
Abstract
Background:
There is a dearth of instruments to assess schizophrenia persons’ Family Emotional Climate (FEC).
Aim:
This study aims to explore the relation between family members’ personality traits and FEC.
Methods:
We invited a convenience sample of 50 both gender family members who were accompanying the person with schizophrenia for out-patient department (OPD) consultation to provide data on a socio-demographic proforma and the researcher prepared ‘Emotional climate assessment questionnaire – caregivers’ version’ (ECAQ-C) as well as the Eysenck personality questionnaire.
Results:
Caregivers’ extroversion traits (r = .427, p = .002) were positively correlated and neuroticism traits were negatively correlated (r = −.330, p = .019) with their positive perception of FEC. There was a higher perception of positive FEC (mean scores = 65.5 ± 10.5) while caregivers seemed to perceive less negative FEC (mean scores = 36.5 ± 10.2). Caregivers with education above 11th std perceived less (χ2 = 8.6, p = .013) of negative FEC.
Conclusion:
The findings highlight that caregivers’ personality traits seem to influence the FEC. While caregivers’ perception of FEC is positive in this study, those in the higher education group seem to have a better perception of FEC indicating that education also may influence FEC.
Introduction
A significant number of people with schizophrenia continue to experience long-term impairments, and as a result the illness can have a considerable effect on people’s personal, social and occupational lives. Worldwide, it has been estimated that schizophrenia falls into the top 10 medical disorders causing disability (National Institute for Health and Clinical Excellence, 2010). Illness relapse is a challenge faced by mental health professionals as well as the person with schizophrenia and the family. Several naturalist studies have demonstrated that patients in families having high levels of expressed emotions (EE) are significantly more likely to experience a clinical relapse than patients residing in households with low levels of EE (Nirmala, Vranda, & Shanivaram, 2011). In India, the great majority of schizophrenia patients stay with their families, and more so in joint families (Thara, Padmavati, Kumar, & Srinivasan, 1998), whereas an estimated 50%−80% of patients with schizophrenia live with or have regular contact with a family caregiver (Lehman & Steinwaches, 1998). The importance of the patient’s home environment is highlighted by the vulnerability stress model of schizophrenia which postulates interaction between an enduring vulnerability and stressful events in the environment as a predictor of breakdown and relapse (Nuechterlein & Dawson, 1984). Research has consistently established that persons with mental illness, such as schizophrenia, who live with close relatives who have negative attitudes, are significantly more likely to relapse (Bebbington & Kuipers, 1994; Brown, 1985). The family’s EE has been shown to be predictive of outcome in mental and physical illnesses in a variety of cultural settings (Nirmala et al., 2011).
EE are neither pathologic nor unique to only families of persons with mental illness. Not much is known about why some relatives display high EE whereas others do not do so. Critical relatives are more likely than non-critical relatives to believe that schizophrenia patients’ negative behaviours are intentional (Clough & Hooley, 2003). A critical evaluation of the various measures of EE (Hooley & Parker, 2005) helped us identify various instruments. These were the Camberwell Family Interview (CFI) (Leff & Vaughn, 1985), the Five Minute Speech Sample (FMSS) (Magaña et al., 1986), the Level of Expressed Emotion Scale (LEE) (Cole & Kazarian, 1988), the Family Attitude Scale (FAS) (Kavanagh et al., 1997) and the Perceived Criticism Scale (PC) (Hooley & Teasdale, 1989). However, none of these instruments could be used with Indians as the items were culturally not relevant. Hence, we had to develop a culture specific instrument. We could not find any research on the influence of personality factors of relatives of persons with schizophrenia on their EE. We decided to explore whether personality could be associated with the family emotional climate (FEC). We preferred to study FEC rather than EE. Developed in the 1960s and 1970s in England by Brown and Rutter (1966) and Brown, Birley and Wing (1972) respectively, EE reflects the extent to which the close family members of an identified patient express critical, hostile or emotionally over-involved attitudes towards the patient during a private interview with a researcher (Hooley & Parker, 2005). From this, we understand that only non-therapeutic emotional expression is considered as EE. It is probable that therapeutic and warm emotions are also expressed within the family. FEC would then comprise of both warm emotions that are therapeutic as well as EE. We report in this article the caregivers’ perception of FEC as well as the impact of their personality traits on the FEC and the utility of a culture specific tool in an out-patient department (OPD) setting.
Methods
Subjects and sampling
The follow-up OPD of a neuro-psychiatric tertiary super-speciality hospital in Bangalore, India, was selected as the setting for data collection. Follow up out-patient services are available on all week days except specific government holidays. Every day a minimum of 50 persons with schizophrenia avail services. Of these, both gender caregivers who were above 18 years of age and staying with the patient for at least last 6 months were included in the study. Those who had visual or hearing impairment were excluded from the study. Caregivers of patients who were restless, symptomatic and violent were also excluded as they would not be able to spend time with the investigators. Caregivers of patients who had two and more than two episodes of either paranoid or undifferentiated schizophrenia (International Classification of Diseases (ICD) 10 classification) only were included in this study. Subjects who were willing to participate were selected for the study after informed consent. Convenience sampling technique was used to invite subjects to participate in the study.
Procedures
The study was approved by the Institute Ethics Committee. Written informed consent was obtained from the subjects who were then invited to participate in the study, and declaration of confidentiality was made before the interview. Interviews were conducted by the second author after establishing inter-rater reliability for the tool. All information was collected through face-to-face interviews in a room providing complete privacy in the OPD of the hospital. The investigator sat face-to-face with each subject and requested to fill the demographic proforma. Thereafter, questioning technique was used to collect data with all the tools used in the study. The completeness of all the interviews and tools was checked immediately.
Instruments and measures
A socio-demographic profile questionnaire was developed specifically for this study and included variables classified as caregivers’ profile such as age, gender, education, occupation, marital status, domicile and presence of any psychiatric or physical illness as well as patients’ profile such as duration of contact with the caregiver, duration of illness, number of illness episodes and number of admissions.
The Eysenck personality questionnaire (Eysenck & Eysenck, 1991) was used to assess the caregivers’ personality traits. The tool was purchased and permission sought for translation into Kannada and Telugu. The translated version was validated through back translation.
The ‘Emotional climate assessment questionnaire – caregivers’ version’ (ECAQ-C) was developed to specifically explore caregivers’ EE that could be construed to be negative as well as indicated warmth. It consisted of 40 items on a 1- to 4-point scale (From ‘never’ i.e. 1 to ‘always’ i.e. 4) and with six domains – Criticism, hostility, emotional over-involvement (EOI), warmth, positive reinforcement and optimism. The items in the criticism, hostility and EOI domains comprised negative FEC and those in the warmth, positive reinforcement and optimism domains comprised positive FEC. Higher scores in the negative FEC domains indicated higher negative FEC and higher scores in the positive FEC domains indicated higher positive FEC. This tool was validated by a multi-disciplinary team of psychiatrist, clinical psychologist, psychiatric social worker and psychiatric nurse. The validated tool was translated to Kannada and Telugu. Back translation was also done. Inter-rater reliability was established (.78, p = .008) and the tool was pilot-tested before use in the main study.
Statistical analysis
The
Results
Caregiver characteristics
There were 50 caregivers with mean age of 44.7 ± 13.1 years, minimum age being 19 years and maximum age being 72 years. More female caregivers (62%) accompanied the patient to the OPD. There was a lack of formal education in 26% and only 24% had reached up to graduate level while the rest had varying degrees of intermediate education. Most of them were married (74%) and belonged to nuclear (74%) families. In most cases, the mother (36%) accompanied the patient while the rest were accompanied by their wife (12%), husband (18%) or children (34%). Some (4%) of the caregivers had both hypertension and diabetes mellitus, while 6% had hypertension, 2% had diabetes mellitus and 2% had paranoid schizophrenia, 2% substance abuse and 2% had depression. The caregivers’ illness profile was self-reported. However, the authors had not checked if the caregivers with mental illness were in remission.
Patient characteristics
The mean duration of patients’ stay with the family member was 19.8 ± 12.1 years ranging from a minimum of 1 to 45 years and median 23 years. Majority of the patients (46%) had two illness episodes, 36% had three episodes, 4% had five episodes and 8% had six episodes. Most (42%) of the patients were admitted once, 36% were admitted twice, 8% were earlier admitted thrice after the onset of illness and the rest (14%) had been earlier admitted five times. The median duration of illness was 12 years and ranged from 2 to 32 years.
Caregivers’ personality traits
As shown in Table 1, the mean score for extroversion was 11.96 + 4.13, psychoticism was 4.22 + 1.91 and neuroticism was 11.16 + 4.19, with a lie score of 17.14 + 3.33. More caregivers seemed to be having extroversion as a major personality trait and psychoticism as a minor trait. The lie score was high.
Mean scores of family members’ (n = 50) personality traits.
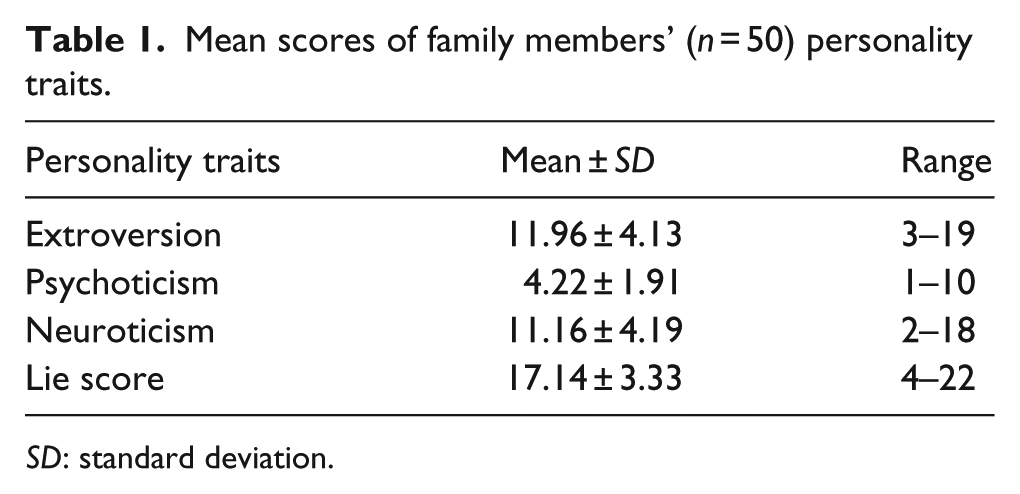
SD: standard deviation.
Caregivers’ perception of FEC
Caregivers seemed to perceive more of positive FEC as depicted in Table 2. The mean scores of optimism (22.94 ± 3.7), positive reinforcement (18.3 ± 3.31) and warmth (24.3 ± 3.9) seemed to be higher than the mean scores of criticism (13.1 ± 4.4), hostility (12.38 ± 3.7) and EOI (11.1 ± 3.3). The overall mean scores (65.5 ± 10.5) of positive FEC were also higher when compared to the overall mean scores (36.5 ± 10.2) of negative FEC.
Total and domain wise levels of perception of FEC by family members (n = 50).
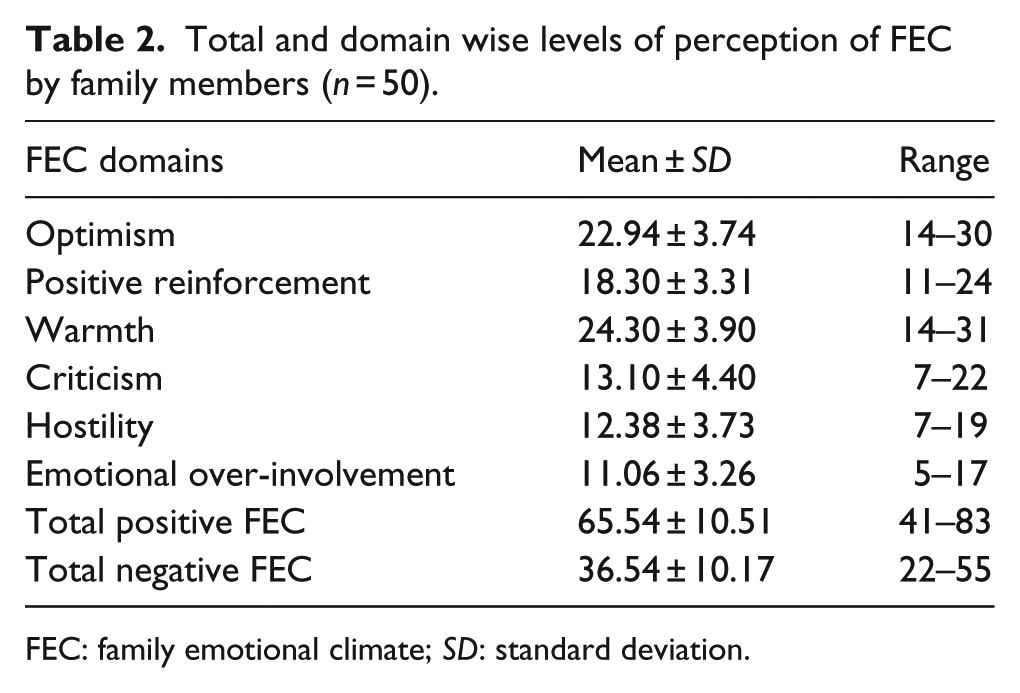
FEC: family emotional climate; SD: standard deviation.
Association of caregivers’ perception of FEC with socio-demographic variables
None of the caregivers’ socio-demographic variables had association with positive FEC. However, as Table 3 shows, caregivers with education above 11th std perceived less (χ2 = 8.6, p = .013) of negative FEC. The association of physical and psychiatric illness in caregivers with perception of negative FEC could not be calculated due to fewer frequencies in the cells. All other socio-demographic variables did not have association with negative FEC.
Association of perceived negative FEC of caregiver group with selected socio-demographic variables (n = 50).
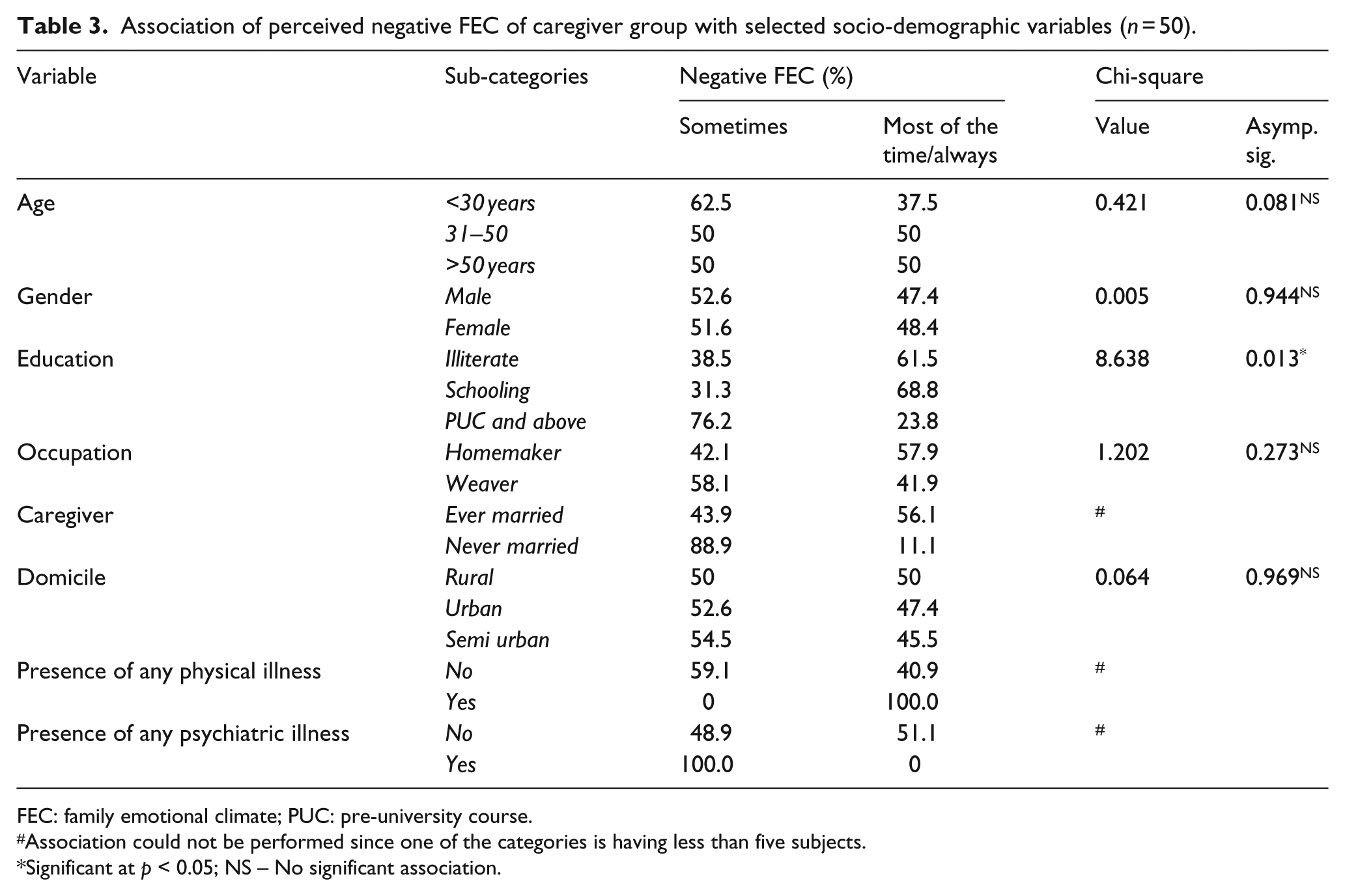
FEC: family emotional climate; PUC: pre-university course.
Association could not be performed since one of the categories is having less than five subjects.
Significant at p < 0.05; NS – No significant association.
Correlation of caregivers’ perception of FEC with their personality traits
As displayed in Table 4, there is a significant positive correlation between caregivers’ extroversion traits (r = .427, p = .002) and negative correlation between caregivers’ neuroticism traits (r = −.330, p = .019) with their positive perception of FEC. There is a significant positive though moderate correlation between caregivers’ extroversion traits (r = .402, p = .004), psychoticism traits (r = .306, p = .031) and neuroticism traits (r = .456, p = .001) with their perception of negative FEC.
Correlation of perceived FEC of subjects in caregiver group with the levels of personality traits.

FEC: family emotional climate; SD: standard deviation.
Significant at p < .05; NS – not significant.
Discussion
EE is a significant characteristic of the family milieu that has been found to predict symptom relapse in a wide range of mental disorders (Butzlaff & Hooley, 1998). The importance of EE depends on research that has consistently established that persons with mental illness, such as schizophrenia, who live with close relatives who have negative attitudes, are significantly more likely to relapse (Butzlaff & Hooley, 1998). However, in India, family is the main support system for the person with mental illness. Caregivers’ contribution and partnership in the treatment process is invaluable. Many of the available assessments focus on negatively classifying the families and their positive side has been neglected in the EE evaluation (Amaresha & Venkatasubramaniam, 2012). Another shortcoming of the current assessments is that they have been constructed, standardized and validated in the western countries and while applying in different cultural context, one has to consider various methodological constraints (Amaresha & Venkatasubramanian, 2012). In our search for a suitable instrument, we were unable to find one that was appropriate for and could be easily understood by Indian subjects. Hence, we felt the necessity to construct and validate a culture specific tool. Amaresha and Venkatasubramanian (2012) in their overview on EE in schizophrenia also emphasized that culture specific measurements have to be constructed and validated.
Most caregivers accompanying the patient to the OPD in our study were either women (62%) or mothers (34%) indicating that more of women in Indian families take on the caring role. Families in India also generally do not abandon the person with mental illness and may support them on the road to recovery. Recovery meant living with family, working for the family and contributing to the family because issues in the family relationships could be seen during the illness state (Jose et al., 2015).
In our study, more caregivers seemed to be having extroversion (mean score: 11.96 + 4.13) and neuroticism (mean score: 11.16 + 4.19) as a major personality trait and psychoticism (mean score: 4.22 + 1.91) as a minor trait. However, these scores have to be treated with caution as first the caregivers belonged to a diverse age group (19–72 years) and second the lie score was high, indicating that the caregivers might have given false ratings. Moreover, extraneous factors that could affect the caregivers’ rating on the Eysenck personality questionnaire (Eysenck, H. J., & Eysenck, S. B. J., 1991) were not controlled in this study. Although the precise reason for high or low EE attitudes in caregivers is not yet completely unravelled, it has been suggested that EE might partially reflect caregiver’s personality traits (Hooley & Hiller, 2000). A critical comment (CC) of the caregiver is dependent less on the degree of the patient’s symptoms than on the caregiver’s own personality factors (Amaresha & Venkatasubramanian, 2012). Conversely, in another study, results seemed to suggest that EE is largely reactive to deterioration manifested by the young person developing a psychotic disorder, rather than a trait of family members (McFarlane & Cook, 2007).
Surprisingly, in our study, caregivers seemed to have perceived the FEC as more positive (total mean score: 65.5 ± 10.5) than negative (total mean score: 36.5 ± 10.2). The ratings were subjective and considering the high lie score on the Eysenck personality questionnaire (Eysenck & Eysenck, 1991), this result may have to be treated with caution. Moreover, 6% of the caregivers had self-reported mental illness. It was assumed that they were in remission. They were not assessed for this. It is possible that their clinical status could have influenced their rating on the FEC. However, since it is a small proportion of the sample (6%), its influence on the overall outcome may be small. It generally takes half a day or the entire day for a patient to complete follow-up interviews with his or her psychiatrist in the OPD. Reluctance to rate the questionnaire because of time constraints or time consumed to complete the assessment (although the pilot study revealed that assessment could be done in 15 minutes) or an instinct to give desirable answers could have contributed to this result. At the same time, one needs to remember that these were caregivers of out-patients who were most probably reasonably preserved and stable and probably this was the reason for a positive and warm FEC. Similar results were reported in another study from the East (China) wherein a proportion of relatives rated as high-EE was 28.2%, and the Chengdu relatives expressed significantly fewer CCs and less EOI than respondents in other similar studies in the West. Within the Chengdu sample, city dwellers were significantly (p < .05) more expressive than villagers expressing warmth, positive remarks, and EOI (Ran Mao-Sheng, Leff Julian, Hou Zai-Jin, Xiang Meng-Ze, and Lai-Wan Chan Cecilia, 2003) . Kumar, Gupta and Shweta (2007) reported that there was a significant difference in family environment between 50 normals and 50 persons with schizophrenia matched for age and gender. High levels of EE and EOI were reported in a sample of 35 caregivers of persons with schizophrenia attending the day care centre of a psychiatric hospital (Nirmala et al., 2011). The duration of illness was 5.8 ± 3.6 years and duration of caregiving was 5.9 ± 3.6 (Nirmala et al., 2011), whereas in our study, the illness duration was much higher with median of 12 years and mean duration of caregiving was 19.8 ± 12.1 years. Despite this, the caregivers perceived positive FEC. Possibly, this study emphasizes the need for shorter culture specific questionnaires to explore FEC which can be used in a busy OPD and would be sensitive enough to pick up EE.
In our study, caregivers with education above 11th std perceived more of positive FEC showing that education does seem to influence FEC favourably. The significantly negative though moderate correlation between personality traits and negative FEC indicates that it is possible that caregivers’ personality traits do influence their expression of emotions towards the person with mental illness.
Our study had several limitations. The sample size is small, non-randomized and consists of family members of persons with schizophrenia visiting the OPD of a neuro-psychiatric tertiary super-speciality at Bangalore, India and hence is not representative of the Indian population considering the diverse socio-cultural features across the country. Results have to be treated with caution keeping in mind the high lie score in the Eysenck Personality Questionnaire (Eysenck & Eysenck, 1991) and that 6% of the caregivers themselves had mental illness which might have influenced their rating on the FEC. Family members may be in a hurry to return home after their consultation. Hence, we recommend that OPD studies require a shorter assessment tool which can capture the FEC. The tool prepared for this study is culture specific; however, it may be better used in the in-patient or community setting where family members can respond in a more relaxed manner. However, the ECAQ-C is a preliminary tool and has to be standardized on diverse groups including a normal population before further decisions can be made on its sensitivity and cultural appropriateness. Persons with schizophrenia who come for OPD consultation may be more stable and less symptomatic. Hence the findings of this study may apply to such a population only. Further studies could be done to understand the patients’ perception of FEC, mental health professionals’ perception and observation of family’s EE within the hospital.
Conclusion
Culture-specific tools are necessary to capture FEC in its true form. Western tools may give mis-leading data when used in a country like India which has people with diverse cultures. A shorter version of this tool that can be administered in a busy OPD may give insight to the mental health professional about the FEC and this may help in counselling the family members about therapeutic communication and effects of EE on illness relapse as well as recovery. A comparison of perception of FEC between the family members and person who has schizophrenia may help mental health professionals in conceptualizing and preparing need-based interventions which may contribute to therapeutic FEC which can help in recovering with mental illness.
Footnotes
Acknowledgements
We wish to acknowledge the time taken by the family members who have participated in this study as well as all the experts from the multi-disciplinary team who have validated the tool used in this study. We also thank the administrative authorities as well as the institute ethics committee for permitting us to conduct this study. Data will be provided as supplementary material in excel sheet if needed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.