the mental health of adult Latin American immigrants to Canada; (2) peer-reviewed material; and (3) research studies written in English and conducted in Canada.
In consultation with the senior librarian at the Centre for Addiction and Mental Health, a comprehensive electronic literature search was undertaken in the following databases: Medline, PsycINFO and CINAHL. PAIS International, ProQuest Dissertations and Theses (PQDT) were also included in order to capture any additional studies that could address these topics in disciplines related to social sciences and humanities. The electronic searches were conducted during the first two weeks of April 2012.
We used combinations of subject headings and keywords. We performed searches using ‘or’ in four different groups of keywords in all the fields on record in each database. Then we carried out a search using the preposition ‘and’ combining groups 1–4 as outlined below:
Group 1: Immigration, refugees, migrant worker.
Group 2: Latinos/Latinas, racial and ethnic groups, Hispanic, Latin American, Central American, South American, Mexican.
Group 3: Mental health, emotional adjustment, well-being, mental disorders, mental health services, community mental health services.
Group 4: Canada, Canadian, British Columbia, Alberta, Saskatchewan, Manitoba, Ontario, Quebec, Newfoundland, Nova Scotia, New Brunswick, Prince Edward Island.
We undertook supplementary searches in the aforementioned databases including only one keyword per row to ensure that no literature was missed. We located through Google Scholar those studies that used Statistics Canada’s databases focused on the health of immigrants to Canada. This search targeted in particular those studies that presented data on Latin American immigrants to Canada. All the abstracts were read; for the review, full papers were obtained.
We also performed forward- and backward-tracking exercises on the papers selected (Wooding, Hanney, Buxton & Grant, 2005), although these techniques did not add other articles to the review. We then conducted a narrative review.
Results
We identified 179 abstracts from the electronic databases. After a manual review, 157 studies were excluded for a variety of reasons: (1) duplications (43 studies); (2) abstracts included one or more keywords but the research study was either not conducted in Canada or was not on Latin American immigrants who arrived in Canada as adults or was not directly related to mental health (90 studies); (3) studies focused on neurological and/or biological research only (18 studies); (4) studies focused on drugs and/or substance abuse (three studies); and (5) studies did not include original research findings (three studies). From the 179 abstracts selected from the electronic database, 22 articles were selected for the literature review.
The Google Scholar search identified three further studies: one that used the Longitudinal Survey of Immigrants to Canada (LSIC) and two that used the Canadian Community Health Survey. This review includes 25 papers (Figure 1).
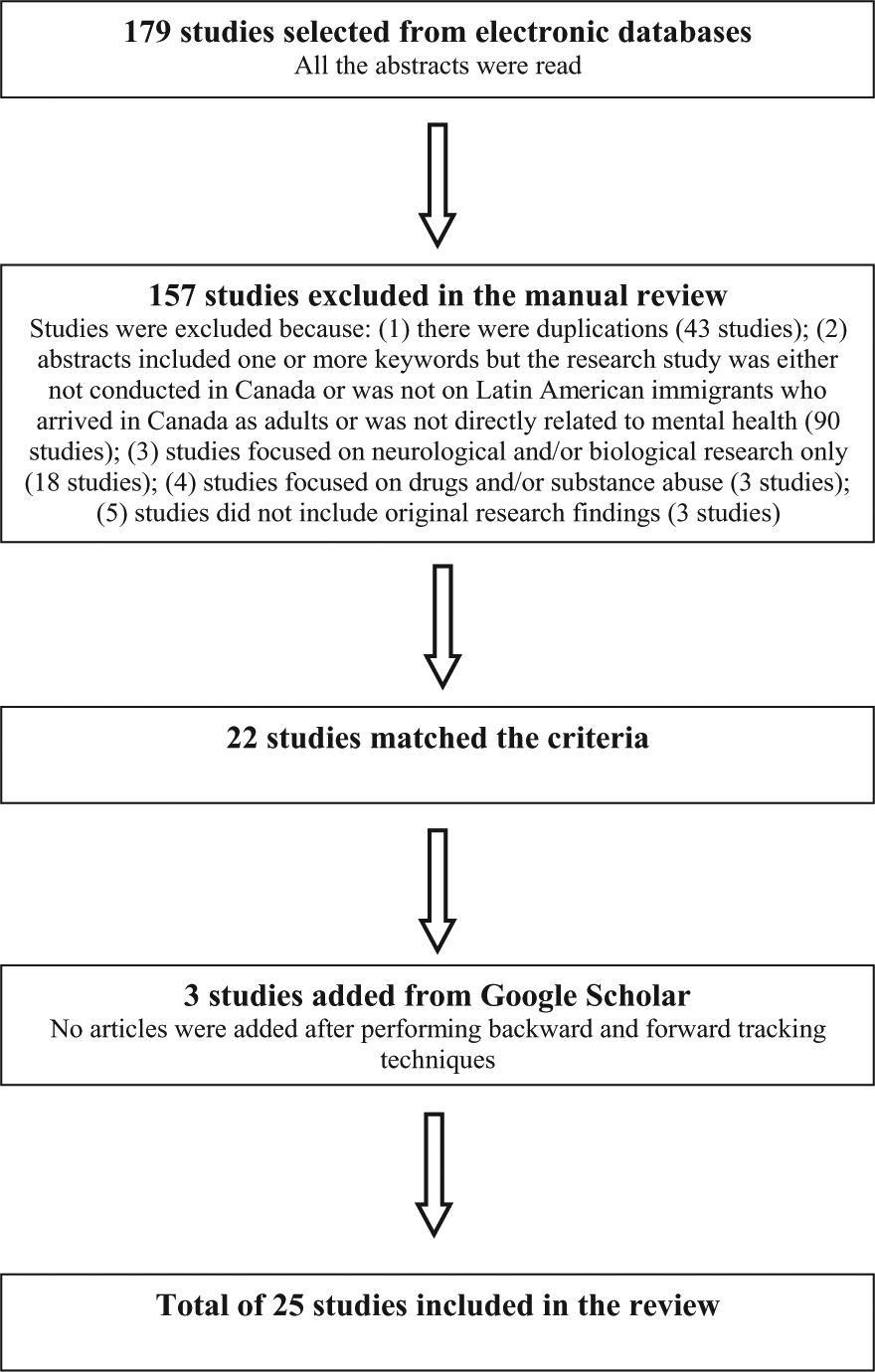
Procedure to select the papers.
The papers are both qualitative and quantitative. They span three decades. Studies investigated a number of different populations: some addressed ‘Latin Americans’ in general; some analysed Latin American women; some reported on the populations of the Central American region; others described populations from particular countries. Because of migration patterns, a significant number of studies measured the mental health of Central American refugees.
Three studies investigated the rates of mental illness, four investigated barriers to care, but the majority investigated social determinants and risk factors for mental illness.
Rates of mental illness among Latin American immigrants to Canada
Citizenship and Immigration Canada’s Research and Evaluation Branch conducted a study on the mental health of recent immigrants to Canada. The study drew data from Statistics Canada’s 2005 Longitudinal Survey of Immigrants to Canada (LSIC) and followed up individuals at three different times: six months (Wave 1), two years (Wave 2) and four years (Wave 3) after arrival. It reports that immigrants from Central or South America are among three groups with the highest levels of stress (approximately 33 per cent) for Waves 2 and 3. ‘Stress level’ was measured using a self-assessment of stress on most days: being stressed (very/extremely) or not being stressed (not at all/not very/a bit). (Results were obtained using responses to a question included in the LSIC questionnaire (Robert & Gilkinson, 2010).) Table 1 provides a complete summary of the studies that analyse the rates of mental illnesses among Latin American immigrants in Canada.
Studies that analyse the rates of mental illness among Latin American immigrants in Canada.
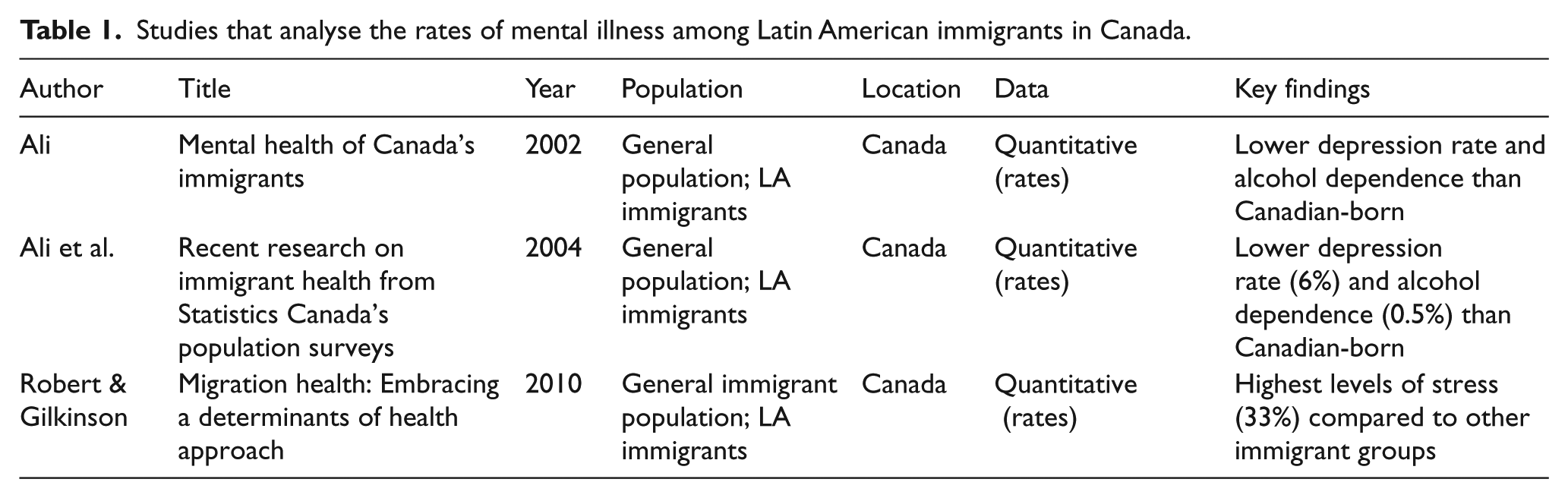
Analysing data from the 2000/01 Canadian Community Health Survey, Ali et al. (2004) found that immigrants from South and Central America had a depression rate of 6 per cent, similar to those coming from African countries. In this study, immigrants from Mexico are grouped with immigrants from the USA (as North Americans). This group (North Americans) reaches a depression rate of 7 per cent. The same study analysed alcohol dependence and found that the highest rates were among Europeans and North Americans. Asians, Africans as well as Latin Americans had lower rates of alcohol dependence. Latin Americans showed lower depression rates and alcohol dependence than the Canadian-born (Ali, 2002; Ali, McDermott & Gravel, 2004).
Risk factors affecting the mental health of Latin American immigrants
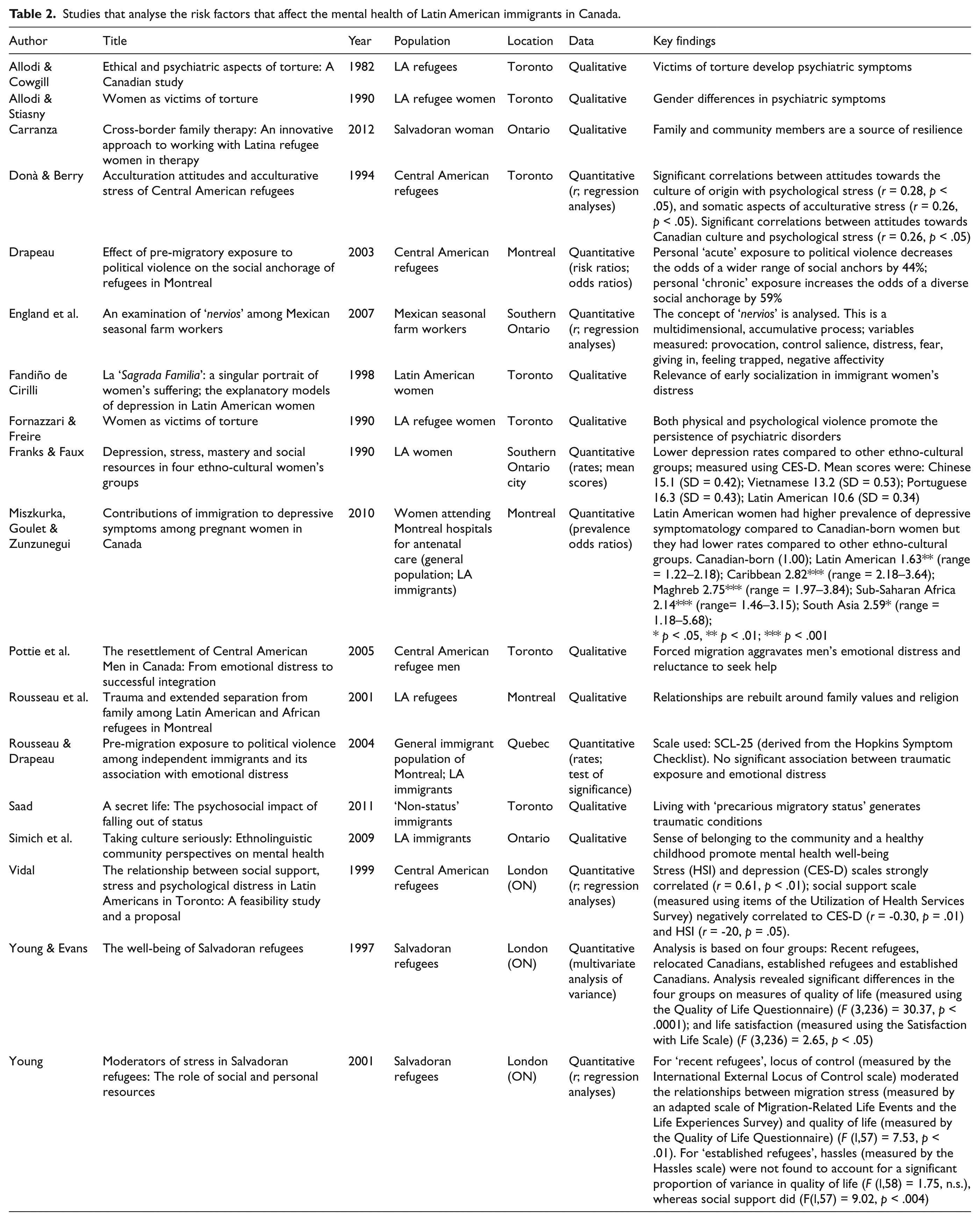
Twelve studies focused on the impact of exposure to political violence in the home country and refugee status as factors that influence the mental health of Latin Americans in Canada (Allodi & Cowgill, 1982; Allodi & Stiasny 1990; Carranza 2012; Donà & Berry, 1994; Drapeau 2003; England, Mysyk & Gallegos, 2007; Fandiño de Cirilli, 1998; Fornazzari & Freire, 1990; Franks & Faux, 1990; Pottie, Belle Brown & Dunn, 2005; Rousseau & Drapeau, 2004; Rousseau, Mekki-Berrada & Moreau, 2001; Saad, 2011; Simich, Maiter, Moorlag & Ochocka, 2009; Vidal, 1999; Young, 2001; Young & Evans, 1997). For example, in examining a group of recently arrived refugees, Allodi & Cowgill (1982) reported psychiatric symptoms, including severe nervousness, insomnia, cognitive or mental function disturbances, depression and suicide ideation.
During the 1990s and early 2000s, as the Central American refugee population grew larger, eight research studies analysed the interrelationships of depression, distress and social and personal resources (Donà & Berry, 1994; Drapeau 2003; Pottie et al., 2005; Rousseau & Drapeau 2004; Rousseau et al., 2001; Vidal, 1999; Young, 2001; Young & Evans, 1997).
A quantitative study reported that stress (measured with items of the Hispanic Stress Inventory) is associated with depression (measured with the CES-D scale) (Vidal, 1999). Results also indicated that higher self-esteem (measured with the Self-Esteem Inventory) (Young, 2001) and better social relationships (measured with items of the Utilization of Health Services Survey) (Vidal, 1999) decrease the impacts of stress and have a positive impact on the mental health of Central American refugees (Vidal, 1999; Young, 2001).
Qualitative results are in line with the quantitative findings as they highlight the relevance of diverse types of resources (social, personal, familial) to protect refugees against mental disorders (Pottie et al., 2005; Rousseau et al., 2001). Table 2 provides a complete summary of the studies that analyse the social factors that affect the mental health of Latin American immigrants in Canada.
Studies that analyse the risk factors that affect the mental health of Latin American immigrants in Canada.
Access and barriers to care and services
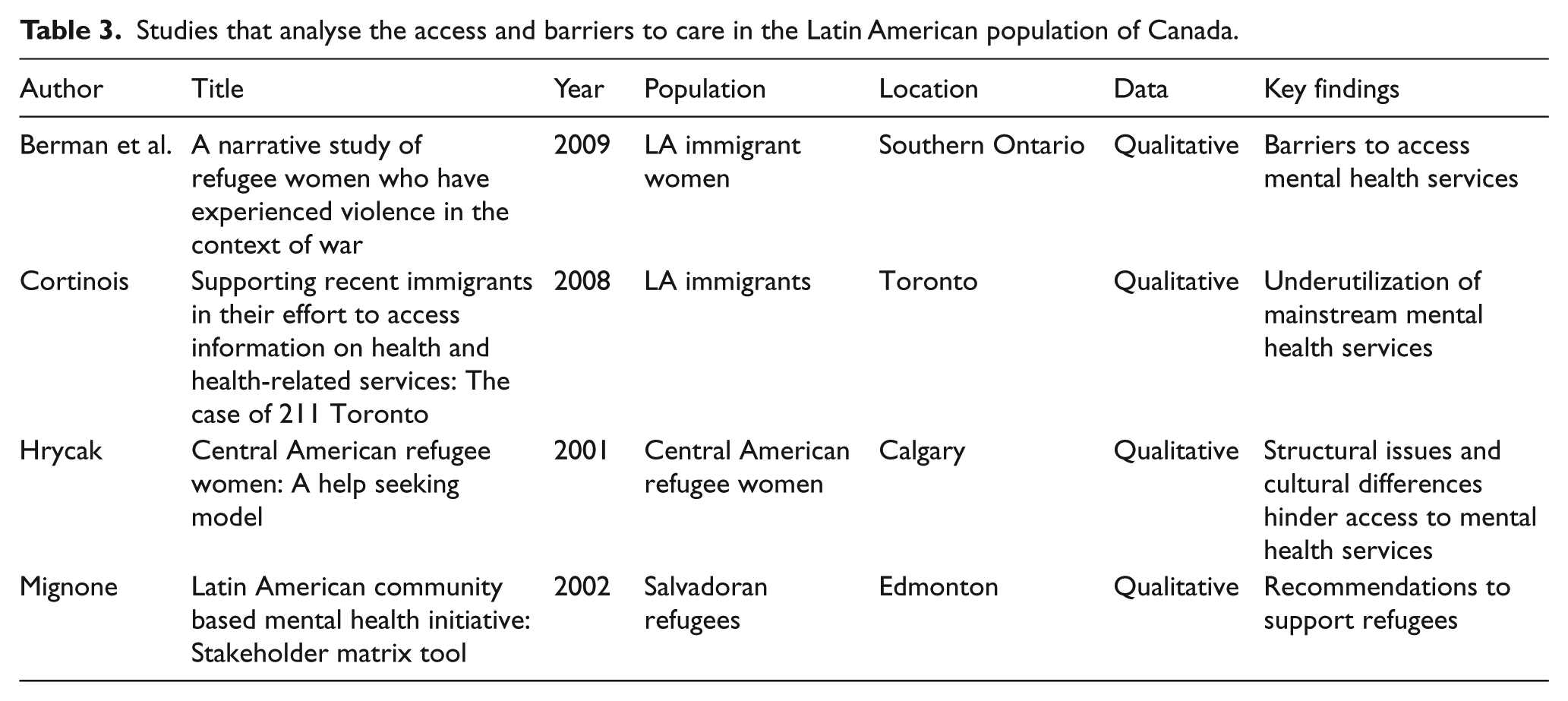
Very few studies analyse the issues that arise when Latin American immigrants have to navigate the mental health care system in Canada (Berman, Giron, & Marroquin, 2009; Cortinois 2008; Hrycak, 2001; Mignone, 2002). These studies, which mostly focus on Central American refugees, indicate the existence of significant clinical challenges for providers of both physical and mental health services. These issues emerge not only as a result of cultural issues such as language barriers and challenges in understanding the health care procedures in Canada (Hrycak, 2001), but also as a consequence of structural problems like racism, marginalization and exclusion (Berman et al., 2009).
Cortinois (2008) notes that Latin American immigrants find it difficult to navigate the health care system in Canada. Challenges include difficulties in finding a family doctor; the perception that consultations are too quick; the perception that providers are not interested in their problems; and long waiting times at health care facilities. In his research, Cortinois (2008) points out that the vast majority significantly underutilized mainstream mental health services. Table 3 provides a complete summary of the studies that analyse the access and barriers to care in the Latin American population of Canada.
Studies that analyse the access and barriers to care in the Latin American population of Canada.
Discussion
This paper presents a review of the literature on the mental health of Latin American immigrants to Canada. The review presented in this paper indicates that the most frequently examined risk factor for mental health issues among Latin American Canadians is displacement, which occurred because of war, political persecution and torture. Twelve out of 18 studies that analyse risk factors focus on this topic; and nine out of these 12 studies analyse Central American refugee populations. A significant part of the studies that address the mental health issues of Latin American immigrants in Canada are at least a decade old and analyse the consequences that individuals face when they have to flee their own country because of war, torture and political persecution. These works, which focus mostly on Central Americans, explore the coping strategies that refugees use to overcome the trauma and distress originated in a war-type environment. The demographic particularities of this wave, including its low educational level, urban poor and rural composition, are well documented (Garay, 2000; Ginieniewicz, 2007). This is relevant as it has been suggested that this demographic structure may have had an impact on individuals’ ability to find and utilize adequate resources to protect their mental health (Vidal, 1999).
Most papers that analyse ‘risk factors’ focus on refugees
Very few studies focus on other groups. For example, two works analyse the distress and fear suffered by Mexican seasonal farm workers (England et al., 2007) and ‘uninsured’ immigrants (Saad, 2011). The fact that these studies are more recent suggests that incipient, novel research is addressing the diversity and complexity of this population.
Overall, there is a lack of studies that relate the mental health of Latin Americans in Canada to key demographic variables like educational attainment, income, employment, length of residence, language proficiency or country of origin. Nowadays, the Latin American population in Canada is very diverse. Prior to the Central American wave, in the 1970s, another relatively small wave of Latin American refugees had arrived in Canada from the Southern Cone. This group was mainly composed of community organizers, intellectuals and professionals involved in politics, who also escaped political violence. Later, in the 1990s and 2000s, another large wave of skilled and well-educated Latin American immigrants arrived in Canada as a result of successive political and economic crises in the region (Ginieniewicz, 2007). This wave also included a significant number of refugees, mainly from Colombia.
The complexity of this heterogeneity has been properly captured in several studies that addressed the political behaviours and patterns of civic engagement in the community (Ginieniewicz, 2010; Goldring, 2006; Schugurensky & Ginieniewicz, 2007b). Nonetheless, the information on the mental health of this heterogeneous and diverse community is still very limited. In fact, the overall results drawn from this review suggest that, given the diversity of the population involved, the category of ‘Latin American’ may be challenged. This is important as assuming homogeneity in such a diverse population may lead to erroneous conclusions.
Data drawn from Statistics Canada’s 2005 Longitudinal Survey of Immigrants to Canada (LSIC) indicate that recent Latin American immigrants are among three groups with the highest levels of stress (Robert & Gilkinson, 2010). But this study is limited in its ability to identify the reasons and consequences of this stress. Earlier studies conducted among Central American refugees in the 1990s in London (Ontario) have suggested that stress is associated with depression and that social resources could moderate this association (Vidal, 1999). However, studies of this kind have yet to be undertaken using larger population-based samples, beyond the refugee group.
Our understanding of the reasons and consequences that link Latin Americans to an array of diagnoses, including anxiety, depression and schizophrenia, is extremely limited.
This review demonstrates that we have limited information on the specific needs, and capacity to access services, of the diverse groups that composed this population. This is crucial as the size and heterogeneity of this population have increased dramatically in the past 10 years (Ginieniewicz, 2010).
Evidence that service utilization is low has been reported, but information regarding the factors that hinder access to care is scant. Knowing in more detail the rates of use and type of help sought by each subgroup would help to map the specific barriers and how to overcome them.
The Latin American population in Canada is no longer composed of a majority of refugees. The diversity of socio-economic statuses, cultural backgrounds and countries of origins of this group indicate that a more precise evaluation of the different subgroups is necessary. Moreover, part of the immigrant population who arrived in the early 1970s may soon be facing the mental health issues that particularly affect senior populations. It may be pertinent to highlight that most of those who comprise the ‘soon-to-be-senior’ population suffered torture and confinement and had to leave their home countries because of political persecution.
New challenges and issues, specifically affecting the 1.5 (those immigrants who arrived in Canada in their childhood or early adolescence) (Schugurensky & Ginieniewicz, 2007c) and second generations, have also started to emerge. For example, the impact of identity issues on the mental health of those raised and socialized both in Canada and Latin America remains unknown. In addition to this, the high rate of school dropout and the consequences on the health of the Latin American youth are generating increasing concern among community members (Schugurensky, 2009; Serrano, 2009).
While relevant to provide a useful framework, findings from the USA cannot be automatically extrapolated to Canada. There is evidence that local context and the reception that immigrants get in a new country are important risk factors to develop mental health problems and illnesses among economic immigrants and refugees (Porter & Haslam, 2005). In addition, Latinos in the USA and Latin Americans in Canada are different. Although it is one of the fastest-growing minorities in the country, Latin Americans in Canada represent a much smaller proportion of the total population than Latinos in the USA. Moreover, in Canada, Latin Americans represent a much younger population. Most Latin American Canadians are first-generation immigrants. Conversely, Latinos have lived for many years in what is nowadays the USA, even before the annexation of Mexican territories in 1848. Unlike in the USA, until the 1990s most Latin Americans arrived in Canada as refugees (Ginieniewicz, 2007). Overall, immigration policies as well as particular social, economic, political and historical developments have made Canada’s approach to immigration unique. Local information on the mental health of the Latin American population in Canada is needed in order to properly inform the development of an equitable health-sector response.
It is relevant to mention that some findings in the literature may be embedded in the text of studies as incidental findings and may not be clearly about Latin Americans. These findings may have not turned up in the searches.
Conclusion
There is little information on the mental health issues that affect Latin American immigrants in Canada beyond the group of Central American refugees. There is a need to know more about what factors currently influence the mental health of this heterogeneous population and their specific barriers to services and care.
Footnotes
Funding
This research was supported by the Social Aetiology of Mental Illness training programme (SAMI). SAMI is a Strategic Training Initiative in Health Research funded by the Canadian Institutes of Health Research at the Centre for Addiction and Mental Health and the University of Toronto.