
Abstract
Background:
The shortage of specialized human resources in mental health in Bangladesh requires active recruitment of psychiatric residents. In addition, the involvement of positively inclined health personnel, for example, medical doctors, emerges as an immediate priority.
Aim:
To explore stigma among medical students toward persons with mental disorders (PMDs) and their attitudes toward psychiatry.
Method:
A cross-sectional study was conducted at Faridpur Medical College in Bangladesh before (First year) and following psychiatric rotation (Fifth year). Students (N = 200) filled anonymous questionnaires measuring stigma toward PMDs and attitudes to psychiatry.
Results:
Upper medical school year (p = .028), older age (p = .005), mother’s lower academic level (p = .043), upper and lower socioeconomic level affiliation (p = .008) and self-consultation for mental or neurological complaints (p = .032) were associated with increased stigma toward PMDs. More favorable attitudes toward psychiatry were found in upper medical school year (p = .073) and were significantly associated with female gender (p = .018) and middle socioeconomic level affiliation (p = .013).
Conclusion:
The relative improvement in attitudes toward psychiatry in the upper medical school year is overshadowed by the increased stigma toward PMDs. Specific anti-stigma program in the curriculum and strategies to improve the attitudes are required.
Introduction
Worldwide, 12-month prevalence rates of mental disorders are relatively high, ranging from 8.4% to 29.1% (World Health Organization (WHO) International Consortium in Psychiatric Epidemiology, 2006). Equally high is the treatment gap, defined by the difference between the true and the untreated prevalence. The gap ranges from 32.2% to 78.1% according to the type of disorder, methods and region of the world (Kohn, Saxena, Levav, & Saraceno, 2004). Bangladesh, a lower–middle income country, according to the World Bank classification, shares this world condition. A recent nationwide study showed that about 16.1% of the adult people were diagnosed with mental disorders (Firoz, Karim, Alam, Rahman, & Zaman, 2006), and of them, a small rate (approximately 32 per 100,000 people) sought help from psychiatric facilities (WHO and Ministry of Health & Family Welfare, 2006). For schizophrenic disorders, Lora et al. (2012) estimated a 97% treatment gap.
Also, the treatment lag, the time elapsed from disorder onset to reaching specialized care, was found wide. The median delay from disease onset to reaching any caregiver was 4.0, 24.5 and 14.5 weeks, for depressive, anxiety and psychotic symptoms, respectively (Giasuddin, Chowdhury, Hashimoto, Fujisawa, & Waheed, 2012). Importantly, this study (Giasuddin et al., 2012) also showed that 84% of the service users in Bangladesh consulted other caregivers before seeking help from a mental health professional (MHP).
Bangladesh is not up to facing the above-noted mental health challenges. For example, the country has one of the lowest rates of psychiatrists and other MHPs in the world, about 0.5 MHPs (0.07 psychiatrists) per 100,000 population (WHO and Ministry of Health & Family Welfare, 2006). While the need to increase the number of psychiatrists is obvious, it is unlikely that this will occur in the immediate future. As a result, the general health sector is called in to fill the vacuum. The implementation of such strategy requires that the primary care practitioner receive appropriate training during and after medical school. Following training, medical students, our study population, should be expected to be better informed and more able to overcome the widely spread public mental health stigma. This stigma does not skip health professionals (Hussain, Mohit, Alam, Ahmed, & Rabbani, 2008; Qusar, 2010; Sartorius, 2002; Tasman & Mohr, 2011). Of note, medical students’ attitudes to psychiatry influence their future professional practice, such as the response to their patients’ psychological problems as well as their recruitment into the specialty (Feifel, Montier, & Swerdlow, 1999; Samimi, Noroozi, & Mottaghipour, 2006). (Parenthetically, Bangladeshi doctors, who are also working abroad, may be carrying along the stigmatized attitudes and practices from their homeland.)
Public mental health stigma is widespread in Asia (Lauber & Rössler, 2007). Despite geographical distance, the beliefs about the causes of mental disorders and the attitudes toward persons with mental disorders (PMDs) in Asian countries have more commonalities with Western countries than there are differences (Lauber & Rössler, 2007). Ironically, the public acceptance of modern views in different places of the world about mental disorders is coupled with a stubborn persistence of negative opinions, attitudes and behaviors (Pescosolido, Medina, Martin, & Long, 2013). As noted above, the health professionals are not free from stigma toward PMDs (Lawrie et al., 1998; Ücok et al., 2006) and may behave negatively toward a service user once a psychiatric diagnosis is suspected (Magliano et al., 2011; Sartorius, 2002). Indeed, focus group studies found that PMDs receive less attention and care from family physicians and other health care providers because of stigma (Pinfold, Byrne, & Toumlin, 2005; Schulze & Angermeyer, 2003).
Stigma toward PMDs and attitudes to psychiatry have been found associated with many variables, such as socioeconomic conditions (Braunholtz, Davidson, Myant, & O’Connor, 2007), quality of living conditions (Economou, Richardson, Gramandani, Stalikas, & Stefanis, 2009; Tabuchi, Fukuhara, & Iso, 2012), knowledge about mental illness (Corrigan & O’Shaughnessy, 2007), familiarity with PMDs (Corrigan, Green, Lundin, Kubiak, & Penn, 2001), personal or family experience with mental disorder and contact with PMD (Corrigan et al., 2001; Corrigan & O’Shaughnessy, 2007; Holmes, Corrigan, Williams, Canar, & Kubiak, 1999), parental attitudes (Scheff, 1966) and the culture of affiliation (Korszun, Dinos, Ahmed, & Bhui, 2012; Pescosolido et al., 2013). With regard to medical students, for example, age (Al-Ansari & Alsadadi, 2002), gender (Al-Ansari & Alsadadi, 2002; Alexander & Eagles, 1986; Korszun et al., 2012), contact with PMD (Korszun et al., 2012), academic year (Ay, Save, & Fidanoglu, 2006) and rotation through psychiatry (Ay et al., 2006; Holm-Petersen, Vinge, Hansen, & Gyrd-Hansen, 2007; McParland, Livingston, & McManus, 2003) also were found to influence stigma and attitudes formation. As a result, factors that precede medical training, if they enhance stigma, may hinder potential advances to be achieved by medical training and, conversely, if the latter is not well conceived and conducted, it may further increase pre-medical school negative attitudes.
Objectives
To examine stigma toward PMDs and attitudes toward psychiatry among medical students in Bangladesh at their pre- (first year) and post-rotation (fifth year) in psychiatry, and selected variables associated with those outcomes.
Methods
Sample
This study was conducted at the state-run Faridpur Medical College, one of the 70 medical schools in the country. This 5-year school has a total of 635 students. It is situated at about 145 km from Dhaka, the capital city. The students are selected through a nationwide common admission process. In this study, we included first and fifth year students. The latter were recruited after completion of the set of lectures and 5-week psychiatry ward teaching.
All the students of the respective medical school years of Faridpur were included. The acceptance to the invitation to participate was almost complete, 100 of the 107 students in first year, and 100 of the 101 enrolled in fifth year (N = 200). The few students who were not available during the survey or dropped out from the academic year were excluded. The first year students made up the pre-exposure group, and the fifth year students made up the post-exposure intervention group. Anonymous information was obtained from all participants. A brief, non-biasing description of the survey was made prior to handing over the self-administered questionnaires. The study was approved by the College Ethical Review Committee.
Measures
It comprised three instruments: (1) On sociodemographic variables (age, gender, permanent address, marital status, parents’ education, family’s socioeconomic status (SES), academic year, previous consultation for mental/neurological complaints (by the respondent, family members or friends) and media exposure to psychiatric issues). (2) The 26-item ‘Modified Corrigan Attribution Questionnaire’ (MCAQ), that was constructed after the ‘Attribution Questionnaire-27’ (AQ-27) (Corrigan, Markowitz, Watson, Rowan, & Kubiak, 2003), was used to assess stigma toward psychiatric illness. The MCAQ provides a brief vignette about Hasib, a 30-year-old single man with schizophrenia who lives alone and works as a clerk at a large private firm. He had been hospitalized six times because of his illness. We selected a vignette depicting a service user with schizophrenia because in Bangladesh, it is the general doctor who is entrusted with the care as a result of the lack of dedicated psychiatric services. One question from the original questionnaire was deleted: ‘If I were in charge of the treatment of Hasib, I would force him to live in a group home’, since this service option is unavailable in the country. The responses were given on a 0–9 Likert scale, where 0 meant full rejection and 9 meant full approval. The responses of each subject were summed into a total score (range: 0–234), where higher score denoted higher level of stigma. The scale had good internal reliability (Cronbach’s alpha = .71). (3) The 31-item ‘Modified Balon Attitudes Questionnaire’ (MBAQ), which was used to assess attitudes toward psychiatry. Our version included three questions that differed from the original questionnaire (Balon et al., 1999): ‘Because my fellow students or other friends will laugh at me if I select psychiatry, I would not go into it even if I am well paid’; ‘I think the psychiatric hospital is not a place to treat patients’; and ‘To me, all psychiatrists are strange people’. One question, ‘With few exceptions, clinical psychologists and social workers are just as qualified as psychiatrists to diagnose and treat emotionally disturbed persons’ was omitted, due to their unavailability in the services. The responses were given on a 1 (strongly disagree) to 4 (strongly agree) Likert scale. The responses of each subject were summed into a total score (range: 31–124), where higher score denoted more favorable attitudes toward psychiatric issues. A few items were scored in the reverse direction. The scale showed good reliability (Cronbach’s alpha = .79).
Both the MCAQ and MBAQ were translated from the original English version into Bengali by expert translators, and back-translated by another group. Subsequently, they were compared with the original versions, and necessary corrections were made. Whenever there was doubt regarding the most appropriate Bengali term, expert opinions from senior psychiatrists were obtained.
Data analysis
Associations between medical school year, MCAQ and MBAQ were tested using t-tests and Pearson correlations. Following the bivariate association tests, we examined background and exposure variables as possible confounders of the associations between school year and MCAQ and MBAQ scores. Background variables were gender, permanent address (urban, rural), marital status (married, unmarried), father’s and mother’s educational level (lower, higher) and family’s SES (upper, middle, lower). Exposure variables were consultation for mental or neurological complaints by self, family or friends, and media exposure. Since the variables did not show an association with both school year and MCAQ or MBAQ scores, we tested the effects of the variables showing associations with questionnaires’ scores in separate analysis of variance (ANOVA) models, each including the background/exposure variable and medical school year. We used SPSS (Statistical Package for Social Sciences, 20th version) for Windows (IBM Corporation, New York) to analyze the data.
Results
The sociodemographic characteristics of the students, exposure to psychiatry-related issues through texts and visual media and previous contact with a caregiver for mental or neurological complaints are presented in Table 1. Associations with medical school year were noted with regard to age only (t = 36, df = 198, p < .001).
Medical students by sociodemographic characteristics and exposure to psychiatric issues.
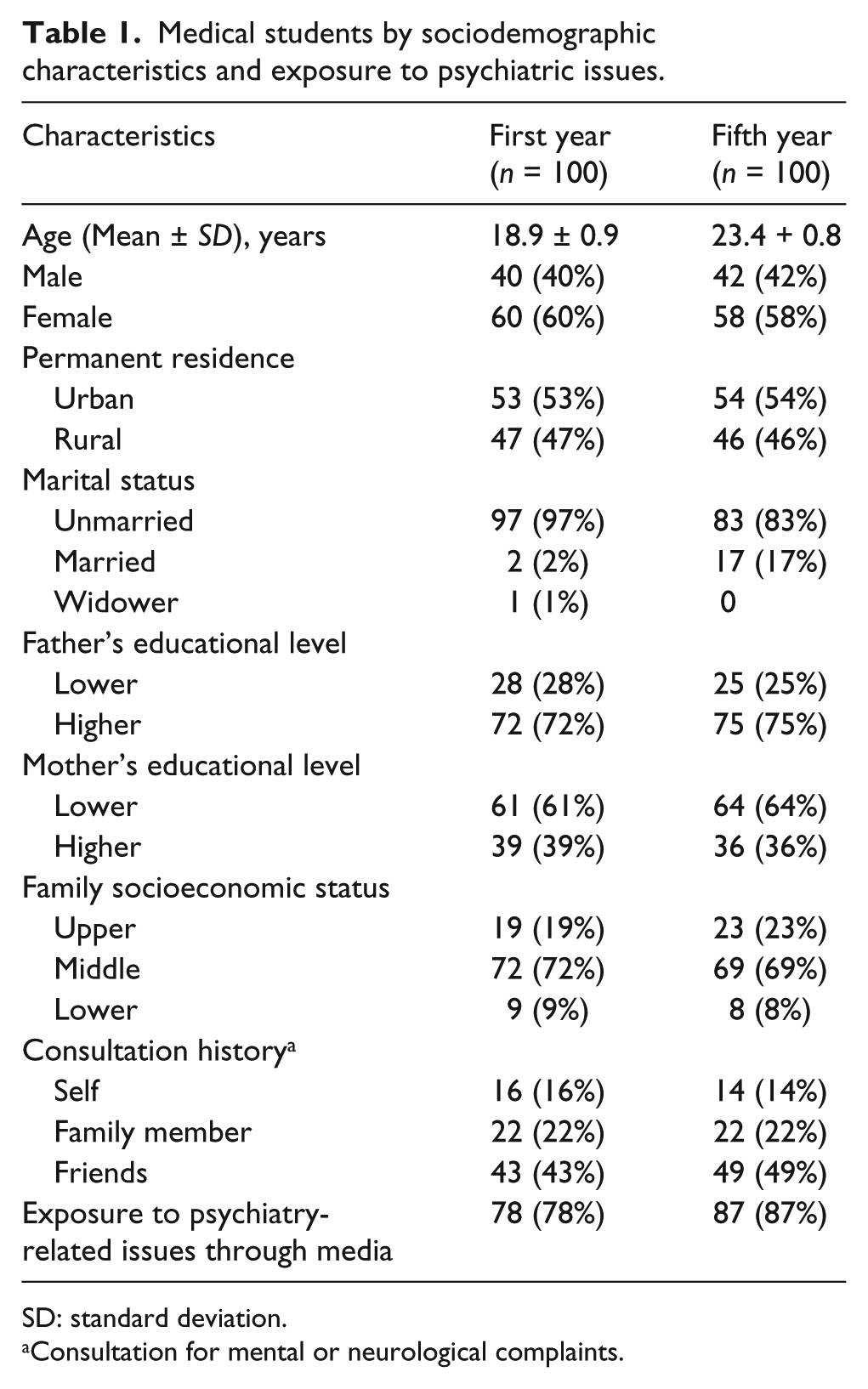
SD: standard deviation.
Consultation for mental or neurological complaints.
Higher level of stigma toward PMDs as indicated by MCAQ scores was shown by fifth year (119.8 ± 22.8) compared to first year (113 ± 2.1) students (t = 2.21, df = 198, p = .028). In addition, slightly more favorable attitudes to psychiatry as indicated by MBAQ scores were shown by fifth year (98.8 ± 11.5) compared to first year (96.2 ± 8.7) medical students (t = 1.81, df = 198, p = .073).
A positive correlation was found between students’ age and MCAQ score (r = .20, p = .005). No association was found between age and MBAQ scores (r = −.11, p = .11). Significant associations with MCAQ were found for mother’s education and SES. Students who reported lower mothers’ education showed higher MCAQ scores (stigma) compared to those reporting higher education (Table 2). The 2 × 2 ANOVA indicated a main effect of mother’s education (F = 4.13, df = 1,196, p = .043), but not mother’s education by school year interaction (p = .7). In addition, higher MCAQ scores were observed among students of both lower and upper compared to middle SES. The 2 × 3 ANOVA indicated a main effect of SES (F = 4.90, df = 2,194, p < .01), but not SES by school year interaction (p = .7).
Multivariate ANOVA findings on factors associated with MCAQ and MBAQ scales.
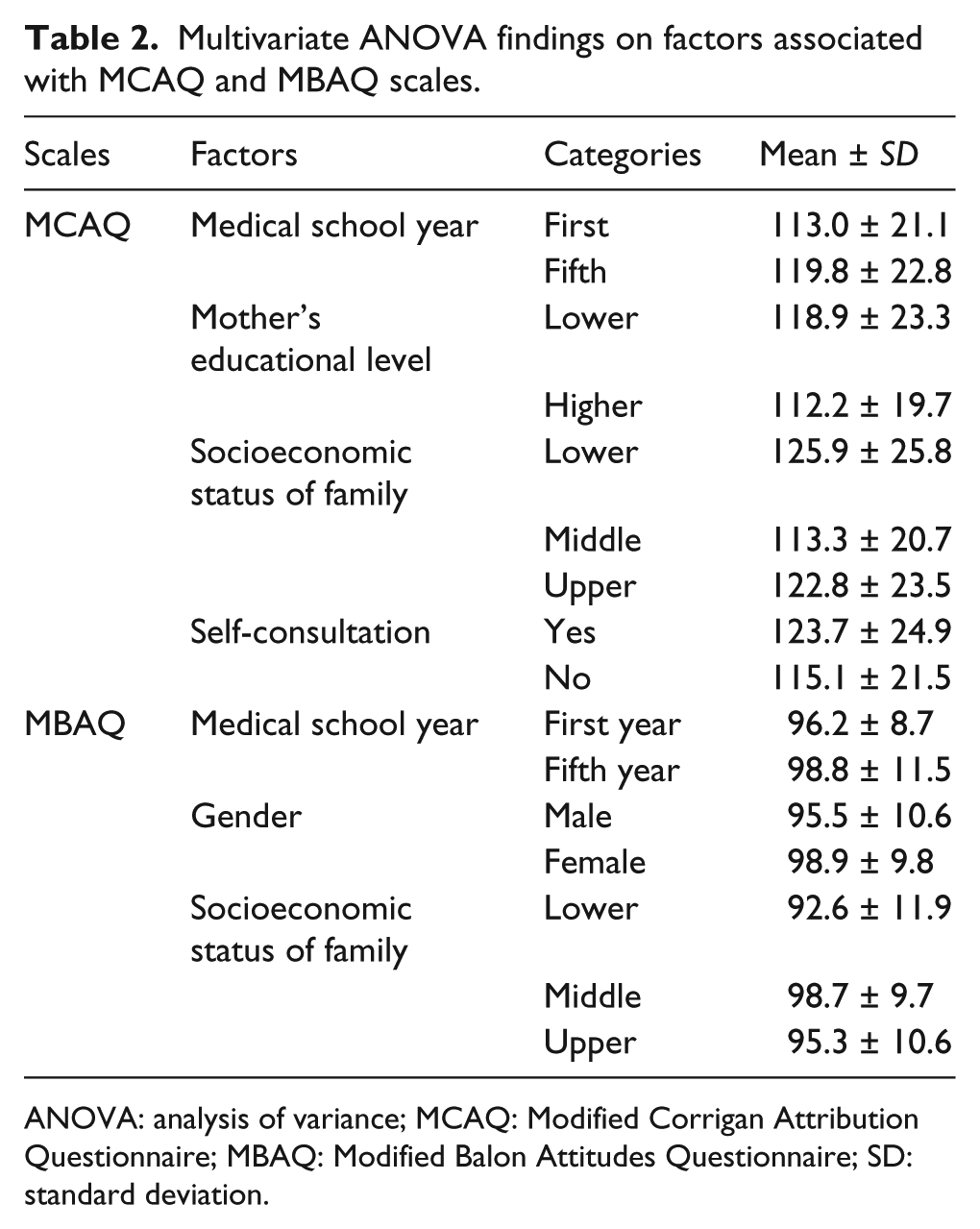
ANOVA: analysis of variance; MCAQ: Modified Corrigan Attribution Questionnaire; MBAQ: Modified Balon Attitudes Questionnaire; SD: standard deviation.
Significant associations with MBAQ scores (attitudes) were found for gender and SES. Women showed higher MBAQ scores compared to men (Table 2). The 2 × 2 ANOVA showed a main effect of gender (F = 5.69, df = 1,196, p = .018), but no gender by school year interaction (p = .17). While at fifth year middle SES was associated with higher MBAQ scores compared to both lower and upper status, no such difference was seen in first year medical students. The 2 × 3 ANOVA showed a main effect of SES (F = 4.44, df = 2,194, p = .013), as well as a SES by school year interaction that approached significance (F = 2.96, df = 2,194, p = .054).
MCAQ scores (stigma) were significantly higher among students that consulted a care provider for mental or neurological complaints (F = 4.66, df = 1,196, p = .032) (Table 2). In contrast, no association was found between MBAQ scores (attitudes) and self-consultation (F = −1.09, df = 1,196, p = .3). No significant associations were found between MCAQ scores and consultation history by family (F = 0.01, df = 1,183, p = .9) or friends (F = 0.62, df = 1,145 p = .4). Similarly, MBAQ scores regarding family and friend consultation were not significant (F = 1.02, df = 1,183, p = .3; F = 2.96, df = 1,145 p = .088, respectively).
With respect to media exposure, no significant difference were observed with MCAQ (F = 0.01, df = 1,191, p = .9) or MBAQ scores (F = −0.26, df = 1,191, p = .6) between students who were and were not exposed to text or visual media regarding psychiatry-related issues.
Discussion
This study measured two important constructs with regard to mental health care, stigma and attitudes to psychiatry, both pre- and post-exposure to the respective rotation of medical school students. Both constructs influence the choice of psychiatry as a field of practice and, more generally, mental health–related practice among the primary care doctors and other specialists. Several factors were associated with stigma (age, mother’s educational level, SES, self-consultation and, importantly, year of study) and the attitudes to psychiatry (gender, SES and year of study). Students whose mothers have lower academic level and those from lower and upper socioeconomic levels showed increased level of stigma. Stigma toward PMDs was significantly higher in those students who consulted for themselves for mental or neurological complaints, a possible result of self-stigma and/or negative treatment experience.
With regard to attitudes to psychiatry, female students and students from middle socioeconomic level showed more favorable attitudes. More specifically to the effect of the medical studies, we found that the exposure to training increased stigma, but improved attitudes to psychiatric issues slightly. It seems that the first year medical students carry into their cycle of studies the stigmatic attitudes toward PMDs originated in their home environments (Firoz et al., 2006; Qusar, 2010). Ours does not constitute a single finding in the literature: increase in stigma toward PMDs was seen after completion of training in psychiatry in Greece (Economou, Peppou, Louki, & Stefanis, 2012) and Turkey (Ay et al., 2006). Increased level of stigma in higher academic year was observed also in Italy (Magliano et al., 2011). Conceivably, the increase in stigma may result from the quality/nature of the psychiatry curriculum, the attitudes of the teaching staff and the site and scope of training. The identification of these and other possible factors calls for further studies. Improved attitudes toward psychiatry following rotation or training in psychiatry was observed in Malawi (Platt, Beaglehole, Baig, Leuvennink, & Eagles, 2010), Spain (Bulbena, Pailhez, & Coll, 2005), the United Kingdom (Baxter, Singh, Standen, & Duggan, 2001) and Portugal (Xavier & Almeida, 2010). As Pescosolido et al. (2013) stated, a stubborn persistence of negative opinions, attitudes and behaviors seems to intermingle with the considerable acceptance of the modern medical views of mental disorders.
As found elsewhere (Lyons, 2013), psychiatry showed limited capacity to attract students – too few of them expressed interest to specialize in psychiatry. To compound the problem, a large number of them work outside the country; the number of psychiatrists enrolled in the United Kingdom and the United States currently totals (n = 149) almost equal to the number working in native Bangladesh (Jenkins et al., 2010). Thus, the national cadre of specialists (WHO and Ministry of Health & Family Welfare, 2006) may remain small. In parallel, the reliance on non-specialized medical staff to care for PMDs, as promoted by WHO (2008), may face attitudinal obstacles that need to be carefully addressed. Hopefully, by doing so, the mhGAP (Mental Health Gap Action Program) efforts of the WHO (2008) to upgrade the quality of care of mental health problems provided by general physicians will be facilitated. At the same time, we need to involve and empower the PMDs and caregivers in the treatment process to deliver acceptable, affordable and quality services that are evidence-based, as rightly noted by the anonymous reviewer.
The study has a few limitations. The sample was taken from only one medical school. However, the participant students came from a common intake process established for all medical schools, and the institution where the study was conducted does not differ much from all other schools in both academic settings and facilities. Another limitation may derive from the translation of the MCAQ and the MBAQ. However, the validation of the back-translated version reduced the amount of disparity with the original versions to a minimum. The case vignette described in MCAQ referred to a specific mental health scenario only, schizophrenia, limiting its ability to generalize to all cases of mental disorders. Also, the respondents faced a hypothetical situation in the case vignette which may not anticipate their actual behavior in real-life situation. Important strength of the study is the high response rate achieved through the assurance of total anonymity, an assurance that was fully honored.
Conclusion
As elsewhere, we found that the stigma toward the PMDs, often found among all medical students, increased following the psychiatric rotation. The recommendations for change are simple to formulate but, perhaps, less easy to attain them. In addition to seminars on the etiology, course and patterns of recovery from psychiatric disorders, well-tailored activities to decrease stigma are required. For example, joint rounds with other medical specialties are advisable to highlight the interaction between mental and physical disorders. It is necessary to encourage and give proper remuneration to the psychiatrists to attract them to this profession and to prevent the draining of specialists to high-income countries like the United Kingdom or Australia. Contact with persons who have recovered from psychiatric disorders or are living with the illness may improve students’ attitudes toward psychiatry and PMDs. At all times, students need to be made aware of the destructive impact of stigma on the lives of the PMDs, and on the doctor–user relationship. Up to now, the undergraduate medical curriculum in Bangladesh does not have any specific anti-stigma training component. This deficit has to be met, and its changes monitored and evaluated.
Footnotes
Appendix 1
Acknowledgements
The publication is the shortened form of thesis submitted at Nova University of Lisbon, Portugal, for completion of International Master’s in Mental Health Policy and Services of the first author (N.A.G.). The authors express gratitude to the first and fifth year students of the study duration for their time to complete the responses.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.