
Abstract
Background:
Intimate partner violence (IPV) is a significant public health threat that contributes to a wide range of mental and physical health problems for victims.
Aims:
The purpose of this study was to examine IPV-related experiences and mental health outcomes among college students in Japan, Singapore, South Korea and Taiwan.
Methods:
The data were obtained from the Inter-University Consortium for Political and Social Research (ICPSR), the International Dating Violence Study (IDVS) 2001–2006 (ICPSR 29583; N = 981; Japan n = 207; Singapore n = 260; South Korea n = 256; Taiwan n = 258).
Results:
Co-experience of physical IPV victimization and perpetration was associated with borderline personality traits and posttraumatic stress disorder (PTSD), but not with depression. Childhood sexual abuse, gender hostility and violence socialization were significant predictors of borderline personality traits, depression and PTSD. While country and gender variations in mental health are noted, there are two specific populations that may need special attention for mental health interventions: Taiwanese women especially for borderline personality traits and PTSD, and Japanese men especially for depression.
Conclusion:
IPV victimization and perpetration, childhood sexual abuse, gender hostility and violence socialization have a significant impact on the mental health of college students in Japan, Singapore, South Korea and Taiwan. Since IPV and mental health are significant public health issues, research on IPV and mental health consequences of IPV victimization and perpetration in these countries should be further expanded in order to better understand the interventions that will be effective in treating victims, perpetrators and victim/perpetrators of IPV.
Keywords
Introduction
Intimate partner violence (IPV) is a significant public health threat that contributes to a wide range of mental and physical health problems for victims (Ellsberg, Jansen, Heise, Watts, & Garcia-Moreno, 2008). IPV includes physical, sexual and/or psychological harm inflicted by a current or former intimate partner, such as a dating partner, fiancée or spouse (Center for Disease Control and Prevention, 2015), and these types of behaviors are used to gain power and control over a partner (United States Department of Justice, 2015). Worldwide, the lifetime prevalence of physical IPV among female victims varies from 15% to 71% (Garcia-Moreno, Jansen, Ellsberg, Heise, & Watts, 2006).
This study focused on IPV and mental health among four Asian countries, Japan, Singapore, South Korea and Taiwan, which were examined in the International Dating Violence Study (IDVS) and have a comparable sample size. The IDVS examined IPV among college students in 32 countries. The World Health Organization (WHO) multi-country study found that the lifetime prevalence of female IPV victimization in Japan is 12.9% Garcia-Moreno, Jansen, Ellsberg, Heise, & Watts, 2006). Other studies have found that the lifetime prevalence of female IPV victimization in Singapore is 18% (Chan, Straus, Brownridge, Tiwari, & Leung, 2008), in South Korea is 28% (Chan et al., 2008) and in Taiwan is 19% (Shen, 2009). One study in South Korea found that women are more likely to report verbal IPV perpetration and victimization (28.2% victimization, 26.7% perpetration) than men (24.4% victimization, 25.3% perpetration), while men are more likely to report physical IPV perpetration (5.1%) than women (3.4%) (Lee, Stefani, & Park, 2014).
In Japan, IPV victimization of women is associated with tobacco use and alcohol abuse (Yoshihama, Horrocks, & Bybee, 2010). In South Korea, female IPV victimization is associated with depression which has been found to increase the risk of further incidences of IPV (Kim & Lee, 2013). As in other studies, being a victim of child abuse is a predictor of being a victim of IPV in South Korea (Gover, Park, Tomsich, & Jennings, 2011; Jennings et al., 2014). In Taiwan, a survey of college students found that 19% of the participants had experienced IPV victimization and 11% of the participants had experienced both IPV victimization and child abuse (Shen, 2009). Experiencing both IPV and child abuse was associated with trauma symptoms and behavioral problems in young adulthood (Shen, 2009). There are very few studies on IPV in Singapore. One study which surveyed female victims of IPV found that the percentage of female victims who sought help for IPV increased between 1992 (20.6%) and 2002 (50.9%) (Foo & Seow, 2005). This could indicate an increased awareness of IPV-related services in this country.
Borderline personality traits, posttraumatic stress disorder (PTSD) and depression are common adverse mental health consequences of IPV victimization and/or perpetration. Borderline personality traits are associated with IPV but vary differently for men and women. Borderline personality traits are related to both perpetration and victimization among men while only related to victimization among women (Maneta, Cohen, Schulz, & Waldinger, 2013). Borderline personality traits increase the risk of developing PTSD among female victims of IPV (Kuijpers, van der Knaap, Winkel, Pemberton, & Baldry, 2011). Wolford-Clevenger et al. (2015) found an association between being a male perpetrator of IPV and having a diagnosis of depression and borderline personality disorder. PTSD is a consequence and risk factor of IPV victimization and perpetration (Kuijpers, van der Knaap, & Winkel, 2012). It has been shown that treating PTSD and depressive symptoms can reduce recurrent IPV among female victims (Iverson et al., 2011). Treating borderline personality traits may also have an impact on IPV victims.
In addition to IPV, the following individual experiences are often considered factors that mediate the association between IPV and mental health and include substance abuse (Connelly, Hazen, Baker-Ericzen, Landsverk, & Horwitz, 2013; Evans & Shapiro, 2011; Hellmuth, Gordon, Moore, & Stuart, 2014; Illangasekare, Burke, Chander, & Gielen, 2013), history of childhood sexual abuse (Devries et al., 2011; Ouellet-Morin et al., 2015), childhood neglect (Nikulina, Widom, & Czaja, 2011), gender hostility (Filson, Ulloa, Runfola, & Hokoda, 2010) and violence socialization (Jeyaseelan et al., 2004). Yet, the association between IPV-related experiences and mental health has not been fully examined in many areas of the world, including Asia.
While previous studies have examined IPV-related experiences and mental health in Japan, South Korea and Taiwan (but not in Singapore to the best of our knowledge), the comprehensive information about IPV-related experiences and mental health is still lacking in these countries. Thus, the purpose of this study was to examine IPV-related experiences and mental health outcomes among college students in Japan, Singapore, South Korea and Taiwan. This study contributes to the increased knowledge about mental health issues related to IPV and other violence-related experiences among college students that will aid the development of intervention programs for IPV, borderline personality disorder, depression and PTSD.
Methods
Data
The data were obtained from the Inter-University Consortium for Political and Social Research (ICPSR), the IDVS 2001–2006 (ICPSR 29583). The data were collected from college students at 68 universities in 32 countries by the members of an IDVS research consortium. The detailed information of the entire study, including data collection procedures, is available at http://pubpages.unh.edu/~mas2/. This study analyzed the data from the IDVS data set. In addition, the US data were included to provide a comparison between the four countries. The original collector of the data, ICPSR, and the relevant funding agency bear no responsibility for the use of the data or for interpretations or inferences based upon such uses.
Samples
Japan sample
The Japan sample includes 207 participants from one university (men, n = 99; women, n = 108). More than 60% of the participants (men, n = 62, 62.6%; women, n = 71, 65.7%) had ever had an intimate partner. There were four different types of relationships: dating (n = 108, 81.2%), engaged (n = 15, 11.3%), married (n = 4, 3.0%) and cohabitating (n = 6, 4.5%) (percentages are based on the participants who had ever partnered). Two of the participants (both women) reported that they had a same sex partner. The mean age of the participants was 20.3 years (standard deviation (SD) = 1.1 years).
Singapore sample
The Singapore sample includes 260 participants from one university (men, n = 83; women, n = 177). More than 80% of the participants (men, n = 67, 80.7%; women, n = 149, 84.2%) had ever had an intimate partner. There were four different types of relationships: dating (n = 162, 75.0%), engaged (n = 16, 7.4%), married (n = 34, 15.7%) and cohabitating (n = 4, 1.9%) (percentages are based on the participants who had ever partnered). Six of the participants (three men and three women) had a same sex partner. The mean age of the participants was 24.7 years (SD = 3.7 years).
South Korea sample
The South Korea sample includes 256 participants from one university (men, n = 93; women, n = 163). More than 80% of the male participants (n = 77, 82.8%) and 70% of female participants (n = 113, 69.3%) had ever had an intimate partner. There were four different types of relationships: dating (n = 174, 91.6%), engaged (n = 5, 2.6%), married (n = 10, 5.3%) and cohabitating (n = 1, 0.5%) (percentages are based on the participants who had ever partnered). One of the male participants had a same sex partner. The mean age of the participants was 24.3 years (SD = 3.8 years).
Taiwan sample
The Taiwan sample includes 258 participants from one university (men, n = 73; women, n = 185). More than 50% of the male participants (n = 39, 53.4%) and 60% of female participants (n = 123, 66.5%) had ever had an intimate partner. There were four different types of relationships: dating (n = 152, 93.8%), engaged (n = 0), married (n = 1, 0.6%) and cohabitating (n = 9, 5.6%) (percentages are based on the participants who had ever partnered). Eleven of the participants (two men and nine women) had a same sex partner. The mean age of the participants was 20.1 years (SD = 1.8 years).
Measures
All measures used in the IDVS have been tested for validity and reliability and have been used widely in many countries (Straus, 2004; Straus, Hamby, Boney-McCoy, & Sugarman, 1999). IPV was measured using the revised Conflict Tactics Scale (CTS2) (Straus, Hamby, Boney-McCoy, & Sugarman, 1996). The CTS has been used widely not only in the United States but also in many other countries (Straus, 2008). The CTS measures both perpetration and victimization of IPV. Physical IPV (physical assault) items included incidents such as kicked, pushed or shoved, or used a knife or gun by a partner or self. In this study, the lifetime (ever) prevalence of victimization and perpetration of physical IPV was used for analysis.
Borderline personality was measured in two aspects, instability and self-harm, using nine items. The example to measure instability (five items in total) is ‘I change suddenly from being one kind of person to another’. The example to measure self-harm (four items in total) includes ‘I have had thoughts of cutting or burning myself’. Symptoms of depression, individual characteristics and experience, and couple relationship items were asked using a 4-point Likert scale (1 = strongly disagree, 4 = strongly agree). Some of the items are reversely coded. This study used the scoring method based on the theoretical maximum score, which was scaled from 0 to 100. There were eight items to measure depression (e.g. ‘I have thought about killing myself’ and ‘I feel sad quite often’). PTSD was measured using eight items (four items related to avoidance/arousal and four items related to re-experiencing). The examples of the PTSD items include ‘I’ve been terrified by things that have happened to me’ (avoidance/arousal) and ‘I have bad dreams about terrible things that happened to me’ (re-experiencing).
Statements measuring substance abuse included alcohol use (four items, for example, ‘I sometimes drink enough to feel really high or drunk’ and other drug use (four items, for example, ‘I worry that I have a drug problem’). Childhood sexual abuse history included sexual abuse by an adult family or non-family member or a child family or non-family member. The IDVS did not include other forms of childhood abuse or neglect such as physical and emotional abuse or witnessing IPV. Statements measuring childhood sexual abuse included the following: (1) ‘An adult or child family or non-family made me look at or touch their private parts (sex organs), or looked at or touched mine’; and (2) ‘An adult or child family or non-family had sex with me (vaginal, anal or oral)’. The violence approval measure has three subtopics: (1) family violence (four items, for example, ‘It is sometimes necessary to discipline a child with a good, hard spanking’), (2) male violence (three items, for example, ‘A man should not walk away from a physical fight with another man’) and (3) sexual aggression (three items, for example, ‘A woman who has been raped probably asked for it’). History of childhood neglect was measured by eight items in four areas: cognitive needs, supervisory needs, emotional needs and physical needs. The examples of the items include ‘My parents did not help me to do my best in school’ (cognitive needs), ‘My parents did not care if I got into trouble in school’ (supervisory needs), ‘My parents did not comfort me when I was upset’ (emotional needs) and ‘My parents did not keep me clean’ (physical needs). Gender hostility combined hostility to men (five items) and hostility to women (five items). The examples of the items include ‘Men/women are rude’ and ‘Men/women irritate me a lot’. The violence socialization scale included two parts: violence socialization with family (five items, for example, ‘When I was a kid, I saw my mother or father kick, punch or beat up their partner’ and ‘My father or mother told me to hit back if someone hit me or insulted me’) and violence socialization by non-family (three items, for example, ‘When I was a kid, I often saw kids who were not in my family get into fights and hit each other’ and ‘When I was a kid, people (adults or kids) who were not part of my family pushed, shoved or slapped me or threw things at me’).
Statistical analysis
Data were analyzed using SPSS (version 22). Descriptive statistics were used to describe the distribution of the outcome and independent variables. Comparisons were conducted using Pearson’s Chi-square tests for categorical variables (if each cell had more than five respondents) and analysis of variance (ANOVA) tests for continuous variables. Multivariate regression analysis (General Linear Model) was conducted to test the association between mental health (borderline personality traits, depression and PTSD), IPV-related experiences (substance abuse, childhood sexual abuse, neglect, gender hostility and violence socialization) and demographic characteristics (age and gender). In addition, reference variables of a country (reference = Taiwan) were included to control country differences. Regression coefficients (standard errors) were used to obtain 95% confidence intervals (CIs).
Results
Table 1 describes the lifetime prevalence of victimization and perpetration of physical IPV by country and gender. Overall, approximately one-fourth of the ever-partnered participants (n = 188, 26.8%) had been both a victim and perpetrator of physical IPV with a range of 6.9% (Singaporean men) to 37.1% (Japanese men). The overall prevalence of being a victim but not a perpetrator was very low (n = 16, 2.3%), with a range of 0% (Japanese men and women and Taiwanese men) to 7.5% (Singaporean men). The overall prevalence of being a perpetrator but not a victim was 9% (n = 63), with a range of 2.6% (Taiwanese men) to 16.3% (Taiwanese women).
Lifetime prevalence of victimization and perpetration of physical IPV.
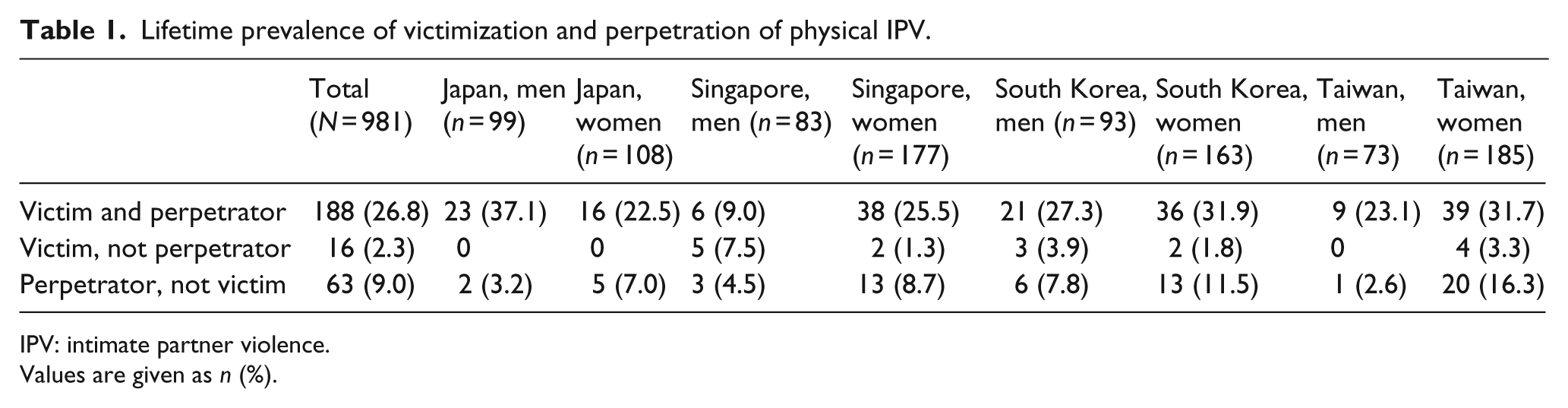
IPV: intimate partner violence.
Values are given as n (%).
Table 2 summarizes and compares mental health and violence-related experience by gender and country. The results of ANOVA tests were significant for all items. Taiwanese women had the highest scores for borderline personality, PTSD and gender hostility. Japanese men had the highest score for depression. South Korean men had the highest score for substance abuse and South Korean women had the highest score for childhood neglect. Taiwanese men had the highest score for childhood sexual abuse and violence socialization.
Descriptive statistics of mental health and violence-related experience.
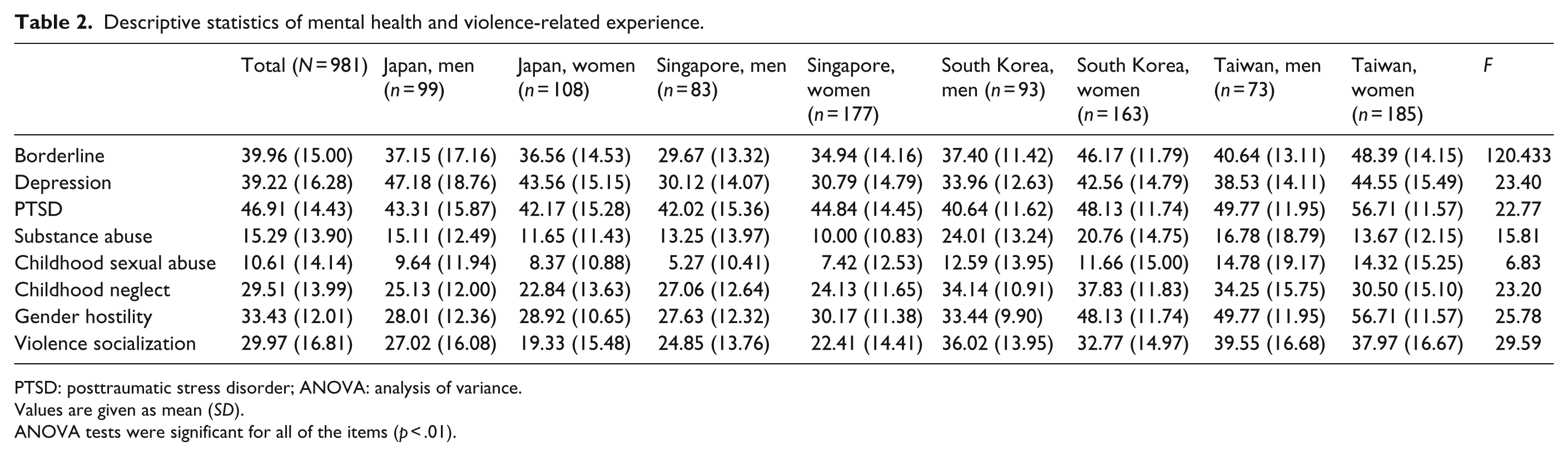
PTSD: posttraumatic stress disorder; ANOVA: analysis of variance.
Values are given as mean (SD).
ANOVA tests were significant for all of the items (p < .01).
Table 3 presents predictors of mental health outcomes. Physical violence victimization and perpetration were significantly related to higher scores of borderline personality and PTSD, but not to depression. Childhood sexual abuse, gender hostility and violence socialization were significantly associated with higher scores of borderline personality, depression and PTSD. Childhood neglect was significantly related to borderline personality, but not to depression and PTSD. Younger age and female gender were significantly associated with borderline personality and PTSD. Compared to Taiwanese participants, Japanese participants reported lower levels of PTSD, but higher levels of depression. Singaporean participants reported lower levels of borderline personality than Taiwanese participants. South Korean participants reported lower levels of depression and PTSD than Taiwanese participants.
Predictors of mental health (N = 981).
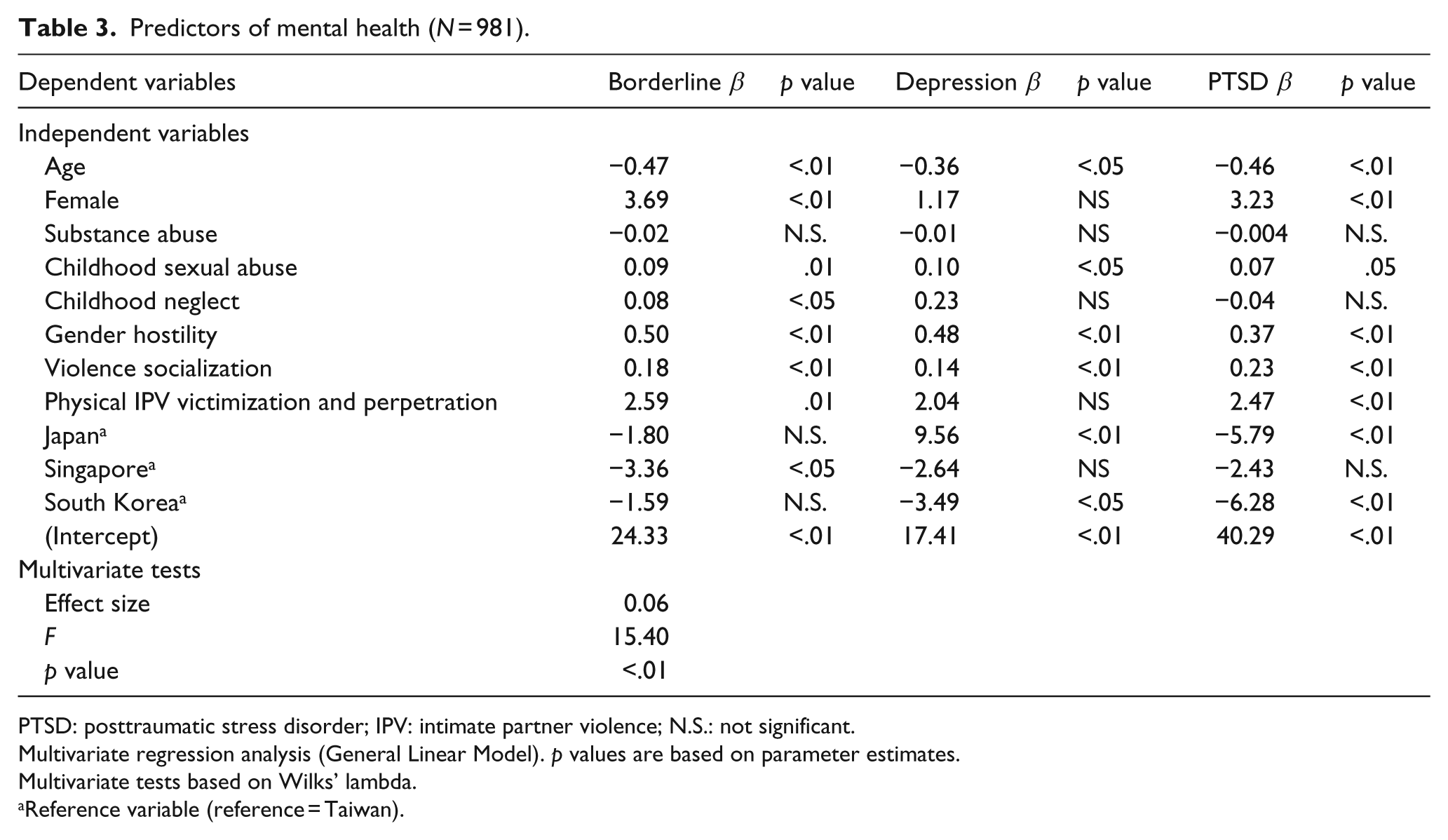
PTSD: posttraumatic stress disorder; IPV: intimate partner violence; N.S.: not significant.
Multivariate regression analysis (General Linear Model). p values are based on parameter estimates.
Multivariate tests based on Wilks’ lambda.
Reference variable (reference = Taiwan).
Discussion
This study examined IPV-related experiences and mental health among college students in Japan, Singapore, South Korea and Taiwan. There are three main findings. First, co-experience of physical IPV victimization and perpetration was associated with borderline personality traits and PTSD, but not with depression. Second, childhood sexual abuse, gender hostility and violence socialization were significant predictors of borderline personality traits, depression and PTSD. Third, while country and gender variations in mental health are noted, there are two specific populations that may need special attention for mental health interventions: Taiwanese women especially for borderline personality traits and PTSD and Japanese men especially for depression.
The results of this study suggest that the co-occurrence of IPV victimization and perpetration is related to higher levels of borderline personality traits and PTSD. Overall, the levels of borderline personality traits and PTSD among the study participants (range: 29.67–48.39 for borderline personality traits; range: 40.64–56.71 for PTSD) are higher than percentile norms (25 at the 91th percentile for borderline personality traits and the 93rd percentile for PTSD) (Straus, 2010). A previous study found that perpetration of IPV among men and women is associated with borderline personality traits (Ross, 2011). This study added new knowledge that the co-occurrence of IPV victimization and perpetration, not just IPV perpetration, can be a risk factor for borderline personality traits. Likewise, while previous studies found associations between PTSD and female victims of IPV (Carleton, Mulvogue, & Duranceau, 2015; Hebenstreit, Maguen, Koo, & DePrince, 2015), the results of this study found an association between PTSD and the co-occurrence of IPV victimization and perpetration. Also, previous studies show that female victims of IPV (e.g. Beydoun, Beydoun, Kaufman, Lo, & Zonderman, 2012; Ouellet-Morin et al., 2015) who display aggression toward males (Vaeth, Ramisetty-Mikler, & Caetano, 2010) tend to report depressive symptoms. The co-occurrence of IPV victimization and perpetration was not associated with depression in this study. The results suggest that people who are both victims and perpetrators of physical IPV suffer more from borderline personality traits and PTSD than depression.
The finding that childhood sexual abuse is related to PTSD is consistent with previous studies (e.g. Brown, Burnette, & Cerulli, 2015). Childhood sexual abuse and gender hostility seem to be important predictors of borderline personality traits, depression and PTSD. Previous studies focusing on male-to-female hostility and mental health among women found that women who feel powerless are more likely to be victims of IPV and suffer from depression (Filson et al., 2010). The perception of male superiority is related to IPV in Japan (Nagae & Dancy, 2010). The results of this study indicate that gender hostility can affect mental health of both men and women. Furthermore, violence socialization and a history of childhood sexual abuse have a significantly negative impact on the mental health of college students in these Asian countries.
There were country and gender differences in IPV victimization and perpetration, mental health and other violence-related experiences. However, Taiwanese women and Japanese men may need special interventions. Taiwanese women reported the highest levels of PTSD compared to other country/gender groups, and they reported the highest level of gender hostility (which may affect PTSD). In addition to gender hostility, Taiwanese women may have other traumatic experiences. A study on college students in Taiwan found that one-third of college students had experienced a natural or manmade disaster and/or had seen someone being beaten or killed (Shen, 2009). The high levels of PTSD among Taiwanese women might be from traumatic experiences not necessarily related to IPV. Future research is necessary to identify risk factors for PTSD among Taiwanese women.
Japanese men reported the highest levels of depression and the highest prevalence of the co-occurrence of victimization and perpetration of physical IPV. In general, the lifetime prevalence of depression in Japan (3%–7%) is lower than that in Western countries (3%–16%) (Japan Ministry of Health, Labor and Welfare, 2015). Most of the depression research in Japan has focused on the impact of natural disasters (Nishigori et al., 2015; Sakuma et al., 2015), the elderly (Imai et al., 2015; Takagi et al., 2013) and caregivers of the elderly (Arai, Kumamoto, Mizuno, & Washio, 2014; Oura et al., 2012). The research on depression and IPV experiences among male college students in Japan is lacking. Future research should further examine Japanese male college students’ depression related to IPV victimization and perpetration.
It is important to note that the prevalence of IPV perpetration, that is, ‘perpetrator, not victim’, was higher among women than men in these countries. The literature on the issue of IPV perpetration and victimization presents conflicting results. Worldwide, there is an assumption that perpetrators of IPV are men and victims of IPV are women (Rothman, Butchart, & Cerdá, 2003). However, some studies show that the prevalence of IPV perpetration among women is the same as or even higher than that among men (e.g. Williams, Ghandour, & Kub, 2008). Taiwanese women who reported a higher prevalence of ‘perpetrator, not victim’ also reported higher levels of borderline personality traits, PTSD and gender hostility compared to all other sample groups including both women and men. These traits may be related to female perpetration, particularly in Taiwan. Conversely, Singaporean men, who reported the lowest prevalence of ‘perpetrator and victims’ and ‘perpetrator, not victim’ reported the lowest levels of borderline personality traits and depression. Studies on female IPV perpetration are notably lacking (Carney, Buttell, & Dutton, 2007). Therefore, future studies should further examine the causes and context of female IPV perpetration.
Limitations
This study used a cross-sectional design and is limited to analyze causal relationships among the variables. The data were based on self-reports. The samples were convenience samples from one university in each country and do not necessarily represent all college students in these countries. In addition, the sample size in each country was relatively small. The data do not include the time of onset of the mental health measures and therefore do not specify whether the mental health issues predate or follow IPV. The diagnoses were not verified by clinical assessment. The CTS does not explain the context of IPV and other experiences. For example, the data do not specify what happened first, victimization or perpetration. While analyzing for associations (risk factors and mental health outcomes) for IPV victims and perpetrators combined may be problematic because this category included only a quarter of the sample, the number of participants in the category of ‘victim, not perpetrator’ (n = 16, 2.3%) or ‘perpetrator, not victim’ (n = 63, 9%) was very small and was not sufficient to conduct a separate analysis.
Strengths
Despite the limitations, this study has a number of strengths and contributes to existing literature on mental health and IPV-related experiences in Asia since there is a paucity of this type of research in Asia. In addition, most previous studies on IPV in Asia and other regions mostly focused on female victims abused by male intimate partners and do not include the co-occurrence of victimization and perpetration. The results of this study suggest the importance of considering the co-occurrence of male and female victimization and perpetration and its association with mental health. These data have important implications for future research.
Conclusion
IPV victimization and perpetration, childhood sexual abuse, gender hostility and violence socialization have a significant impact on the mental health of college students in Japan, Singapore, South Korea and Taiwan. Since IPV and mental health are significant public health issues, research on IPV and the mental health consequences of IPV victimization and perpetration in these countries should be further expanded in order to better understand the interventions that will be effective in treating victims, perpetrators and victim/perpetrators of IPV. The inclusion of the co-occurrence of IPV victimization and perpetration for both genders is important for future research. At the same time, the results of this study indicate that there are evident country and gender variations in IPV-related experiences and mental health. Country- and/or gender-specific factors need to be considered when developing effective intervention programs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.