
Abstract
Background:
In routine clinical practice, the subcategories of various somatoform disorders are rarely used by the primary care physicians and there is lack of data to suggest any difference in the clinical manifestations of these subcategories.
Aim:
To compare the symptom profile, anxiety, depression, alexithymia, somato-sensory amplification and hypochondriasis of patients with persistent somatoform pain disorder with other subtypes of somatoform disorder.
Method:
A total of 119 patients diagnosed with somatoform disorders according to the International Classification of Diseases–10th Revision (ICD-10) were evaluated for prevalence of somatic symptoms, anxiety, depression, alexithymia, hypochondriacal worry and somato-sensory amplification.
Results:
No significant differences were found in the prevalence of various somatic complaints between those with persistent somatoform pain disorder group and those diagnosed with other somatoform disorders. Co-morbid anxiety and depression were seen in two-thirds of the patients, but again there was no difference in the prevalence of the same between the two groups. Similarly, no significant differences were found on alexithymia, hypochondriasis and somato-sensory amplification scales between the persistent somatoform pain disorder group and the group with other somatoform disorders.
Conclusion:
There are no significant differences between the various subcategories of somatoform disorders with regard to the prevalence of somatic symptoms, anxiety or depression and psychological correlates of alexithymia, hypochondriasis and somato-sensory amplification.
Introduction
Somatization is a universal phenomenon across all the cultures, with presentation of somatic symptoms being influenced by the psychological, social and ethnic factors (Kirmayer & Sartorius, 2007; Kirmayer & Young, 1998). Somatization has been viewed as the psychological distress which presents as physical complaints that are considered to be more acceptable for the sufferer and significant others in their cultural context (Escobar & Gureje, 2007; Kirmayer & Robbins, 1991). Current nosological system classifies somatoform disorder as somatization disorder, undifferentiated somatoform disorder, hypochondriacal disorder, somatoform autonomic disorder, persistent somatoform pain disorder, other somatoform disorders and somatoform disorder (unspecified) (as defined in The ICD-10 Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research; World Health Organization, 1993). These different categories are based on the duration of symptoms, predominant type of symptoms, associated help-seeking behaviour and so on. Furthermore, there is little evidence to suggest any treatment specificity of these various categories of somatoform disorder, except perhaps for the hypochondriacal disorder (Ghanizadeh & Firoozabadi, 2012).
Patients with various somatoform disorders form a major proportion of patients seen in primary care (Kroenke, 2003). They also form a major proportion of patients seeking help in various medical and surgical clinics, and it is suggested that one-third to two-thirds of patients attending general medical clinics do not receive any biomedical explanations for their symptoms (Nimnuan, Hotopf, & Wessely, 2001). Existing literature suggests that various diagnostic subcategories of somatoform disorder are less commonly used by the primary care physicians because of the overlapping nature in the symptom composition (Gureje, 2004; Simon, Von Korff, Piccinelli, Fullerton, & Ormel, 1999). The existing literature is also not sufficient to suggest the validity of each subcategory of the somatoform disorder (Starcecic, 2006). There is also lack of data with regards to the comparison of symptom profile and psychological correlates of various symptoms in patients with various forms of somatoform disorders (Dimsdale, Sharma, & Sharpe, 2011; Starcecic, 2006). Studies from primary care also suggest significant symptom overlap and co-morbidity between the symptoms of somatoform disorders, anxiety disorders and depression (Gureje, 2004; Simon & Gureje, 1999; Simon et al., 1999).
Due to all these factors, researchers have questioned the validity of physical symptom counts in defining somatoform disorders (Mayou, Kirmayer, Simon, Kroenke, & Sharpe, 2005). There has been emphasis on assessment of somatic symptoms from a dimensional perspective, taking into consideration symptom perception and attribution, bodily preoccupation, doctor–patient interaction, personality traits, and illness-related attitudes and behaviour (Duddu, Issac, & Chaturvedi, 2006).
In this background, this study aimed to (1) examine the prevalence of various somatic symptoms, anxiety and depression in patients diagnosed with various subtypes of somatoform disorders; (2) study the psychological correlates in the form of alexithymia, hypochondriacal worry and somatoform sensory amplification in patients diagnosed with various subtypes of somatoform disorders; and (3) compare the symptom profile of patients with persistent somatoform pain disorder with other subtypes of somatoform disorder.
Methodology
The study was carried out at the Department of Psychiatry of the Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, which is a multispecialty teaching tertiary care hospital providing service to a major area of North India. This department is a general hospital psychiatric unit with both inpatient and outpatient facilities. Many of the patients evaluated in the various medical and surgical outpatient departments after being evaluated thoroughly for medical–surgical problems are referred to this department for psychiatric consultation.
For this study, all the patients were recruited after obtaining written informed consent. The ethical clearance for the study was obtained from the Institutional Review Board.
The study sample comprised consecutive patients attending the walk-in-clinic of psychiatry outpatient department during the period of March 2012 to July 2012. All the consenting patients aged ≥ 18 years who received a diagnosis of any subcategory of somatoform disorder according to International Classification of Diseases–10th Revision (ICD-10; World Health Organization, 1993) based on a semi-structured interview conducted by a qualified psychiatrist were included in the study. However, those with co-morbid mental retardation, organic brain syndromes and psychotic disorder were excluded.
Instruments
The following instruments were used:
Screening for Somatoform Symptoms (SOMS; Rief, Hiller, & Heuser, 1997): This is a screening questionnaire for the identification of persons with somatoform disorders based on the criteria of Diagnostic and Statistical Manual for Mental Disorders–Fourth Revision (DSM-IV) and ICD-10. The questionnaire includes all 33 physical complaints of the DSM-IV somatization disorder symptom list, ICD-10 somatization disorder and somatoform autonomic dysfunction disorder. The validity and reliability of the tool has been found to be good. As per the instrument of the symptom checklist, the subjects are asked whether they have experienced any of the listed physical symptoms during the last 2 years, which had a significant influence on them for which the doctors were unable to find a sufficient explanation. Adding the number of positive responses provides a severity index known as somatization index. For this study, this symptom checklist was translated and back translated to Hindi by bilingual experts. Patients were asked to complete the same.
Beck’s Depression Inventory (BDI; Beck, Ward, & Mendelson, 1961): This is a 21-item self-reporting scale of depression used to assess severity of depression. A score of 10–18 indicates mild depression, 19–29 suggests moderate depression and 30–63 is indicative of severe and very severe depression. This scale has good reliability and validity. For this study, the Hindi version of the scale, which is available, was used.
Generalized Anxiety Disorder scale (Spitzer, Kroenke, Williams, & Lowe, 2006): The seven-item Generalized Anxiety Disorder (GAD-7) scale is a brief screening tool for assessing generalized anxiety disorder. The responses are rated on a four-point Likert scale with ‘not at all’, ‘several days’, ‘more than half the days’, and ‘nearly every day’ scored as 0, 1, 2 and 3, respectively. The total score ranges from 0 to 21. The scale is sufficiently sensitive to differentiate generalized anxiety disorder from panic disorder, social phobia, and post-traumatic stress disorder. The internal consistency (Cronbach’s α = .92) and test–retest reliability are good (intraclass correlation = .83). For this study, this symptom checklist was translated and back translated to Hindi by bilingual experts.
Toronto Alexithymia Scale (TAS; Bagby, Parker, & Taylor, 1994): This is a self- rated scale to assess alexithymia. The scale has 20 items, each item is rated on five points, with total score ranging from 20 to 100. The items are further subgrouped into three factors, namely, difficulty in identifying feelings and distinguishing them from bodily sensations (TAS factor 1), difficulty in describing feelings to others (TAS factor 2) and externally oriented thinking (TAS factor 3). The scale has a Cronbach’s α score of .89, indicating high internal consistency. It has been translated into Hindi with adequate internal consistency and good test–retest reliability (Pandey, Mandal, Taylor, & Parker, 1996).
Somato-Sensory Amplification Scale (SSAS; Barsky, Wyshak, & Klerman, 1990): This scale was used to assess the somato-sensory amplification. It is a 10-item self-reporting scale which measures the subject’s sensitivity to a range of normal bodily sensations and to neutral and noxious stimuli. The response is recorded on a Likert scale ranging from ‘not at all’ (rated as 1) to ‘extremely’ (rated 5) characteristic of respondent in general. Test–retest reliability of this scale is .79 (p = .0001) and the internal consistency is .82 (Cronbach’s α). For this study this symptom checklist was translated and back translated to Hindi by bilingual experts.
Whitely Index (WI; Pilowsky, 1967): This is a 14-item self-rating scale to assess the hypochondriacal worries. The WI total score is the sum of all the positively answered items. The test–retest reliability of WI is .81 (p < .001). For this study, this symptom checklist was translated and back translated to Hindi by bilingual experts.
All the patients diagnosed with somatoform disorder by a qualified psychiatrist were approached for participation into the study. They were explained about the nature of the study. Those who provided written informed consent were requested to complete the self-rated questionnaires, namely, BDI, TAS-20, SSAS and WI. Those who were not able to complete the questionnaires on their own were provided assistance by the clinicians, clinical psychologist or a psychiatric social worker.
Statistical analyses
Statistical analyses were performed using the Statistical Package for the Social Science Version 14. Descriptive analyses were computed in terms of mean and standard deviation with range for continuous variables and frequency with percentage for ordinal and nominal variables. Correlation analysis was done for the inferential analysis. Comparisons were done by using Chi-square test, t-test, Mann–Whitney U test and Fisher exact test.
Results
During the study period of 4 months and 2 weeks, 3,064 new patients were evaluated in the psychiatry outpatient, of whom 114 were less than 18 years of age. Of the total eligible subjects, 249 were diagnosed with different somatoform disorders by a qualified psychiatrist. Of these, 137 patients could be approached for informed consent, of which 123 patients provided informed consent and were recruited for the study. However, four patients did not complete all the assessments for the study. Resultantly, the final study sample was of 119 patients.
Persistent somatoform pain disorder was the most common diagnosis, given to more than half of the participants (N = 64; 54%); this was followed by the diagnostic category of undifferentiated somatoform disorder (n = 23; 20%), hypochondriacal disorder (n = 14; 12%), somatization disorder (n = 12; 10%) and somatoform autonomic dysfunction (n = 3; 3%), which was the least common specific diagnosis. Three cases were diagnosed to have other unspecified somatoform disorders. For comparison purpose, all the categories other than persistent somatoform pain disorder were clubbed together.
Socio-demographic profile
The mean age of the study sample was 37 (standard deviation (SD) = 11) years. More than half of the sample comprised females (59%). Majority of the participants were married (87%) and two-thirds of them came from rural background (67%). More than half of the participants were educated beyond 10th standard (55%), were not on paid employment (60%) and came from non-nuclear families (55%). Two-thirds of them were from rural background (67%) and three-fourths (76%) of the participants were Hindus. When those with persistent somatoform pain disorder were compared to those with other somatoform disorders, both the groups did not differ on any of the socio-demographic parameters.
Clinical profile
The mean age of onset of illness of the whole study sample was 32 years (SD = 10.3) and mean duration of illness was 61 (SD = 62) months. Co-morbid psychiatric disorder was seen in more than one-third of subjects (40%); a co-morbid substance use disorder was present in around one-tenth of study participants and about one-sixth (17%) of the study participants had a co-morbid physical disorder (but this was insufficient to explain the somatic symptoms). Almost all the participants (90%) had consulted a physician prior to their psychiatric consultation and more than half (56%) had consulted faith healers. Only two-fifths (41%) of the study participants acknowledged that their somatic symptoms may be of psychological origin. About three-fifths (59%) of the participants had a history of self-medicating themselves with pain killers. One-fifth (22%) had a history of self-medicating themselves with benzodiazepines. Most of the participants (86%) had undergone physical investigations for their current symptoms. With regard to expectations from treatment, three-fifths (60%) expected the psychiatrists to suggest further investigations and three-fourths (77%) expected that they would be prescribed medications. Participants with persistent somatoform pain disorder did not differ from those with other somatoform disorders on any of the above-described clinical parameters.
Profile of somatic symptoms
The frequency of each somatic symptom as reported on the SOMS is shown in Table 1. The five most commonly reported symptoms were headache (81%), excessive tiredness on mild exertion (81%), pain in legs and/or arms (78%), bloating (74%) and backache (73%). The mean number of somatic complaints in the study participants were 17 (SD = 8). Participants with persistent somatoform pain disorder did not differ from those with other somatoform disorders on the prevalence of various symptoms, except for the lower prevalence of low appetite (χ2 = −4.0; p = .046), frequent diarrhoea (χ2 = −4.7; p = .029), loss of libido (χ2 = −8.5; p = .004). Furthermore, compared to those with other somatoform disorders, female patients with persistent somatoform pain disorder had higher prevalence of irregular menses (χ2 = −9.1; p = .003) and excessive menstrual bleeding (χ2 = −4.0; p = .046).
Prevalence of somatic symptoms as assessed on screening for somatoform disorders (SOMS).
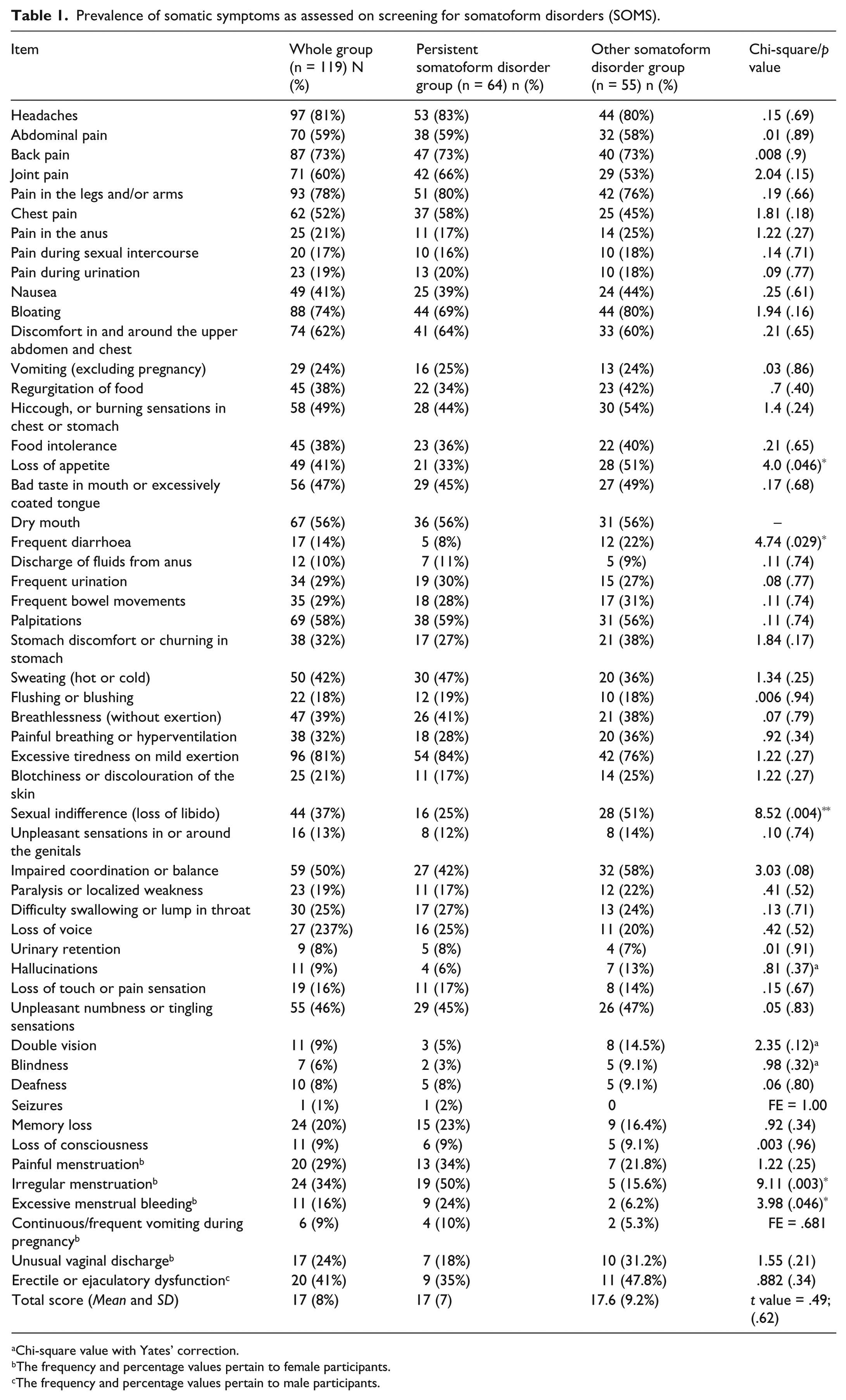
Chi-square value with Yates’ correction.
The frequency and percentage values pertain to female participants.
The frequency and percentage values pertain to male participants.
Level of anxiety, hypochondriasis, alexithymia and somato-sensory amplification
As shown in Table 2, the mean GAD-7 score of the study subjects was 11 (SD = 4; range = 0–19). A total of 75% of participants scored above the cut-off score of 10, which was used for identifying cases of generalized anxiety disorder, with two-thirds (66%) of the participants scoring in the range of moderate levels of anxiety (GAD-7 score of 10–14) and 8% scoring in the range of severe anxiety (GAD-7 score of 15–19).
Comparison of the persistent somatoform pain disorders with other somatoform disorders on scales of alexithymia, somato-sensory amplification, anxiety and depression.
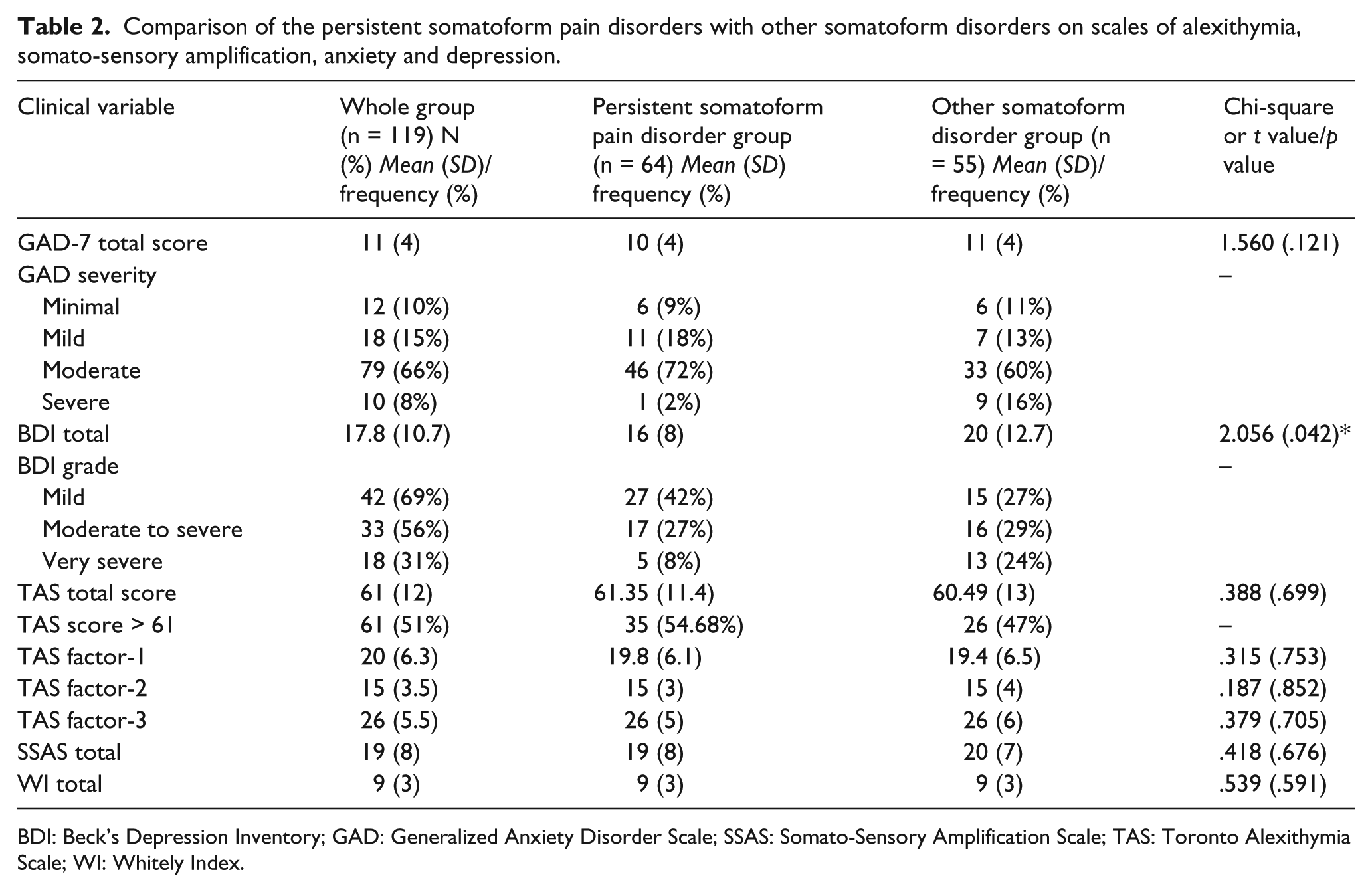
BDI: Beck’s Depression Inventory; GAD: Generalized Anxiety Disorder Scale; SSAS: Somato-Sensory Amplification Scale; TAS: Toronto Alexithymia Scale; WI: Whitely Index.
The mean BDI score of study subjects as whole group was 18 (SD = 11) with mild depression in one-third subjects (n = 42; 35%), moderate to severe depression in slightly more than one-fourth participants (n = 33; 27.7%) and very severe depression in 15% of subjects (n = 18; 15%). The mean BDI score of those diagnosed with persistent somatoform pain disorder was 16 (SD = 8) and with other somatoform disorders was 20 (SD = 13), with a significant difference between the two groups on total BDI score (t value = 2.06; p = .042).
The mean TAS-20 score for the study sample was 61 (SD = 12) and nearly half of the study participants (51%) scored above the cut-off score for alexithymia (TAS-20 total score of > 60). With regard to the subscales of TAS-20, the mean score for the domain of ‘difficulty in identifying feelings’ was 20 (SD = 6), 15 (SD = 3.5) for the domain of ‘difficulty in describing feelings’ and the mean score for the domain of ‘externally oriented thinking’ was 26 (SD = 5.5). The mean scores on WI and SSAS were 9 (SD = 3) and 19 (SD = 8), respectively.
TAS-20 total score and scores on the three subscales of TAS-20, total WI, total SSAS and GAD-7 did not differ between those with persistent somatoform pain disorder and those with other somatoform disorders.
Correlation analysis for whole study group
A significant positive correlation (Pearson’s product moment correlation) was found between the total SOMS score and the total BDI score (Pearson’s correlation coefficient = .36; p < .001), GAD-7 (Pearson’s correlation coefficient = .23; p = .014), total SSAS score (Pearson’s correlation coefficient = .290; p = .001) and total WI score (Pearson’s correlation coefficient = .34; p < .001), suggesting that patient who reported more somatic symptoms had more of anxiety, depression, excessive somato-sensory amplification and hypochondriacal worries. No correlation was found between the total SOMS score and total score of TAS-20 and three subscales of TAS-20. SOMS total score had no correlation with age at onset and total duration of illness.
Correlation for persistent somatoform pain disorder group and other somatoform disorders group
For the persistent somatoform pain disorder group, a significant positive correlation was found between the total SOMS score and the total BDI score (Pearson’s correlation coefficient = .4; p = .001) and total SSAS score (Pearson’s correlation coefficient = .25; p = .048). For the group with other somatoform disorders significant positive correlations were seen between total SOMS score and total BDI score ((Pearson’s correlation coefficient = .33; p = .014); TAS factor 1, that is, ‘difficulty in identifying feelings’ (Pearson’s correlation coefficient = .27; p = .047); TAS factor 2, that is, ‘difficulty in describing feelings’ (Pearson’s correlation coefficient =.28; p = .041); total SSAS score (Pearson’s correlation coefficient = .34; p = .011); total WI score (Pearson’s correlation coefficient = .45; p = .001); and total GAD-7 score (Pearson’s correlation coefficient = 35; p = .009).
Discussion
Although somatic symptoms are common, none of the studies have evaluated the diagnostic validity of various subtypes of somatoform disorders as described in ICD-10. The current study aimed at examining the prevalence of various somatic symptoms, level of anxiety and depression in subjects with somatoform disorders. It also attempted to assess the psychological correlates in the form of alexithymia, hypochondriacal beliefs and somato-sensory amplification in patients with somatoform disorders. The symptom profile and the psychological correlates of patients with persistent somatoform pain disorder were compared with those of patients with other categories of somatoform disorders. The basic aim was to come up with a symptom profile and psychological correlate profile which can help in distinguishing various subtypes of somatoform disorders.
In this study, there was no significant difference on the various socio-demographic parameters of patients diagnosed with persistent somatoform pain disorder or other categories of somatoform disorders, suggesting that the patients with various subcategories of somatoform disorder do not differ from each other on various socio-demographic variables.
In our study sample, too many patients with various somatoform disorders had co-morbid psychiatric disorders. The prevalence of co-morbid psychiatric disorders was more when assessed on rating scales compared to evaluation by the qualified psychiatrist. This finding over-emphasizes the fact that although the rating scale may be sensitive in identifying co-morbid disorders, these are not as specific as clinician evaluation. However, it is important to note that the prevalence of various co-morbid disorders in our study sample is within the reported range in literature (Fink, Hansen, & Oxhoj, 2004; Henningsen, Zimmermann, & Sattel, 2003; Lowe et al., 2008; Toft et al., 2005; Wollburg, Voigt, Braukhaus, Herzog, & Lowe, 2013). Lack of difference in the prevalence of various co-morbid psychiatric disorders across different study groups suggests that psychiatric co-morbidity may not be useful to distinguish various subcategories of somatoform disorders.
The most common somatic symptoms observed in our study cohort were headache (81.5%), excessive tiredness on mild exertion (80.7%), pain in legs and/or arms (78.2%), bloating (73.9%), back pain (73.1%), discomfort in and around the upper abdomen and chest (62.2%), joint pain (59.7%), abdominal pain (58.8%), palpitations (58%) and dry mouth (56.3%). Studies from other parts of the world have also reported a similar profile of symptoms in patients with somatoform disorders (Hanel et al., 2009; Hessel, Beutel, Geyer, Schumacher, & Brahler, 2005; Rief, Hessel, & Braehler, 2001).Some of the differences in the prevalence of various subtypes of symptoms and the mean number of symptoms are due to differences in the assessment scales used across different studies.
The interesting finding of this study is that it did not reveal any difference in the prevalence of most of the somatic symptoms and the mean number of somatic symptoms across different subgroups of somatoform disorders. This suggests that the division of somatoform disorders on the number of number symptoms is just an artificial boundary to separate various subcategories, which in real sense do not exist. Many experts have also criticized this approach of current nosological systems and suggest that the subgrouping based on symptom count lacks face validity (Fink, 1996; Mayou et al., 2005). Authors have also criticized the construct of persistent somatoform pain disorder which places absolute emphasis on somatic presentations by the patients and ignores the behavioural and psychological attributes of the sufferers (Birket-Smith & Mortensen, 2002; Rief & Issac, 2007; Voigt et al., 2010). Our finding also supports this criticism in that patients with persistent somatoform pain disorders also have similar level of anxiety and hypochondrial worry as patients with other subcategories of somatoform disorders. Furthermore, our findings also provide insight into the fact as to why it is difficult for the non-psychiatric physicians to differentiate between the somatoform pain disorder category and other categories of somatoform disorders, as pointed out by various authors (Dimsdale et al., 2011).
However, our finding of lack of difference in symptom profile and the correlate profile was contrary to what we expected. The possible reasons for lack of differences could be the non-specific nature of these symptoms, as somatic symptoms occur across various disorders and these cannot be considered to predict any specific diagnosis. Other reason of lack of difference could be due to the socio-cultural factors, for example, in our culture expression of psychological distress in the form of somatic manifestation is quite common. This lack of difference also suggests that the underlying biological mechanism for development of various somatic symptoms is the same and our attempt to nosologically separate these disorders is artificial and should be abandoned. Accordingly, in routine psychiatry clinical practice and while dealing with colleagues from other specialties, we should attempt to talk about somatoform disorders as a homogenous group with similar symptom profile, demographic profile and clinical correlates. Taking this approach in the research setting will also help in carrying out further research in this area.
Diagnostic and Statistical Manual of Mental Disorders–Fifth Revision (DSM-5) category of somatic symptom disorder (SSD) has attempted to overcome some of these limitations in that it emphasizes the fact that the diagnosis must not be based solely on the basis of somatic presentations, but that associated cognitions also must be taken into account. Our findings suggest this would possibly help in making appropriate diagnosis of various subcategories by incorporating specific cognitions in the definition of various subcategories.
In terms of psychological correlates, the findings of this study suggest higher prevalence of alexithymia in patients with somatoform disorder, which is similar to that reported in literature (Duddu, Issac, & Chaturvedi, 2003; Jyvasjarvi et al., 1999; Sarkar & Chandra, 2003). There were minor differences in the correlation between the mean number of somatic symptoms and psychological constructs like alexithymia, somato-sensory amplification and hypochondriacal worry between those with persistent somatoform pain disorder and other somatoform disorders. These differences suggest that there is a need to focus on the cognitions of the patients with somatoform disorders to arrive at the different subcategories of the disorder, rather than the number of somatic symptoms.
Our correlation findings suggest that in all patients with somatoform disorder, the number of somatic symptoms increases with increase in level of depression and somato-sensory amplification. However, in patients with somatoform disorder other than the persistent somatoform pain disorder, the increase in the number of somatic symptom is also associated with increase in the hypochondriacal worry and alexithymia. It would be premature to draw a cause–effect relationship, but it can be hypothesized alexithymia plays a more important role in the development of other somatoform disorders.
To conclude, the findings of this study suggest that the current methodology of subcategorizing various somatoform disorders lacks validity and there is a need to change the approach in defining various somatoform disorder categories.
Our study has certain limitations. The study was conducted in a tertiary care centre and included a limited study sample. The number of patients in various subcategories of somatoforms disorder other than the persistent somatoform pain disorder was small. Future studies must attempt to overcome these limitations. Furthermore, there is a need to replicate our findings so that these will not be considered as incidental observations.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.