
Abstract
Background:
The etiology of mental illness has been attributed to many different causes by people of various cultural backgrounds, including supernatural beliefs. This in turn affects the help-seeking behavior. Aim of this study was to explore the supernatural belief and pathways of care in patients with obsessive compulsive disorder (OCD) attending a tertiary care hospital located in north India.
Methodology:
In all, 89 consecutive patients diagnosed with OCD (according to the International Classification of Diseases–10th Revision (ICD-10)) and ≥ 15 years of age were evaluated for their supernatural belief and help seeking.
Results:
More than half of the patients (54%) believed in supernatural causes and 57.3% attributed their illness to supernatural causes. In addition to supernatural causes, many patients also attributed their illness to stress (household/work-related stress) or chemical imbalance in the body and or mind. About two-thirds of the patients (n = 58; 65.2%) first contacted a psychiatrist for their symptoms of OCD. Those who first contacted faith healers believed in one of the supernatural causations.
Conclusion:
Patients with OCD hold multiple beliefs regarding the etiology and treatment of mental illness which can affect their pathways to care.
Introduction
Obsessive compulsive disorder (OCD) is a severe mental disorder with lifetime prevalence rate of 2%−3% (Karno, Golding, Sorenson, & Burnam, 1988). It is associated with a high rate of functional impairment, disability and caregiver burden (Chakrabarti, Kulhara, & Verma, 1993; Grover & Dutt, 2011; Rasmussen & Eisen, 1992; Vikas, Avasthi, & Sharan, 2011). Studies suggest that many patients with OCD either do not seek treatment, or when they seek treatment, it is only after about 7–10 years of onset of symptoms (Fireman, Koran, Leventhal, & Jacobson, 2001; Rasmussen & Eisen, 1992).
Some of the data suggest that patients with OCD often minimize and normalize their first set of symptoms of OCD. According to the patients, their relatives also usually trivialize the occurrences. The lack of knowledge about illness and adequate professional help available has been reported to be a major predictor of delay in treatment seeking in patients with OCD (Beşiroğluet al., 2004; Goodwin et al., 2002).
Pathways of psychiatric care have been defined as the sequence of contacts with individuals and organizations, initiated by the distressed person’s efforts and those of his significant others to seek appropriate help (Rogler & Cortes, 1993). Study of the pathways to care provides information regarding the individual’s health-seeking and illness behavior (Goldberg & Huxley, 1980). First, caregivers constitute the most important part of the psychiatric pathways as this gives a direction to further pathways of care. The delay in seeking treatment is mostly attributed to the choice of the first caregivers (Lincoln, Harrigan, & Mcgorry, 1998). Studies from India and other developing countries which have assessed the pathways of care of patients with different mental disorders suggest that many patients usually consult traditional healers first (Gureje, Acha, & Odejide, 1995; Jain et al., 2012). All these leads to delay in reaching the psychiatric service. Data also suggest that appearance of religious healers in the pathway is associated with greater superstitious beliefs about mental illness (Faizan, Raveesh, & Ravindra, & Sharath, 2012). The main reasons for choosing a particular facility are trust, recommendations by the significant others and belief in supernatural causation of illness (Chadda, Agarwal, Singh, & Raheja, 2001). Few studies from India have specifically evaluated the supernatural beliefs and etiological models held by patients of schizophrenia and their caregivers (Kate, Grover, Kulhara, & Nehra, 2012; Kulhara, Avasthi, & Sharma, 2000; Saravanan, Jacob, Johnson, Prince, & Bhugra, 2007; Srinivasan & Thara, 2001) and pathways to care in patients with psychiatric disorder (Chadda et al., 2001; Lahariya, Singhal, Gupta, & Mishra, 2010; Mishra, Nagpal, Chadda & Sood, 2011; Pradhan et al., 2001). In spite of OCD being a disabling disorder, studies have not evaluated the etiological models and pathways of care in patients with OCD.
Aim
The aim of this article is study the supernatural beliefs and pathways of care in patients with OCD attending the outpatient clinic of a tertiary care center. Additionally, an attempt was made to study the relationship between supernatural beliefs and the first treatment contact.
Methodology
Study setting and sample selection
In all, 89 consecutive new patients attending the outpatient clinic of Department of Psychiatry of a tertiary care hospital in north India (Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh) during the period of July 2011 to December 2011 were recruited. To be included in the study, the patients were required to fulfill the diagnosis of OCD (F42) as per the International Classification of Diseases–10th Revision (ICD-10) and aged ≥ 15 years. Those with comorbid mental retardation and organic brain syndromes were excluded.
The study was approved by the Institute’s Ethics Review Board. Written informed consent was obtained from all the patients prior to recruitment.
Instruments
Supernatural Attitude Questionnaire (patient version)
This scale was designed at our center (Kulhara et al., 2000). It consists of 17 items worded in simple language with ‘yes’ and ‘no’ responses designed to study the individual’s various types of magico-religious beliefs, the role of magico-religious beliefs in the causation of mental illness/behavioral abnormalities and the role of treatment based on such beliefs. Various items of the questionnaire are based on commonly prevalent magico-religious beliefs in our society. One item in the questionnaire evaluates the role of stress in the development of mental illness, and another item evaluates the understanding of patients with respect to the role of change in neuro-chemicals in the brain as the etiology of mental illness. According to this questionnaire, the term ‘supernatural beliefs’ is used to cover the commonly held cultural beliefs thought to influence the individual’s mental and physical health. The term ‘supernatural beliefs’ was used as an umbrella term to cover commonly held beliefs like sorcery, evil spirit, spirit intrusion, divine wrath, planetary/astrological influences and past deeds, and so on.
Pathway to care
Pathways to care were assessed by self-designed questionnaire. By using a semi-structured interview, patients and their caregivers (wherever available) were asked about their help seeking for symptoms of OCD. The duration of treatment in each health-care facility they had contacted was also enquired, and the sequence of contact with different agencies was prepared.
Statistical analysis
Data were analyzed using SPSS-14 (Statistical Package for the Social Sciences, 2005, Chicago, IL, USA). Means and standard deviations were calculated for continuous variables and frequencies, and percentages were calculated for discontinuous variables. Chi-square test, t-test and Mann–Whitney U test were used for comparisons. Association between different variables was studied by using Pearson’s product moment correlations and Spearman’s rank correlation.
Results
Sociodemographic and clinical profiles
The study included 89 patients. The mean age of the participants was 29.24 years (standard deviation (SD) = 9.54), and the mean number of years of education was 13.36 years (SD = 3.5). About two-thirds of the patients included in the study were male (n = 58; 65.2%) and one-third were females (n = 31; 34.8%). Nearly equal proportions of patients were married (n = 44; 49.5%) and single (n = 45; 50.5%). Slightly more than half of the patients belonged to nuclear families (56.2%). About three-fifths of patients were Hindus (59.25) and two-thirds (67.45) were residing in urban locality.
Most of the patients (n = 85; 95.5%) were diagnosed to have OCD, mixed thoughts and acts, and only four (4.5%) patients had diagnosis of OCD, predominantly obsessions. The mean duration of illness was 73.39 months (SD = 91.82).
In all, 42 (47.2%) patients had comorbid psychiatric illness. Most common psychiatric comorbidity was of depressive disorders (n = 25; 21 had single episode of depression and 4 had recurrent depressive disorder), followed by anxiety disorders (n = 11). Three patients had comorbid bipolar affective disorder and one patient had comorbid psychotic disorder.
About one-fourth of the patients (23.6%) had already received one adequate anti-obsessional trial (adequate dose of an selective serotonin reuptake inhibitor/serotonin reuptake inhibitor for at least 12-week duration), one-tenth (10.1%) had received two anti-obsessional medication trials and seven (7.9%) patients received three anti-obsessional medication trials, prior to the current consultation. About one-fourth (n = 21; 23.6%) were treatment naive at the time of recruitment.
Pathways to care
First contact agency
As is evident from Table 1, about two-thirds of the patients (n = 58; 65.2%) first contacted a psychiatrist for their symptoms of OCD. One-sixth (n = 15; 16.9%) of the patients first contacted a physician (including the registered medical practitioners), whereas another one-sixth (n = 16; 18%) contacted faith healers and other traditional healers for their symptoms of OCD.
Agency of first contacts.

OPD: outpatient department; PGIMER: Postgraduate Institute of Medical Education and Research.
Pathways of care when first contact is with psychiatrist in government setup
In our study, 12 patients had first contact with a psychiatrist in government hospital. Out of these 12 patients, 8 patients had second contact with our facility. Four patients had one contact with other helping agencies (2 patients contacted a faith healer and 2 patients contacted an exorcist) before reaching to our center. The pathways for these patients are shown in Figure 1.

Pathways of care when first contact is with psychiatrist in government setup.
Pathways of care when first contact is with psychiatrist in private setup
In all, 33 patients had first contact with a psychiatrist in private setup, out of which for 20 patients contact with our facility was the second place of consultation. Seven patients had contact with one helping agency, five patients had contact with two helping agencies, and two patients had contact with three helping agencies before reaching our center. The pathways for these patients are shown in Figure 2.
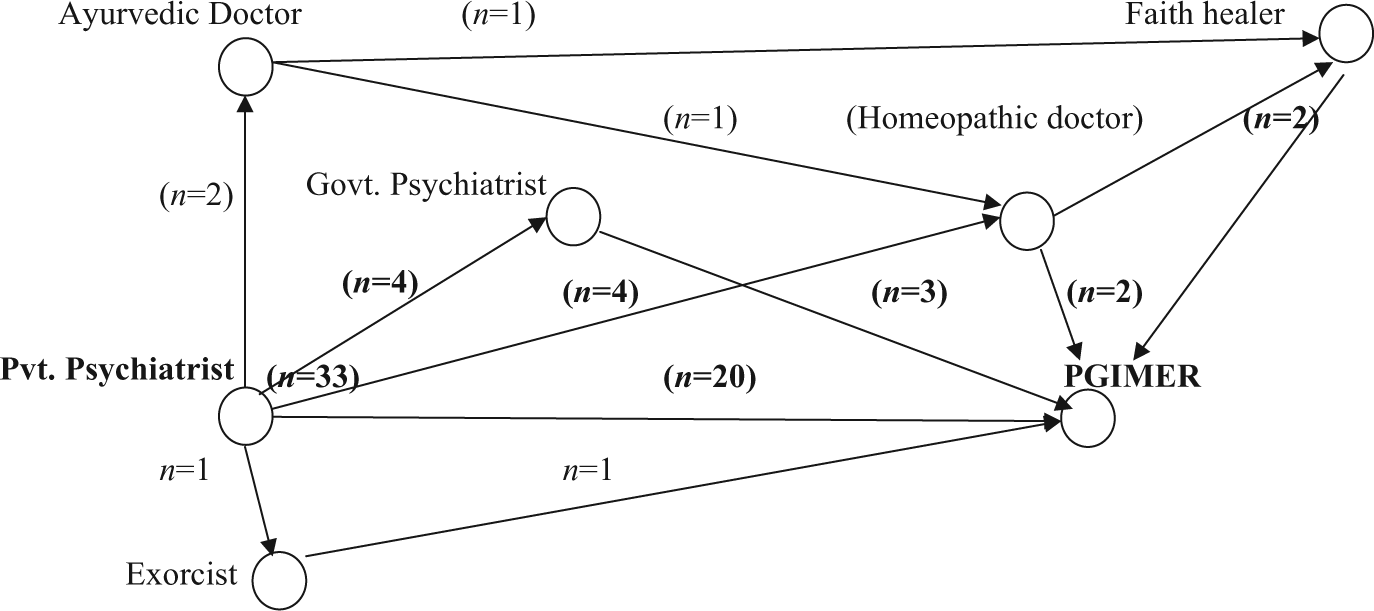
Pathways of care when first contact is with a psychiatrist in private setup.
Pathways of care when first contact is with a private physician
In all, 12 patients had first contact with private physicians. Out of the 12 patients, 3 patients directly came to our center. Four patients had one contact with other helping agency, five patients had two contacts, and one patient had four contacts before coming to our center. The pathways for these patients are shown in Figure 3.

Pathways of care when first contact is with a physician.
Pathways of care when first contact is with a physician in government setup
Three patients had first contact with general physicians in government hospitals. Out of which two patients directly came to our center. One patient had one contact with Ayurvedic doctor before coming to PGIMER.
Supernatural belief of the patients
Personal supernatural beliefs
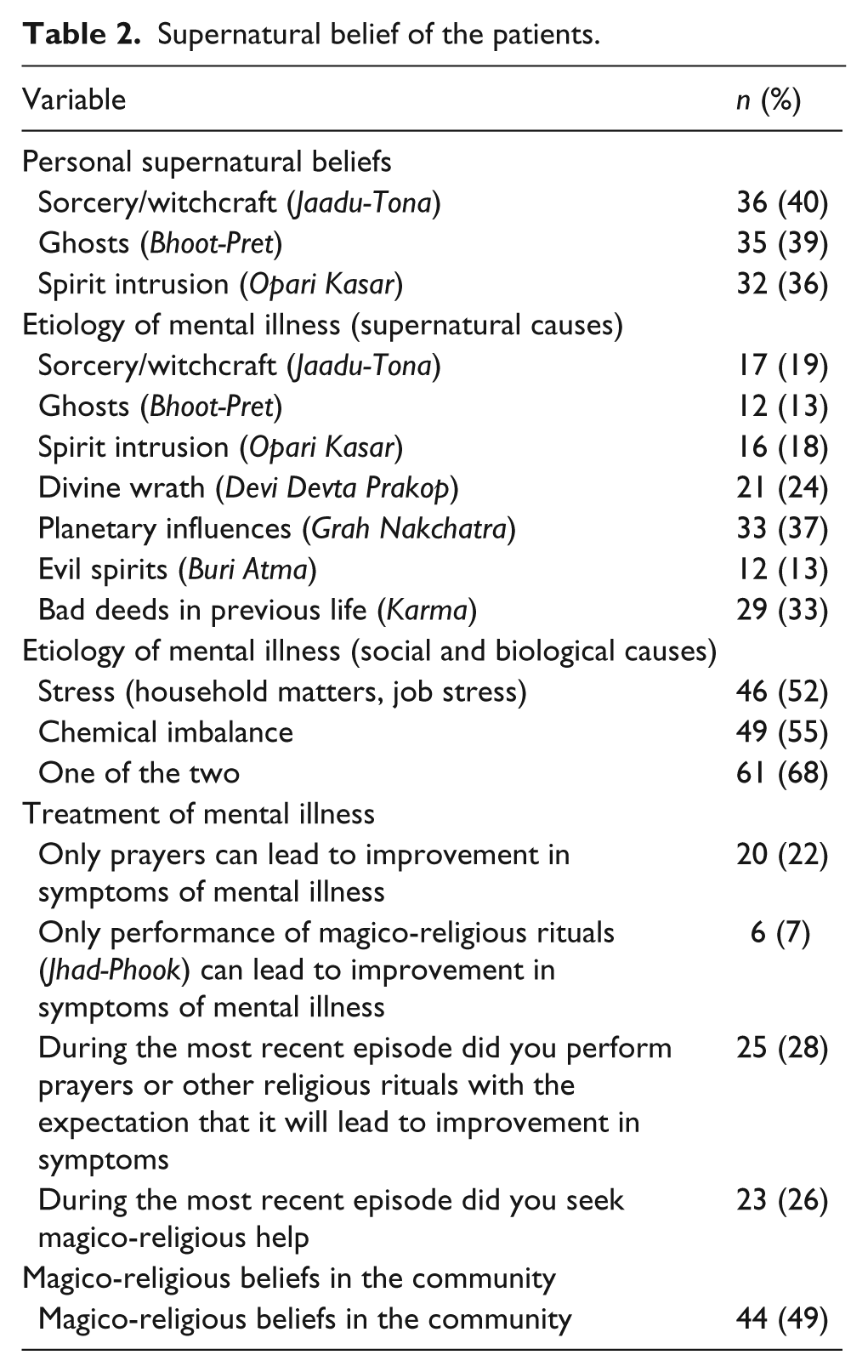
Out of 89 patients, 41 (46.06%) patients did not have any of the supernatural beliefs. A total of 36 (40.4%) patients believed in sorcery/witchcraft (Jaadu-Tona), 35 (39.3%) patients believed in ghosts/evil spirits (Bhoot-Pret) and 32 (36%) patients believed in spirit intrusion (Opari Kasar). Overall, 31 (34.8%) patients had more than one supernatural beliefs (Table 2).
Supernatural belief of the patients.
Etiological models of OCD as held by patients
The most common supernatural cause to which the patients attributed their OCD was planetary influences (n = 33; 37.1%). This was followed by bad deeds in previous life (Karma) (32.6%), divine wrath (Devi Devta Prakop) (23.6%), sorcery/witchcraft (Jaadu-Tona) (19.1%) and spirit intrusion (Opari Kasar) (18%).
In all, 21 (23.6%) of the patients attributed their symptoms of OCD to one supernatural cause, six (6.7%) patients attributed their symptoms to two supernatural causes, and 24 (26.96%) patients attributed their symptoms to three or more supernatural causes. A substantial proportion of patients (42.7%) did not attribute their symptoms to any of the supernatural causes.
A total of 46 (51.7%) patients believed that their mental illness could be due to any type of stress (household/work-related stress), and 49 (55.1%) patients felt that mental illness was due to chemical imbalance in the body and or mind. When both these factors were taken together, slightly more than two-thirds (n = 61; 68.5%) of the patients attributed their symptoms of mental illness to either of these causes, with 34 (38.2%) patients attributing the illness to both. However, slightly less than one-third (n = 38; 31.5%) of the study sample did not consider that their symptoms were due to either stress or chemical imbalance.
Beliefs about treatment and help-seeking behavior
In all, 20 patients (22.5%) considered that offering prayers only was sufficient for treatment of their symptoms of OCD. Few patients (n = 6; 6.7%) considered that performing magico-religious rituals only was sufficient for management of their symptoms of mental illnesses. In all, 25 (28.1%) patients actually performed prayers during the most recent episode to get rid of their symptoms, and 23 (25.8%) patients or their family members had gone to faith healers to perform magico-religious rituals during the most recent episode of illness. A total of 17 (19.1%) patients both performed prayers and also sought help from faith healers. In all, 44 (49.4%) patients admitted that their neighbors and people in their society also held these beliefs.
Relationship between supernatural beliefs of patients and sociodemographic and clinical variables
Significantly more number of patients from urban area believed in ghosts (chi-square value = 4.159*; p = .04), and more patients with comorbid psychiatric illness believed that their mental illnesses were due to sorcery/witchcraft (chi-square value = 7.22; p = .007), planetary influences (chi-square value = 7.22; p = .05), evil spirits (chi-square value = 4.3; p = .038) and chemical imbalance (chi-square value = 6.29; p = .012).
Those who believed that their mental illness could be affected by bad deeds in previous life had significantly longer duration of illness than those who did not believe in the same (Mann–Whitney U = 609.5; p = .022). Those who believed that their mental illness could be due to stress had higher number of years of education (M = 14.07; SD = 3.2) than those who did not believe (M = 12.6; SD = 3.6), and this difference between the two groups was significant (t value = 2.00; p = .048). There were significant differences in patients’ income between the groups who believed and who did not believe that chemical imbalance to be the cause of mental illness (Mann–Whitney U = 573.5; p = .004) with significantly higher income for those who considered chemical imbalance to be responsible for the symptoms.
Relationship between sociodemographic variables, clinical variables and supernatural beliefs with first treatment contact
Based on the first treatment contact, the study group was divided into three groups, that is, those who choose to seek treatment from a psychiatrist as first contact (i.e. those who first contacted a psychiatrist in government hospital, private clinic or those who came directly to our psychiatry outpatient clinic), those who first sought treatment from a physician (government/private sector) and those who first contacted faith healers and other traditional healers. As is evident from Table 3, higher proportion of those who first visited faith healers believed in spirit intrusion and sorcery/witchcraft. Higher proportion of those who first contacted faith healers and traditional healers attributed their symptoms to sorcery/witchcraft, ghosts, spirit intrusion, divine wrath, planetary influences and evil spirit. However, there was no difference in attribution of symptoms to other causes like stress and chemical imbalance, and in the beliefs and acts of performance of prayers and religious rituals among those seeking their first treatment from different settings.
Relationship of supernatural beliefs of patients and first treatment contact.

PGIMER: Postgraduate Institute of Medical Education and Research.
Discussion
A better understanding of the way in which people understand and seek care for mental disorders is important for planning mental health services, for the organization of training and for the organization of referrals to psychiatrists from other sources of health and social care (Fujisawa et al., 2008). Medical educators also need teaching and learning approaches and philosophies that consider health attributions, beliefs and practices of patients (Vaughn, Jacquez, & Baker, 2009). Keeping this in mind, it is important to understand the beliefs and the help-seeking behavior of patients with severe mental disorder, like OCD, which is highly prevalent, associated with high rate of functional impairment, disability and caregiver burden (Chakrabarti et al., 1993; Grover & Dutt, 2011; Rasmussen & Eisen, 1992; Vikas et al., 2011). However, in our literature search, we could not find any study addressing this issue in relation to OCD. Hence, this study was a preliminary attempt to fill this void.
Findings of this study suggest that about one-fifth (18%) of the patients choose to contact faith healers as their first treatment contact. Additionally, another 12% went to faith healers/exorcists after the first contact with the psychiatrist/physicians. Furthermore, with regard to supernatural beliefs, findings of this study suggest that 54% had faith in supernatural beliefs and about 47% attributed their OCD to supernatural causes. Additionally, the findings of this study suggest that most patients have multiple etiological models for their mental illness and the number of etiological models increase with the presence of comorbid psychiatric disorders.
As there are no previous studies from India and other parts of the world, which have specifically looked at the pathways of care and etiological models of patients with OCD, we would try to compare the findings of this study with some of the existing literature that have evaluated these parameters in patients with other psychiatric disorders.
There is lack of consensus with regard to first treatment contact in studies from India, with some reporting that psychiatrists are the most common first treatment contact (Chadda et al., 2001; Mishra et al., 2011), whereas others have reported that faith healers are the most common first treatment contact (Lahariya et al., 2010). The findings are possibly influenced by the major diagnostic group and sociodemographics like percentage of participants from urban or rural locality. One of the recent studies compared the pathways of care and faith in supernatural beliefs in two samples of patients with schizophrenia, one belonging to a private psychiatric center at New Delhi and the other from a government medical college at Bilaspur in the state of Chhattisgarh, and it was reported that there was wide variation in the attribution of illness to supernatural forces at the two centers, with significantly higher prevalence in those from Chhattisgarh. However, there was not much difference in the faith healers being the first contact of treatment, although at both the centers the first contact with faith healer exceeded 50% (Naik, Pattanayak, Gupta, & Pattanayak, 2012).
Findings of this study support the existing literature which describes that psychiatrists are the most common first treatment contact (Chadda et al., 2001; Mishra et al., 2011). Various explanations can be proposed for higher rate of first contact with psychiatrists. First, compared to other disorders, OCD in general is considered to be a disorder with biological underpinnings. Second, compared to the past, over the years, the number of mental health professionals available at different places across the country has increased; hence, it is quite possible that this could have impact on the first treatment contact. Third, possibly this may also be a reflection of reduction in stigma attached with mental illnesses. Fourth, compared to other disorders, in general, treatment of OCD involves pharmacotherapy and behavior therapy, which are provided only by the mental health professionals, and physicians and other professionals are in general reluctant to treat patients with OCD. Hence, it is quite possible that this information is available to the sufferers from various sources, and therefore, they prefer to have psychiatrists as the first treatment contact. This is also reflected by the fact that a reasonably high proportion of patients contacted our tertiary care facility which provides services for behavior therapy, which are at times not available with all the private psychiatrists.
Our findings also support the notion that belief in supernatural forces as etiological factors for mental illness is quite prevalent among people in India (Kate et al., 2012; Kulhara et al., 2000; Naik et al., 2012; Saravanan et al., 2007), which was the same in patients with OCD and those reported for schizophrenia and other disorders in the literature from India (Kate et al., 2012; Kishore et al., 2011; Kulhara et al., 2000; Naik et al., 2012; Saravanan et al., 2007) and other countries (Kua et al., 1993). Findings of this study also suggest that beliefs in certain supernatural causes also influence the first treatment contact. These findings suggest the knowledge about the psychiatric illnesses is poor in India, and there is an urgent need to clarify the cultural myths associated with mental illnesses. Furthermore, there is a need to sensitize the non-psychiatrist physicians, faith healer and other non-allopathic doctors about the need of early identification, timely referral and proper management of various mental health problems. This will possibly help in reducing the delays in treatment, improving the prognosis and reducing the cost of treatment (Mishra et al., 2011). As only few studies have used the same scale to assess the culturally held beliefs, we would like to compare the findings of OCD with other studies based on the same scale. When we compare the findings of this study with those with schizophrenia (Kate et al., 2012), it is evident that significantly lesser proportion of patients with OCD attributes their illness to sorcery/witchcraft. However, the beliefs in other domains do not appear to differ much. Studies which have evaluated patients with depression by using other scales (Grover et al., 2012) also suggest attribution of depression to similar kind of beliefs in nearly equal proportion of patients as those with OCD seen in this study. One study from eastern India that included 120 patients with different illnesses evaluated the etiological beliefs and help-seeking behavior of patients with mental illnesses, which also included 10 patients with OCD and other anxiety disorders and 26 patients with dissociative disorders. This study showed that high proportion of patients with any psychiatric disorder, including OCD and dissociative disorders attributed their illness to supernatural causes, and there was no significant difference in proportion of patients attributing their mental illness to supernatural causes (Chakraborty et al., 2013). Taken together, these findings suggest that beliefs in supernatural causes may not be disorder specific per se. Possibly, these beliefs are more culturally entrenched and are attributed to all mental illnesses per se.
In this study, majority of the patients expressed that OCD could be due to any type of stress (51.7%) or chemical imbalance (55.1%). Additionally, many patients had more than one etiological model, including supernatural causes, stress and chemical imbalance. The multiple etiological models in the patients can be understood from various perspectives. First, to start with, many patients have supernatural etiological models or do not have any specific etiological model. Second, with repeated treatment contact, possibly due to some knowledge provided by the psychiatrists and physicians, patients become aware about the role of stress and OCD being a biological disorder due to chemical disturbances in the brain. Third, although the patients become aware of the biological nature of the illness, they are not able to leave their original etiological model, possibly due to lack of benefit from the biomedical model of treatment. This is reflected by the fact that a significant proportion of patients do consult faith healers or physicians of non-allopathic school of thoughts like Ayurveda or homeopathy.
Findings of this study also suggest that certain supernatural beliefs are associated with certain sociodemographic and clinical variables like higher prevalence of beliefs in ghosts in those from urban background and less likely attribution of illness to chemical imbalance and stress among those with lower income and education. These findings suggest that sociodemographic variables have important influence on the etiological models and should be taken into account while evaluating patients with OCD and while providing psychoeducation.
Although the study included consecutive patients, the findings should be interpreted in the light of the fact that the study sample was relatively small. Furthermore, the study included only those patients who were attending outpatient clinic of a tertiary care center and the findings cannot be generalized to community setting. We also did not evaluate the referral patterns from different types of care providers to psychiatrists. We also did not evaluate the influence of family members and significant others in choosing the treatment facility. We also did not look at the fact that some of the patients might be following advice of more than one care provider. The study did not include a control group, which could have helped to compare the findings of patients with OCD with those without any mental or physical illness living in the community. Future studies must attempt to overcome the limitations of the study by recruiting more number of OCD patients drawn from general population.
To conclude, this study demonstrates that most of the patients with OCD seek treatment from psychiatrist as the first source of contact and nearly half of them do not believe in supernatural causes as the etiological factors responsible for their OCD. More than half of the patients attribute their illness to stress and chemical imbalance. However, a reasonable proportion of patients believe in supernatural causation, which influences help seeking. Hence, there is an urgent need to address the knowledge and beliefs about mental disorders in the community, so that this will lead to better recognition and management of OCD. The clinicians managing the patients with OCD should specifically evaluate the beliefs about causes and treatments in patients with OCD and should clarify the misattributions to supernatural causes. This can, in the long run, lead to improved treatment adherence and outcome.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.