
Abstract
Aims:
This review will focus on the rates, clinical characteristics, risk factors and methods of self-harm and suicide in different ethnic groups in the United Kingdom, providing an update synthesis of recent literature.
Methods:
Studies that met the inclusion criteria between 2003 and 2013 were reviewed using the following databases: MEDLINE, PsycINFO, EMBASE and CINAHL. The methodological quality of each study was then assessed using a structured scoring system.
Results:
A total of 2,362 articles were retrieved, 10 of which matched the inclusion criteria were reviewed. Significant differences were found in the rates of self-harm between ethnic groups with Asian males being least likely to self-harm and Black females being most likely to self-harm. Also, Black and South Asian people were less likely to repeat self-harm. Factors that may help protect or predispose individuals to self-harm or attempt suicide (such as religion, mental health and coping styles) also differ between ethnic groups.
Conclusions:
There are clear ethnic differences in self-harm and suicide, which may be affected by factors such as cultural pressures and prevalence of mental illness. An awareness of these differences is vital to help prevent further attempts of self-harm and suicide. Further research into differences between ethnic and cultural groups and self-harm continues to be important.
Introduction
Self-harm is a common clinical problem that poses a significant public health concern (Kapur et al., 1998; Perry et al., 2012) and places a substantial burden on the health services (Bhui, McKenzie, & Rasul, 2007). It can also be the most significant risk factor for future self-harm and completed suicide (Kapur et al., 2005; Owens, Horrocks, & House, 2002). Self-harm has been defined as any form of self-destructive behaviour (Lundh, Karim, & Quilisch, 2007) that refers to an individual deliberately hurting or mutilating their body with or without the intention of dying, which includes behaviour such as skin carving, puncturing, scratching, burning, hitting oneself and ingesting harmful substances (Baguelin-Pinaud, Seguy, & Thibaut, 2009; Lengel & Mullins-Sweatt, 2013). However, problems arise from classifying self-harm as there is no clear consensus (Latimer, Meade, & Tennant, 2013) or clinical agreement regarding what constitutes self-harm (Husain, Waheed, & Husain, 2006). Therefore, given that the United Kingdom has one of the highest rates of self-harm and suicide in Europe (Schmidtke et al., 1996), and around 14% of individuals in England and Wales are of an ethnic minority (UK Data Service Census Support, 2011), it is important to fully understand factors that contribute to its occurrence.
Geographical variations in the rates of self-harm and completed suicide have been detected across the world, for example, annual rates of suicide reported in some South American countries were low, and high rates were observed in Russia and some eastern bloc countries (McKenzie, Serfaty, & Crawford, 2003). Also, some of the highest rates of suicide and self-harm have been seen in Black and minority ethnic (BME) groups and South Asian women in the United Kingdom (Baldwin & Griffiths, 2009; Bhugra, Desai, & Baldwin, 1999). However, the reasons for the cultural differences in self-harm and suicide remain unclear, thus exemplifying the need for understanding this association and highlighting the importance of attempting to address this difference.
Several risk factors pertaining to the prevalence of self-harm and suicide have been identified. Socioeconomic status affects the levels of suicide with those from a lower socioeconomic background being more likely to attempt suicide (Aschan et al., 2013). Also, those who are unemployed have been shown to be more at risk of self-harming as well as those who are single, divorced, separated or widowed (Aschan et al., 2013; Johnston, Cooper, Webb, & Kapur, 2006). These factors may differ in minority groups. Cooper, Spiers et al. (2013) found marital status to be a prominent factor when predicting self-harm in South Asian individuals but less so for White individuals, thus exemplifying the differences between ethnic groups in rates of self-harm. Moreover, they identified other risk factors such as alcohol abuse to be a stronger predictor of self-harm in South Asian groups. In addition, a history of mental illness has been shown to predict self-harm and suicide across all ethnic groups (Cooper et al., 2006).
Clinical management of patients who self-harm should ideally take into account their cultural and ethnic background. Thus, the relative lack of research into the potential differences in risk factors for self-harm and suicide clinicians can call upon is a concern. This article aims to update and advance previous reviews by reporting the findings of a systematic review of studies investigating self-harm and suicide among at least two ethnic groups in the United Kingdom. We include studies published after the start date of the last published systematic review in 2007 (K. Bhui et al., 2007). The aim of the review was to build on previous work and establish recent evidence for the prevalence, clinical characteristics, risk factors and methods of self-harm by each of the largest of minority ethnic groups in the United Kingdom.
Method
Although the aim of this article is to review self-harm, many studies investigate self-harm and suicide together. Therefore, our search strategy targeted publications on both self-harm and suicide.
The full text of studies were retrieved if, following abstract screening, the study was confirmed to (a) compare rates or clinical risk factors or methods of self-harm and suicide, (b) include data on two more ethnic groups living in the United Kingdom and (c) studies were published in English between 2003 and the start date of this review, 2013. These abstracts were screened (C.R.K. and A.A.) and if the abstract was ambiguous, the full text of the study was examined.
The following databases were searched: MEDLINE, PsycINFO, EMBASE and CINAHL. The following search terms were used: (a) SUICIDE or (b) SUICIDAL IDEATION or (c) SUICIDAL THOUGHTS or (d) SUICIDAL BEHAVIOUR or (e) SELF-HARM or (f) DELIBERATE SELF-HARM. This resulted in 71,925 articles being found. Then, (a) ETHNICITY or (b) ETHNIC or (c) RACE or (d) CULTURE or (e) CULTURAL was entered into the same search engines which identified 252,758 articles. The findings were then combined with the previous findings revealing 2,362 articles, 10 of which matched the strict inclusion criteria were reviewed (see Figure 1).

Flow chart of the selection process.
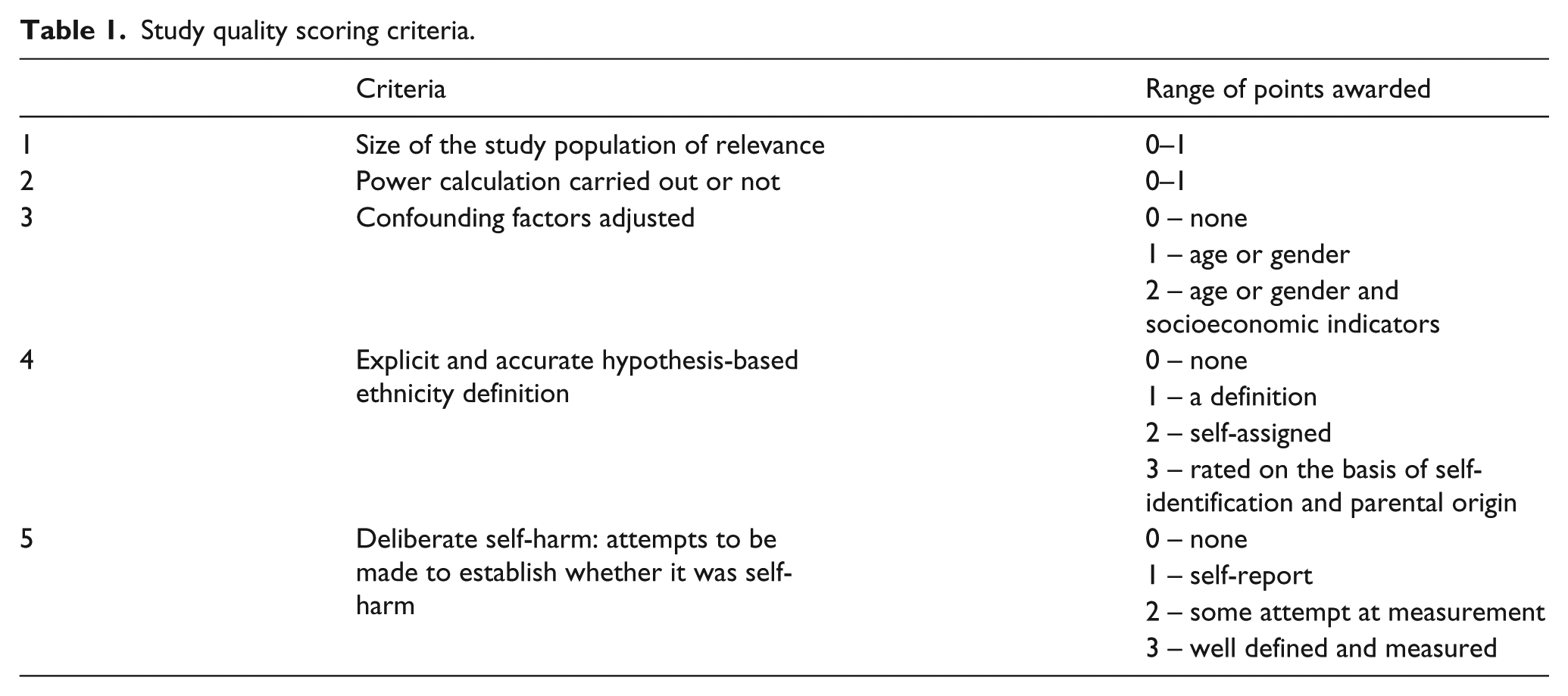
Two reviewers (A.A., C.R.K.) independently reviewed all articles, screened and agreed with the articles included in the review. An independent reviewer (R.U.) was available to settle any disagreements that arose. It was not necessary to contact authors of the studies included in the review for additional information. The methodological quality of studies was assessed independently using a standard scoring system adopted by Raine (2000) (see Table 1). Results were then tabulated into study characteristics (Table 2) and risk factors and rates of self-harm across ethnic groups (Table 3).
Study quality scoring criteria.
Study characteristics in self-harm and ethnic groups.
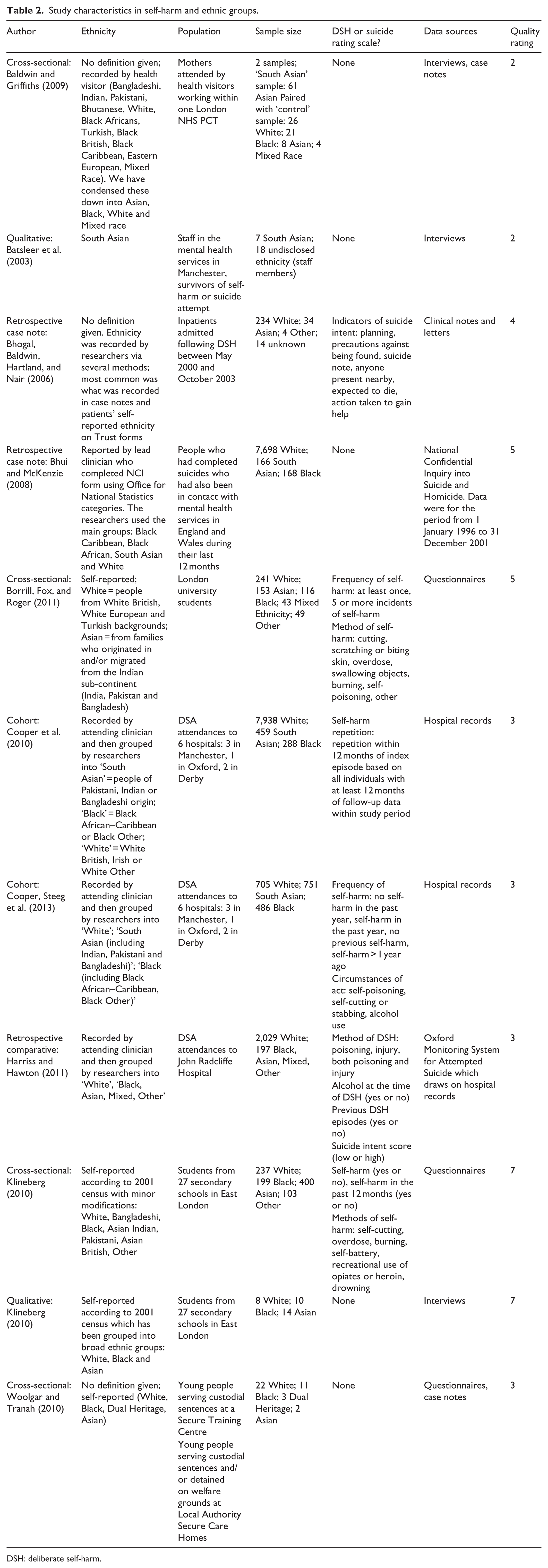
DSH: deliberate self-harm.
Risk factors and rates of self-harm across ethnic groups.
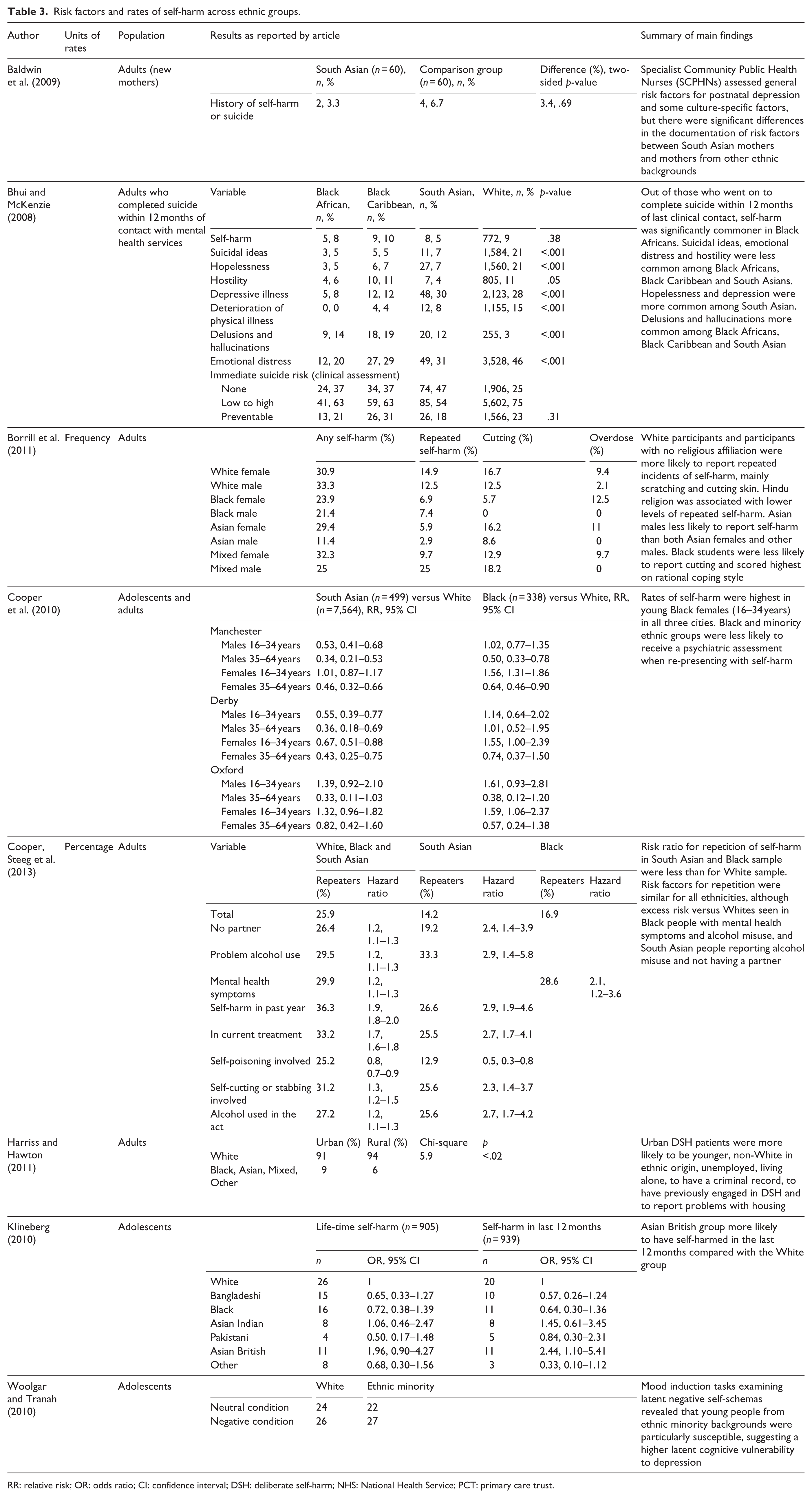
RR: relative risk; OR: odds ratio; CI: confidence interval; DSH: deliberate self-harm; NHS: National Health Service; PCT: primary care trust.
Data on study characteristics and quality rating are presented in Table 2. Data on clinical risk factors for self-harm and suicide, methods of self-harm and suicide and prevalence or rates of self-harm and suicide were extracted and are presented in Table 3.
Results
Clinical characteristics and risk factors
Rates of self-harm
The rates of self-harm were considered by three of the studies reviewed, and all agree that the rates of self-harm differ in gender and ethnicity. Borrill, Fox, and Roger (2011) noted that low levels of self-harm was found in Asian males compared to and all other male groups. In contrast to this, Klineberg (2010) found that Asian British males were most likely to self-harm. Cooper et al. (2010) found that Black females were most likely to self-harm than Asian and White groups.
Repeated attempts and completed suicide
Two studies reviewed focused on repeated attempts of self-harm. Borrill et al. (2011) identified the highest rates of repeated attempts of self-harm among White individuals with no religious affiliation. They found that Hindus and Sikhs were less likely to repeat self-harm, but Christian females displayed high levels of repeated self-harm defined as being more than five incidents. Repeating self-harm was found in 11.7% of female Christians and 13.2% non-religious females. Cooper, Steeg et al. (2013) also reviewed differences between ethnic groups and repeated attempts of self-harm. They found that, compared to White individuals, Black and South Asian individuals were less likely to repeat self-harm when matched on clinical and social characteristics.
A broad definition of suicide was adopted whereby cases in which the coroner recorded a verdict of death by suicide were employed by K. S. Bhui and McKenzie (2008). This is following the guidelines by Linsley, Schapira, and Kelly (2001). They found that of those who died by suicide within 12 months of last clinical contact, the rate of self-harm was significantly higher in Black African individuals. They also found that those of Black African decent experienced suicidal ideas (5%), emotional distress (20%) and hostility (6%) than Black Caribbean, South Asian and White individuals. Hopelessness (17%) and depression (30%) were more common in South Asian individuals. Delusions and hallucinations were also more common among the Black African (14%), Black Caribbean (19%) and South Asian (12%) communities.
Psychiatric disorder and management
Two studies fell into this category; these were Cooper et al. (2010) and Cooper, spiers et al. (2013). Both studies assessed psychiatric disorder using clinical diagnosis rather than any assessment scales. They focused on psychiatric disorders and management and self-harm. Cooper, Speirs et al. (2013) found that Black individuals who self-harm and experience a psychiatric condition were more likely to self-harm than the White individuals who self-harm. They also found that South Asian participants were more likely to self-harm than White participants if they abused alcohol and did not have a partner. Also, Cooper, spiers et al. (2013) noted that the risk of repeated self-harm was linked with alcohol misuse, particularly in BME groups. Cooper et al. (2010) found that BME groups were also less likely to receive a psychiatric assessment and follow-up care than White individuals. However, Cooper, spiers et al. (2013) speculate that this may be due to BME groups being disillusioned by the mental health-care services when previously seeking treatment or as a result of not possessing the characteristics that are known to increase the risk of self-harm.
Location
Urban or rural differences in mental health specifically suicide and self-harm, suggested by Harriss and Hawton (2011), highlight the potential effect of location on mental health. Harriss and Hawton (2011) found that self-harm in urban areas was more likely to occur in those who are non-White, unemployed, living alone, who have a criminal record and those who experience housing problems.
Methods of self-harm
Only one study addressed the methods used when self-harming. Borrill et al. (2011) reported scratching as the most common form of self-harm among White individuals, and Black males were the least likely to employ this method of self-harm.
Coping styles
Coping styles have been found to be vital in self-harming behaviour. Poor coping mechanisms have also been linked with distress and poor skills in managing emotions (Borrill et al., 2011). Borrill et al. (2011) explored coping styles in self-harming behaviour and found that Black students adopted a rational style of coping compared to White and Asian students. Furthermore, Asian students possessed an avoidance coping style and scored highly on emotional inhibition scales compared to White students.
Methodological quality
Using the quality assessment set out by Raine (2000), six studies obtained a low score (3 or less) (Baldwin & Griffiths, 2009; Batsleer, Chantler, & Burman, 2003; J. Cooper et al., 2010; Cooper, Steeg et al., 2013; Harriss & Hawton, 2011; Woolgar & Tranah, 2010), three studies obtained a medium score (between 4 and 6) (Bhogal, Baldwin, Hartland, & Nair, 2006; K. S. Bhui & McKenzie, 2008; Borrill et al., 2011) and two studies scored highly (7 and over) which were both carried out by Klineberg (2010). Four studies incorporated adolescents into their sample and scored between 3 and 7 (Borrill et al., 2011; Klineberg, 2010; Woolgar & Tranah, 2010). This review includes three qualitative studies which used the format of semi-structured interviews, namely, Klineberg (2010), Batsleer et al. (2003) and Baldwin and Griffiths (2009). Two components of the quality assessment (power calculation and degree of adjustment for obvious confounders) could not be applied to the qualitative studies.
Three studies employed a questionnaires design (Borrill et al., 2011; Klineberg, 2010; Woolgar & Tranah, 2010). Clinical case notes were used by four studies, namely, Bhogal et al. (2006), Bhui et al. (2008), Cooper, Steeg et al. (2013) and Cooper et al. (2010). Bhui et al. (2008) used national statistics derived from the National Confidential Inquiry which records suicides among people in contact with services in the preceding 12 months. Harriss and Hawton (2011) employed a retrospective comparative study design.
Four studies adopted a cross-sectional design; Woolgar and Tranah (2010), Baldwin and Griffiths (2009), Borrill et al. (2011) and one study by Klineberg (2010). Structural content analysis of semi-structured mixed method interviews carried out on 60 matched pairs Specialist Community Public Health Nurses (SCPHN) records (Baldwin & Griffiths, 2009). Klineberg (2010) and Borrill et al. (2011) employed a cross-sectional, questionnaire design. Woolgar and Tranah (2010) also used a cross-sectional design whereby participants were randomly assigned to one of four conditions following mood induction. Participants completed a questionnaire and then an intellectual assessment exercise. After each exercise, mood checks were administered. Bhogal et al. (2006) used retrospective case note study.
Discussion
General findings
This review supports the clear finding of an ethnic difference in self-harm presentation in the United Kingdom, with much of the research supporting the assumption that Asian males are least likely to self-harm and Black females are most likely to self-harm (Borrill et al., 2011; J. Cooper et al., 2010). Moreover, the research reviewed also suggests that there are differences in repeated attempts of self-harm with Black and South Asian individuals being less likely to repeat self-harm. Protective and predisposing factors of self-harm have also been identified such as religion (Borrill et al., 2011) and coping styles (Borrill et al., 2011; Woolgar & Tranah, 2010). An individual’s location seems to be an important factor in the rates of self-harm and suicide as identified by McKenzie et al. (2003) and has also been supported by Harriss and Hawton (2011). The presence of a psychiatric disorder and its management seems to affect levels of self-harm and suicide (Cooper et al., 2006) which differs between ethnic groups (Cooper, Spiers et al., 2013).
Considering the existence of an ethnic difference in self-harm and risk of suicide is vital for the clinical management of patients; thus, our findings will have clinical relevance to front-line mental health and emergency teams. Differences in rates of self-harm between ethnic groups may be a result of BME groups being left disillusioned by the health-care services after treatment (Cooper, Spiers et al., 2013) or because of differences in help-seeking behaviour. Therefore, our evidence supports the view that ethnic background must be taken into consideration when treating individuals. The research reviewed identified differences between ethnic groups in the methods of self-harm with White males being most likely to report scratching unlike Black males (Baguelin-Pinaud et al., 2009; Lengel & Mullins-Sweatt, 2013). These findings suggest that there are differences in the rate, contributing factors and the methods used by different ethnicities and contribute to the knowledge base for factors that lead an individual to self-harm or attempt suicide.
It has previously been asserted that clinical services need to widen access and better reflect the population they serve (Fernando, 2005). Common mental health conditions, such as depression, personality disorder and psychosis, often include self-harm and suicidal ideation. Thus, services targeting self-harm need to be in the context of better mental health services for people from minority groups. The use of community settings without stigma (Lamb, Bower, Rogers, Dowrick, & Gask, 2012), such as those integrated to mosques, churches and barbershops, has been suggested, but it is clear that further evidence is still required (Lamb et al., 2012). However, it has been shown that primary care physicians need to be alert to patients from minority ethnic groups with mental illness presenting with somatisation (Cooper, Spiers et al., 2013).
Limitations
Several factors prevented a meta-analysis from being conducted including the methods used by the studies reviewed, the samples of these studies and distinct outcomes. The samples from which the studies were drawn from were different. This has been exemplified by some studies looking at the levels of re-attendance of emergency departments (Harriss & Hawton, 2011), whereas other studies looked at methods of deliberate self-harm (DSH) (Borrill et al., 2011; Klineberg, 2010). Also, various samples were used such as young people serving custodial sentences (Woolgar & Tranah, 2010), university students (Borrill et al., 2011) and hospital patients (Cooper, Spiers et al., 2013; Harriss & Hawton, 2011). Classification of ethnic groups differed between each study, for example, some studies categorised an ethnic group called ‘Black’ (Cooper Spiers et al., 2013; Harriss & Hawton, 2011), whereas other studies adopted a more precise category definition such as ‘Black Somali’ or ‘Black British’ (Klineberg, 2010). The use of broad definitions to define ethnicity may have been used to overcome small numbers or because of coding used to categorise ethnic groups by medical staff, such as in Cooper, Steeg et al. (2013). However, clustering together potentially diverse ethnic groups does not account for cultural differences between ethnicities, thus limiting conclusions.
Future research
To improve on the previous research, a precise definition of ethnic groups would allow more focused conclusions and confident inferences to be drawn from the data. An unclear definition of ethnic groups restricts the ability to carry out appropriate and definitive statistical testing necessary for meta-analyses and clouds the true nature of ethnic differences in self-harm and suicide. Also, given the rise in Eastern European immigrants to the United Kingdom, it seems crucial to explore rates of self-harm and suicide in these groups and to compare this to other ethnic groups, which may be important when devising appropriate treatment plans and managing self-harm patients. As noted, there is no consistency in terms used when defining ethnic groups. Future research must use more informative and meaningful terms when defining ethnic groups and take into account what generation migrant they are. Learning which generation of migrant would be useful in understanding the stability of cultural identity over different generations and how this may influence rates of self-harm which is particularly important given the increasing levels of migration. Various interventional studies have been used to help tackle levels of self-harm and suicide (Hawton, Saunders, & O’Connor, 2012). Interventions based on psychological principles initially showed promise (Wood, Trainor, Rothwell, Moore, & Harrington, 2001), but this was failed to be replicated (Hazell et al., 2009). The usefulness of anti-depressants in treating individuals who are self-harming or at risk of suicide remains unclear (Wheeler, Gunnell, Metcalfe, Stephens, & Martin, 2008). Psychological interventions promoting social inclusion and help-seeking behaviour may be of particular benefit to individuals of BME groups who are at risk of suicide or who self-harm. This indicates a clear gap in our knowledge and demonstrates that future research is needed to explore ethnicity and suicide, and the role of self-harm therein.
Conclusion
We have shown that there is a potential ethnic difference in self-harm in the United Kingdom, and it is thus important that the clinical management of patients who have self-harmed or attempted suicide be informed by knowledge of this difference. Also, factoring the patients’ ethnic background into the clinical management of this patient groups may help develop appropriate treatment options and thus prevent further attempts of self-harm (Cooper, Stieg et al., 2013). Last but not least, several other factors associated with self-harm such as socioeconomic grouping, marital status and premorbid mental illness (Cooper, Spiers et al., 2013) have also been implicated in the different rates of the prevalence of self-harm and should be controlled for in future larger studies.
Footnotes
Acknowledgements
R.U., A.A. and C.R.K. contributed to the development of the review including design and drafting of this article. C.R.K. and A.A. screened and reviewed the articles and R.U. was available to resolve any disagreements and approved the articles reviewed in the review. R.U., A.A. and C.R.K. contributed to the development of this article. All authors read and approved this article.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.