
Abstract
Background:
Little is known about the intergenerational and cross-cultural differences in emotional wellbeing and acceptability of psychological treatments for Arab Australians.
Aim:
To contribute to the emerging data about the mental health status and needs of Arab Australians.
Method:
An Internet survey examined psychological distress and functional impairment as measured by the Kessler 10 Item scale (K-10) and the Sheehan Disability Scale (SDS) among Arab Australians. Additional questions enquired about their help-seeking behaviours, barriers to accessing psychological treatments and preferences for delivery of psychological treatments. A total of 252 participants were recruited through public talks, media and online promotions.
Results:
Forty-three percent of the respondents reported moderate-to-severe functional impairment (M = 9.5; standard deviation (SD) = 1.8), 32% reported high psychological distress (M = 28.5; SD = 5.4) and 30% were born overseas. First-generation Arab Australians experiencing high psychological distress (i.e. K-10 ≥ 22), reported a greater preference for Internet-delivered treatment when compared to their second-generation counterparts. Only 18% of the sample reported seeking help from a mental health professional in the past year. The significant barriers reported by respondents with high psychological distress were poor mental health literacy, lack of time and stigma. Respondents preferred face-to-face (90%) over Internet-delivered treatment (55%). Finally, Arab Australians experienced higher psychological distress and underutilised mental health services when compared to the Australian population.
Conclusion:
Targeted public health campaigns that make culturally relevant interventions such as modifying existing Internet-delivered treatment for Arab Australians may reduce barriers and increase treatment options for this population.
Keywords
The Arabic-speaking communities in Australia (Arab Australians) include diverse groups of people with origins from 22 countries in North Africa and the Middle East. In the last 15 years, this community has grown by about 50% (Australian Bureau of Statistics, 2006, 2011) and is now the sixth largest group of immigrants to Australia comprising 1.4% of the total Australian population with 38.5% born in Australia (Australian Bureau of Statistics, 2011). Surprisingly, however, little is known about the mental health of this growing population. A small body of research has identified comparatively high rates of psychological distress and multiple barriers to treatment in this population. For example, a study examining the mental health of Arab Australians born in Lebanon and living in New South Wales (NSW) reported that 20% had elevated levels of psychological distress, that is, a rate twice that of the general population (Centre for Epidemiology and Research, 2010). An earlier study identified that Arab Australians (Youssef & Deane, 2006) experience similar barriers to accessing mental health treatment as Arab Muslim Americans (Aloud & Rathur, 2009) and Arab adolescents in Israel (Guterman, Haj-Yahia, Vorhies, Ismayilova, & Leshem, 2010), including low mental health literacy, shame, stigma and personal beliefs about treatment, and lack of trust in mental health professionals (Gearing et al., 2012; Guterman et al., 2010). Unfortunately, no research has explored questions of the prevalence of distress and barriers to treatment in the same research project. Such research would assist in the successful planning and provision of mental health services to Arab Australians.
An additional gap in the literature is information about the mental health status of first-generation (FG) compared to second-generation (SG) Arab Australians. FG are individuals born in an Arabic-speaking country who have migrated to Australia; SG are the children of parents who have migrated to Australia from an Arabic-speaking country and born in Australia. Such information is important because research in other countries indicates risk, and therefore, the need for services may differ between FG and SG individuals. For example, research has found that FG Middle Easterners living in Sweden (Hjern & Allebeck, 2002) and California (Nasseri & Moulton, 2011) have slightly lower risk levels of death by suicide when compared to their SG counterparts. Furthermore, a meta-analysis examining the risk for psychotic disorders among FG and SG from several different cultures found that an increased risk of psychotic disorders continued into the SG (Bourque, van der Ven, & Malla, 2011).
The aim of this study was to contribute to the emerging data about the mental health status and needs of Arab Australians. Specifically, this study sought to explore intergenerational (FG vs SG) and cross-cultural (Australians vs Arab Australians) differences in mental health status, treatment-seeking experiences and preferences, the barriers to treatment and the acceptability of different treatments to Arab Australians. To explore these issues, an online survey was developed based on a protocol used in similar research with other populations (Cuijpers, Donker, van Straten, Li, & Andersson, 2010; Lu, Dear, Johnston, Wootton, & Titov, 2013; Spence et al., 2011; Wootton, Titov, Dear, Spence, & Kemp, 2011). Based on previous research from the intergenerational differences in Arab and other ethnic populations, it was hypothesised that FG Arab Australians would have (1) lower rates of psychological distress and functional impairment and (2) lower mental health service utilisation and be less willing to try psychological treatments when compared to their SG counterparts. Furthermore, based on previous findings (Aloud & Rathur, 2009; Bourque et al., 2011; Gearing et al., 2012; Slade, Johnston, Oakley Browne, Andrews, & Whiteford, 2009; Youssef & Deane, 2006), it was expected that, compared to the general Australian population, Arab Australians would have (3) higher levels of psychological distress (4) lower rates of mental health service utilisation and a preference for ‘non-medical’ support from family, friends and religious leaders and (5) that a significant proportion of respondents would be willing to try psychological treatments, including Internet-delivered treatment for symptoms of stress, anxiety and low mood.
Method
Participants
Between October 2012 and April 2013, an anonymous online survey was conducted and promoted through multiple parallel channels. The survey was promoted through published articles in Arabic newspapers and radio interviews on Arabic radio shows. It was also promoted through the circulation of the survey to over 100 organisations providing services to Arab Australians, to over 100 Arabic-speaking service providers (e.g. general practitioners, medical specialists, allied health professionals, psychologists, social workers and counsellors) and to 20 spiritual leaders of an Arabic-speaking background in Australia.
Over that time, 261 people provided informed consent and volunteered to participate. Participants were invited to complete the Internet survey through our research website (www.ecentreclinic.org). Inclusion criteria were as follows: (1) resident of Australia, (2) overseas-born or Australian-born person who self-identified as being of Arabic ancestry and (3) being over the age of 18 years. Of the 261 respondents, nine were excluded for not completing the measure of psychological distress, the Kessler 10 Item Scale (K-10; Kessler et al., 2002), leaving 252 eligible for analysis. Entry into a draw to win an iPad was offered as compensation for participation.
Survey questionnaire and ethics
A bilingual (i.e. English and Arabic) 33-item online survey was developed for this study. Items were drawn from a review examining the barriers to and strategies for effective treatment implementation in Middle Eastern countries (Gearing et al., 2012) as well as several previous surveys (Lu et al., 2013; Spence et al., 2011; Wootton et al., 2011). The items were presented in both English and Arabic for all participants in order to aid understanding.
The bilingual survey was translated using a three-stage process. First, a professional translator (L.N.K.) conducted the forward translation, that is, a translation from English to Arabic. Second, the lead author (R.K.), in consultation with two bilingual speakers (M.K. and E.N.), conducted the backward translation, that is, from Arabic to English. Third, a bilingual psychologist (M.M.) reviewed the final translation. The questions and functionality of the survey were piloted with a small non-clinical convenience sample (n = 6) of Arab Australians. Questions were subsequently modified to improve the comprehension, interpretability and functionality of the survey. No formal analysis of validity was conducted.
The survey comprised the following six sections:
Demographics questions. A total of 14 items examined the age, marital status, education, country of birth, country of birth of parents/grandparents/great grandparents, length of time living in Australia, religion, Internet skills, average time spent on the Internet per week and English proficiency and reading ability.
Emotional wellbeing questions. The K-10 (Kessler et al., 2002) and the SDS (Sheehan, Harnett-Sheehan, & Raj, 1996) were used to assess psychological distress and functional impairment, respectively. The K-10 is a 10-item scale measuring non-specific psychological distress strongly related to diagnoses of anxiety and depression, with a total score of ≥22 indicating a high level of psychological distress (Andrews & Slade, 2001). The SDS is a three-item scale used to assess functional impairment in school/work, social and family life (Sheehan et al., 1996). Both measures are widely used and known to have good psychometric properties. Cronbach’s alpha for the K-10 and the SDS was .93 and .91, respectively, in this study.
Help-seeking. Seven items were completed by respondents who endorsed having concerns about their stress, anxiety and low mood in the last 12 months. Response options were based on the published literature (Gearing et al., 2012) and assessed the form of help sought by participants experiencing distress, their preferences for seeking help and the barriers that stopped them from seeking help from mental health services in Australia (e.g. ‘I had language difficulties’) using yes and no response options.
Adjusting to life in Australia. Three items examined perceived opportunities (e.g. ‘Education’), current challenges faced living in Australia using open text responses and services that may have facilitated adjustment (e.g. ‘Information about community support services’).
Preferred model of service delivery (i.e. face-to-face vs Internet). Three items assessed respondents’ preferences to utilising Internet and/or face-to-face treatment for symptoms of stress, anxiety or depression.
Interest in future research. Three items enquired whether people were interested in future research and if they would like to enter the draw to win an iPad.
The Human Research Ethics Committee of Macquarie University granted ethics approval, and based on previous surveys (Lu et al., 2013; Spence et al., 2011; Wootton et al., 2011), this survey was designed to take approximately 15 minutes to complete.
Statistical analysis
The relationship between demographic variables (i.e. age and number of years since migration to Australia) and psychological distress was examined using Pearson’s correlations. The relationship between demographic variables (gender, marital status and educational levels) and level of psychological distress (i.e. low vs high; based on a cut-score of K-10 = 22) was examined using chi-square tests. Using the McNemar test (Sheskin, 2000), differences were analysed between the following variables: (1) the preferences for Internet and face-to-face treatments and (2) country of origin and preferences for Internet and face-to-face treatment. Respondents with missing data were omitted from specific analyses in which the missing information occurred.
Hypotheses were tested by creating categorical groups. The first and second hypotheses were tested by dividing respondents into FG (overseas-born) or SG (Australian-born) and comparing the intergenerational differences on K-10 and SDS scores, the frequency of mental health service utilisation, treatment barriers and preferences for psychological treatment. The third hypothesis was tested by dividing respondents into Low and High distress groups based on K-10 scores. The fourth hypothesis was tested by measuring the frequency of mental health service utilisation of Arab Australians in this study. The fifth hypothesis was tested with each preferred mode of delivery of treatment (i.e. Internet vs face-to-face) divided into either No or Yes/Maybe groups. Differences between groups were assessed using chi-square and McNemar tests, while mean differences in age, intergenerational status (i.e. FG vs SG) and symptom severity scales (i.e. K-10 and SDS) were assessed using one-way analyses of variance (ANOVAs). Analyses were performed using the Statistical Package for Social Sciences (SPSS) version 20.0 for Windows (SPSS Inc., Chicago, IL).
Results
Demographic characteristics
More females (n = 148; 59%) than males (n = 104; 41%) participated. The age range and mean age of respondents were 18–73 years and 37.2 years (standard deviation (SD) = 12.6), respectively. The majority of respondents were either married/de facto (n = 138; 55%) or single (n = 99; 40%) and Christian (n = 223; 88%) or Muslim (n = 24; 9.5%). Most were born in Australia (n = 176; 70%) or Lebanon (n = 60; 23%). Respondents born overseas (n = 76; 30%) reported that they had lived in Australia for a mean of 25.5 years (range: 1–60; SD = 14.2). A total of 41% of the sample (n = 107) had attained at least an undergraduate degree, 38% (n = 99) had attained a trade or other certificate, while 21% (n = 55) completed some level of High School. The greatest proportion of participants reported residing in NSW (n = 217; 86%), followed by Victoria (n = 24; 9.5 %), Australian Capital Territory (n = 7; 3%), South Australia (n = 3; 1%) and Queensland (n = 1; 0.5%). A total of 161 (65%) respondents reported spending at least 10 hours per week using the Internet. Most respondents rated their English proficiency (n = 196; 78%) and Internet skills (n = 154; 61%) as between average or very good.
Hypothesis 1: No differences in intergenerational differences of mental health status
There was no significant difference in K-10 scores between FG and SG respondents, F(1, 251) = 0.39, p = .53. However, SG respondents reported marginally higher SDS scores when compared to FG, F(1, 251) = 3.83, p = .052. In terms of mental health service utilisation, of the 81 respondents who experienced high levels of psychological distress and sought help, the FG respondents (4/22; 18%) were not significantly more likely to seek help from a mental health professional when compared to SG (14/59; 23%). In terms of treatment barriers, there were no significant differences in barriers to treatment between FG and SG respondents.
Hypothesis 2: Intergenerational differences in preferences for psychological treatments
The McNemar test (Sheskin, 2000), using binomial distribution, showed a significant difference between the preference for Internet treatment and intergenerational status (N = 76; p < .001). Of the 76 FG and SG respondents who experienced high levels of psychological distress and responded to the question about preference for Internet-delivered treatment, FG Arab Australians (16/22; 73%) were significantly more likely to indicate that they would try Internet-delivered treatment compared to SG (30/54; 55%). Finally, there was no significant intergenerational difference in preferences for Internet versus face-to-face treatments.
Hypothesis 3: Higher levels of psychological distress among Arab Australians
Psychological distress levels did not differ significantly as a function of gender, marital status (categorised into married and not married), educational levels (categorised into up to year 12, at least a tertiary certificate and at least a bachelor’s degree) and country of birth (categorised into FG and SG), (p range = .48–.88). The sample mean on the K-10 was 19.1 (range: 10–45; SD = 7.6). Eighty-one of the 252 (32%) respondents reported high psychological distress on the K-10 (K-10 ≥ 22; M = 28.5; SD = 5.4). Also 43% of respondents reported moderate to high levels of functional impairment (M = 9.5; SD = 1.8), as measured by the SDS (total score ≥ 7).
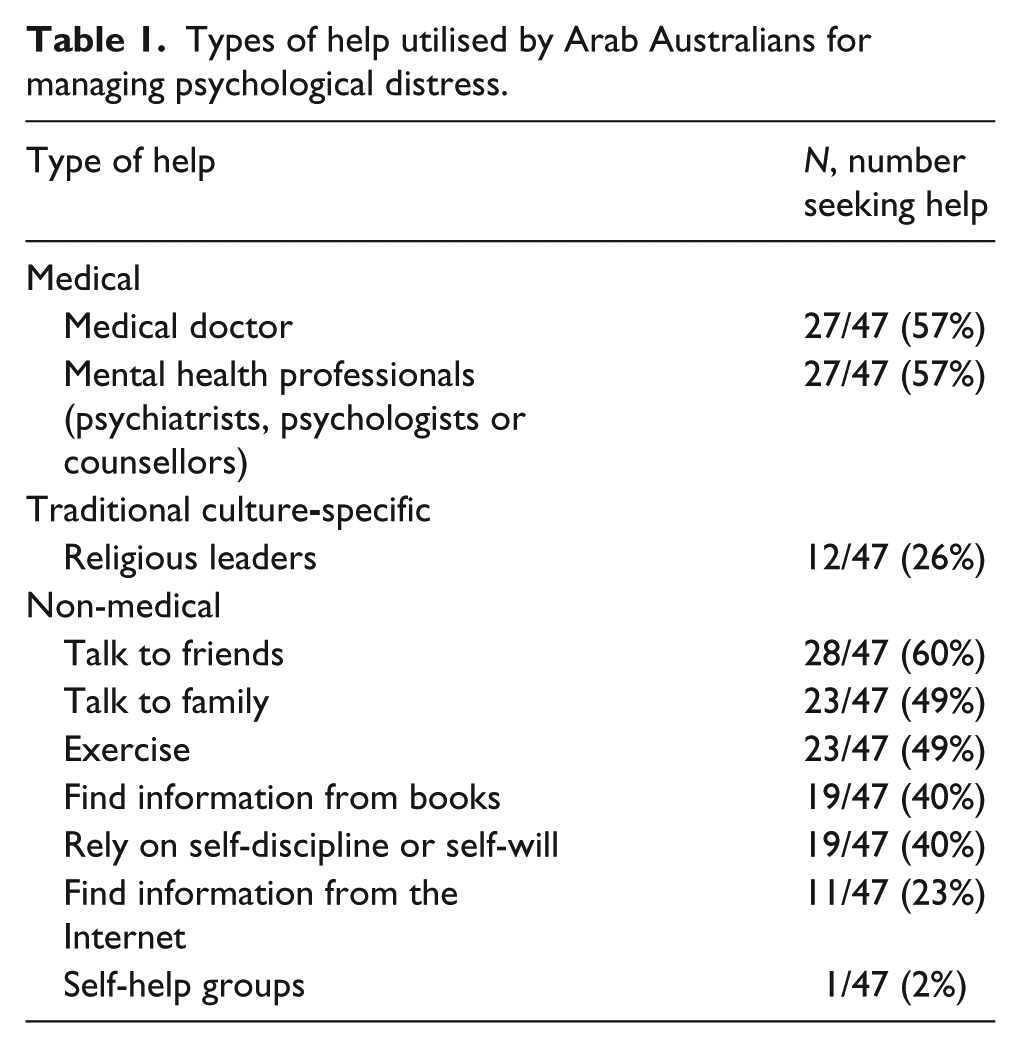
Hypothesis 4: Lower mental health service utilisation among Arab Australians
Table 1 shows that of the 147/252 (58%) respondents who reported concerns about their stress, anxiety and low mood in the last 12 months, only 47/147 (32%) sought some form of help. Overall, 47/252 (18%) sought help from a mental health professional (i.e. psychiatrists, psychologists or counsellors) in the previous year. The most frequently endorsed help-seeking behaviours of this sample, in order, included talking to friends, medical doctors and mental health professionals, followed by talking to family, engaging in exercise, relying on self-discipline or information from books and consulting religious leaders and the Internet.
Types of help utilised by Arab Australians for managing psychological distress.
Respondents with high psychological distress who answered questions about barriers to accessing treatment (n = 47) cited the reasons described in Table 2. These have been divided into reasons relating to cultural barriers, mental health literacy and practical barriers.
Reported barriers to seeking mental health services reported by respondents with high psychological distress.

Hypothesis 5: Psychological treatments are acceptable to Arab Australians
The majority of participants who answered the question about preferences for treatment (220/233; 94%) indicated they would or might be prepared to try psychological treatments for their concerns about stress, anxiety or depression. The McNemar test (Sheskin, 2000), using binomial distribution, showed a significant difference between participants who had a preference for Internet or face-to-face treatments (N = 233; exact p < .001). Specifically, analyses revealed that a greater number (209/233; 90%) of respondents indicated they would or might try face-to-face treatment than those who indicated they would or might try Internet-delivered treatment for their concerns about stress, anxiety or depression (128/233; 55%). Furthermore, of the 81 respondents who experienced high levels of psychological distress, only 76 answered the question related to preferred mode of psychological treatment. These respondents also indicated a significantly greater preference (N = 76; exact p < .001) for face-to-face treatment (66/76; 86%) over Internet-delivered treatment (46/76; 61%).
Discussion
The aim of this study was to contribute to the emerging data about the intergenerational (FG vs SG) and cross-cultural (Australians vs Arab Australians) differences in mental health status, treatment-seeking experiences and preferences, the barriers to treatment and the acceptability of face-to-face and Internet delivery of treatment to Arab Australians. The first hypothesis that FG would have lower psychological distress and functional impairment when compared to SG was not supported, despite the marginal trend that FG reported lower disability levels. The first part of the second hypothesis that FG would have lower rates of mental health service utilisation and greater barriers to treatment when compared with their SG counterparts was not supported. The second part of hypothesis 2 that FG would be less likely to prefer psychological treatments when compared with their SG counterparts was also not supported. In fact, FG Arab Australians were more likely to prefer Internet-delivered treatment when compared with their SG counterparts. However, the hypotheses that, compared to the general Australian population, Arab Australians would have (3) relatively higher levels of psychological distress; (4) there would be lower rates of mental health service utilisation and a preference for ‘non-medical’ support from family, friends and religious leaders and (5) that a significant proportion of respondents would be willing to try psychological treatments for symptoms of stress, anxiety and low mood were all supported.
No significant intergenerational differences were found in mental health status, barriers to treatment and preferences for psychological treatment (except for Internet-delivered treatment), indicating a fairly homogeneous sample. This study did not support previous findings, which indicated greater risk of suicide and psychotic disorders for SG when compared to FG (Bourque et al., 2011; Hjern & Allebeck, 2002; Nasseri & Moulton, 2011), but found no intergenerational differences in psychological distress levels and a marginal trend, indicating greater functional impairment levels in SG respondents. The similar intergenerational treatment barriers, lower mental health literacy and treatment utilisation rates may account for this unexpected finding. These three contributing factors may also explain the high psychological distress across generations reported in this sample.
Irrespective of the generational status, Arab Australians in this sample reported having a lack of awareness about local treatment services, did not think their problem was serious enough and reported having a lack of awareness about mental health symptoms, indicating intergenerational poor mental health literacy. Furthermore, Arab Australians reported other barriers such as a lack of time, cost and transportation; shame for family and loss of face; and being seen as crazy if others found out. Combining these treatment barriers and the lack of mental health literacy may contribute to the lower intergenerational utilisation rates and higher psychological distress levels found in this study. This pattern of findings replicates previous findings with an Arab sample in Israel (Al-Krenawi, 2002), Qatar (Bener & Gbuloum, 2011) and a cross-national study of Arab students in Israel, Palestine, Kuwait and Egypt (Al-Krenawi, Graham, Al-Bedah, Kadri, & Sehwail, 2009). The encouraging finding is that across generations the Arab Australians were willing to try psychological treatments. Overall, their preference was for face-to-face treatment, with FG having a greater preference for Internet-delivered treatment when compared to SG.
This study found cross-cultural differences with higher levels of psychological distress reported among Arab Australians completing the survey when compared to the general Australian population. Indeed, respondents reported mean K-10 scores (M = 19.1; SD = 7.6) slightly higher than those reported by the general Australian population (M = 14.2; SD = none reported) (Australian Bureau of Statistics, 2008). Moreover, 33.7% of the respondents reported high to very high levels of psychological distress (K-10 ≥ 22) compared to 9.6% in the general Australian population (Australian Bureau of Statistics, 2008). Respondents in this survey also indicated elevated levels of functional impairment indicating that psychological distress is disrupting some Arab Australians’ vocational, social life, recreational, family and home responsibilities. These findings are consistent with results of a recent survey identifying high levels of psychological distress among people born in Lebanon and living in NSW (Centre for Epidemiology and Research, 2010) and highlight that, compared with the general population (Australian Bureau of Statistics, 2008), significantly higher symptoms of psychological distress are present among this sample of Arab Australians.
Also, compared with the general Australian community (Slade et al., 2009), and consistent with other similar surveys (Lu et al., 2013; Spence et al., 2011) and other Arab-based surveys (Al-Krenawi, 2002; Aloud & Rathur, 2009), Arab respondents reported lower rates of mental health service utilisation. In particular, only 22% of the sample that reported high levels of psychological distress sought treatment from a mental health professional. This is lower than the rates of treatment seeking among the general Australian population, in which 35% with symptoms of stress, anxiety and depression reported seeking treatment (Slade et al., 2009). These findings of lower rates of utilisation of mental health services in an Arab migrant population compared with the dominant host population replicated previous findings of Arabs and Jews living in Israel (Al-Krenawi, 2002). This lower rate of mental health service utilisation may be related to the barriers to treatment seeking identified by respondents.
Of those who reported they sought treatment, many preferred to seek informal and non-medical help from friends and family, a finding replicated with Chinese immigrants (Chan & Parker, 2004), Chinese students in Australia (Lu et al., 2013), Arabs in Qatar (Bener & Gbuloum, 2011) and Arab Muslims (Al-Krenawi et al., 2009; Al-Krenawi & Graham, 2011; Aloud & Rathur, 2009). Surprisingly, respondents reported a preference for seeking help from mental health professionals compared to what might be considered more traditional options, such as seeing a religious leader. This is not consistent with some previous research that, for example, found that Arab Americans had a more negative view of mental health professional
However this is consistent with other studies that have found a differential pattern of using mental health service, based on nationality (Al-Krenawi et al., 2009), gender (Al-Krenawi, 2002; Bener & Gbuloum, 2011) and religion (Al-Krenawi & Graham, 2011). For example, Palestinian and Israeli Arabs reported a greater preference to seek mental health treatment for a psychological problem when compared to their Kuwaiti and Egyptian counterparts (Al-Krenawi et al., 2009), Arab males in Israel and Qatar were more likely to seek mental health treatment when compared to their female counterparts (Al-Krenawi, 2002; Bener & Gbuloum, 2011), and Arab Christian students in Israel reported being more open to mental health treatment and less likely to endorse traditional healers when compared to their Muslim counterparts (Al-Krenawi & Graham, 2011). This study did not find any differences based on country of origin (i.e. Australian-born vs overseas-born), gender or religion in preferences for seeking help from mental health services, with Arab females and Muslims who are experiencing high psychological distress as likely to seek psychological treatment as their male and Christian counterparts, respectively. Unfortunately, the small sample of overseas-born respondents (n = 76) prevented subgroup analyses based on Arab country of origin.
The lack of gender and religious differences in the current sample could be attributed to the acculturation levels. Al-Krenawi and Graham (2000) postulated that as Arabs become more acculturated to Western culture, they are more likely to seek psychological treatment. Unfortunately, this was not examined in this study; hence, we can only tentatively suggest that acculturation may be a relevant factor, but future research would need to explore the relationship between increased preference for psychological treatment and acculturation. Moreover, in line with emerging evidence in some Arab countries (Al-Krenawi, 2002; Al-Krenawi et al., 2009; Al-Krenawi & Graham, 2011), Arabs are becoming more open to mental health treatment, and in this study, there is a significant number of Arab participants who endorsed both face-to-face and Internet-delivered treatments as acceptable.
Overall, a significant proportion of respondents reported they would try psychological treatments. There was a preference for face-to-face over Internet-delivered treatments, which may reflect the familiarity of the former. Notwithstanding their preference for face-to-face treatment, respondents in this sample experiencing high psychological distress are willing to try Internet-delivered treatments (61%). These findings are encouraging and suggest that Arab Australians are prepared to access treatment in non-traditional formats.
Limitations
Despite attempts to engage all relevant Arabic-speaking organisations in Australia, the sample was relatively small and had a high proportion of people of a Christian faith. Thus, the generalisability of the results of this study is somewhat limited, and caution is needed in interpreting the results. It is also important to note that Arab Australians are a highly heterogeneous group, and the relatively small number of participants in this study prevent potentially important subgroup analyses (Blignault, Ponzio, Rong, & Eisenbruch, 2008). Furthermore, by virtue of the methodology involving an Internet survey selection bias may be present with respondents having pre-existing positive attitudes towards research, mental health services and Internet-delivered treatments. A final limitation is the lack of independent validation of the accuracy of self-report data on service utilisation rates. Notwithstanding these limitations, these data represent an important contribution to the limited amount of what is known about the emotional wellbeing, help-seeking history, barriers and preferences for psychological treatment of Arab Australians.
Implications
The intergenerational barriers to treatment identified in this study, that is, low mental literacy, lack of time, and stigma and shame, have been found to occur within and across cultural groups within Australia and also internationally (Chan & Parker, 2004; Gearing et al., 2012; Guterman et al., 2010; Lu et al., 2013; Spence et al., 2011). This suggests that barriers to accessing treatment might be transcultural and that seeking help poses challenges irrespective of culture, although there may be some specific language or cultural barriers for people from culturally and linguistically diverse backgrounds. This indicates the importance of identifying barriers to treatment for improving mental health among these groups and also the potential of innovative models of service delivery. A significant finding of this study is that more than 60% of respondents who reported high levels of distress indicated they would try Internet-delivered treatment, and, given the promising research regarding other cultural groups (Choi et al., 2012), this points to the potential of using Internet-delivered treatments for providing psychological treatment to Arab Australians. Reflecting this, our research team are currently conducting a series of research trials to examine the acceptability, efficacy and feasibility of Internet-delivered treatment for Arab Australians with anxiety and depression.
Conclusion
Arab Australians in this study experience higher levels of psychological distress and underutilise mental health services when compared to the general Australian population. This may be due to common barriers reported across cultural groups, particularly lack of time, shame and stigma, and limited mental health literacy. As Arab Australians are becoming more open to psychological treatment and are willing to try face-to-face and Internet-delivered treatments, novel ways of engaging this cultural group and improving access to new models of mental health treatment services are critical. One such way could be the development of Internet-delivered treatments for Arab Australians.
Footnotes
Acknowledgements
The authors wish to acknowledge all participants, translator (Liliane Keyrouz), bilingual speakers (Edmond Nehme, Mona Kayrouz), bilingual psychologist (Medhat Metry), Sheik Misab Lagha, Monsignor Shora Maree, service providers, Arabic-speaking organisations and other agencies that supported this study. R.K. designed and promoted the study, assisted in the backward translation, conducted the analyses and drafted the article. N.T. reviewed the design and the article. B.D., L.J. and R.L. reviewed the article. L.N.K. and E.N. assisted in the translation of the survey and promotion of the study. All authors have contributed to and have approved the article.
Funding
The funding for the study was provided by Macquarie University as part of the lead author’s (R.K.) PhD candidature.