
Abstract
Background:
This study used attitude statement and vignette methodology to examine a mixed British sample’s belies about the causes and consequences of depression.
Aims:
To test whether the group would recognise both vignettes with having depression and that the favoured cure would be Psychotherapy/Talking Cure.
Method:
In all, 320 adults completed a two-part questionnaire. In the first part, they were given two vignettes describing a 30-year-old female and a 45-year-old male both with depression. They were asked what they thought (if anything) was wrong with the person and how they could best be helped. In the second part, they completed two questionnaires, one which lists 47 possible causes and the other 48 possible treatments for depression.
Results:
Most participants ‘diagnosed’ depression for the two vignettes although they chose very different terms and offered a variety of ‘cures’, including medication and counselling. The questionnaires about cause and cure factored into seven interpretable factors which were logically correlated. A series of regressions showed that sex, age, media interest, political beliefs, experience with depression and other mental illnesses as well as having known of others diagnosed with depression predicted different beliefs about the causes and cures of depression.
Conclusion:
People have a detailed and multidimensional view of the causes and cures for depression which is systematically related to each other.
Introduction
The term ‘mental health literacy’ (MHL) was introduced by Jorm and colleagues (1997) to mean ‘… knowledge and beliefs about mental disorders which aid recognition, management or prevention …’ (p. 182). This includes the ability to recognise specific disorders, knowledge about the causes and risk factors and knowledge of the help available. MHL is important as it can ensure that mental disorders are recognised early, and the appropriate help-seeking behaviour is encouraged (Jorm, 2012).
Most, but not all, of these studies have used the vignette technique which involves showing people a three- to six-sentence description of a person with specific symptoms of a particular disorder. Most studies have concentrated on depression and schizophrenia. Indeed, there are now studies which refer to ‘depression literacy’ (Deen & Bridges, 2011), ‘schizophrenia literacy’ (Furnham & Blythe, 2012) and a number of studies on ‘psychiatric literacy’ which have tended to focus on the personality disorders (Furnham & Winceslaus, 2012).
Previous studies relating to MHL have found that people have difficulty recognising mental disorders when they are described in a vignette (Link, Phelan, Bresnahan, Stueve, & Pescosolido, 1999). Furthermore, many people hold common misconceptions, for example, that schizophrenia involves a ‘split personality’ (Angermeyer & Matschinger, 1999; Furnham & Chan, 2004; Furnham & Rees, 1988). Early studies found that correct recognition rates of depression and schizophrenia were 39% and 27%, respectively (Jorm et al., 1997). Studies have also found that these have increased to around 50% for schizophrenia (Klimidis, Hsiao, & Minas, 2007) and 60%–70% for depression (Jorm, Christensen, & Griffiths, 2005). A higher rate for depression than schizophrenia may be due to the higher prevalence of depression in the population, which therefore increases the likelihood of contact with the disorder.
An important finding in this area is that the recognition of schizophrenia predicts endorsement of a biological or genetic aetiology (Jorm et al., 1997). Studies also show that both younger and more educated people have more informed beliefs about mental disorders (Fisher & Goldney, 2003; Shurka, 1983; Yoder, Shute, & Tryban, 1990). Significant effects of gender (Furnham & Manning, 1997), political persuasion (Furnham & Thompson, 1994) and religiousness (Furnham & Haraldsen, 1998) have also been found. This suggests that demographic variables may have some value in predicting MHL.
There are a number of studies on beliefs about depression. Furnham and Kuyken (1991) carried out a factor analysis of patients’ ideas about the causes for their depression and found six factors: social structure deprivations, interpersonal difficulties, traumatic experiences, affective deprivations, negative self-image and interpersonal loss. Kuyken, Brewin, Power, and Furnham (1992) confirmed that depressed patients and non-depressed laypersons have extensive beliefs about the causes of depression comparable to those held by clinical psychologists. However, depressed patients tend to endorse biological explanations of the causes of depression to a greater extent than clinical psychologists. Furthermore, the clinical psychologists assigned a more important causal role to unconscious processes and childhood vulnerability factors than do either depressed patients or non-depressed lay controls.
This study was replicated in Turkey on a student population. Cirakoglu, Kokdemir, and Demirtuku (2003) found that the perceived causes for depression resulted in six factors labelled trauma, job problems, loss intamacy, disposition and isolation. The cure items factored into seven factors labelled hobby, sensation seeking, avoidance, professional help, religious practices, esteem and spiritual activities. Studies have been replicated across cultures showing more evidence of similarity than differences (Hagmayer & Engelmann, 2014).
Most of the MHL literacy work in this area has used vignettes (Heim, Smallwood, & Davies, 2005). Swami (2012) reviewed a number of depression vignette studies done over a 10-year period and noted that the ability of the general public to identify someone with depression rose from around 40% to 70%. In his study, he varied the sex of the person in the depression vignette and found overall people thought the hypothetical male, compared to the female, was less likely to suffer any mental disorder and that female respondents were more likely to indicate that the male vignette had a mental disorder compared to the female. Loo, Wong, and Furnham (2012) showed that overall people were less able to identify depression in children than adolescents.
A number of studies using the same questionnaire have been done in Malaysia (Loo & Furnham, 2012, 2013; Swami, Loo, & Furnham, 2010). They reported studies that looked at culture differences in the identification of illness in two vignettes, the first reporting classic depression symptoms and the second depression with suicidal intentions. They essentially found four things. First, urban populations had a higher MHL than rural populations. Second, between one-third and two-thirds of the different populations (Chinese, Indian and Malay) were able to specifically identify the vignettes as people with depression. Third, the factor analysis of the causes of depression questionnaire tended to factor into similar identifiable factors labelled health and lifestyle, stress and trauma, biology and brain, supernatural/destiny/God and personality/will power. Fourth, the depression cure scales tended to factor into readily identifiable clusters labelled lifestyle change, professional treatment, religion and alternative therapies.
This study aimed to replicate the above in Great Britain, but also considering the role of participant ideology (political and religious beliefs) and media consumption as factors related to depression literacy. We hypothesised that over three-fourth of the group would recognise both vignettes with having depression (H1) and that the favoured cure would be Psychotherapy/Talking Cure (H2). We also predicted that those who had themselves been diagnosed with depression would have a less fatalistic theory about cause (H3) and cure (H4). Finally, we hypothesised that those with personal experience of others with depression would have a more medical/biological than psychological perspective on cause (H5) and cure (H6).
Method
Participants
Overall, 322 adults (105 males) with an average age of 26.20 years took part. Most were ethically White Europeans (63%), but there were a number of British South East and East Asians (27%) and Africans (2%). Just over half (50.6%) had at their maximum qualification a school leaving certificate, while 18% had a degree and 29% some other post-schooling qualification. They rated themselves on a religious scale from 1 = not at all to 7 = very (M = 2.80, standard deviation (SD) = 1.77) and political beliefs from 1 = strongly right wing to 7 = strongly left wing (M = 4.12, SD = 1.15). They were also asked whether they had ever been diagnosed with/suffered from depression (15% said yes) or another mental disorder (8% said yes). They were also asked whether they know anyone who had been diagnosed with depression (52% said yes). Finally, they were asked to rate on a 7-point scale (1 = not at all, 7 = very much) to what extent they had consulted various sources to understand media: Television (M = 2.91, SD = 1.61), Internet (M = 3.13, SD = 2.11), Academic books (M = 2.84, SD = 1.94), Science books (M = 2.17, SD = 1.56), Magazines (M = 3.02, SD = 1.69) and Radio (M = 1.98, SD = 1.36). The Cronbach’s alpha for consulting the media was .85.
Materials
This was in three parts. The first part involved the identification of two vignettes using names from the original Malaysian studies:
Case 1
Siti is 30 years old. She has been feeling really down for the last few weeks. She doesn’t enjoy things the way she normally would. In fact, nothing gives her pleasure. Even when good things happen, they don’t seem to make Siti happy. She has to force herself to get through the day, and even the smallest things seem hard to do. She finds it hard to concentrate on anything and has no energy at all. Even though Siti feels tired at night, she still can’t sleep, and wakes up too early in the morning. Siti feels worthless and feels like giving up. Her family has noticed that she hasn’t been herself for about the last month. She doesn’t feel like talking and isn’t taking part in things like she used to. In your opinion, what is wrong, if anything, with Siti? How do you think Siti could best be helped?
Case 2
Johan is 45 years old. In the recent month, Johan has been feeling unusually sad and miserable. He does not enjoy being with his friends and family as before. Even though he feels tired every day, he found it difficult to sleep at night and struggles to get out of bed in the mornings. He does not feel like eating and has lost a lot of weight. Johan cannot concentrate in his daily tasks, and finds it very difficult to function in the home and at work. Johan cannot keep his mind on his work and puts off making important decisions. This is causing problems in his job and his boss is concerned about his lowered productivity. Johan thinks he is a burden to his family and believes that they would be better off without him. Johan feels so strongly that he is unable to cope with life and unable to be happy anymore, he has been thinking of ways to end his life. In your opinion, what is wrong, if anything, with Johan? How do you think Johan could best be helped?
The second part involved the rating on a number of causes and treatments for depression (see Tables 1 and 2). These were derived from the anthropological, psychological and sociological literature (Angermeyer & Matschinger, 1999). Each was rated on a 7-point agree–disagree scale.
Frequency of diagnoses in Case 1.

SSRI: selective serotonin re-uptake inhibitor; GP: general practitioner; NHS: National Health Service; CBT: cognitive behavioural therapy; PMS: pre-menstrual syndrome; SAD: seasonal affective disorder.
Frequency of diagnoses in Case 2.
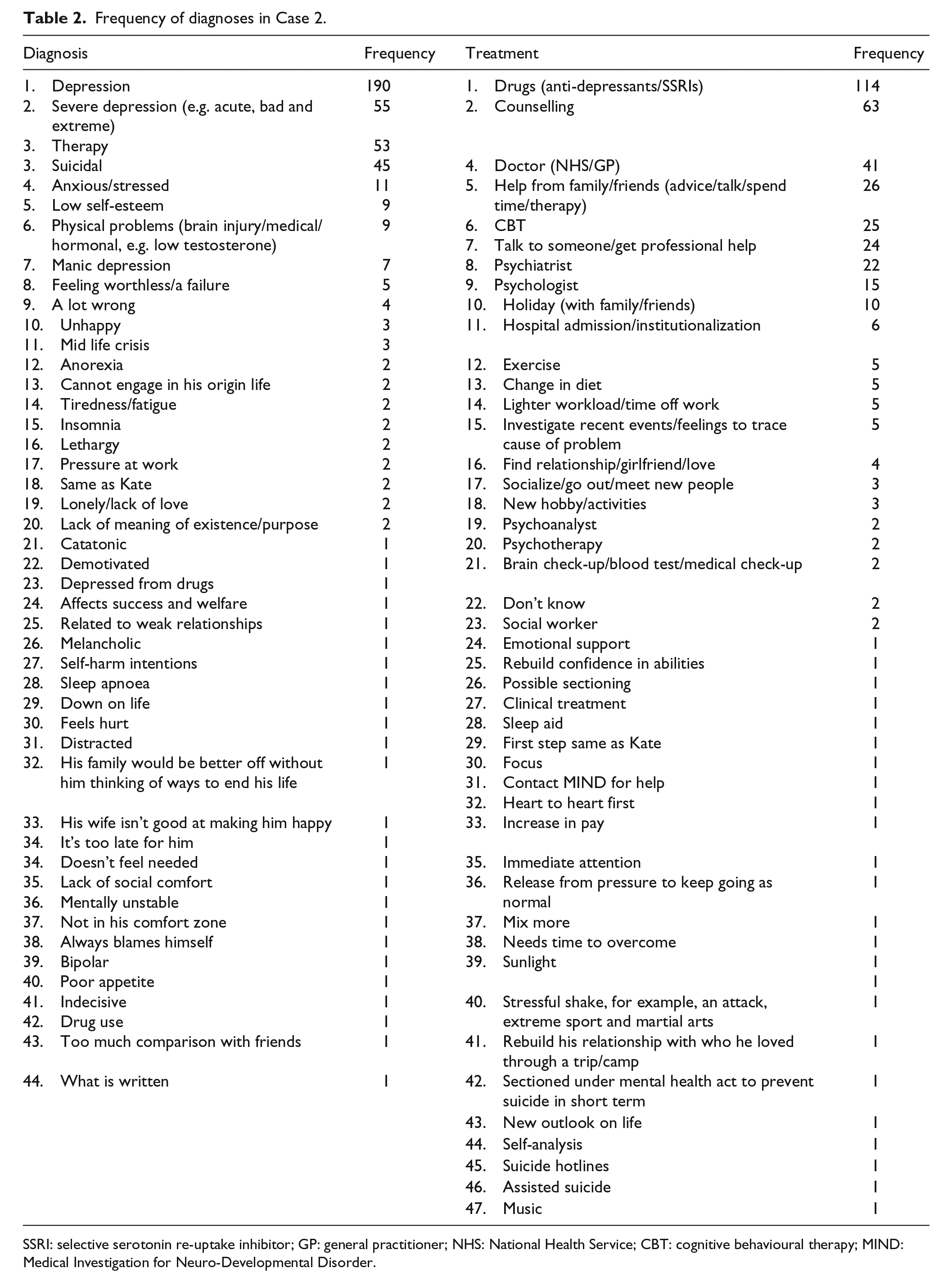
SSRI: selective serotonin re-uptake inhibitor; GP: general practitioner; NHS: National Health Service; CBT: cognitive behavioural therapy; MIND: Medical Investigation for Neuro-Developmental Disorder.
Procedure
Ethics permission was sought and received. The respondents were recruited from public places (parks, railway stations) and were approached by the researchers. Each was asked whether they could spare 10–15 minutes to take part in research. Of those who agreed, the response rate was over 90%. Each respondent was then debriefed by the researcher and assured that their responses would remain anonymous.
Results
Vignette
A Spearman’s rho test revealed no evidence of a correlation between age and perceived knowledge of depression r(306) = .03, p = .63. Table 1 shows that the vast majority (78%) used the word depression in the first vignettes and 76% in the second, supporting H1. There was less consensus about the best cure. In the first vignette, 39% said medication or doctor and 34% said counselling/psychologist/psychiatrist. The results were similar for the second vignette where 48% said doctor/drugs and 53% said counselling/therapy/psychologist/psychiatrist.
Causes of depression
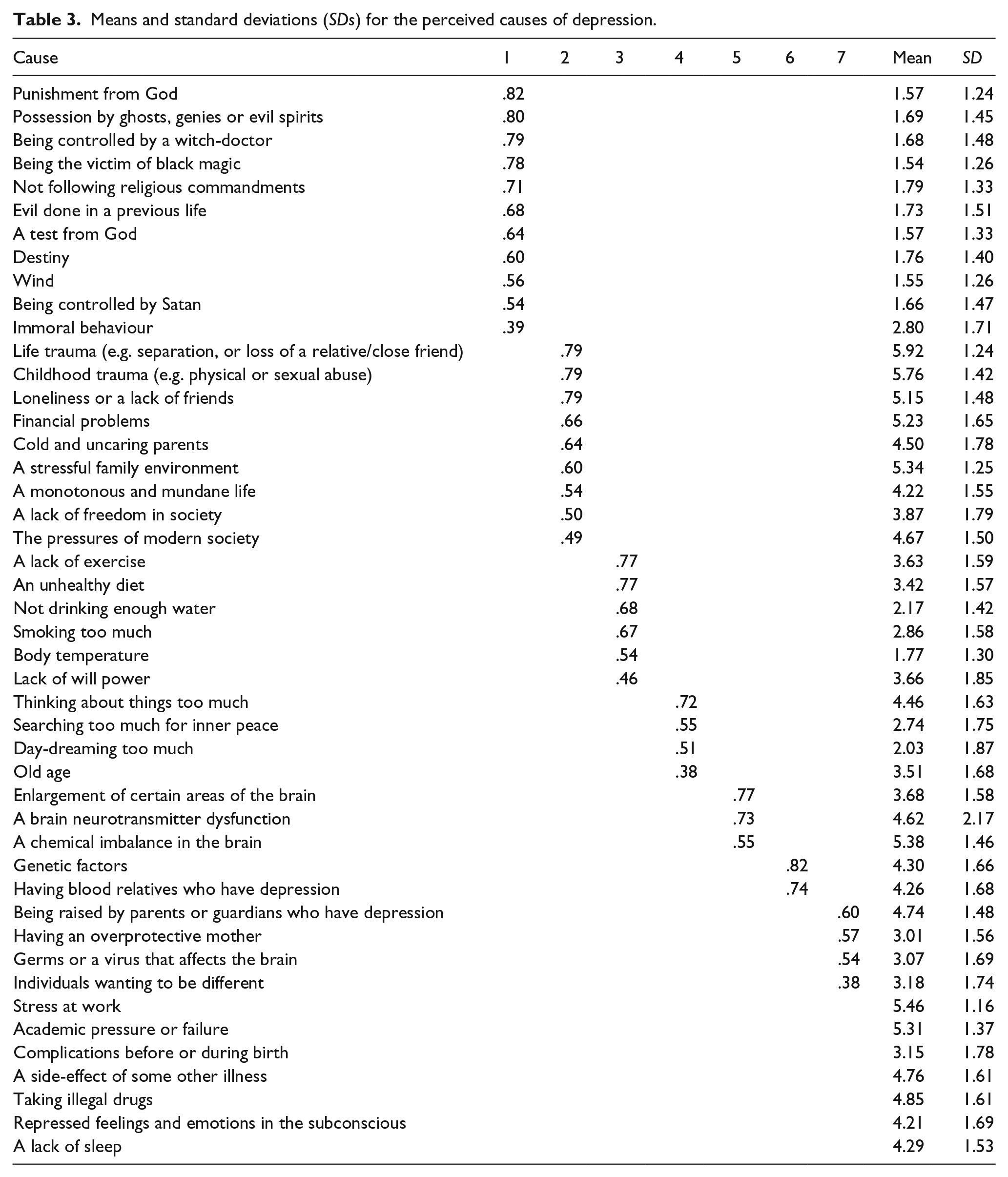
Table 3 shows the results of the Varimax-rotated factor analysis, as well as the means for each items. The seven factors accounted for 54% of the variance, respectively. The factors were clearly interpretable and similar to previous factor analyses. They were labelled God/Fate, Environmental, Health, Self-obsession, Brain, Genetics and Parents. It was apparent from the means that respondents thought the first factor (God/Fate) an unlikely cause of depression, while the second factor (Environmental) was the most likely cause.
Means and standard deviations (SDs) for the perceived causes of depression.
Following this, seven regressions were computed with the factor score as the criterion variable and sex, age, religious beliefs and political beliefs, media interest, experience of depression, diagnosed with another illness and know another diagnosed with depression as the predictor variables (see Table 4). It is apparent from Table 4 that while most of the regressions were significant, they accounted for very little of the variance. Furthermore, while some variables were not significant in any of the regressions (i.e. sex, personal diagnosis of depression, knowing others with depression), age was significant in three regressions and religion in two, rejecting H5. Two regressions accounted for around 10% of the variance. Age was a negative predictor and religiosity was a positive predictor of Environmental factor. Also, media interest was a positive predictor and diagnosed of other illnesses was a negative predictor of Genetic explanation for the causes of depression. However, personal experience of depression did not significantly predict any explanations, so not confirming H3. Age was negatively and religiosity was positively related to Brain explanations, while political belief was a negative predictor of God/Fate explanations.
Results for the regressions onto each factor for causes of depression.

p < .05; **p < .01; ***p < .001.
Cures for depression
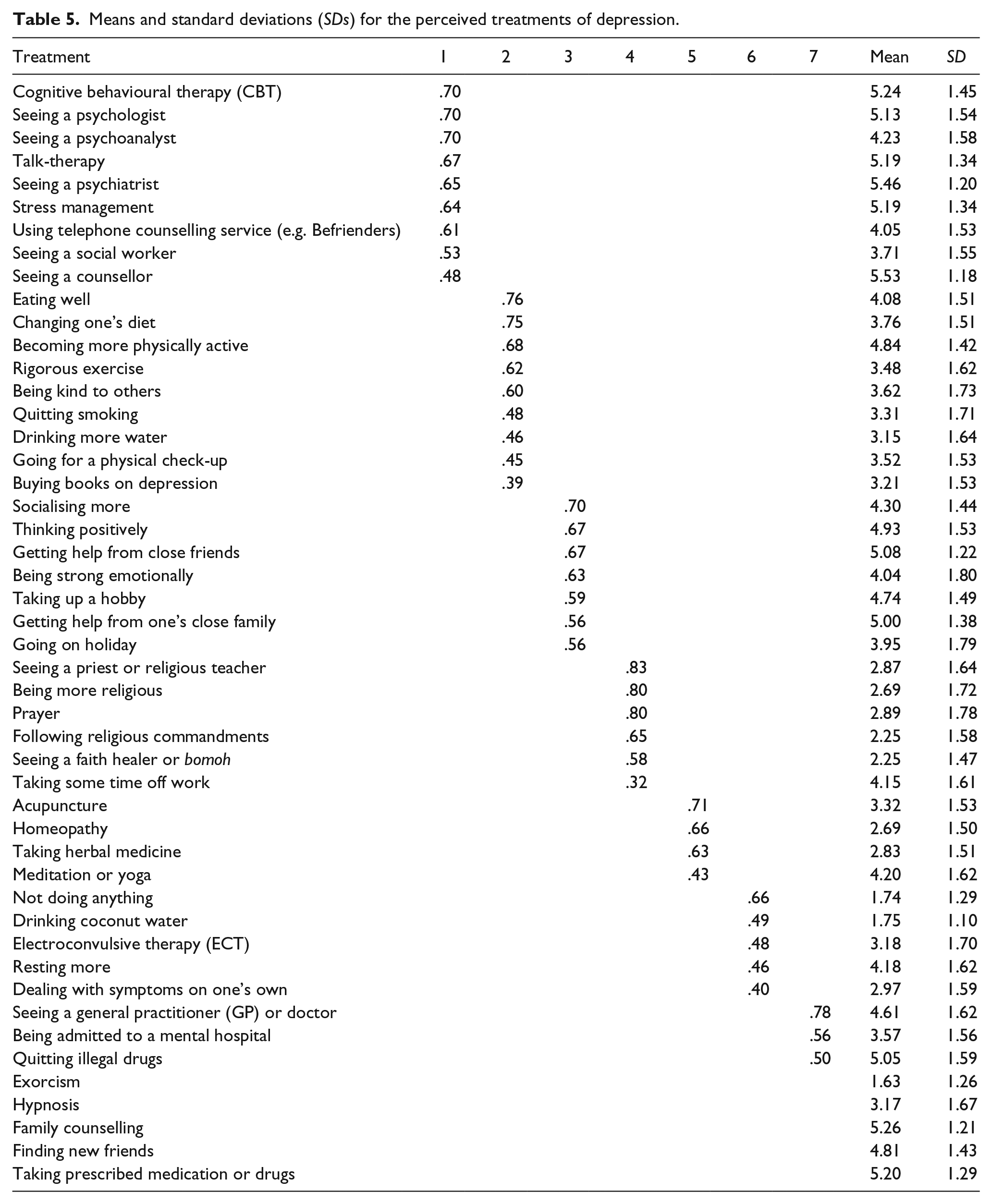
Table 5 shows the results of the Varimax-rotated factor analysis. The seven factors accounted for 52% of the variance and were labelled, respectively, as Talking Cure, Lifestyle Change, Social Support, Faith, Alternative Medicine, Self-help and Medical. It also shows the means and SD scores for each item. It is apparent from the means that respondents endorse Talking Cures as treatment, but not turning to religion. This confirms H2.
Means and standard deviations (SDs) for the perceived treatments of depression.
Following this seven regressions were computed with the factor score as the criterion variable and the same predictor variables as above (see Table 6). Five of the seven regressions were significant. The regression which accounted for most of the variance (26%) indicated religiosity was a positive predictor, while having been diagnosed with depression or any other mental illness was a negative predictor of Faith. The seventh factor (Medical) explained 22% of the variance, positively predicted by having known of others who have been diagnosed for depression and negatively by religiosity, supporting H6, but not H4. Following that, the regression for Lifestyle Change also accounted for 16% of the variance. Religiosity and frequency of consulting the media positively, while age negatively, predicted Lifestyle Change. Among the other significant regressions, we found that sex and having been diagnosed with depression were negative predictors, while frequency of consulting the media was a positive predictor of Talking Cure; age was a negative predictor and having known of others who have been diagnosed for depression was a positive predictor of Self-help.
Results for the regressions onto each factor for cures of depression.
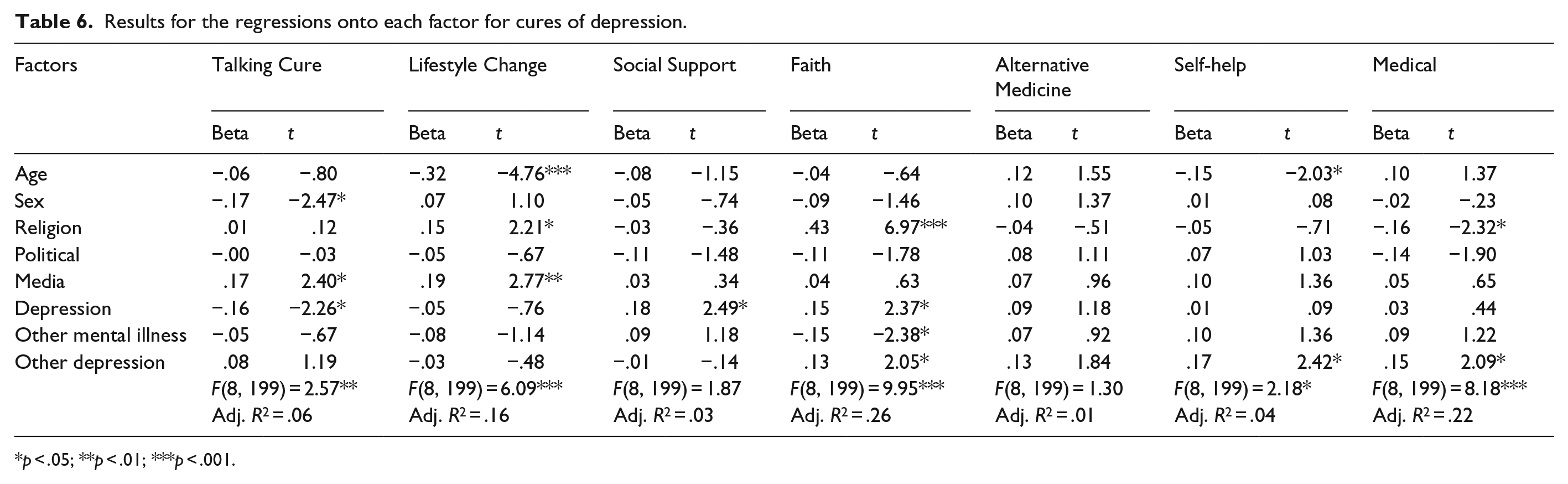
p < .05; **p < .01; ***p < .001.
Discussion
This study aimed to replicate the factor structure of a questionnaire assessing beliefs in causes and cures of depression (Loo & Furnham, 2012, 2013; Swami et al., 2010) in Great Britain. Furthermore, we set out to test six hypotheses, of which three (H1, H2 and H6) were supported. We also aimed to examine other correlates of MHL, namely, ideology and media consumption.
As predicted, over three-fourth of the group identified the characters in both vignettes as having depression. Furthermore, the hypothesised favoured cure as Talking Cures was also supported, as indicated by the low mean scores of items constituting this factor (see Table 5). These findings suggest higher MHL regarding depression in Great Britain, as compared to other countries like Malaysia (Loo & Furnham, 2012, 2013; Swami et al., 2010) and Australia (Jorm et al., 2005). Furthermore, the percentage of respondents in Great Britain identifying depression in the vignettes has also increased from 42% in Furnham, Daoud, and Swami (2009), in line with Swami (2012). This may, however, be a function of the unrepresentative sample.
Factor analyses revealed seven factors for both causes and cures of depression. Although the number of factors differed from previous research using the same measure (Loo & Furnham, 2012, 2013; Swami et al., 2010), the themes emerged were similar.
The regression analyses shed light into the high MHL concerning depression in Great Britain. Those who endorse the Environmental factor as a more important cause tended to be younger and more religious, whereas those who consulted the media more and had less personal experience of other mental illness favoured a Genetic explanation for the causes of depression. Those who endorsed factors related to the brain as causes of depression tended to be younger and more religious, while endorsing God/Fate as a cause was more likely among those who are more affiliated with right wing. However, the little variance explained by the regression models is a clear indication that there are other factors contributing towards different beliefs in the causes of depression.
For cures of depression, the factors explored accounted for more variance, indicating that these variables play substantial roles in constituting beliefs in depression cures. More religious individuals who were less likely to having been diagnosed with depression or any other mental illness tended to believe in religious practice as a source of cure. On the other hand, those who were less religious and more likely to having known others who have been diagnosed for depression were more inclined to perceive medical means as appropriate for treating depression.
The findings suggest that inexperience with mental health issues and high religiosity contribute largely to beliefs that depression can be cured via religious means, whereas low religiosity and exposure to depression through others are important factors leading to beliefs in medical treatment for depression. Younger, more religious respondents who more frequently consult the media tended to believe depression can be cured via a change in lifestyle. This could mean that the media may be depicting a change of lifestyle as an effective way of treating depression. Furthermore, this emphasises the significance of media in shaping and sustaining beliefs in cures of depression among the general population. Men who were less likely to having been diagnosed with depression and who frequently consult the media were more inclined to see Talking Cure as a cure for depression, while younger respondents who were more likely to having known someone with depression tended to see Self-help as a good way to treat depression.
One limitation of the study concerns the design of the questionnaire, particularly the design of the demographics section. The options given in the questionnaire, ‘European Caucasian’, ‘Asian’ or ‘Other’, were not able to give an accurate impression of the spread of ethnicity of the sample. As well as this, there was a large amount of missing data for this variable. Being able to define respondents by ethnicity would be beneficial, as it has been shown that different cultures have different levels of depression literacy and attitudes to mental illness (Hernandez & Organista, 2013; Wong, Xuesong, Poon, & Lam, 2012).
It would have been desirable to get a large representative sample as this may have been biased to younger better educated people. Furthermore, it would have been describable to compare the beliefs of this group with other health professionals, especially those dealing with mental health. Finally, it has been established that the MHL with respect to depression is considerably greater compared to other disorders, and it would be interesting to see whether the similar results would have occurred for other disorders such as anxiety and eating disorders as well as schizophrenia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.