
Abstract
Background:
Several guidelines consider psychosocial treatments an essential component of clinical management of bipolar disorders in addition to drug therapy. However, to what extent such interventions are available in everyday practice to the average patient attending mental health services is not known.
Aims:
This study aims to investigate access of people with bipolar disorders to psychosocial treatments in a community-based care system.
Method:
Information on care delivery and service utilization were retrieved from the psychiatric database of Lombardy, Italy, covering a population of 9,743,000, for all adults who had at least one contact in 2009 with psychiatric services. Rates of patients with a diagnosis of bipolar disorder who had access to individual psychotherapy, couple/family therapy, group psychotherapy and family interventions were calculated and compared to patients with schizophrenia and depression.
Results:
A total of 8,899 subjects with bipolar disorder had been in contact with psychiatric services, corresponding to a treated annual prevalence rate of 1.1‰. More than 80% of patients were treated in community settings. Rates of patients receiving structured psychosocial treatments ranged from 0.7% for couple/family therapy to 6.1% for individual psychotherapy. No differences with patients with schizophrenia and depression were found. Patients with schizophrenia received more interventions labeled as rehabilitation.
Conclusion:
Few people with bipolar disorders had access to psychosocial treatments. Even in a well-developed system of community care, offer of psychosocial interventions for bipolar disorders is inadequate. This issue should be a target for future research on dissemination and implementation strategies.
Introduction
Bipolar disorder represents a significant public health challenge, because of its 1-year prevalence around 1% of the population, lifetime prevalence up to 4% and long-term course often associated with functional impairment and incomplete symptomatic recovery (Ferrari, Baxter, & Whiteford, 2011; Merikangas et al., 2011; Salvatore et al., 2007).
Recent guidelines consider psychosocial treatments an essential component of clinical management of bipolar disorders in addition to drug therapy (Goodwin & Consensus Group of the British Association for Psychopharmacology, 2009; Yatham et al., 2013). A treatment update identified the following evidence-based treatments: cognitive-behavioral therapy, family-focused therapy, interpersonal and social rhythm therapy and group psychoeducation (Geddes & Miklowitz, 2013). A review focusing on psychosocial interventions (Reinares, Sánchez-Moreno, & Fountoulakis, 2014) concluded that benefits are proven for psychoeducation, cognitive-behavioral therapy, family therapy, interpersonal and social rhythm therapy, group psychoeducation, with a positive impact on prevention of recurrences, reduction of symptoms, functional improvement, burden and wellbeing of patients and relatives. Preliminary data are promising for cognitive remediation and mindfulness-based psychotherapies. In addition to evidence from clinical research, it is worth noting that surveys of patient preference reveal a strong wish by people with bipolar disorders for both self-help and psychological therapies (Pontin, Peters, Lobban, Rogers, & Morriss, 2009). Patients, relatives and advocacy organizations claim a need for education, information and awareness programs for affected people, their carers, clinicians and lay public, in order to offer the best available treatments, while reducing current levels of stigmatization and facilitating reintegration in the community (Elgie & Morselli, 2007; Powell, Silk, & Albeck, 2000).
Almost all trials of psychosocial interventions, however, have been realized in specialized centers with highly selected groups of patients. To what extent such interventions can be transferred to everyday practice for the average patient attending mental health services is not known. Unfortunately, our current knowledge about how to actually implement guidelines in clinical practice is still weak, so the uptake of evidence-based treatments at the implementation level, despite promising research findings and proliferation of guidelines, has lagged behind.
Some recent trials tried to address this problem, by training clinicians from different service settings and examining the feasibility of structured psychosocial interventions in mainstream services (Castle et al., 2010; Fiorillo et al., 2014; Lobban et al., 2010). Preliminary results look promising and underscore the need for large scale pragmatic trials in naturalistic settings.
Given the good evidence base and the strength of recommendations, it is important to know to what extent psychosocial interventions are available for people with bipolar disorders in real-world clinical practice. In general, implementation of evidence-based care for severe mental disorders is unsatisfactory and guidelines are not routinely followed by clinicians (Bauer, 2002). Surveys of guideline concordance rates in bipolar disorders show mixed results, ranging from 20% to 80% (Paterniti & Bisserbe, 2013). Most of these studies were not conducted on community samples, but on small selected samples, unlikely to reflect current practice, and only considered concordance with guidelines related to drug treatment. Data on implementation of psychosocial treatments are scant, although preliminary evidence from other areas of psychiatric care shows poor results (Gearing, Townsend, Elkins, El-Bassel, & Osterberg, 2014).
An Italian study assessed the adequacy of treatment for bipolar disorders using data from the Lombardy Region Psychiatric Information System (Lora, Conti, Leoni, & Rivolta, 2011). In 2007, 56% of people with a diagnosis of bipolar disorder received minimally adequate treatment. However, adequacy was defined as receiving at least 2 months’ supply of antipsychotics and/or mood stabilizers plus at least four visits by a psychiatrist, excluding any assessment of psychosocial interventions.
We decided to use more recent data from the same database to focus on psychosocial treatments. The aim was to answer the following questions: Do patients with a diagnosis of bipolar disorder treated by mental health services in a well-developed system of community care have access to psychosocial interventions? How do they compare with patients with schizophrenia and unipolar depression? Do the interventions received reflect evidence-based indications?
Method
Setting
Lombardy is the largest and most affluent region of Italy, with a total population of 9,743,000 in 2009, including the metropolitan area of Milan, Italy’s second largest city.
The mental health system of Lombardy has been described elsewhere (Lora, Barbato, Cerati, Erlicher & Percudani, 2012). The Departments of Mental Health (DMHs) are the public agencies providing care to the population of the respective catchment areas through a range of community services including outpatient clinics, outreach teams, hospital, day care and residential facilities. The organizational model of DMHs is centered on multi-disciplinary teams including psychiatrists, psychologists, nurses, social workers, rehabilitation counselors and other professionals.
Each DMH should provide its population with the full range of psychiatric care, from acute emergency treatment to long-term rehabilitation.
In 2009, the network of psychiatric services in Lombardy comprised 64 DMHs, with a total of 98 Community Mental Health Centers, 105 Day Care Centers with 2 places/10,000 adult population, 54 General Hospital Inpatient Units with 1 bed/10,000 and 273 Community Residential Facilities with 4 places/10,000. Private Day Care and Residential Facilities managed by non-governmental organizations work on referral by DMHs and are considered a component of the system.
Patients can directly access specialist mental health services, although they are often referred by general practitioners. Community Mental Health Centers are the entry point of the system for the overwhelming majority of cases.
Data source
Since 1999, data on mental health services in Lombardy have been routinely collected by the Regional Psychiatric Information System. All DMHs and private day care and residential facilities provide information to the system, allowing a full description of service activities and treatments provided to patients by any professional. Very few private hospital psychiatric beds, not reporting to the system, are available in the region (De Girolamo et al., 2007). When this study was planned, 2009 was the last year with full data available.
As a psychiatric case register, the system collects demographic information (sex, age, marital status, living arrangement, employment, education) and ICD-10 (International Classification of Diseases, 10th Revision) diagnoses on any resident in Lombardy with at least one contact with mental health services. All care episodes and interventions in any setting (outpatient and home contacts, day treatment attendance, admissions to hospital and residential facilities) are recorded. Diagnoses are regularly checked and updated.
All interventions, professionals and treatment settings are classified and coded according to the operational definitions provided in the Regional Psychiatric Glossary (Regione Lombardia, 1996).
Data on mental health care delivery and service utilization were retrieved for 143,184 cases, including all the residents in Lombardy ⩾18 years old who had at least one contact in 2009 with mental health services. All patients with a diagnosis of bipolar disorders according to ICD-10 codes (F30, F31, F34.0, F38.0) were identified as the reference group. Patients with a diagnosis of schizophrenia and related disorders (ICD-10 F20–F29) and unipolar depression (ICD-10 codes F32, F33, F43.20, F43.21) were selected to allow comparisons with patterns of care for the other main categories of major mental disorders, as in previous studies (Lora et al., 2011). The study was approved by the Health Department of Lombardy Region. To preserve patient privacy, the identification codes from the database were converted into anonymous codes and the conversion table was destroyed.
Data analysis
We first assigned a specific package of care to each patient, through a method presented in previous papers (Lora, Cosentino, Gandini, & Zocchetti, 2007; Monzani, Erlicher, Lora, Lovaglio, & Vittadini, 2008), and calculated the distribution of care packages across the three diagnostic groups. Care packages have been defined as the cluster of services, based on carefully constructed components, provided to each patient in different settings by different professionals in a specific time frame (Grigoletti et al., 2010; National Health Service (NHS) Executive, 1997). As described elsewhere (Lora et al., 2007), a previous analysis identified five mutually exclusive packages for individual patients in the course of 1 year:
Clinical package. At least one outpatient contact with psychiatrists or psychologists, without admission to day care, hospital or community residential facilities.
Community package. At least one outpatient contact with psychiatrists or psychologists and other professionals, such as nurses, social workers, rehabilitation counselors, without admission to day care, hospital or community residential facilities.
Day Care package. At least 1 day in a day care center, with or without outpatient contacts, without admission to hospital or community residential facilities.
Hospital package. At least one hospital admission, with or without outpatient contacts, without admission to community residential facilities.
Residential package. At least one admission to a community residential facility, independently of contacts with any other facility.
Second, in accordance with the indications of the Regional Psychiatric Glossary, we grouped the interventions registered by the Information System in outpatient and home care settings into seven broad categories and calculated the number of patients who received them:
Psychotherapy. Psychological intervention using a specific clinical model delivered by a psychiatrist or a psychologist to individuals, groups, couples or families.
Family intervention. Intervention aimed at supporting or consulting patient’s families.
Social support. Intervention aimed at supporting the patient in everyday life activities in real life settings.
Socialization. Intervention aimed at helping the patient participate in social activities in individual or group settings.
Rehabilitation. Intervention aimed at improving the patient’s social, interpersonal, vocational and illness management skills.
Network intervention. Intervention aimed at supporting or consulting the patient’s formal or informal network.
Visit. Outpatient or home contact with any professional not belonging to the previous categories.
Third, we classified as ‘psychosocial interventions’ the following specific interventions included in the ‘psychotherapy’ and ‘family intervention’ categories: individual psychotherapy, couple/family therapy and group psychotherapy in the ‘psychotherapy’ category; meeting with relatives, family psychoeducation and relatives group in the ‘family intervention’ category, calculating the number of patients who received them.
Descriptive statistics for all variables were computed for each diagnostic group. For psychotherapy and family interventions, in addition to the percentage of patients receiving the intervention, we also reported the median number of interventions delivered. For each variable, comparisons of the bipolar disorder group and the schizophrenic disorder and depressive disorder group were made using chi square statistics for categorical variables and t-test for continuous variables. Because of the large sample size, most of the comparisons were statistically significant; therefore, we did not flag all the significant comparisons in the tables and graphs in which this information would have been redundant. All analyses were done with IBM SPSS Statistics v. 21.
Results
Sample characteristics
Diagnosis was missing for 4,936 cases (3.4%). Among 139,248 cases with a valid diagnosis, 8,899 (6.4%) had a diagnosis of bipolar disorder, 34,338 (24.7%) of schizophrenia and 29,609 (21.3%) of unipolar depression. Treated prevalence on adult population was 1.1‰ for bipolar disorders, 4.1‰ for schizophrenia and 3.5‰ for unipolar depression. However, in some cases (6.9% for bipolar disorders, 4% for depression, 10.1% for schizophrenia), information on psychosocial interventions was missing or incomplete, therefore a final sample of 8,285 cases of bipolar disorder, 30,908 of schizophrenic disorder and 28,425 of depression, with full information on treatments, was targeted for analysis.
Sociodemographic characteristics of the three diagnostic groups are shown in Table 1. Only 11% of patients with bipolar disorders were younger than 34 years. Most of them were female and more than one-third had completed high school. The great majority were in contact with a mental health service before 2009. Distribution by sex across diagnostic groups showed a majority of women among people with bipolar and depressive disorders, with a larger percentage in unipolar depression.
Sample characteristics.

MHS: mental health service.
Comparisons adopted bipolar disorder as a reference group.
Statistically significant differences (chi square): *p < .5; **p < .01.
Care packages
Table 2 shows that more than 80% of bipolar disorders were treated on outpatient basis, as indicated by the high frequency of clinical (45.4%) and community (35.6) packages. A few had one or more hospital admissions and even fewer were treated in residential or day care settings. Compared to the bipolar group, patients with schizophrenia received more community (48.6%), day care (6.5%) and residential (7.8%) packages and fewer clinical (27.1%) and hospital (9.9%) packages. The proportion of patients with bipolar disorder admitted to hospital was low but higher than for patients with schizophrenic or depressive disorders.
Distribution of care packages across diagnostic groups.
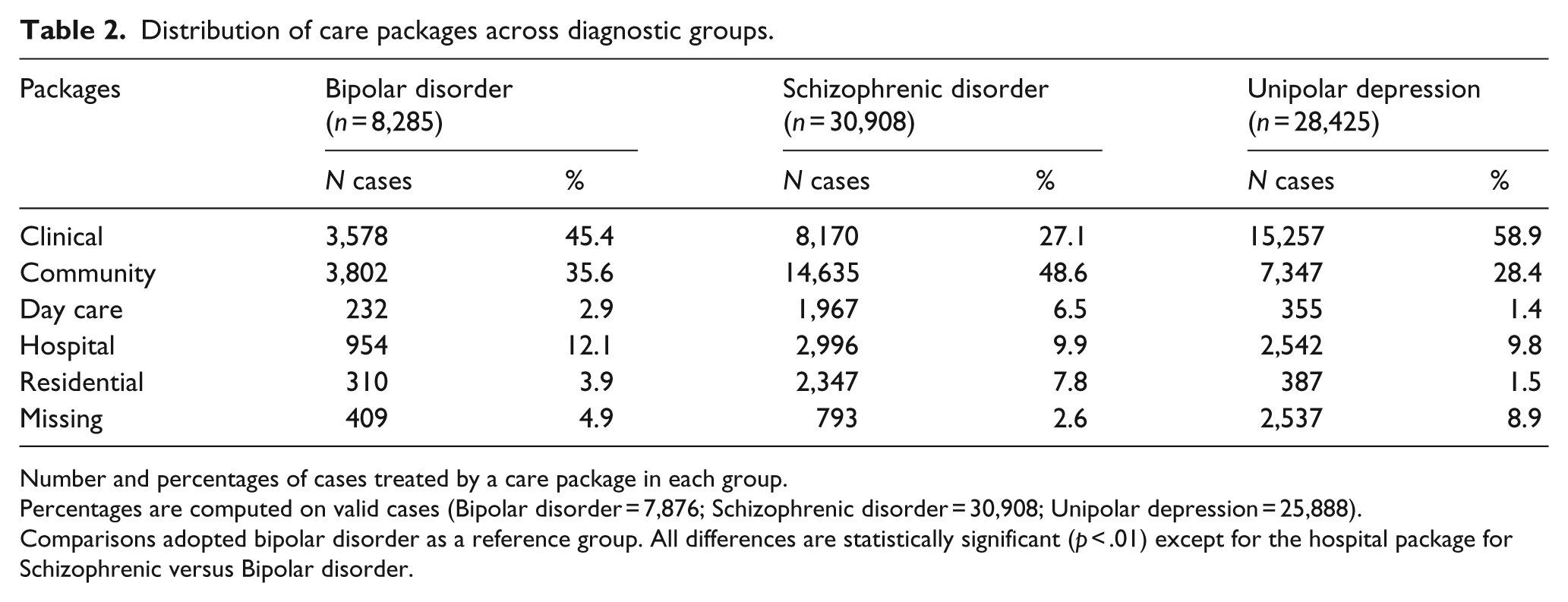
Number and percentages of cases treated by a care package in each group.
Percentages are computed on valid cases (Bipolar disorder = 7,876; Schizophrenic disorder = 30,908; Unipolar depression = 25,888).
Comparisons adopted bipolar disorder as a reference group. All differences are statistically significant (p < .01) except for the hospital package for Schizophrenic versus Bipolar disorder.
Categories of interventions received
Almost all patients received generic mental health care, represented by the ‘visit’ category (Figure 1). This included drug prescription and monitoring, assessment, evaluation and supportive counseling. Contacts with families were relatively common for people with schizophrenia and bipolar disorders, involving 41% and 32% of patients, respectively. By contrast, structured psychotherapy was delivered to a very small proportion of patients, without significant between-group differences.

Percentage of patients receiving intervention categories.
With regard to social support, socialization, rehabilitation and network interventions, a steady difference between groups was observed: people with bipolar disorder received less than people with schizophrenia but more than those with depression.
Psychosocial interventions
Tables 3 and 4 allow a deeper analysis of interventions included in the ‘psychotherapy’ and ‘family interventions’ categories. Only the intervention labeled ‘meeting with relatives’ was delivered to a substantial number of people with bipolar disorder. Very few of them received other interventions, ranging from 0.7% for ‘Couple/family therapy’ to 6.1% for ‘Individual psychotherapy’. Excluding meetings with relatives, less than 7% of the individuals with bipolar disorder had access to any structured psychosocial intervention. The median number of interventions delivered shows the very low intensity of all psychosocial interventions and raises doubts about the adequacy of treatments.
Distribution of psychosocial interventions across diagnostic groups.
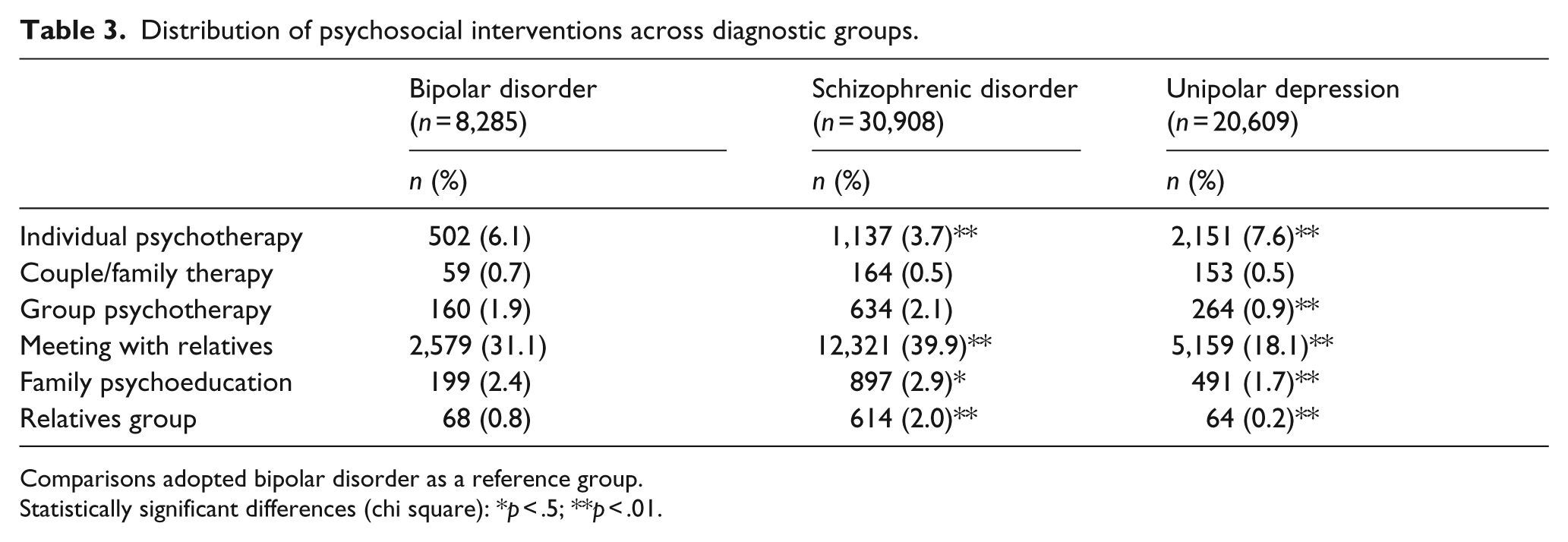
Comparisons adopted bipolar disorder as a reference group.
Statistically significant differences (chi square): *p < .5; **p < .01.
Median numbers of sessions by diagnostic groups.
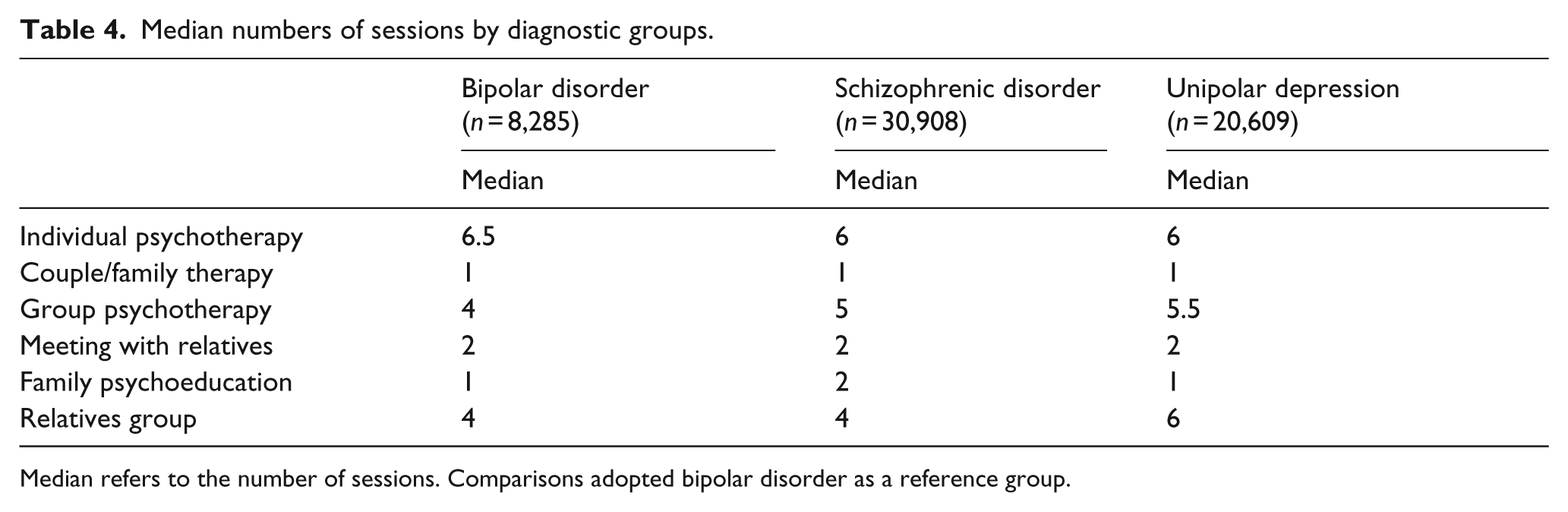
Median refers to the number of sessions. Comparisons adopted bipolar disorder as a reference group.
Differences across groups, although in some cases statistically significant, were of little clinical relevance. The only exception was the huge difference between the schizophrenia and depression groups in the percen-tage of patients whose relatives had meetings with the professionals.
Stratification by age
Subjects with a bipolar disorder or depression in the aged more than 65 years most frequently received a clinical package, with 52% of subjects aged more than 65 years with a bipolar disorder being in this care package and 63.8% of subjects aged more than 65 with a diagnosis of depression, and received the lowest amount of residential care (1.3% and 0.8% respectively). Among individuals with a diagnosis of schizophrenia, those aged 55–64 received the highest amount of community package treatments, and those >65 years the lowest amount of residential care.
Across the three diagnostic groups, people younger than 25 years received more individual psychotherapies compared to the other age classes. Meetings with relatives were more frequently delivered to subjects under 25 years in the bipolar disorder (41%) and schizophrenia (52%) diagnostic groups, and in the depression diagnostic group meetings with relatives were more common for subjects over 65 years (23.9%).
Discussion
The bipolar disorder treated prevalence in specialist mental health services of 1.1‰ was very low, about one-fifth of treated prevalence found in other countries (Bih et al., 2008; Bulloch et al., 2011). By contrast, treated prevalence of schizophrenia fits around the median of population-based prevalence found in 188 international studies (Saha, Chant, Welham, & McGrath, 2005). The treated prevalence of 3.5‰, for major depression, is less than one-tenth of the expected prevalence of 4% (Waraich, Goldner, Somers, & Hsu, 2004), the vast majority however being treated in the primary care sector (Kisely et al., 2009), not covered by the Lombardy Region database.
Although no nationwide epidemiological figures on major mental disorders are available for the Italian population, a community survey in six areas of Italy showed a prevalence of bipolar disorder of 3% (Carta et al., 2012). Conservative estimates of the true prevalence of bipolar disorders in Western Europe are around 8‰ (Ferrari et al., 2011). These data suggest in our sample a treated specialist prevalence of less than 15% of the population-based prevalence. Although treated prevalence lower than the true prevalence can be expected, because people with mild forms of any disorder do not contact the health care system, such a low figure requires an explanation.
Misdiagnosis can partly account for this, because it has been suggested that up to 40% of bipolar disorders are misdiagnosed as unipolar depression or, to a less extent, as schizophrenic spectrum disorder (Hirschfeld, Lewis, & Vornik, 2003). It is also possible that an unknown number of patients are treated in private practice or in primary care. Recent findings from a study of lithium prescriptions in Lombardy provide some support for this hypothesis (Parabiaghi et al., 2015). The prevalence rate of lithium prescriptions was 1.5‰, about 50% higher than the bipolar disorder treated prevalence in psychiatric services. Moreover, general practitioners accounted for 75% of prescriptions. Since lithium is mostly used for bipolar disorders, this means that a sizeable group of patients with bipolar disorder is probably treated in primary care or in office-based private practice. It has been suggested that for bipolar patients, private practice is first or second (after family doctors) line of treatment, because only the most severe cases are referred to public services (Benazzi, 2003). However, no data are available to support this claim. Moreover, private specialists usually send their recommendations for drug treatment to general practitioners, who then complete the prescription forms. Therefore, taking everything into account, a huge treatment gap cannot be ruled out.
The answer to our first question is straightforward: although the majority of people with a diagnosis of bipolar disorder are treated in community settings, only a tiny minority have access to any psychosocial intervention. For the average patient, contacts with mental health services are therefore limited to routine visits, assessments and drug prescriptions, with poor provision of specific psychosocial interventions. The relatively high rate of family interventions shows that services kept to some extent in touch with patients’ relatives. However, they failed to deliver structured interventions, such as family therapy or family psychoeducation. It is worth noting that intervention labeled as ‘meeting with relatives’, representing the vast majority of family interventions, include, according to the regional psychiatric glossary (Regione Lombardia, 1996), any encounter of any professional with patients’ relatives. Therefore, its classification under the heading of psychosocial interventions could be questioned. This confirms a previous survey of a randomly selected sample of outpatients with bipolar disorder and their key relatives recruited in 26 Italian mental health centers. Only 3% received some form of psychoeducation (Magliano et al., 2009). The failure to provide such interventions is especially striking, if we consider the level of family burden linked to bipolar disorders and its influence on course and outcome (Del Grande da Silva et al., 2014), as well as the characteristics of the Italian socio-cultural background characterized by strong family ties and involvement of relatives in caregiving (Luciano et al., 2012).
Concerning the second question, lack of access to structured psychosocial treatments in Lombardy was not limited to the bipolar group, but was also found in the two comparison groups. However, patients with schizophrenia received significantly more interventions in the rehabilitation category, thus indicated, as noted in previous studies (Lora et al., 2011), that the mental health system in Lombardy, although operating as a generalist rather than illness-specific programming, is to some extent more oriented toward the needs of people with schizophrenia and related disorders.
It is harder to answer the third question. Although, as we said before, we have no direct information on models and quality of treatments, we can assume that the very low intensity shown by the low median of interventions delivered falls below the minimal thresholds for any intervention to be considered of acceptable quality. Generally speaking, minimally adequate treatment for any psychotherapy has been defined as requiring at least eight contacts (Wang et al., 2005) and even more if we consider evidence-based interventions specific for bipolar disorders (Miklowitz, 2008). Swartz (2014) has raised the possibility that, at least for some subgroups of patients, a less intensive intervention (only three sessions of family psychoeducation) can be effective. However, the median of psychoeducation sessions delivered to our sample was one.
Although psychiatric services in Italy are community-based and espouse a public health approach, it has been noted that the attitude to invest in evidence-based treatment is still unsatisfactory (Thornicroft & Tansella, 2014). The finding that in a well-developed system of community care based on generalist services people with bipolar disorders have very limited access, if any, to effective psychosocial interventions, could confirm Vieta’s (2013) opinion that centralized expert treatment centers may be more effective than standard community care for those patients. This is supported by a recent study showing that treatment in a specialized mood disorder clinic early in the course of bipolar disorder substantially reduced hospital readmissions and increased satisfaction in comparison with generalist services (Kessing et al., 2013). However, other studies reached different conclusions: a controlled trial by Candini et al. (2013) showed that group psychoeducation targeted at bipolar disorders, in addition to drug therapy, was effective in preventing hospitalization and reducing inpatient days in routine clinical settings of ordinary services. This study is important because it was done in the region covered by our own data collection.
The reasons for the lack of implementation of well-known guidelines should be urgently investigated. It has been observed that guidelines can be implemented only if the changes involved are affordable and if are sufficiently consistent with staff opinions. This may be particularly true for psychosocial interventions (Morriss, 2008). Lack of access to psychotherapy, even in models based on shared care, has been noted for depressive disorders as well (Kates & Mach, 2007).
Efforts to understand the reasons for limited provision of structured treatments, such as psychoeducation, in psychiatric settings generally gave unsatisfactory results. In a survey of UK teams, lack of research evidence was not reported as a reason for not providing psychoeducation. The main reasons were financial constraints and excessive workload (Getachew, Dimic, & Priebe, 2009). A recent Italian study by Fiorillo et al. (2016) addressed the feasibility of psychoeducational family intervention for bipolar disorder in 11 mental health centers. Professionals, although reporting several benefits, found high level of organizational difficulties, mainly related to problems in integrating the intervention with service duties. However, these reasons are non-specific and are always likely to be mentioned for any innovation.
Probably, we need implementation strategies of interventions found effective in clinical trials at the national and local levels (Briand & Menear, 2014). A recent Health Evidence Network Consensus Conference precisely suggested technical assistance center that would include academic experts to support the implementation, supervision and quality control of individual psychosocial interventions and psychotherapies for severely mentally ill (Institute of Health Economics, 2014).
Study limitations should be kept in mind when interpreting these results. First, the database did not cover private practice by psychiatrists or psychologists nor primary care. Second, interventions delivered during admission to inpatient care were not included. Third, reliability of the information routinely collected by the system could be open to question. Fourth, operational definitions of interventions provided by the regional glossary refer to the treatment format (individual, group, family) but do not specify the treatment model. Fifth, no information on quality of intervention was available.
Therefore, the possible influence of these limitations on the results has to be considered. Although interventions delivered during inpatient admission are not recorded by the system, the number of patients receiving them would be small, because more than 80% of bipolar cases were treated as outpatients, and interventions delivered in hospital could not change the whole picture. We already noted that some patients with bipolar disorders are treated in primary care, so treatments received by this group are not covered by the psychiatric information system. However, it is unlikely that general practitioners in Italy deliver specific psychosocial interventions. It is possible that such interventions are offered to a subgroup of patients by psychiatrists and psychologists in office-based private practice, but we have no information on this. Epidemiological studies of private practice are very scarce and we acknowledge that this should be the focus of thorough investigations. Problems related to the quality of data collected by the system and the lack of information on treatment models do not affect the key finding of limited access to psychosocial interventions.
Conclusion
This large scale survey shows that, despite feasibility studies and proliferation of evidence-based recommendations and guidelines, offer of psychosocial interventions to people with bipolar disorders by community-based mental health services in the largest Italian region was clearly inadequate.
These negative results are a matter of concern and pose some major questions. Studies of effective ways of implementation and dissemination of psychosocial interventions for bipolar disorders should be considered more important than further trials of the effectiveness of interventions.
Barriers to the adoption of evidence-based practices and investigation of successful strategies for training professionals, implementation and dissemination in mainstream mental health services are top targets for the future research agenda in this area.
Footnotes
Acknowledgements
We thank Germana Agnetti and Paolo Rigliano for their useful comments and Judith Baggott for the English language revision. This study was carried out in the framework of the ENBREC (European Network of Bipolar Research Expert Centers), a project funded by the European Union designed to foster multinational collaboration among centers with expertise in the clinical management of and/or research in bipolar disorders (Henry et al., 2013).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the project was provided by the European Union’s seventh framework program FP7/2007–2013 under grant agreement 223102.