
Abstract
Aim:
To record and measure the nature and severity of stigma and discrimination experienced by people during a first episode of schizophrenia and those with a first episode of major depressive disorder.
Methods:
The Discrimination and Stigma Scale (DISC-12) was used in a cross-sectional survey to elicit service user reports of anticipated and experienced discrimination by 150 people with a diagnosis of first-episode schizophrenia and 176 with a diagnosis of first-episode major depressive disorder in seven countries (Austria, Croatia, Czech Republic, Poland, Romania, Sweden and Turkey).
Results:
Participants with a diagnosis of major depressive disorder reported discrimination in a greater number of life areas than those with schizophrenia, as rated by the total DISC-12 score (p = .03). With regard to specific life areas, participants with depression reported more discrimination in regard to neighbours, dating, education, marriage, religious activities, physical health and acting as a parent than participants with schizophrenia. Participants with schizophrenia reported more discrimination with regard to the police compared to participants with depression.
Conclusion:
Stigma and discrimination because of mental illness change in the course of the mental diseases. Future research may take a longitudinal perspective to better understand the beginnings of stigmatisation and its trajectory through the life course and to identify critical periods at which anti-stigma interventions can most effectively be applied.
Introduction
Stigma and discrimination against people with mental illnesses are a global public health challenge (Evans-Lacko, Brohan, Mojtabai, & Thornicroft, 2012; G. Thornicroft, 2006) and can adversely affect all aspects of a person’s life, from employment and housing to social and family life (Corrigan, Larson, & Rüsch, 2009; Livingston & Boyd, 2010; Perlick et al., 2001).
Stigma can be conceptualised as having three distinct elements (G. Thornicroft, 2006). First, misinformation regarding the stigmatised condition is seen as ignorance. Second, a negative attitude towards a stigmatised group or individual is seen as prejudice. Third, the behavioural manifestation of stigma is discrimination. Discrimination can occur when stigmatised views of a person or a group of people are acted upon. Historically, stigmatising attitudes within the general public towards people with schizophrenia or depression have differed. People diagnosed with schizophrenia have tended to be seen as violent and dangerous (Crisp, Gelder, Rix, Meltzer, & Rowlands, 2000), while people with depression may be seen as more responsible for their illness (Crisp et al., 2000). Furthermore, symptom continuity has been found to be a factor in desire for social distance, with continuity being seen more as a feature of depression than schizophrenia (Schomerus, Matschinger, & Angermeyer, 2013); accordingly, social distance is more desired from those diagnosed with schizophrenia than depression (Schomerus et al., 2013). Additionally, although mental health literacy was found to have increased in Germany between 1993 and 2001, it was found that desire for social distance increased for both schizophrenia and depression (Angermeyer, Holzinger, & Matschinger, 2009). General population surveys suggest that attitudes towards people with schizophrenia are generally more negative than those towards people with depression (Crisp et al., 2000; Pescosolido et al., 2010). Recent research has more often investigated levels of stigma and discrimination using direct reports from mental health service users. The results of such research suggest that levels of stigma and discrimination are high, regardless of the type of diagnosis (Corker et al., 2013; Lasalvia et al., 2013), and are typically reported by over 85% of service users in a wide range of countries and contexts (Corker et al., 2013; G. Thornicroft et al., 2009). There are ongoing programmes to decrease stigma and discrimination in several European countries (Beldie et al., 2012), including Denmark, England, the Netherlands, Scotland, Spain and Sweden (Sartorius & Schulze, 2005). A recent review found that most programmes aimed to increase awareness of mental illness and to improve mental health literacy. In the countries that have conducted evaluations of their programmes, anti-stigma activities were shown to have mixed results in reducing negative attitudes towards people with mental illness. Austria and Sweden, for example, found that negative attitudes towards people with mental illness increased after anti-stigma campaigns, while Croatia found improvements in attitudes after an anti-stigma campaign. (Beldie et al., 2012). Rather than dismiss such campaigns, Beldie and colleagues encourage future campaigns to draw on the experience of previous work and to incorporate rigorous evaluation in order to formalise efforts to reduce stigma.
It is not known whether discrimination experienced by people with mental illness occurs right from the diagnosis of the first episode. The aim of this specific study was to compare levels of discrimination experienced between people diagnosed with first-episode depression or schizophrenia across several European countries.
Methods
Design
The study was a cross-sectional survey in which face-to-face interviews with people experiencing a first episode of schizophrenia and people with the first episode of depression were carried out. The interviews were carried out between June 2011 and June 2012.
Study sites and settings
Participants were recruited through psychiatric outpatient services in each participating country (Austria, Croatia, Czech Republic, Poland, Romania, Sweden and Turkey). The sites were identified through contact with members of the World Psychiatric Association (WPA) Global Programme against Discrimination because of Schizophrenia. Teams in Belgium, Hungary and Slovenia participated in the development of the study but for a variety of reasons could not recruit a sufficiently large sample in their site. The choice of recruitment location was left to the discretion of the study leader at each site. It was stipulated that the recruitment location should be reasonably representative of the usual treatment services provided to people with schizophrenia or major depression and that participants should be reasonably representative of patients with those diagnoses treated in those settings. All data collection took place in psychiatric outpatient clinics located in large urban centres. Invitation packs were given to potential participants from each participating country. They contained complete information about the study, including lists of interview topics, contact details of the researchers in case of questions and a consent form.
Participants
Participants were eligible to take part if they had been clinically diagnosed with schizophrenia or major depressive disorder and had had their first contact with specialist mental health services within 1 year prior to the study assessment. Our target was to include 25 people with a diagnosis of depression and 25 people with the diagnosis of schizophrenia at each study site. These targets were set on pragmatic grounds of feasibility at each study site, based on two previous studies. At the Swedish site, only people with a diagnosis of schizophrenia were included in the study (Tables 1 and 2).
Socio-demographic and clinical characteristics of participants with major depression.
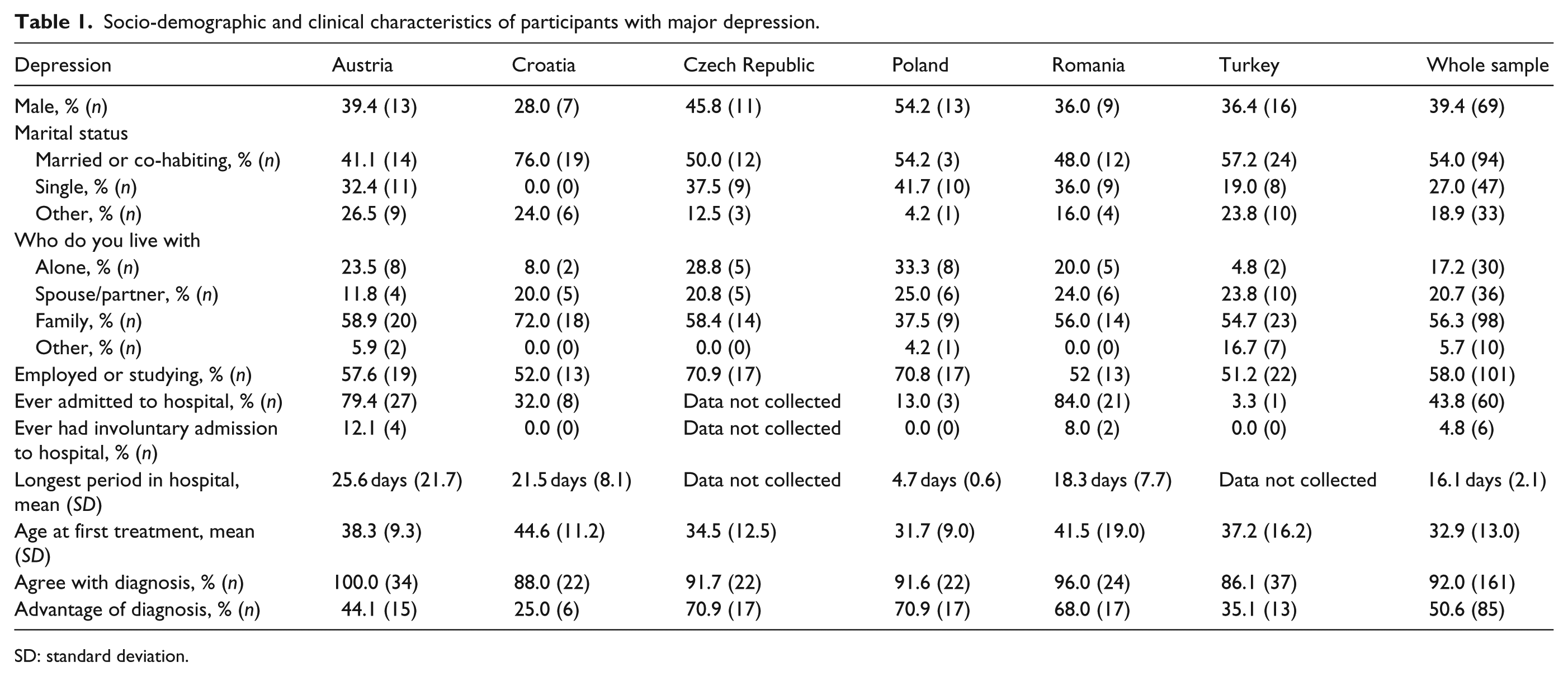
SD: standard deviation.
Socio-demographic and clinical characteristics of participants diagnosed with schizophrenia.
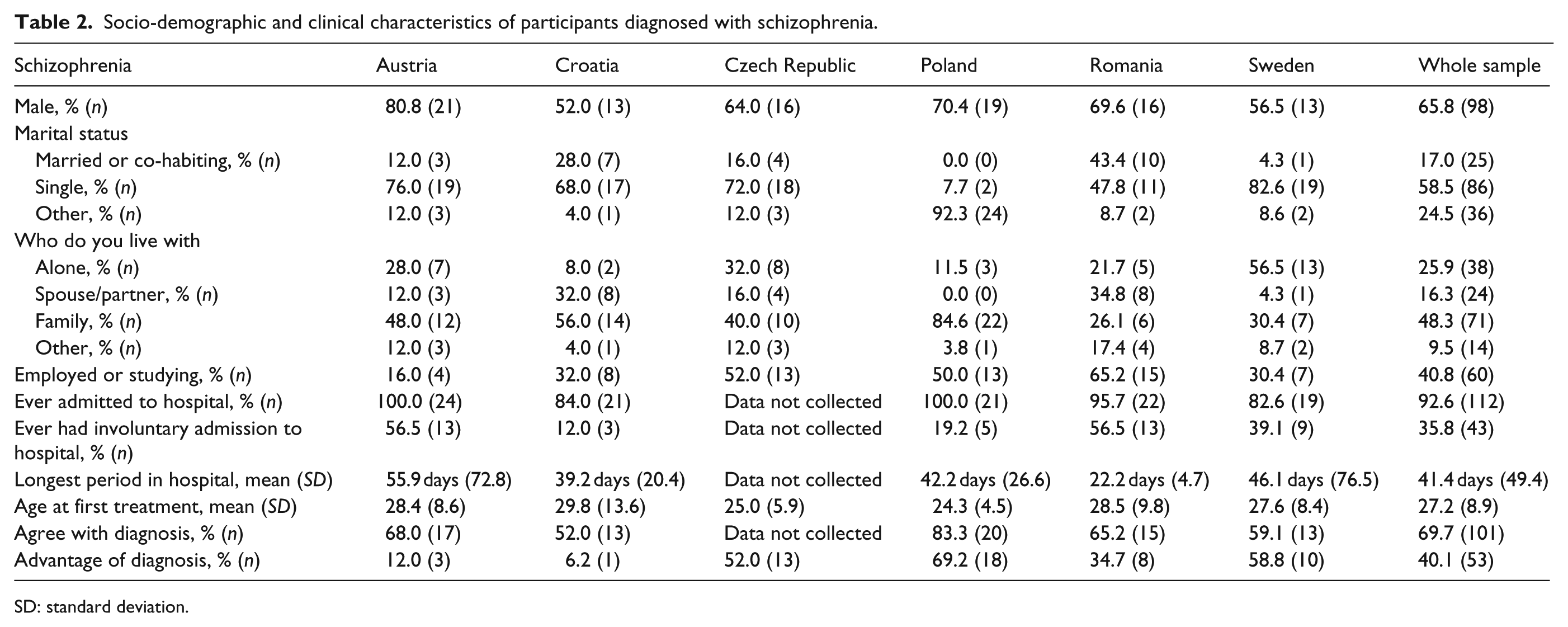
SD: standard deviation.
Data collection
The Discrimination and Stigma Scale (DISC-12) was used to measure experienced discrimination, anticipated discrimination, coping with stigma and discrimination and positive discrimination (Brohan & Thornicroft, 2013; G. Thornicroft et al., 2009). Socio-demographic characteristics and brief clinical information were also recorded. Details of the DISC-12 are given elsewhere (G. Thornicroft et al., 2009). Briefly, the DISC-12 is interviewer-administered and contains 21 items on negative, mental health–related experiences of discrimination in various life areas, plus one other ‘catch all question’ and four items to assess anticipated discrimination. All responses are given on a 4-point scale from ‘not at all’ to ‘a lot’. Higher scores indicate higher levels of discrimination. Where items related to situations which were not relevant to the participant in the previous 12 months (e.g. in relation to having children or seeking employment) or if a diagnosis could not have been known about in that situation, a ‘not applicable’ option was used. Recent analysis of the DISC-12 has found that it has strong psychometric properties (Brohan & Thornicroft, 2013). This report uses data from selected items of the negative discrimination subscale only.
Each interviewer was trained in individual training sessions conducted by the coordinating site and supervised in the course of the study. The DISC-12 has been used previously in all the countries in which the sites of this study were located and has been translated and adapted into each local language using a standardised translation/back-translation technique. The study received ethical approval in each of the participating countries and from the Psychiatry, Nursing & Midwifery Research Ethics Subcommittee, King’s College London.
Statistical analysis
Data analyses were conducted using SPSS (version 20). Total experienced discrimination scores were the number of items endorsed by participants. Mean experienced discrimination scores were calculated by summing individual items scores (0−4) and dividing by the number of applicable items. T-tests were used to assess differences between the diagnostic conditions. In order to test for differences between DISC-12 items in the diagnostic groups, the items were converted into binary variables (no discrimination versus any discrimination). Chi-squared tests were then performed to establish which DISC-12 items differed by diagnoses. A series of regression analyses were carried out using the DISC-12 items that were significantly different between diagnostic groups as the dependent variable and controlling for a set of potentially explanatory demographic differences between diagnoses, whether the participant thought the diagnosis was an advantage, whether the participant had ever been admitted to hospital, whether the participant had ever been admitted to hospital involuntarily, marital status, with whom the participant lived, highest education level, current employment status, whether the participant knew their diagnosis and gender.
Results
Socio-demographic and clinical characteristics
The data analyses were conducted for results from 326 participants, of whom 150 had a primary clinical diagnosis of schizophrenia and 176 had a clinical diagnosis of major depressive disorder. Overall, 51.2% of the sample were male, 37.0% of the sample were married or had a co-habiting partner and 28.0% of the sample were not currently employed.
Experienced discrimination by diagnosis
For the total DISC-12 score (i.e. the total number of areas of life for which participants reported negative discrimination), overall, participants reported a mean score of 2.7 (standard deviation (SD): 3.22) (out of a total possible score of 21). In terms of the total DISC-12 score for experienced discrimination, the depression group reported a mean score of 3.0 (SD: 3.71) and the schizophrenia group reported a mean score of 2.3 (SD: 2.48), which was a significant difference (p = .03). For the mean DISC-12 score, the group as a whole had a mean of 0.25 (SD: 0.34). Participants with schizophrenia reported an average mean DISC-12 score of 0.22 (SD: 0.26), while participants with depression reported a mean DISC-12 score of 0.27 (SD: 0.39), a non-significant difference (p = .17).
At the item level, there were significant differences between the reported experiences of unfair treatment of people with the diagnosis of schizophrenia and those with the diagnosis of depression in eight life areas. With regard to discrimination from neighbours, 25.0% of participants with depression reported discrimination, compared to 12.8% of participants with schizophrenia (p = .007). For discrimination experienced during dating or intimate relationships, 19.4% of participants with depression reported discrimination, compared to 6.7% of participants with schizophrenia (p = .001). In relation to discrimination regarding education, 14.8% of participants with depression reported discrimination, compared to 6.0% of participants with schizophrenia (p = .012). When commenting on discrimination in marriage (including divorce), 20.5% of participants with depression reported discrimination, compared to 10.7% of participants with schizophrenia (p = .022). On discrimination experienced with religious practices, 10.2% of participants with depression reported discrimination, compared to 3.4% of participants with schizophrenia (p = .017). For discrimination experienced with the police, 8.1% of participants with schizophrenia reported discrimination, compared to 2.9% of participants with depression (p = .045). Related to discrimination experienced with regard to physical health, 14.3% of participants with depression reported discrimination, compared to 2.0% of participants with schizophrenia (p < .001). Finally, when discussing discrimination experienced while acting as a parent, 11.4% of participants with depression reported discrimination, compared to 2.7% of participants with schizophrenia (p = .003) (see Figure 1). There were no other significant differences at item level between the diagnoses.

Comparison of the frequency of percentage of participants with both diagnoses reporting discrimination.
A logistic regression was carried out for each DISC-12 item (as the dependent variable) in which a significant difference was found between the diagnoses. The regression controlled for differences in country, whether the participant thought the diagnosis was an advantage, whether the participant had ever been admitted to hospital, whether the participant had ever been admitted to hospital involuntarily, marital status, with whom the participant lived, highest education level, current employment status, whether the participant knew their diagnosis and gender. This revealed that the variance in levels of discrimination is not explained by diagnosis for any of the above DISC-12 items with the exception of marriage (see Table 3).
Logistic regression analyses (using DISC-12 item as dependent variable) and percentage of participants reporting discrimination between diagnoses.
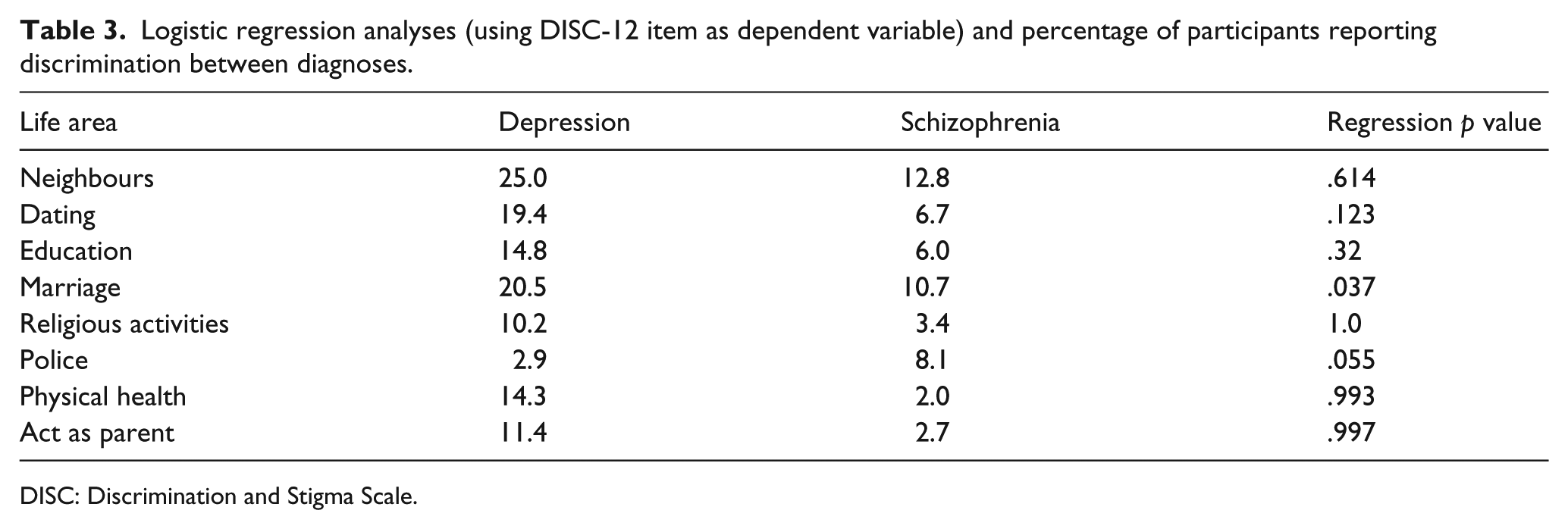
DISC: Discrimination and Stigma Scale.
Discussion
While the DISC-12 has been used in several other projects (G. Thornicroft et al., 2009), those studies did not focus on participants having a first-episode diagnosis. In this study, we have found that the number of participants who did not report discrimination in any life areas was higher than in the previous studies (Corker et al., 2013; C. Thornicroft, Wyllie, Thornicroft, & Mehta, 2014). These results are consistent with the view that the experience of discrimination will increase with the duration of illness. In line with previous work, we found that levels of discrimination were high in both depression and schizophrenia diagnoses (Corker et al., 2013; Lasalvia et al., 2013; G. Thornicroft et al., 2009).
We found that participants with a diagnosis of a first episode of depression reported experiencing discrimination in significantly more life areas than participants diagnosed with schizophrenia across all the countries studied. More specifically, we also found that participants diagnosed with depression more often reported discrimination in the areas of neighbours, dating, education, marriage, religious activities, physical health and acting as a parent more frequently. These results may seem counter-intuitive considering public attitude surveys towards people with mental illness. These studies report greater negative attitudes towards people with schizophrenia than with depression (Crisp et al., 2000). A possible explanation could be that the general public regard depression as being a less serious condition which does not deserve as much care and help as other types of mental illness and so behaviour towards people with a diagnosis of depression may be less supportive and more discriminatory. Alternatively, it is known that people with a diagnosis of depression appraise people and events in negative terms (Lecci, Karoly, Briggs, & Kuhn, 1994). This negative appraisal could be affecting the results here in that events that may have been appraised as neutral by people without a diagnosis of depression may be being appraised as negative and discriminatory by the participants with a depression diagnosis. This hypothesis can be tested in future prospective studies that include repeated measurement of stigma experiences and symptom burden.
Higher discrimination scores in participants with depression can also be potentially explained by illness duration and/or severity. Typically, people presenting to their general practitioners with symptoms of depression will be referred to specialist services less readily than people who present symptoms of schizophrenia. Therefore, it is possible that in this study, participants with depression represent those with more severe symptoms. Similarly, participants in this study with a diagnosis of depression may have had symptoms for a longer duration compared to the participants diagnosed with schizophrenia. In order to address the latter of these problems, the DISC-12 was administered with a time frame from when the participant first received specialist mental health care. No measure of symptom severity was taken for this study, and this could be a consideration for future research.
This study found that the only DISC-12 item in which participants with schizophrenia reported more discrimination than participants with depression was unfair treatment by the police. This could be explained by the higher risk of involuntary treatment in participants with schizophrenia. Some European countries can use the police force to assist in admitting patients to hospital, and reports of unfair treatment have been acknowledged by the European Commission (Salize, Dreßing, & Peitz, 2002). Different countries also have different thresholds for involuntary admission into hospital.
A limitation of this study is that the data are not representative of any of the participating countries. As a result, we have been unable to explore differences between participating countries. We therefore recommend this as a next step in research. Additionally, we did not collect data about the symptoms shown on admission to treatment or immediately before that which might have at least partially explained some of the differences that we found.
In summary, participants diagnosed with a first episode of depression reported negative discrimination due to their diagnosis in more areas of their lives than people with a first episode of schizophrenia, in contrast to population surveys that suggest more discrimination would be directed towards participants with schizophrenia. There were also important differences in the experience of discrimination among people with schizophrenia and depression living in different countries – people with a first episode of mental illness living in Poland and Sweden reported discrimination more frequently than those living in Croatia, Czech Republic, Romania and Turkey. Future research may take a longitudinal perspective to better understand the beginnings of stigmatisation and its trajectory through the life course and to identify critical periods at which anti-stigma interventions can most effectively be applied.
Footnotes
Acknowledgements
All authors would like to thank the participants and clinical staff that made this study possible: Susan Landqvist-Stockman, BSc, Pia Rydell, MD, and the Psychosis Clinic at Sahlgrenska University Hospital, Gothenburg, Sweden, for facilitating the study; Birgitta Sameby, RN, and Katarina Allerby, RN, for actively contributing to data gathering; Lydia Melchior, MD, for administrative assistance in Sweden and Dr Zuzana Čeplová, in the Czech Republic, for intensively collecting data.
Norman Sartorius and Graham Thornicroft are joint last authors.
Other members of the FEDORA study group: Judit Bulucz, Department of Psychiatry and Psychotherapy, Semmelweis University, Hungary, Budapest; Plesnicar Blanka Kores, University Psychiatric Clinic, Ljubljana, Slovenia; Eric Constant, Université catholique de Louvain, Louvain-la-Neuve, Belgium
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and international committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Funding
This work was supported in part by an unrestricted investigator initiated-grant given by Eli Lilly.