
Abstract
Aim:
The aim of this study is to investigate differences in the beliefs about the causes of schizophrenia between Aymara and non-Aymara patients with schizophrenia and their primary caregivers. Ethnic background plays an important role in the formation of beliefs regarding the causes of schizophrenia, and there have been no prior studies on such beliefs among the Aymara, an indigenous community with a population of about 2 million people living in the Andes. We focused on three systems of beliefs distinguished in the literature: biological, psychosocial and magical–religious.
Methods:
The sample comprised 253 patients (n = 117 Aymara, and n = 136 non-Aymara) of public mental health centers in Chile (33.6%), Peru (33.6%) and Bolivia (32.8%) with a diagnosis of schizophrenia, and each patient’s primary caregiver. We administered to patients and caregivers a questionnaire with scales assessing the perceived causes of schizophrenia. Linear regression models were fitted to compare differences in the levels of causal beliefs between Aymara and non-Aymara patients and caregivers, and to identify socio-demographic and clinical predictors of different types of beliefs about the causes of schizophrenia.
Results:
Adjusted for socio-demographic and clinical covariates, levels of psychosocial beliefs were significantly higher for Aymara caregivers (0.33, 95% confidence interval (CI) = 0.05, 0.62) than non-Aymara caregivers.
Conclusions:
Contrary to expectations, beliefs about the causes of schizophrenia among Aymara are not more magical–religious than those of their non-Aymara counterparts. It may be necessary for mental health staff members to evaluate beliefs about the disorder, especially in ethnic minorities, before applying a standard model of treatment.
Introduction
Large-scale deinstitutionalization of psychiatric patients has resulted in a dramatic shift in the burden of caregiving from health care professionals to family members. The beliefs that family members have regarding the causes of their relative’s problems profoundly shape the caregiving process. It is therefore important to understand the specific types of causal beliefs held by family members. Prior studies demonstrate that the family’s cultural background provides a framework for understanding the origins of psychiatric illness as well as for interpreting the changes in mental functioning that family members observe in their relative experiencing a psychiatric disorder – for example, through shared “social representations” of disorder (Holzinger, Kilian, Linderbach, Petscheleit, & Angermeger, 2003). Features of the mental health system itself may also influence family members’ causal beliefs (Kurihara, Kato, Revenger, & Tirta, 2006), and are also important to consider in studying causal beliefs.
Studies of patients’ and caregivers’ beliefs about the causes of schizophrenia are important because beliefs can influence help-seeking, adherence to treatment, disease management and, as a result, clinical outcomes. Some studies in this area show that patients with better clinical outcomes hold a psychosocial model of beliefs, wherein the main causes of schizophrenia originate from external factors such as economic conditions, stressors and educational attainment (Phillips, Li, Storup & Xin, 2000; Saravanan et al., 2007). Causal beliefs are in part dependent on the degree of patients’ insight. Studies show that patients with better insight were more likely to hold a biomedical causal model of beliefs, wherein the causes of schizophrenia originate from inherited factors, brain disorder, and fatigue (Aguglia, De Vanna, Onor, & Ferrara, 2002; Phillips, Li, Storup, & Xin, 2000; Saravanan et al., 2007; Zafar et al., 2008). In contrast, patients with worse insight were more likely to hold magical-religious beliefs in which psychiatric symptoms are thought to originate from external factors over which individual patients have no control; thus, causal beliefs characterized as magical-religious tend to negatively impact clinical outcomes, partly because of treatment delays (Kulhara, Avashi, & Shama, 2000; Saravanan et al., 2007; Borras et al., 2007).
In addition to insight, demographic factors such age, gender and education may be related to patients’ and caregivers’ beliefs about the causes of schizophrenia (Farina et al., 1981; Furnham & Chan, 1978; Brockman & D’Arcy, 1978). Supernatural beliefs are generally more common among patients and caregivers’ with less education, (Kurihara et al., 2006; Kate, et al., 2012), whereas biological and psychosocial beliefs about mental illness are generally related to higher levels education (Phillips et al., 2000; Srinivasan & Thara, 2001). There are exceptions to these patterns however. For instance, a study in Israel there were no differences on gender or patients’ educational level (Al-Krenawi, 1999). Similar results were reported in a recent study in India, which did not find any correlation between the beliefs of patients and caregivers and demographic variables of age, sex, education, and employment (Balhara & Yadav, 2012). Also in this country, patients with schizophrenia were more likely to hold mystical beliefs, but that was not the same for the caregivers that live on urban areas (Kate, Grover, Kulhara, & Nehra, 2012; Saravanan et al., 2007; Srinivasan & Thara, 2001).
Differences in cultural models of schizophrenia also vary across European countries. A study in Spain found that caregivers believe that the main cause of schizophrenia is related to psychosocial factors (Agras, Crespo, Silveira, & Blanco, 2002). In contrast, a study in Germany found that relatives (particularly mothers) are more likely than individuals in the general population to believe schizophrenia is caused by biological and hereditary factors, a finding that Angermeyer and Matschinger (1996) attribute to relatives’ greater exposure to biomedically oriented psychiatrists.
Outside of Europe, there is considerable variability in patients’ and caregivers’ causal beliefs. In China, families of patients with schizophrenia predominantly endorsed social and interpersonal factors and psychological problems as causes of their relative’s schizophrenia, and rarely endorsed biomedical causes (Phillips et al., 2000). In India, patients with schizophrenia commonly subscribe to supernatural causal models, but caregivers rarely do so (Kate et al., 2012; Saravanan et al., 2007; Srinivasan & Thara, 2001). Bedouin-Arab patients in southern Israel uniformly attributed their symptoms of neurotic and psychotic illnesses to supernatural forces (Al-Krenawi, 1999).
It is necessary to consider two important points regarding the studies on beliefs about schizophrenia: the first one is the inconsistency in the results and the second one is that there is scarce literature on what happens within different geographic contexts, and even less among ethnic minorities in Latin America who have high rates of treatment discontinuation (Vicente, Kohn, Rioseco, Saldivia & Torres, 2005). This could be due in part to the discrepancy between the shared models of beliefs within ethnic minority groups and the prevailing biomedical model characteristic of urban mental health clinics. Enhancing our understanding of causal models held by ethnic minority groups is therefore important for improving engagement with service provides and ultimately better psychiatric care (US Department of Health & Human Services (USDHHS), 2001, Tompson, 1995).
This study is the first to address Aymara caregivers and psychiatric patients who are residents of three South American countries: western Bolivia, southern Peru and northern Chile. The Aymara culture, with a population of 2 million people, has lived in the Andes Mountains for centuries, however, recent generations of Aymara have undertaken a massive migration, moving from rural towns in the foothills to large cities (Köster, 1992; Van Kessel, 1996; Nuñez & Cornejo, 2012; Gundermann, 2000; Zapata, 2007).
When discussing the Aymara ‘community’, we remain cognizant that Aymara tradition is not monolithic, and that regional and also local variations exist with respect to the intensivity of certain cultural or social practices – for example, the Aymara language – and to the general degree of intercultural involvement. That said, there remains a strong coherence in the Aymara tradition regarding certain basic principles of life, behavior, rites and – for the specific case that interests us here – ways to understand mental illness (Fernández Juárez, 2002). Our previous study of coping strategies in Aymara caregivers of patients with schizophrenia showed that they tend to use more spiritual help (Caqueo-Urízar, Gutiérrez-Maldonado, Ferrer-García, & Miranda-Castillo, 2012). Similarly, the Aymara family in the community leads the patient, in the first instance, to the healer (Yatiri) who performs a series of rituals to cure the mental disorder. These rites are related to magical–religious beliefs, minerals and herbs (Leiva, 2008).
The aim of the current study is to investigate differences in the beliefs about the causes of schizophrenia between Aymara and non-Aymara patients with a diagnosis of schizophrenia and their primary caregivers. We analyzed three systems of beliefs: biological, psychosocial and magical–religious.
We hypothesized that there would be a greater amount of magical–religious beliefs about schizophrenia, fewer biological beliefs (due to limited access to this type of knowledge) and a greater amount of psychosocial beliefs (since these are related to problems in education, work and finance) in Aymara caregivers and patients versus non-Aymara. We also investigated the socio-demographic and clinical correlates of magical, psychosocial and biological beliefs among patients and caregivers.
Methods
Sample
The process of recruitment of Aymara and non-Aymara patients and caregivers took place in public health sector clinics in each country. We selected the largest public health clinic in each region. The first author reviewed the lists of patients and caregivers who were attending each center, and the research team made assessments over a 3-month period in each country. Patients were invited to participate as they came for their monthly follow-up visits, usually accompanied by their key caregiver. Most of the people agreed to participate.
The study sample comprised patients with schizophrenia who were receiving services from mental health clinics in the Central–Southern Andean regions of northern Chile, southern Peru and central–western Bolivia, and each patient’s primary caregiver, defined as the person who fulfills the primary caring role and spends more time than anyone else with the patient in the task of caring. The sample included both Aymara and non-Aymara patients and caregivers. Aymara patients and caregivers were identified by Aymara surnames as established by legislation regarding indigenous peoples in the three countries, or Aymara self-identification, being this last criterion, the most important for the selection. Both the Aymara and non-Aymara patients live in the same urban areas, are served by the same mental health centers and have roughly comparable socio-demographic characteristics.
We applied a small set of exclusion criteria to the patient (being in a state of psychotic crisis or having a sensory or cognitive type of disorder that prevents being evaluated) and caregiver (presence of organic symptomatology; having a psychoactive substance abuse disorder; having a sensory or cognitive type of disorder that prevents interviewing) groups to ensure ability to participate fully in the interviews. The final sample included 253 patients with an International Classification of Diseases (ICD)-10 diagnosis of schizophrenia (World Health Organization (WHO), 1992) and 253 primary caregivers (33.6% from Chile, 33.6% from Peru and 32.8% from Bolivia). Interviews were conducted between May 2012 and February 2013.
Although these three Latin American countries share several cultural characteristics, there are some differences between them, which should be made explicit: thus, in Bolivia, 13.6% of the population lives with less than US$1 per day; in Peru, this population is 5.9% and it is <2.0% in Chile, which shows some difference in relation to the poverty index (Organización Mundial de la Salud (OMS), 2013). Some other differences are associated with psychiatric care facilities (per 100,000 inhabitants, Bolivia has 0.1 psychiatric hospitals, Peru has 0.01 and Chile 0.003; this last country has a greater number of outpatient institutions), mental health staff (the number of psychiatrist in Bolivia is 0.1; Peru: 0.1 and Chile: 0.6 per 100,000 inhabitants), lack of day hospitals (Bolivia: 0.1; Peru: 0 and Chile: 0.5) and residential care (Bolivia: 0; Peru: without data and Chile: 103) (OMS, 2013; Organización Panamericana de la Salud (OPS), 2013).
Measures
Survey for relatives and patients regarding causes of schizophrenia
This survey was developed for research purposes and the questions were based on the Causal Models Questionnaire for Schizophrenia in China (Phillips et al., 2000) and on the Questionnaire for Beliefs Regarding Schizophrenia in Bali (Kurihara et al., 2006). The Bali survey presents a Cohen’s kappa coefficient of between .71 and .92, with a mean value of .82 for 15 items and .90 for the most important cause, indicating that the test–retest reliability was high.
The survey tool for the current study has 16 items distributed in a Likert scale where 0 = no cause; 1 = possible cause; and 2 = cause. The items of the survey are divided into three subclasses, and a score is obtained for each subscale: (1) biological causes has a score ranging from 0 to 8 and includes the following four items: brain disorder, heredity, physical disease, fatigue; (2) psychosocial causes has a score range from 0 to 14 and includes the following seven items: stress related to persons outside the family, personality problems, work stress, financial problems, stress related to family members, low educational level and school stress; and (3) magical–religious causes has a score range from 0 to 10 and includes the following five items: punishment by God, fright sickness, ‘grab from land’ (a belief that a bad force from the land can induce sickness), witchcraft and black magic. This subscale was developed from key informant interviews (anthropologists, an intercultural Aymara consultant) as well as from the literature review. In the current sample, Cronbach’s alphas (a measure of internal consistency reliability) were .80 for the magical–religious factor, .73 for psychosocial factor and .58 for the biological factor for the patients’ survey, and were .81 for the magical–religious factor, .63 for psychosocial factor and .49 for the biological factor for the caregivers’ survey. Scores on the three domains of beliefs about the causes of schizophrenia were standardized to a mean (M) of 0 and SD of 1.
Demographic and clinical characteristics
Participant demographic characteristics included sex, age, educational level (high or low), kinship (mother or other), marital status (with a partner or without a partner), occupation, religious involvement (level of the person’s participation in a religious community, expressed as high or low), family income (measure of the total salary per month for all members of the family, expressed in US dollars) and receipt of government assistance (whether or not the patient received monthly financial support from the government). Patient clinical characteristics included age at onset of treatment, years of living with the disorder, type of treatment (whether the patient received only pharmacological treatment by the mental health services or integrated treatment, meaning pharmacological plus psychotherapy, family psychoeducation, day care hospital) and hospital admission(s) in the last 3 years.
Procedures
The study was approved by the Ethics Committee of the University of Tarapacá and the National Health Service of Chile. Two psychologists, who were part of the research team and were supervised by the principal researcher, conducted the evaluations of family members and caregivers under the auspices of the mental health services of each country. The length of time of the evaluation of the caregivers was between 15 and 20 minutes; the evaluation of the patients was more extensive, between 20 and 30 minutes.
Before the start of the survey, informed consent was requested and received from the relative and the patient. The objectives of the study were explained as well as the voluntary nature of participation. No compensation was offered for participating in the study.
Data analysis
Hypotheses regarding differences in the beliefs about the causes of schizophrenia between Aymara and non-Aymara patients and caregivers were evaluated by fitting linear regression models for each of the three domains of beliefs (magical–religious, psychosocial, biological). Two models were fitted for each domain, one including only ethnicity as the predictor, and the second including socio-demographic and clinical characteristics. We hypothesized that Aymara patients and caregivers would have higher mean scores on the scales of magical–religious and psychosocial beliefs than non-Aymara patients and caregivers, and a lower mean score on the scale of biological beliefs than non-Aymara patients and caregivers. We used the adjusted models for each domain of beliefs to identify significant demographic and clinical correlates of beliefs about the causes of schizophrenia. The data were analyzed using SPSS version 17.0.
Results
Table 1 shows the characteristics of the sample of caregivers. The majority of caregivers are women (67%), parents of the patient (76%), with a low educational level and with employment outside of the home (56.9%). Aymara caregivers are more likely than non-Aymara caregivers to work outside of the home; however, their monthly family incomes are lower. With respect to caregivers’ beliefs about the causes of schizophrenia, scores on psychosocial beliefs were higher overall than scores on biological and magical–religious beliefs.
Socio-demographic characteristics and beliefs of the total sample, Aymara and non-Aymara caregivers.

Unstandardized scores.
Table 2 shows the characteristics of patients, most of whom are men without a partner, no children (they live with their parents), without employment outside the home, with low educational level and do not receive monthly financial support from the government. It should be noted that only 12.3% receive integrated treatment, meaning pharmacological plus psychotherapy and family psychoeducation, and in some patients, day care hospital from mental health services. Aymara patients reported less adherence to drug treatment, they receive less monthly financial support from the government and the start of treatment was 1.8 years later than patients who are not Aymara. Among all patients, scores on the scales of causal beliefs were higher for the psychosocial domain than for the magical–religious and biological domains.
Socio-demographics, clinical characteristics, and beliefs of the total sample, Aymara and non-Aymara patients.
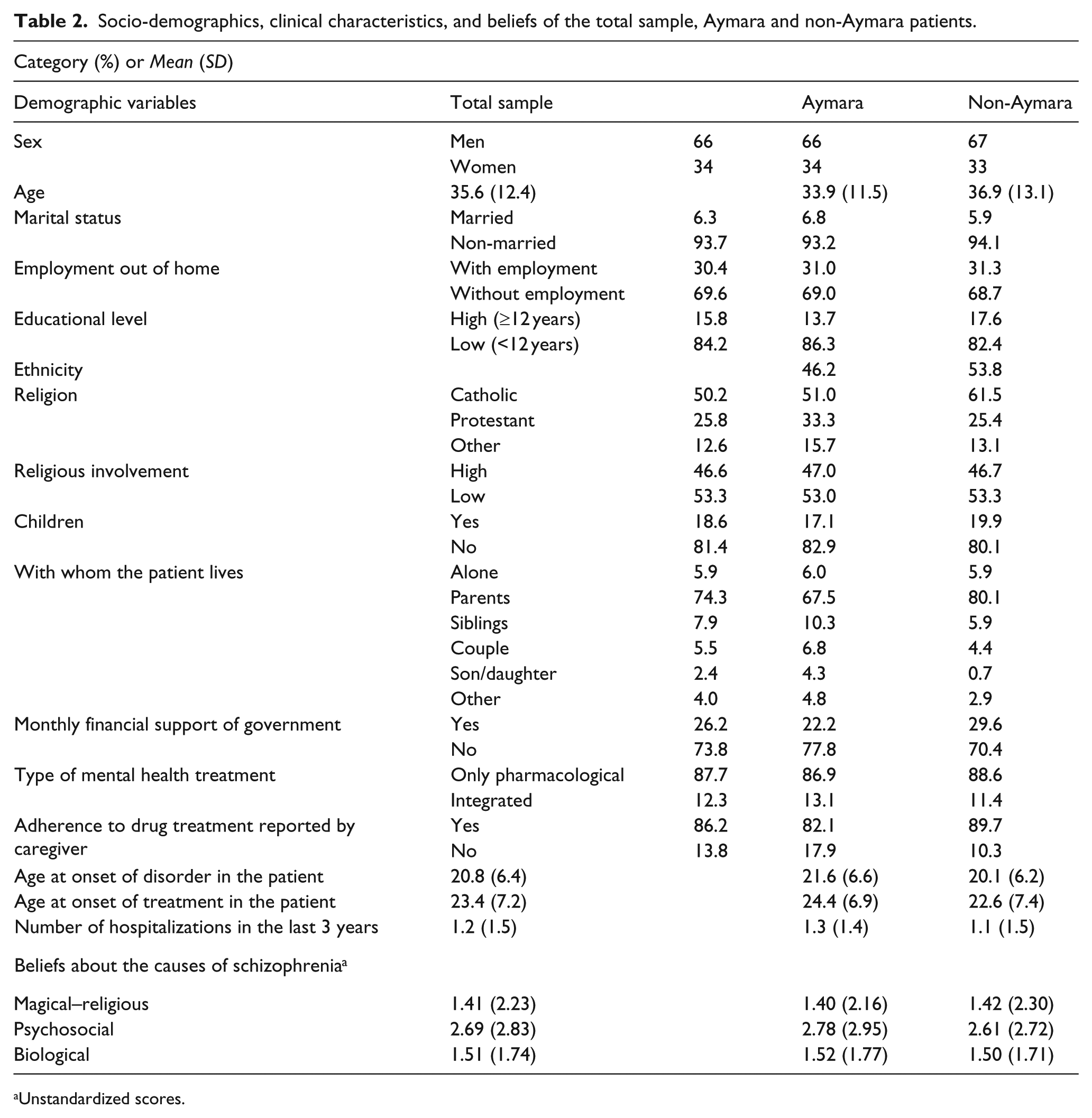
Unstandardized scores.
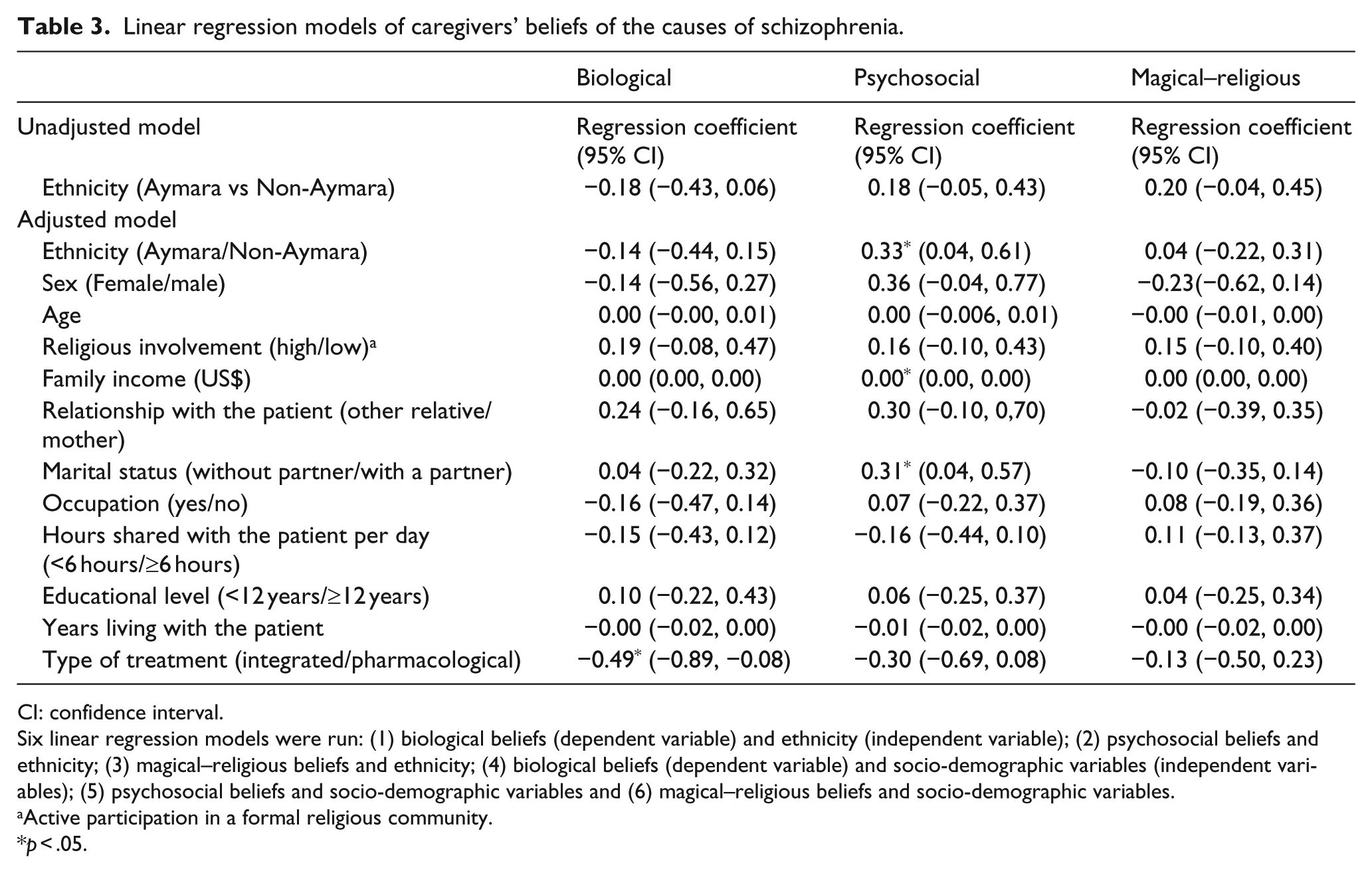
In the unadjusted linear regression model for causal beliefs among caregivers (top row of Table 3), there were no significant differences between ethnic groups in the mean levels of biological, psychosocial and magical–religious beliefs, though the mean differences were in the expected direction (higher psychosocial and magical–religious scores among Aymara caregivers, and lower scores on biological beliefs among Aymara caregivers). Adjusted for socio-demographic and clinical covariates, levels of psychosocial beliefs were significantly higher for Aymara caregivers (0.33, 95% confidence interval (CI) = 0.05, 0.62) than non-Aymara caregivers. In addition, the following factors were significant predictors of mean scores on beliefs: type of treatment was significantly associated with biological beliefs; caregivers of patients receiving integrated treatment had scores on the scale of biological beliefs that were −0.49 (−0.89, −0.08) lower than caregivers of patients receiving pharmacologic treatment scores on the scale of biological beliefs.
Linear regression models of caregivers’ beliefs of the causes of schizophrenia.
CI: confidence interval.
Six linear regression models were run: (1) biological beliefs (dependent variable) and ethnicity (independent variable); (2) psychosocial beliefs and ethnicity; (3) magical–religious beliefs and ethnicity; (4) biological beliefs (dependent variable) and socio-demographic variables (independent variables); (5) psychosocial beliefs and socio-demographic variables and (6) magical–religious beliefs and socio-demographic variables.
Active participation in a formal religious community.
p < .05.
Psychosocial beliefs were associated with higher family income (regression coefficient = .00; CI = 0.00, 0.00), and not having a partner (regression coefficient = .31; CI = 0.04, 0.57). Finally, there were no significant predictors of scores on the scale of magical–religious beliefs.
Regression analyses of beliefs about the causes of schizophrenia among patients are presented in Table 4. Aymara ethnicity was not significantly associated with differences in beliefs about the causes of schizophrenia. Table 4 also presents the coefficients from the adjusted models for each scale of beliefs. Patients with higher levels of religious involvement (coefficient = .37; CI = 0.08, 0.67) and lower levels of education (coefficient = .45; CI = 0.04, 0.86) had higher mean scores on the scale of biological beliefs.
Linear regression model of patients’ beliefs of the causes of schizophrenia.
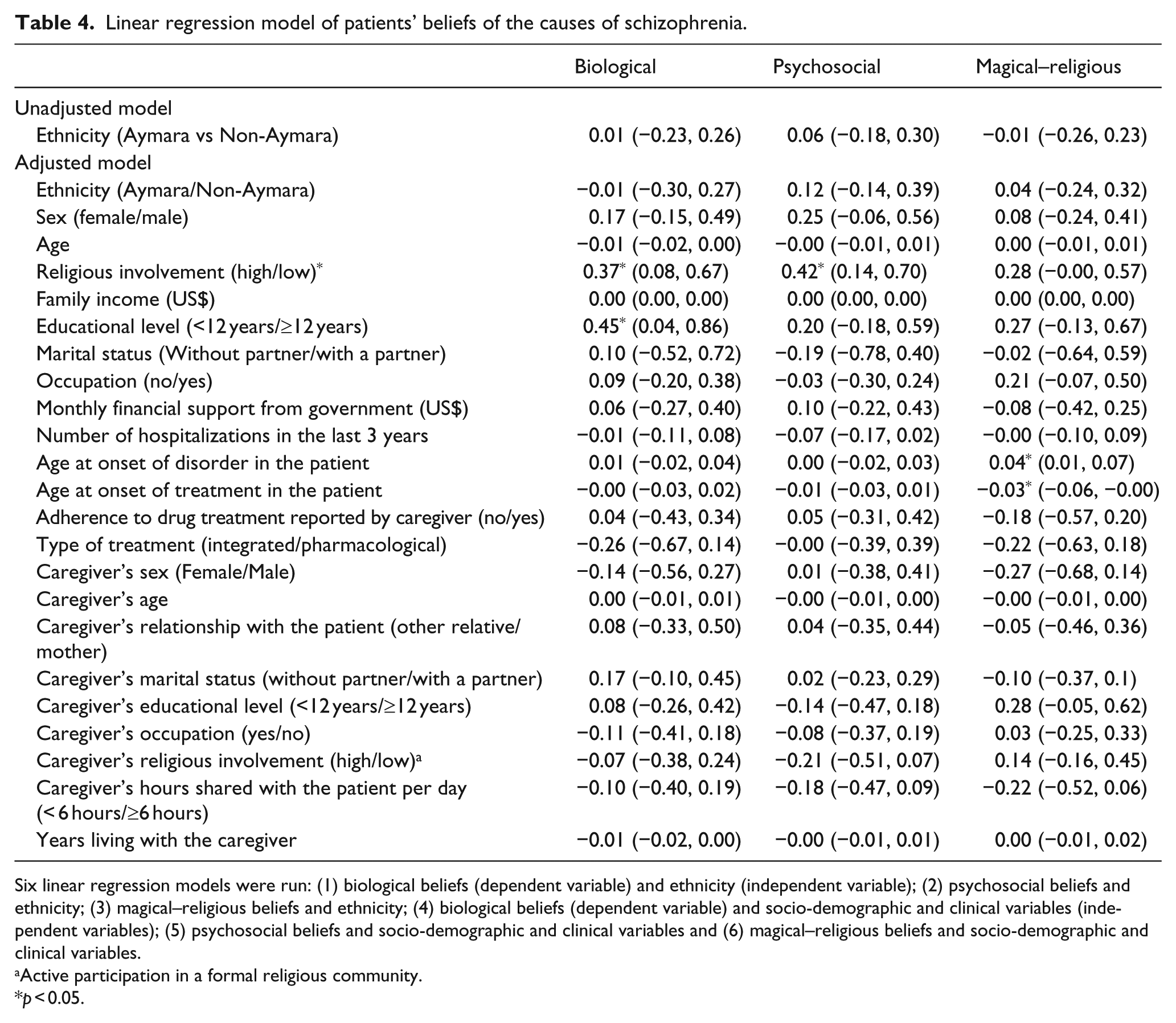
Six linear regression models were run: (1) biological beliefs (dependent variable) and ethnicity (independent variable); (2) psychosocial beliefs and ethnicity; (3) magical–religious beliefs and ethnicity; (4) biological beliefs (dependent variable) and socio-demographic and clinical variables (independent variables); (5) psychosocial beliefs and socio-demographic and clinical variables and (6) magical–religious beliefs and socio-demographic and clinical variables.
Active participation in a formal religious community.
p < 0.05.
Patients with higher levels of religious involvement also had higher mean scores on the scale of psychosocial beliefs (coefficient = .42; CI = 0.14, 0.70). Finally, patients with an older age of onset (coefficient = .04; CI = 0.01, 0.07) had higher magical–religious beliefs, and those who initiated treatment at older ages had a lower level of magical–religious beliefs (−.03; CI = −0.06, −0.00).
Discussion
The study describes the beliefs about the causes of schizophrenia in caregivers and patients who belong to a Latin American ethnic minority. To the best of our knowledge, this is the first research to describe the beliefs of a population that has been rarely studied. We found differences between Aymara and non-Aymara caregivers in the beliefs about causes of schizophrenia in the domain of psychosocial beliefs. In contrast, there were no ethnic differences in beliefs observed among patients. A possible explanation for why we did not find a greater amount of magical–religious beliefs may be that these caregivers and patients have, for the most part, integrated a biomedical model of explanation via the varied mental health services of the three countries, despite the fact that they belong to a different culture with a different worldview. Support of this conjecture is the finding that if a patient receives pharmacological treatment, this medical interaction is significantly related to the biological beliefs of the caregiver.
These findings could be reflecting changes in the values of the Aymara culture wherein the traditional view of mental illness as arising from magical-religious forces has shifted towards psychosocial models of beliefs that emphasize disturbances in social and economic aspects of life as a cause of schizophrenia.
Changes in the Aymara belief structure would appear to coincide with large-scale migration of Aymara from rural to urban areas and, along with it, increasing cultural assimilation (Gunderman, González, & Vergara, 2007; Gundermann, 2000). From an anthropological point of view, urban migration has created “spaces in between” Aymara and non-Aymara culture and increasing “interfaces between systems” of beliefs (Temple, Layme, Michaux, González, & Blanco, 2003).
These areas could be emerging in interesting ways to combine different ways of living (De Munter, 2007). As a consequence, it is clear that the Aymara tradition is more than a single tradition and cannot be considered simply as a homogeneous and isolated whole. Aymara tradition shall always exist in a relative state and is constantly changing (De Munter, 2010).
The results did not show correlations between the magical–religious beliefs and the socio-demographic characteristics of age, sex, educational level and employment in caregivers. Those results are coherent with those of studies from Israel and India (Al-Krenawi, 1999; Balhara & Yadav, 2012).
In patients, the religious involvement variable must be analyzed with caution. A greater religious involvement may be playing a role in biological beliefs and psychosocial (and yet not have an association with magical–religious beliefs as might be expected); this may be explained by the possibility that patients give socially desirable answers and although religious involvement may well have an association with the magical–religious beliefs, they did not report it.
Second, two clinical variables (age at onset of disorder and age at onset of treatment) were associated with patients’ magical–religious beliefs. Thus, it is likely that patients presenting with the disorder at an older age have remained within their family structure and thus influenced by magical–religious beliefs for a longer period of time. Furthermore, it is likely that in such patients, schizophrenia might have been recognized earlier, but these specific symptoms of the disorder may have been consistent with the magical–religious beliefs in relation to the disorder within the family environment.
Along this line of thought, those patients who began their treatment at a younger age may have been affected by a more serious disorder and thus affected more by magical–religious beliefs.
Another main finding of this study shows that the major causes attributed to the disorder were psychosocial in nature. As such, the results are similar to those found in previous studies carried out in China, India, Turkey, Germany and Spain where caregivers and patients designated psychosocial factors as the main cause, including stress at work, in the family, at school, among others (Agras et al., 2002; Angermeyer & Matschinger, 1996; Holzinger et al., 2003; Karanci, 1995; Phillips et al., 2000; Srinivasan & Thara, 2001).
Holzinger et al. explain the emergence of psychosocial models of beliefs using theoretical work by Pollock (1988) which argues that the “stress concept … permits the cause of illness to be located in the behaviour of the individual, who exposes himself excessively to psychosocial stressors… This excessive exposure to stressors makes it possible to hold pathogenic social structures responsible and make the individual the victim of harmful influences” (Holzinger et al., 2003, p. 161). Moreover, as Agras et al. explain (2002), “the attributions of schizophrenia to psychosocial factors allow caregivers to avoid feelings of guilt” (p. 23). This could be viewed as a mechanism of self-protection, especially for caregivers without a partner who bear sole responsibility for caregiving and for whom such guilt would compound the difficulty of their task.
Finally, the results of this study have implications beyond the South Andes. Viewed in the context of studies in diverse cultures globally, our results reinforce the commonality of ethnic variation in causal explanations for chronic mental illness and suggest that this variation has its roots at least partly in the core aspects of ethnic identity (Karanci, 1995; Phillips et al., 2000; Srinivasan & Thara, 2001).
There were some limitations that should be considered in this study. Almost all the patients (99%) in the sample were receiving pharmacological treatment, which could be influencing the association with biological beliefs. Another limitation is that caregivers and patients resided in urban areas. Future studies should consider the assessment of caregivers and patients who actually reside in the Andean highlands.
The cross-sectional design of the research does not allow an analysis of the development of causal beliefs over time, so following up this cohort of patients and caregivers would help understand the effectiveness of the medical care.
Conclusion
The findings on the beliefs about schizophrenia in the current study suggest that there were significant differences in psychosocial beliefs between Aymara versus non-Aymara caregivers in the Andean region of Latin America, in particular a potential change of the understanding of schizophrenia.
It may be necessary for mental health staff members to evaluate beliefs about the disorder, especially in ethnic minorities, before applying a standard model of treatment. The ultimate goal should be to ensure mutual understanding and to improve the therapeutic alliance between mental health services, patients and caregivers.
Footnotes
Acknowledgements
We thank Felipe Ponce and Jorge Escudero for their assistance in the study and also the following people and facilities: Dr Hugo Sánchez, Dr Ricardo Alvites, Dr Andrés Collado, Gladys Coaquira, Vilma Liendo and special thanks to Dr José Revilla from Hipólito Unanue Hospital in Tacna, Perú; Dr Marcio Soto from Arequipa, Perú; Dr Fernando Garitano, Dr Mauricio Peredo and Dra Mabel Romero from Centro de Rehabilitación y Salud Mental San Juan de Dios; and the Director of Hospital Psiquiátrico de la Caja Nacional de Salud from La Paz, Bolivia.
We also thank Dra Magdalena Gardilcic, Ester López and Alejandra Lagos from Servicio de Salud de Arica, Chile, and extend a special thanks to all the patients and caregivers who participated in this study.
Funding
This research was funded by CONICYT and BECAS-CHILE Postdoctorado en el Extranjero (74140004) and also by the Convenio de Desempeño UTA-MINEDUC.