
Abstract
Background:
Globally, smoking remains a significant issue for mental health populations. Many mental health trusts in England are facing challenges of implementing the National Institute for Health and Care Excellence guidance according to which all mental health settings, no matter the type, should be entirely smoke-free and provide comprehensive smoking cessation support.
Aim:
The aim of this paper was to determine if unit type and unit manager smoking status influence mental health smoke-free policy implementation.
Method:
This paper reports on the secondary analysis of data from a cross-sectional survey of 147 mental health inpatient settings in England, in 2010. The original study’s main aim was to understand unit managers’ perceived reasons for success or failure of smoke-free policy.
Results:
Unit managers (n = 131) held a positive stance towards supporting smoke-free policy and most perceived that the policy was successful. Non-smoker unit managers were more likely to adopt complete bans than smoker unit managers, whereas smoker unit managers were more likely than non-smoker unit managers to think that stopping smoking aggravated patients’ mental illness. Smoking rates for staff and patients remain high, as perceived by unit managers, regardless of unit type. Proportion of units offering nicotine replacement therapy and peer support to patients was significantly higher in locked units compared to semi-locked or residential rehabilitation. Applied strategies significantly vary by type of unit, whereas unit managers’ knowledge, attitude and practices vary by their smoking status.
Discussion:
There are nuanced differences in how smoke-free policy is enacted which vary by unit type. These variations recognise the differing contexts of care provision in different types of units serving different patient groups. Addressing staff smoking rates, promoting consistency of staff response to patients’ smoking and providing staff education and support continue to be key strategies to successful smoke-free policy.
Conclusions:
Our results demonstrate the importance of taking into account the type of unit and acuity of patients when enacting smoke-free policy and addressing staff smoking.
Keywords
Introduction
Smoking is the largest preventable cause of death in the United Kingdom (Health and Social Care Information Centre (HSCIC), 2014; ASH, 2014). Research indicates that people diagnosed with a mental disorder are more likely to smoke, and have more than a two-fold increased risk of chronic diseases compared to the general population (HSCIC, 2014; McManus, Meltzer, & Campion, 2010; Royal College of Physicians, Royal College of Psychiatrists, 2013; Ruther et al., 2014; Scott et al., 2012). Furthermore, 42% of adult tobacco consumption in England is by people with mental disorder (McManus et al., 2010). It is estimated that among the 10 million smokers in England, 3 million experience one or more diagnosed mental disorders (Royal College of Physicians, Royal College of Psychiatrists, 2013). This highlights the need for a comprehensive response to address this issue. While general population smoking prevalence has decreased, this has not occurred for people with mental disorder (Morgan et al., 2013; Royal College of Physicians, Royal College of Psychiatrists, 2013; Szatkowski & McNeill, 2014). Globally, this growing health-related inequity in smoking prevalence rates has attracted focused attention from policy makers. Consequently, several countries have banned smoking in workplaces including hospital-based mental health units (World Health Organization (WHO), 2013). England implemented a smoke-free policy in July 2007, to reduce the impact of second-hand smoke on patients and staff, which was extended to all types of inpatient units from 2008 (UK Policy Governance Association (UKPGA), 2006). However, many mental health trusts in England are facing challenges of implementing the National Institute for Health and Care Excellence (NICE; 2013) guidance on smoking cessation in secondary care, according to which all mental health settings, no matter the type, should be entirely smoke-free and provide comprehensive smoking cessation support.
Despite continuous advocacy by health professionals and researchers internationally for smoke-free mental health units, there remain tensions in its implementation due to an entrenched ‘smoking culture’ (Lawn, 2004; Royal College of Physicians, Royal College of Psychiatrists, 2013). Research has shown that mental health staff play a significant role in policy success and that, despite more than a decade of evidence for the success of smoke-free policy in these settings, there continues to be resistance, variation and fragmentation in policy implementation (Lawn & Campion, 2013; Leonardi-Bee et al., 2012a, 2012b; Prochaska, 2011; Ratschen, Britton, & McNeill, 2011). Recent research has highlighted how the ‘socio-material infrastructure’ (local context of structure, culture and leadership) might influence patient safety and service quality in modern mental health care systems where smoke-free policy implementation is being attempted (Allen, 2013, p. 460). It suggests that the heterogeneity of settings might have a role in how smoke-free policy is implemented. Examining these factors in more detail can provide further insights into what needs to be done to enhance policy success.
From existing literature, it is clear that few studies have examined how implementation of smoke-free policy is influenced by type of unit, physical structure of the mental health setting or nature of the population served in such settings (Leonardi-Bee et al., 2012b, p. 91). Only one other study attempted to look comprehensively at these variables by examining the views of 123 nurse unit managers in NSW Australia in the context of specific provision of smoking cessation care in mental health units (Wye et al., 2009; Wye et al., 2010a). It found a lack of association between the type of unit (e.g. acute, non-acute, unlocked, locked) and provision of smoking care (Wye et al., 2009). Furthermore, it analysed unit managers’ views on the provision of nicotine dependence treatment comparing regional and metropolitan sites. Several associations were found to be significant, suggesting nurse manager in regional sites were, for example, more likely to support the provision of smoking cessation support to patients but less likely to believe that patients are interested in quitting than their metropolitan counterparts. However, there was no discussion of these differences according to location, why this might be so or the potential direction of the association, that is, whether unit managers in metropolitan sites were more or less likely to hold such views compared to those in regional settings (Wye et al., 2010a, p. 325). They also found that nurse unit managers who were smokers were more likely than nurse unit managers who were non-smokers to agree that increased smoking bans and interventions would have little impact on patients in their unit (Wye et al., 2010a). Another study in the United States involving 680 staff members of mental health and drug and alcohol units found that staff smoking status did not predict their views towards provision of smoking cessation assistance to patients and staff but did find that non-smokers were more likely to support the entire mental health campus being smoke-free (Steiner, Weinberger, & O’Malley, 2009; see also Dickens et al., 2004; Lawn, Feng, Tsourtos, & Campion, 2014; McNally et al., 2006).
This knowledge gap has encouraged this study to explore potential variations in staff perceptions and approaches to care that might arise due to differences in the populations served and in the different type of units in which care is delivered.
Methods
Methodology
This study employed a ‘general systems theory’ theoretical perspective because it can be used to consider the organisational context in which the smoke-free policy was introduced (Von Bertalanffy, 1950). This theory enables an in-depth examination of organisational processes in which change is being attempted in the presence of a range of groups (clinical staff, patients, policy makers, managers), all of whom might hold differing values and beliefs. The ‘realistic evaluation framework’ introduced by Pawson and Tilley is also considered, as this theoretical approach asks the relevant question: ‘What works where, for whom and in what circumstances’ (Tilley, 2000, p. 4). A realist perspective appreciates that the context surrounding settings may strongly influence how successfully a policy is implemented.
Study aim
The aim of the study was to ascertain mental health unit managers’ perceptions about the smoke-free policy introduced in England, 2 years post-implementation of a smoke-free policy within different settings (i.e. in 2010). We hypothesised that
There was an association between type of unit and the strategies applied to comply with smoke-free policy.
There was an association between unit managers’ own smoking status and their knowledge, attitudes and practices regarding smoke-free policy.
Sampling, recruitment and data collection
Drawing on an earlier Australian national survey (Lawn & Campion, 2010), two of the co-authors developed a similar survey with experts from the Department of Health, London. Parts of the survey were informed by a survey developed by Ratschen, Britton, Doody, Leonardi-Bee and McNeill (2009). Between January and May 2010, the survey was sent to 220 unit managers of a random sample of different types of mental health units across England. This was undertaken by staff at the Tobacco Control Collaborating Centre who identified potential services from available listings within each trust, followed by a letter from the head of the Department of Health to chief executives of mental health trusts asking them to encourage their unit managers to respond. At the time, there were approximately 15,200 adult public mental health beds in approximately 300 units across 58 trusts in England. Nine different adult mental health unit types were approached, reflecting diverse units and patient acuity. These included high, medium and low secure units; acute inpatient, inpatient alcohol/opiate detoxification and psychiatric intensive units; and day care and residential rehabilitation units (see Table 1). Unit managers were chosen because of their routine contact within the unit environment and their role in overseeing the practice of staff teams (and therefore thorough knowledge of those practice and any staff issues) in operationalising service policies. The sampling frame included all mental health units in England (n = 300), with surveys sent to approximately 73% (n = 220) of this total sample. Unit managers in 147 units responded (response rate = 67%). Unit managers in England’s mental health settings are mainly represented by clinical nurses, who play a vital role by taking actions and making daily decisions at the coalface of service delivery. These actions and decisions become the frontline response to smoke-free legislation (Flood, 2013, personal communication).
Type of unit, unit manager response rate, nature of patient population and level of care.

The survey included 52 structured questions comprising Likert-rated, yes/no or multiple-choice questions, complemented by site visits to help verify what was reported, the results of which are reported elsewhere (Lawn et al., 2014; Wareing & Gray, 2010, 2012; see supplementary file). Questions were asked about unit manager characteristics, staffing, unit characteristics, management of infringements, exemptions, staff and patient smoking, training, input from National Health Service (NHS) Stop Smoking Services and monitoring. In addition, the survey included five unstructured questions, allowing open responses about perceived enablers and barriers to implementation of smoke-free policy (Lawn et al., 2014). The original report neither fully analysed the qualitative data nor attempted any inferential statistical analysis of the quantitative data. This study aims to address this gap. Table 2 provides a summary of data items selected for analysis.
Data items used for analysis.
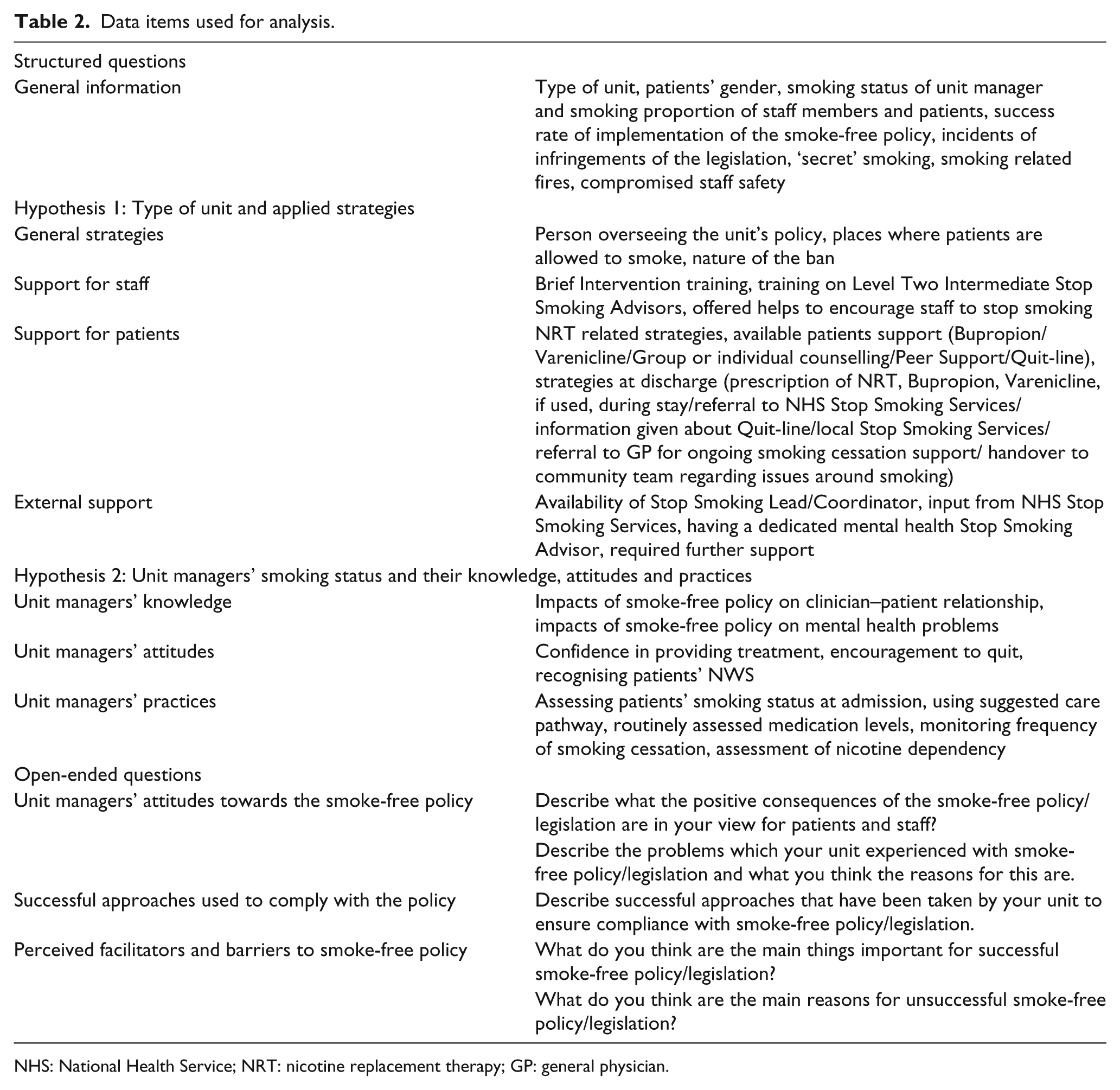
NHS: National Health Service; NRT: nicotine replacement therapy; GP: general physician.
Data analysis
Quantitative analysis occurred with 32 structured questions (excluding questions that were not specifically relevant to the aim of this study and its hypotheses), using SPSS (Version 21). This included relevant univariate, bivariate and multivariate analyses. Pearson’s chi-square test (χ2) and Phi and Cramer’s V
To explore how different unit types might be associated with particular unit managers’ perceptions of complying with the smoke-free policy, this study followed a ‘summative latent content analysis’ (Holsti, 1969) of the five open-ended questions. This process focuses on discovering underlying meanings of the words or the content beyond mere word counts (Babbie, 1992; Morse & Field, 1995). It is especially important for research using a ‘systems approach’ (Von Bertalanffy, 1950) that attempts to understand complex issues, beliefs and behaviours within complex organisations such as mental health settings (Hsieh & Shannon, 2005).
Ethical considerations
The original survey was commissioned and funded by the Department of Health, and was carried out by Tobacco Control Collaborating Centre. This secondary analysis was approved by the Flinders University ethics committee and was undertaken as part of the first author’s Master of Public Health thesis.
Results
Quantitative findings
This study analysed the responses of 131 managers across six different types of mental health unit. Data from detox units, day care and ‘other’ units were excluded as the focus was on inpatient mental health units specifically. In order to meet the assumptions of the χ2 test (Salkind, 2011, p. 287), the variable ‘type of unit’ was recoded by security level, reflecting patients’ freedom of movement in and out of the unit (potentially to smoke), and therefore level of staff supervision. These characteristics were thought to align with how staff would respond to and enact the smoke-free policy in their day-to-day work, and were confirmed as parsimonious after consultation with a clinical expert with experience in these settings (Flood, 2013, personal communication). The recoded unit types were groups as follows:
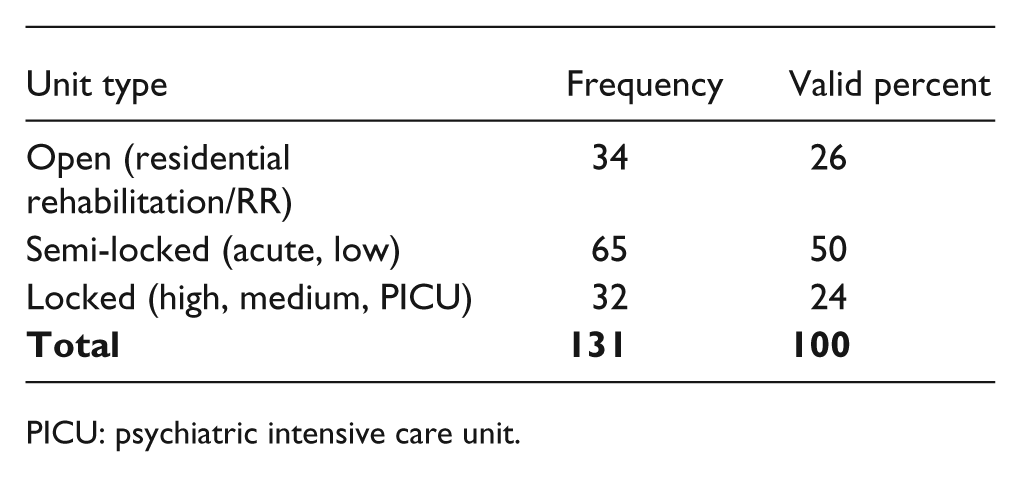
PICU: psychiatric intensive care unit.
Smoking prevalence among unit managers, staff and patients
Smoking rates among unit managers in semi-locked units (30.2%, n = 19) and locked units (26.7%, n = 8) were higher than those in residential rehabilitation units (21.2%, n = 7), though this difference was not significant. Unit managers’ perceptions of staff smoking rates, regardless of unit type, appeared to be well above that of the general population. Unit managers reported that in 56.7% of units (n = 72 of 127 units where unit managers responded to this question) 20%–49% of staff were smokers. They further reported that in 8.7% of units (n = 11/127) ⩾50% of staff were smokers. Unit managers’ perceptions of patient smoking rates were slightly higher in residential rehabilitation units, though this difference was not significant. Regardless of unit type, unit managers reported patient smoking rates of ⩾50% for approximately 75% of units. There were proportionately more residential rehabilitation units with more than 50% of staff and patients who were smokers, than other unit types (see Table 3). This might be because of the greater freedom of movement, and therefore freedom to smoke, afforded to staff and patients in residential rehabilitation units. Small sample sizes limit drawing further conclusions from the data.
Smoking status of unit manager, and their perceptions of proportion of staff members and patients who smoke by type of unit.

PICU: psychiatric intensive care units.
Hypothesis 1: association between type of unit and the strategies applied to comply with smoke-free policy
General strategies
There was a significant (χ2 = 8.455, df = 2, p = .015) but weak association (Cramer’s V = 0.259) between type of unit and whether the ban was partial or complete. Unit managers in locked units (43.3%, n = 13) were more in favour of a complete ban compared with unit managers in residential rehabilitation (15.2%, n = 5) and semi-locked units (19.0%, n = 12). The association remained significant after adjusting for unit manager’s smoking status. The result shows that non-smoker unit managers are more likely to adopt a complete ban. Managers of locked units who were non-smoker managers (40.9%, n = 9) showed better compliance than residential rehabilitation (15.4%, n = 4) and semi-locked units’ managers (15.9%, n = 7).
Support for staff smoking cessation
Regardless of type of unit, few staff smokers (0–10%) had received ‘brief intervention’ and ‘level two intermediate stop smoking advisors’ training. There was a significant but somewhat weak association between group or individual counselling on-site as a means of staff support to stop smoking when compared across different unit types (see Table 4). Furthermore open and semi-locked units had the fewest trained staff, despite these settings likely requiring this knowledge due to the varied needs of their patients, complexity of the environment and potential for their patients to maximise their attempts to quit smoking with support during their hospital stay (Table 4).
Comparison across units regarding strategies applied to support smoking cessation by staff and patients.

NHS: National Health Service; NRT: nicotine replacement therapy.
Support for patients
Proportion of units offering nicotine replacement therapy (NRT) to patients was significantly higher in locked units (53.1%) compared to semi-locked (28.6%) or residential rehabilitation (15.6%; Table 4). Proportion of units offering peer support to patients was significantly higher in locked units (53.1%) compared to semi-locked (30.6%) or residential rehabilitation (25.8%). Across all these variables, locked units offered the highest levels of support.
External support
Proportion of NHS Stop Smoking services with a dedicated mental health Stop Smoking Advisor was significantly higher in semi-locked units (41.7%) compared to locked units (33.3%) or residential rehabilitation (15.2%; Table 4).
Hypothesis 2: unit managers’ smoking status and their knowledge, attitudes and practices
Association between smoking status of unit manager and others
Unit manager smoking status was not associated with the smoking status of other staff members and patients. However, if the unit manager was a smoker, staff and patients tended to smoke more (50% and over).
Association between smoking status of unit manager and opinion about impact of smoking cessation on mental health
Unit managers who were smokers (72.7%, n = 24) were more likely than non-smokers (42.5%, n = 37) to think that ‘stopping smoking aggravated patients’ mental illness’ (χ2 = 8.73, df = 1, p = .003, Phi = 0.270). Smoker unit managers were slightly more likely to assess level of nicotine dependence of patients than non-smoking unit managers (χ2 = 6.714, df = 1, p = .010, Phi = .234). Smoker unit managers (69.7%, n = 23) were more likely to undertake the assessment at admission than non-smokers (43.3%, n = 39). In both cases, the association pertained after inclusion of type of unit, although it was specifically localised in semi-locked units.
In summary, the quantitative analyses revealed that unit managers’ smoking status appears to impact upon their knowledge, attitudes and practices towards smoke-free policy in these settings with non-smoking unit managers holding more positive views than smoking unit managers.
Qualitative findings
The survey included five open-ended questions about facilitators and barriers to smoke-free policy, according to unit type and unit managers’ smoking status. Key findings that emerged from the analysis are presented.
Positive impacts of the smoke-free policy
Feedback included how smoke-free policy had resulted in benefits of a pleasant working and living environment, reduced second-hand smoke in the units, encouraged and helped smokers to give up and resulted in greater staff capacity to provide proper care to patients by saving time that would have otherwise been spent supervising smoking:
… for security reasons smoking had to be supervised. We process mapped this-it was taking 50 hours per week of nursing time. Having to stop for smoke breaks disrupted the therapy time table … (Medium secure, former smoker)
Negative impacts of the smoke-free policy
Feedback included how smoke-free policy had damaged clinician–patient relationship (low, acute), resulted in patient agitation (medium, psychiatric intensive care unit (PICU), low, acute) and violated human rights (high, low, residential rehabilitation (RR)) were reported as major negative impacts of the smoke-free policy by unit managers:
Staff would often go and sit with a patient in an office with tea and cigarettes. Now staff observe patients smoking through a door. (Acute, current smoker) Long stay patients having extreme restrictions placed on them … not very ‘homely’ in their ‘home’. (Residential rehabilitation, former smoker)
Successful approaches used to comply with the policy
Although there were some common approaches (staff training, consistency, risk management, etc.) adopted by all units to comply with the policy, some unit managers reported additional approaches that were particularly relevant to that unit type. More specifically, the way a unit dealt with infringements and policy compliance varied according to unit type and patient population. For instance, ‘one-to-one engagement’ or individual approaches towards patients were reported as taken by many staff in semi-locked units. Unit managers from acute units also reported approaches such as ‘referral to smoking cessation nurse’ and the presence of a ‘pharmacist in ward reviews’. Furthermore, ‘patient engagement’ in decision-making and getting their consent were reported to be the prime facilitators for successful smoke-free policy in semi-locked and open units, as part of a more collaborative and inclusive approach to implementing smoke-free policy:
The unit held patient meetings and meetings with advocacy to work towards the enforcement of the smoke-free legislation. The timings of smoking were agreed within those meetings and have now been implemented successfully since the changes were made by patients. (Low secure, current smoker)
Few unit managers in high secure units mentioned applying a smoking cessation programme/care pathway to patients’ treatment. Few unit managers in low, acute and medium secure units reported using smoking cessation products to help alleviate patients’ smoking withdrawal. However, some units allowed exemptions that enabled some patients to smoke. Only two locked unit managers reported granting exemptions, and this is probably due to the nature of their patients (often detained and with higher acuity).
Perceived facilitators and barriers to smoke-free policy
When unit managers were asked about perceived facilitators of smoke-free policy, they stressed the need for ‘thorough preparation’ (prior information, clear guidelines, support system, trained staff) as an important strategy. They also reported the importance of ‘maintaining consistency’ in applying these strategies. ‘Nature of the patient’ (PICU, medium, RR), ‘collaboration’ (medium, low), ‘fear of consequences’ (medium), fair ‘weather’ to enable patients to leave the ward to smoke (all except locked units) and ‘staff support’ (low, acute) were deemed to facilitate or create barriers to policy compliance. In particular, unit managers from semi-locked units perceived more challenges than unit managers in other units:
We do not have rapid patient turnover. There is no reason for ambiguity in secured psychiatry-all areas can be smoke-free and there is no reason for staff to be exposed to smoke. (Medium secure, former smoker)
There were also differences between unit managers regarding a complete ban being more or less favourable than a partial ban in which designated areas to smoke were available to patients within hospital grounds:
Conflict between patients and staff … a complete ban would possibly help. (Low secure, former smoker) Initially it was a serious problem as smoking was banned from hospital grounds. Now that exceptions can be made and a specific area is available for smokers to use, it is far less problematic. (Acute, former smoker)
Discussion
Overall, results from this study indicate a positive stance from unit managers of England’s mental health units towards supporting smoke-free policy. However, based on their perceptions and regardless of unit type, rates of smoking by staff and patients in England’s mental health units continue to be high compared with rates of approximately 20% for the general population (McManus et al., 2010). This suggests that there is still much work to be done to address smoking for these populations to support successful implementation of smoke-free policy.
When asked about policy success rate, 93.9% (n = 123) of unit managers reported that the policy was implemented successfully (defined as any breaches addressed as part of routine care). The type of unit (as per security level and patient population) appeared to play a significant role in how smoke-free policy was implemented. This relationship has been suggested by others but has not been extensively analysed before (Lawn et al., 2014; Leonardi-Bee et al., 2012b; Schacht, Ortiz, & Lane, 2012).
The results also showed that open and semi-locked units were more likely to experience policy breaches compared to locked settings. This finding confirms previous studies which found that enforcement of smoke-free policy was ‘easier’ in locked units compared to open units (Eadie et al., 2012; Pritchard, McNeill, & Sturdy, 2008). Literature suggests that the nature of the ban, that is, whether partial (smoking permitted in designated areas in the grounds) or complete (smoking not permitted anywhere in the unit or grounds) has a substantial impact on the success of the smoke-free policy (Ballbè et al., 2013; Smith et al., 2013; Wye et al., 2009). Specifically, partial bans have been shown to create more problems and inconsistencies in enforcing the policy (Lawn & Campion, 2013, p. 4228). Ballbè et al. (2013) strongly recommend a complete ban in mental health settings to reduce the harmful effects of second-hand smoke.
The first hypothesis examined whether there were any significant differences between type of units and way strategies were applied in relation to the implementation of and compliance with the smoke-free policy. This included whether partial or complete bans were applied. Results showed that a complete ban was more likely to exist in locked units compared with semi-locked and open units; however, the association is weak. Constraints on patients’ movement and closer monitoring of patients’ behaviour within locked units were likely to have given staff more control over tobacco supply, making locked units conducive environments to implement a complete ban and consequently help to better comply with the legislation (Harris et al., 2007; Wye et al., 2009).
Univariate data analysis also found that locked settings were significantly more likely to provide NRT to patients. Possible reasons for this include that staff in locked units might have been more in favour of using cessation supports than staff in other unit types because of their greater capacity to closely monitor patients, and greater familiarity with managing highly distressed patients, as part of their usual role. On the other hand, in semi-locked and open units where patients can move about and be more autonomous during their stay, staff might rely more on general counselling and external smoking cessation support providers to assist patients to comply with the policy, and be less diligent in offering NRT or see cessation support as their clinical role (Lawn & Campion, 2010, 2013). Overall, using ‘realist evaluation’ principles (Tilley, 2000), it is evident that the nature of the work and type of patients in each setting lead staff to use needs-based and tailored strategies to inform how they implement smoke-free policy, rather than trying to apply the same strategies for all settings.
Although NRT is recommended and is widely viewed as an effective strategy to support patients with smoking cessation (Hehir, Indig, Prosser, & Archer, 2013; Parker, McNeill, & Ratschen, 2012; Royal College of Physicians, Royal College of Psychiatrists, 2013), locked settings were significantly more likely to provide NRT to patients. However, few unit managers in high secure units mentioned applying a smoking cessation programme/care pathway to patients’ treatment. It could be that they are more focused on the here-and-now of patient care needs, which do not include considering support for patients’ long-term smoking cessation once discharged. Few unit managers in low, acute and medium secure units reported using smoking cessation products to help alleviate patients’ smoking withdrawal. This might be because patients in these units were more mobile and could access designated smoking areas which reinforced their ability to continue smoking and not consider ceasing while they were in hospital.
The second hypothesis tested the association between unit managers’ knowledge, attitude and practices and their own smoking status. Staff smoking status has been indicated as a crucial factor in implementing smoke-free policy by a number of studies (Hehir et al., 2013; McNally et al., 2006). Our study found that there was no association between smoking status of the unit manager and other staff members; although unit managers who were smokers were more likely to think smoking cessation aggravated patient’s mental illness which is an important finding and reflected in other studies (Dickens et al., 2004; McNally et al., 2006; Steiner et al., 2009; Wye et al., 2010a). However, in one practice towards patients (assessment of level of nicotine dependence), smoking unit managers showed slightly better practice than the non-smokers. This finding suggests that smoking unit managers were more likely to identify with patients’ smoking behaviours and distress from nicotine withdrawal, and therefore more likely to see it as relevant to flag in relation to clinical assessment. It reflects the embedded complexity of care in mental health units and the characteristics of their staff, which demands further attention.
Overall, more staff education and training is required, to increase staff knowledge and awareness, especially among smoking staff, and among unit managers who are largely responsible leading staff in enforcing the unit’s policy (Ratschen et al., 2009). Staff training to support patients’ smoking cessation is another strategy that has been widely advocated (Lawn & Campion, 2010; Prochaska, 2011; Ratschen et al., 2011; Wye et al., 2010a, 2010b). This study found that, regardless of unit type, such training remained minimal in these settings. Previous research shows that having supportive smoking cessation advisors is an important facilitator to successful quitting in mental health settings (Leonardi-Bee et al., 2012b, p. 11; NICE, 2013).
Quantitative results have shown that, for this sample, applied strategies significantly vary by type of unit (H1: association between type of unit and applied strategies), whereas unit managers’ knowledge, attitude and practices vary by their smoking status (H2: association between unit managers’ own smoking status and their knowledge, attitudes, practices). Therefore, both of these alternate hypotheses are accepted.
Results from the qualitative data help to explain how unit type influenced the way smoke-free policy was implemented in English mental health settings. It revealed underlying complexities of mental health institutions and numerous interlinking factors (mainly type of unit, and unit managers’ smoking status) that have shaped unit managers’ knowledge, attitudes and practices to comply with the policy.
Unit managers from semi-locked units perceived more challenges than unit managers in other units. This might be because semi-locked units are highly complex environments with a less consistent approach to care because patients are more heterogeneous (i.e. housing patients with acuity needs across a broader spectrum, and greater diversity of movement in and out of the unit) than patients in other unit types (Flood, 2013, personal communication).
Study limitations
This research contains several methodological and contextual strengths. The original study has limitations, which subsequently hamper this secondary analysis. For instance, it lacks information on unit managers’ demographic characteristics (age, sex, etc.) and their clinical qualifications, which might have influenced how they enacted the policy. Less than half of all services were surveyed. The audit only sought the views of one unit manager individual from each setting, not other parties impacted by the policy, such as patients, patients’ family, other nurses, psychiatrists and allied health staff, policy makers and administrators. This study relied on a self-reported questionnaire that is susceptible to respondent bias and inaccurate reporting of the smoking status of other staff and patients. Furthermore, some participants might have given more favourable reports than was actually the case, as a consequence of their clinical leadership role. In addition, their perspectives are subjective. These limitations were minimised by drawing ideas from a large sample and by allowing anonymous return of surveys.
Overall, a somewhat small sample size (131 cases) might have limited statistical power. The distribution according to unit type is not symmetrical, which might have influenced the quantitative results (50% of the total cases were from semi-locked units). Qualitative data from open-ended questions were often reported as brief, abridged comments only by respondents, and may have lacked an in-depth understanding of the research problem, or its meaning might have been misinterpreted by the researchers. Finally, since the original survey occurred in 2010, there has been further embedding of smoke-free policy in mental health settings and the wider community. Therefore, views and practices might have changed; however, the finding may well still be of value in England’s units which continue to struggle to implement smoke-free policy fully, or other countries where smoke-free policies are yet to be implemented.
Conclusion
This is the first study to comprehensively compare different inpatient mental health unit types, and to consider a large and diverse range of possible aspects that might influence the ways smoke-free policy is implemented in these settings across England. These aspects included structural and service delivery cultural and clinical practices of the unit, the nature of patients and staff smoking status. The results have shown that all these factors are important determinants of successful smoke-free policy and can vary from unit to unit. This finding might assist policy makers, hospital administrators and staff in implementing strategies tailored to the specific needs of the populations within their settings (both staff and patients), rather than assuming a one-size fits all approach.
Footnotes
Acknowledgements
The authors would like to thank Professor John Wiggers, Dr Samantha Meyer and Mr. Chris Flood for their valuable feedback on this research. We thank staff from the Tobacco Control Collaborating Centre for assisting with data collection and unit managers who participated in the study. We also acknowledge that parts of the original survey were informed by a survey developed by Dr Elena Ratschen from the University of Nottingham.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This original research on which this secondary analysis was based was made possible from a Department of Health grant to the Tobacco Control Collaborating Centre and Chartered Institute of Environment Health, UK.