
Abstract
Background:
Our study explores perceptions of the caregiver support for mental health service users (MHSUs) in a low- to middle-income country setting.
Materials:
We conducted in-depth individual interviews with 16 MHSUs and their treatment partners/caregivers from a treatment partner and text-message intervention study.
Discussion:
Treatment partners/caregivers felt obligated to care for MHSUs, but had a limited understanding of mental illness. They found supporting adherence to treatment difficult due to a number of factors including violence, food insecurity and substance abuse.
Conclusion:
Socioeconomic and environmental factors affecting the lives of MHSUs have impact on caregiver relationships with MHSUs in their care.
Introduction
Mental health services users (MHSUs) often require the assistance of caregivers, increasingly so with the shift of care from hospitals to families (Awad & Voruganti, 2008). Care may include assistance with basic functional tasks such as dressing, hygiene and adhering to their treatment regimen as well as more complex issues such as social inclusion (Dangdomyouth, Stern, Oumtanee, & Yunibhand, 2008; Mall et al., 2013).
Specific factors negatively impacting caregiving have been identified. Lam, Ng, Pan, and Young (2015) found that family caregivers for people with schizophrenia who adopted a more confrontational coping strategy had higher levels of psychological distress as a result of their efforts. These coping strategies entailed being more aggressive in accessing opportunities and community resources to support and inform their caregiving tasks. Poor coping resources and reduced levels of social support have been shown to result in increased caregiver burden (Magliano et al., 1998). Over time, the adoption of less emotion-focused coping strategies and improved social support has sustained and even reduced caregiver burden and can lead to improvement in MHSUs’ social functioning (Magliano et al., 2000).
There are few studies within the South African context exploring the factors impacting the roles of lay caregivers of MHSUs, from their own perspective. Food insecurity has been noted to increase risk of mental illness, with this increased risk being further exacerbated by high stress and social isolation (Martin, Maddocks, Chen, Gilman, & Colman, 2016). Individual factors such as substance abuse, smoking and physical inactivity, as well as social factors such as adverse childhood experiences, poor education, poor housing quality, unemployment and discrimination can exacerbate mental health conditions (Sederer, 2016). It is also well understood that the level of insight, cognitive issues, stigma, substance abuse, access to health care and socioeconomic factors contribute to non-adherence to antipsychotic treatment (Shuler, 2014). Kidman and Thurman (2014) noted that economic vulnerability and struggles with their own AIDS-related illness resulted in increased burden for caregivers of AIDS-orphaned children in rural South Africa. There are, however, few studies that explore the factors impacting an effective caregiving relationship from the perspective of MHSUs and their caregivers, particularly in the context of supporting adherence in our local setting.
Our research team has conducted a task-shifting pilot randomised controlled trial (RCT) at Valkenberg Hospital in Cape Town, South Africa, aimed at supporting adherence. This provided a unique opportunity to explore some of the factors mentioned above. As part of the intervention, MHSUs were assigned treatment partners to provide medication adherence support and local clinic visit adherence support. A psychoeducation and treatment partner contracting session was conducted with MHSUs and their treatment partners prior to discharge. Additionally, text message reminders of clinic appointments were sent to MHSU and treatment partners in the intervention group. MHSUs in the treatment-as-usual group received support from their caregivers as per normal practice and received no text message reminders. The specific findings of this investigation will be reported in an upcoming publication. We conducted a qualitative study exploring contextual issues before the RCT to aid in the design of an appropriate and acceptable intervention, and again after the completion of the intervention, which findings are discussed in this article.
In this article, we seek to explore the factors impacting caregiving, as experienced by both treatment partners who participated in our intervention and caregivers from the treatment-as-usual group. We also seek to elucidate the views of the MHSUs from both arms of the study on their experience of the support they received from their caregivers. The aim is not to compare the two groups but rather to develop an understanding of their caregiving experiences.
Methods
Population and sample
Our sample (n = 16) was purposively selected from the participants who took part in the intervention study described above. These were participants from both the intervention group, that is, those who had been allocated a treatment partner and received text message reminders, as well as participants from the treatment-as-usual group, who had neither been allocated a treatment partner, received a psychoeducation session nor received text message reminders. All participants in the study, regardless of the group they were allocated to, were invited back for a clinical and social review 3 months after discharge from the hospital, at the end of the intervention. In addition to this review, in-depth interviews with both MHSUs and treatment partners were conducted. Participants in the treatment-as-usual arm were accompanied by the caregivers who had been assisting them (see Figure 1). The interviews took place during July 2013. We matched the MHSUs recruited to their treatment partner or caregiver and interviewed them individually.

Study flow diagram.
Research site
The interviews were conducted at Valkenberg Hospital in Cape Town, a government tertiary psychiatric hospital that offers in- and out-patient psychiatric services.
Interview guide
The interview guide (see Appendix 1) was developed collaboratively by the research team taking into account the findings of our initial formative study (Mall et al., 2013). The interview guide consisted of open-ended questions, typical of qualitative research methods (Dicicco-Bloom & Crabtree, 2006). The questions probed the MHSUs’ knowledge and understanding of their diagnosis and medication regimen and explored their experiences at the clinics or day hospitals where they receive treatment after discharge from in-patient care. Interviews also explored the experience of having a caregiver or treatment partner (for the MHSU) and the experience of being a caregiver or treatment partner, as well as the delivery of the intervention. It was important to find out whether the text messages had been delivered, at what frequency and time of day, and whether the psychoeducation and contracting component had been helpful. The interviews lasted between 45 minutes and 1 hour. The interviews were conducted in English, Afrikaans or Xhosa as per the individual participant’s preference. The interviews for participants in the intervention group were conducted by one of the authors (S.M.), an experienced qualitative researcher not known to the MHSUs, while G.S., a junior research fellow in psychiatry, who had carried out the psychoeducation and treatment partner contracting intervention, conducted the interviews for the treatment-as-usual group. The interviews in Xhosa were conducted with the assistance of the hospital’s interpreter.
Data analysis
The interviews were transcribed by an independent transcription service in Cape Town. The data were then reviewed by G.S. and S.M. for codes and themes to gain familiarity with the data and develop a coding process. The interviews with treatment partner and the specific MHSU for whom they cared for were reviewed and analysed together (denoted by the number treatment partner 1 and MHSU 1 or 2, etc.). What followed was a framework analysis consisting of the following steps recommended by Ritchie and Spencer (1993): (1) identifying key themes that emerged from the data and developing a thematic framework or relationship between the themes, (2) charting (drawing further relationships between the different themes) and (3) mapping and interpretation (descriptions of the findings), particularly in relation to the usefulness of the intervention for people with severe mental illness. A qualitative analysis programme (NVivo 8) was used to manage and analyse the data.
Ethical issues
The study was granted ethical approval by the Human Ethics Committee of the University of Cape Town. Participants gave informed consent to participate in the study, were assured of confidentiality and were aware that they could stop the interview at any time should they feel uncomfortable. Assurance was provided that their health care would not be affected should they refuse participation or consent.
Results
Tables 1 and 2 present the demographic details of the MHSUs, treatment partners and caregivers in the study including their relationship to the MHSUs in their care.
MHSU participant characteristics.
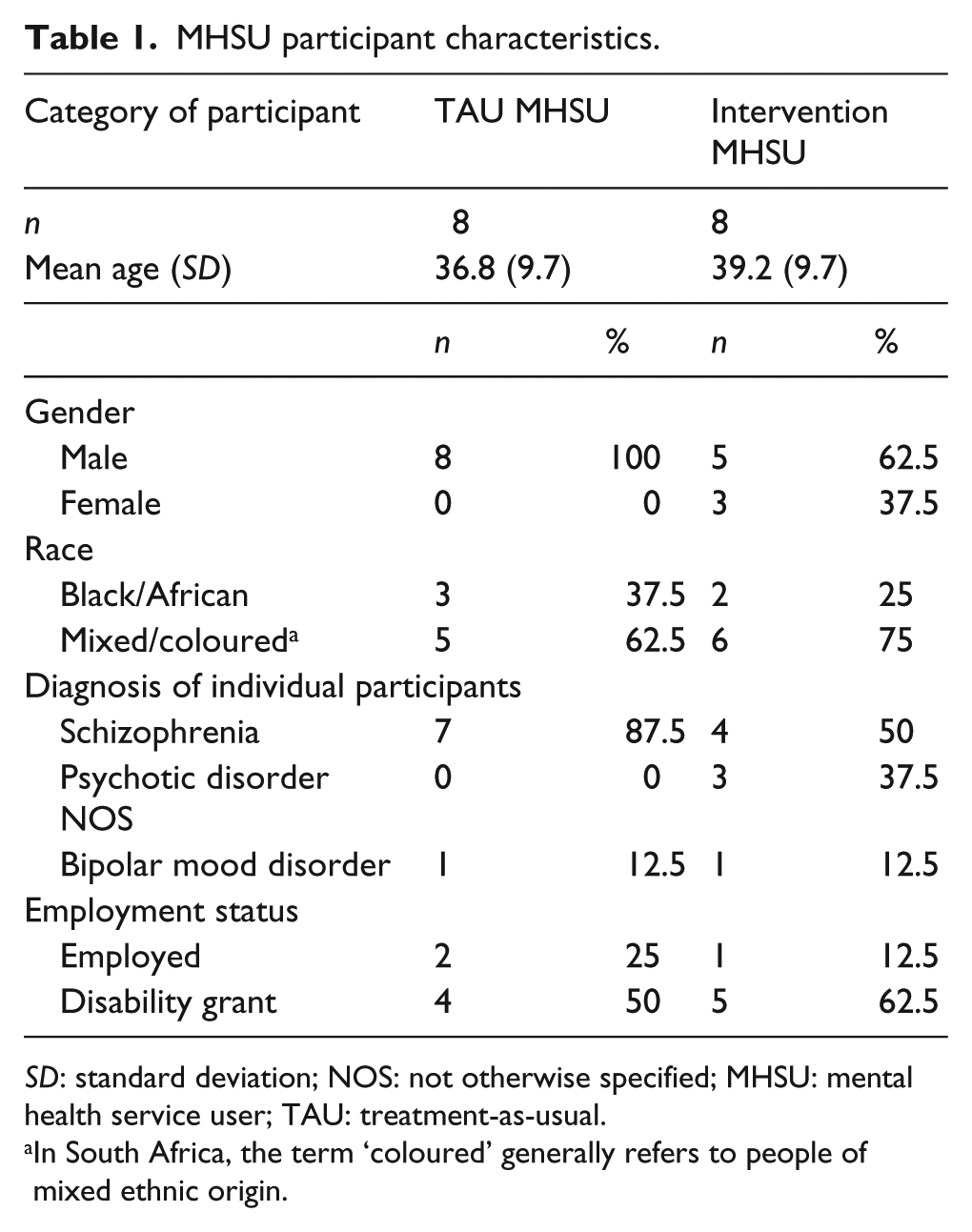
SD: standard deviation; NOS: not otherwise specified; MHSU: mental health service user; TAU: treatment-as-usual.
In South Africa, the term ‘coloured’ generally refers to people of mixed ethnic origin.
Caregiver and treatment partner characteristics.
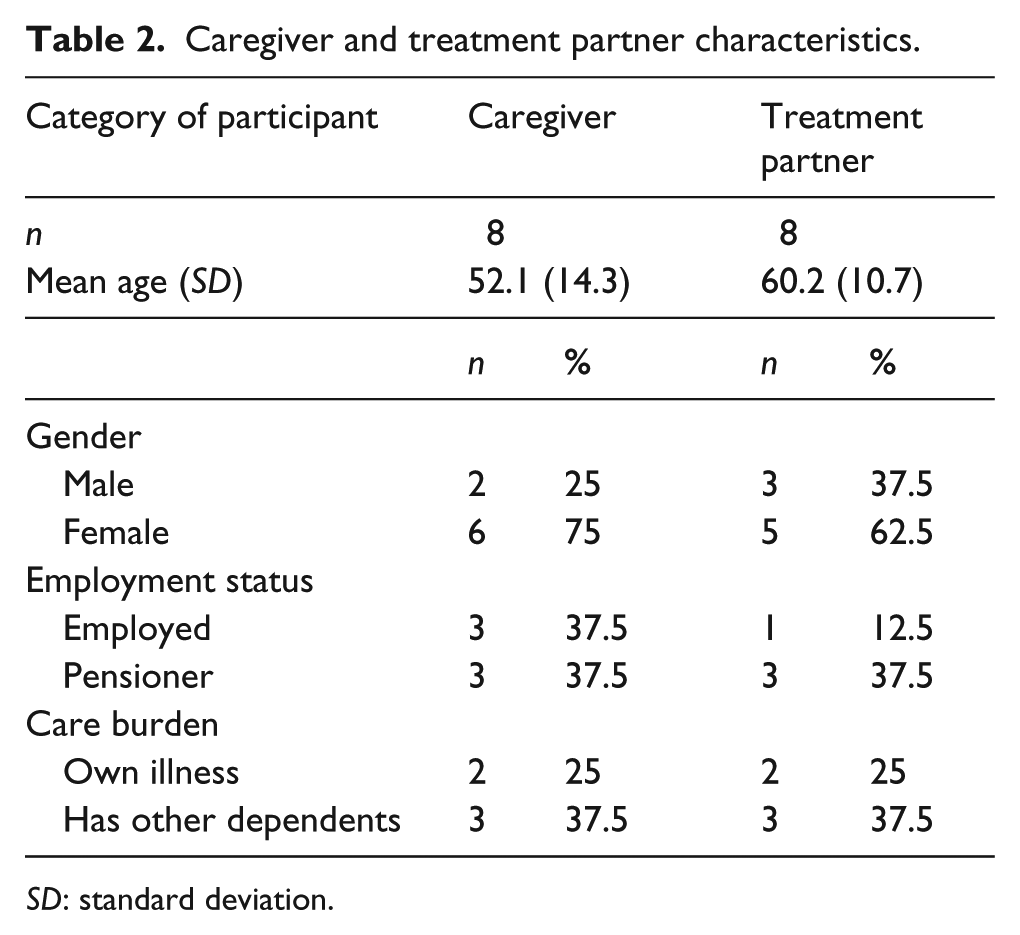
SD: standard deviation.
Several themes emerged from the data. We present the emergent themes: (1) reasons for assuming the caregiver role (for treatment-as-usual group) or agreeing to become a treatment partner (for intervention group), (2) participants’ perceptions of factors impacting caregiving and (3) participants’ perceptions of the intervention in relation to the experience of caregiving.
Reasons for assuming the caregiver role (for treatment-as-usual group) or agreeing to become a treatment partner (for intervention group)
Treatment partners from the intervention group and caregivers from the treatment-as-usual group expressed their reasons for agreeing to become a treatment partner. These included feeling an obligation to take responsibility for the MHSU in their care and concern about the MHSU’s treatment adherence. A mother from the treatment-as-usual group expanded on the challenges she faced as a result of her son’s poor interaction with neighbours due to poor adherence. She explained that as his mother she was forced to witness these incidents and cope,
he’s interfering with the people in the street and he’s sometimes swearing in the … there’s always a conflict on and I’m the mother, I must always be in the middle, … It’s sometimes very hard for me to cope with F because F sometimes get very out of hand, …, …, I don’t know did you see his reactions, he’s not himself because he’s not on treatment. But when he use his tablets then he’s calm, then I can go anywhere with him. (Caregiver 1)
One mother in the treatment-as-usual group reported that her religious convictions gave her strength to care for her son, as MHSU:
trying to help him sometimes you give him water and the tablets, you can see him, never drink the tablets, he put it in his pocket. it’s very hard to live with him, when he is very sick, because when we take him to Somerset and then take him, bring him here, he was breaking things … I think God gives me a strength, I’m just trying, it’s very hard to live with him and he was sick since 1998, it’s a long time, but by that time the father was alive, then his father passed away on 2002 … (Caregiver 2)
A treatment partner who was a friend of the MHSU she had agreed to care for explained that there was no one else who would agree to fulfil role of treatment partner. She therefore felt obligated to agree to act as treatment partner for this MHSU:
Even though I knew that I wouldn’t be able to do all the things that a partner should do, I just said yes I would be her partner because I knew there was no-one else … (Treatment partner 1)
She also reported that the most self-fulfilling aspect of being a treatment partner was to be there for the MHSU in her care.
A brother of an MHSU who accepted the invitation to become treatment partner explained,
actually, I was shocked when my mother told me (I was chosen to be treatment partner). So I didn’t actually know what it was about then the doctor explained so I thought okay, he’s (my brother) choosing me, he never chose my mommy or my daddy or anybody, he chose me, so I must take the responsibility now, try and help him … (Treatment partner 2)
A caregiver from the treatment-as-usual group explained that as the eldest sibling, he was obligated to care for his brother:
I am the eldest so they all depended on me you know. (Caregiver 3)
Two mothers caring for their sons with severe mental illness described aspects of the role of treatment partners. One explained that she saw the treatment partner’s role as helping the MHSUs grow and not be constrained by their disability:
I can move forward, my disability mustn’t (hold) me back in life, it must give me that push in life and say, I can do more, I can do more. This is what I’m saying, if there’s anybody needing help, get a partner and that partner must be positive … (Treatment partner 4)
The other mother spoke of the importance of patience when caring for a family member with severe mental illness:
you must have patience and show him you love him and everything and as a family you sit together and we talk to each other and make each other happy you see and maybe that’s what he was looking for all the time and I didn’t realise it … (Treatment partner 5)
Factors impacting caregiving
Both MHSUs and treatment partners from the intervention group described their perceptions of factors impacting their role as treatment partner or caregiver or of relating to a treatment partner or caregiver (in the case of MHSU) and broader issues of adherence.
Food insecurity and substance abuse patterns in households affect adherence behaviour. Participants found it challenging to care for MHSUs who were aggressive. One mother reported that she was worried her son would be at risk of the negative influence of peers involved in gangsterism:
I feel that it is quite strong, the medication’s quite strong and I didn’t, at home there’s not enough food to eat to balance out, to support the strength of the tablets with the food and, but I took my injection regularly, it’s also the complex injection, a substantial amount of food to support the strength of the tablets, you understand there’s not enough finances at home … (MHSU 3) this morning there wasn’t anything to eat, you see, so I couldn’t give him his pill, but I gave a little bit, just a bit, because he couldn’t have a whole one because we didn’t eat … (Treatment partner 6) it’s his friends [who are involved in gangsterism] that give (TIK – Methamphetamine) A’s using this TIK now, he was in a terrible state he was like getting aggressive with the people and banging this, knocking the, kicking this man’s car and the man came to complain, A started to grab me one very early morning … he pushed me and he pressed me in the wardrobe, I didn’t scream, I didn’t panic. (Treatment partner 3)
Another MHSU reported that he was not in contact with his mother or brother who was initially appointed as a treatment partner. He instead depended on his landlady to remind him to take his medication. He felt that this relationship was working quite well:
I stay there, I pay my board, I pay my rent, I get my food everything …
and she reminds you to take your medication?
yes … (MHSU 4)
One caregiver from the treatment-as-usual group, a sister of the MHSU in her care, reported that she did not understand the manifestations of schizophrenia well. This was despite having attended several appointments with her brother at Valkenberg Hospital. She reported that she is suffering from depression at the same time while caring for her brother. She saw this as a barrier to her caregiving ability:
I think I still need to know more information about what is the meaning of the words and the meaning of schizophrenic you know, but another thing you know, my mother, she also had a nervous breakdown when we were very young and I think it’s something hereditary or something I don’t know, because I’m also suffering from a major depression disorder … (Caregiver 3)
Other participants in the treatment-as-usual group also reflected that they had a poor understanding of their illness:
‘do you know what your diagnosis is?’
‘they didn’t tell me’.
‘so you’re not sure what your diagnosis is?’
‘they just said it was drugs related’. (MHSU 5)
‘what do you think made you sick?’
‘the fact that I’m not working or doing anything …’
‘and anything else?’
‘nothing’. (MHSU 6)
In reality, treatment partners and caregivers change. One participant who had agreed to act as treatment partner for his brother had moved from his family’s home. He explained that his mother was now fulfilling the role of treatment partner:
I’m not actually there anymore so my mother’s looking after him during the day, so my mother told me a few days ago he didn’t want to take it (medication), he never went to fetch it at the clinic … (Treatment partner 2)
Treatment partners had busy schedules, which included caring for themselves as well as other dependents:
because every morning I take my medication then he takes his, he had to take his medication, coz my son also takes medication, that is bed ridden and I myself take my medication … (Treatment partner 7)
Another treatment partner explained that as the area where her friend lived was violent, she found it difficult to visit the MHSU. She further explained that as the MHSU was residing with her mother, she (the treatment partner) would communicate with the mother about the MHSU’s treatment regimen and progress:
I don’t ever go into that area … there’s too much in the newspapers and a family member of ours was recently shot there, so I don’t ever go into that area. We (the mother and I) talk about P, I always ask how she is now and then her mom will tell me … she was at the place she gets her pills … (Treatment partner 1)
Another treatment partner, a mother who had agreed to fulfil this role for her son explained that her son’s methamphetamine addiction affected his adherence to his medication. This posed a challenge for her, in fulfilling her role as caregiver:
(he) went for this TIK (methamphetamine), now he’s uncontrollable, he stole to sell for drugs. I said did you take (your medication) already, as soon as you’ve finished your breakfast you must take it, he said no, no, I’m going to take it and I, as time went then he doesn’t take his medication. He went for TIK now, now he’s so, so, in a terrible, terrible state. (Treatment partner 3)
Participants’ perceptions of their role as treatment partner or caregiver
Participants from the intervention group described their daily functions as treatment partners. This ranged from individually focused to family adherence programmes:
my mother gives him the tablets and they (the other family members) watch him (take their medication) … (Treatment partner 2)
Two mothers, appointed as treatment partners described family adherence efforts where two or more members including the MHSU take their medication together:
every morning I take my medication then he takes his, he had to take his medication, coz my son also takes medication, that is bed ridden and I myself take my medication … (Treatment partner 3) I’d say it’s been a good help for me, it makes me realise I also have to take my tablets (for arthritis and hypertension) … (Treatment partner 5)
An MHSU from the intervention group explained that his mother had been originally appointed as treatment partner but had to work long hours. His sister would then take over from her as treatment partner. In his view, this arrangement appeared to be working quite well:
she’s working, every day then she will phone my sister and at night if she’s working overtime … she would also phone or she would be at home then she would take the tablets out and after supper then give it to me. My sister also helped … (MHSU 5)
He further explained that he would like a treatment partner to explain more about the side effects of the medication:
(I would like more information) about the (side) effects. I now sometimes I want to take more of that yellow tablets … they will tell me – no, don’t do that, they would always be there for me and they would talk to me, talk sense into me sometimes when I don’t want to take the medications so, so they’re very helpful to me … (MHSU 5)
Participants were asked whether they had found the treatment partner contracting and psychoeducation session useful.
One treatment partner indicated that better mental health knowledge was helpful but could still be further reinforced:
I have more information about this sicknesses and I think it would be more helpful for me to know this is how I am supposed to treat him. I shouldn’t treat him otherwise as I’m treating him, but it would have been better for me to know that this is T’s situation and is there something that I can do to change it or whatever … (Treatment partner 8)
She also explained that it was useful to become a treatment partner:
well I want to move forward, there’s more things in life that I can achieve. You see and that makes it helpful for them, if you, the partner is positive, it mustn’t be negative about things going around, whether he’s sick or whatever, but you must be positive of helping that person and say to that person, look here man, you don’t have to stay here, there’s more things in life that you can achieve …
Discussion
Our main findings were that (1) treatment partners and caregivers, who are often family members, feel obligated to care for MHSU, but may also derive fulfilment from the caregiving relationship; (2) caregivers’ and treatment partners’ understanding of mental illness is limited; (3) treatment partners find it difficult to negotiate harsh environments where there are several factors, including substance abuse and violence, which increase the risk of poor adherence and readmission to hospital; and that (4) treatment partners’ circumstances may change, for example, having to move out of the home where their MHSU resides for employment opportunities, impacting their direct availability to provide support.
Treatment partners and caregivers feel obligated to care for MHSU, who can be dependent on their treatment partners/caregivers to remind them to take their medication (Kittay, Jennings, & Wasunna, 2005). In our previous study, we found that family members were available treatment partners as they lived in the same residence as the MHSU in their care (Mall et al., 2013). This finding also emerged in a study conducted by Asmal, Mall, Emsley, Chiliza, and Swartz (2013) in another hospital in Cape Town, where the investigators sought to investigate the feasibility of family therapy for schizophrenia through a qualitative design. They additionally noted that family members expressed a desire to protect the MHSU in their care from stigma and abuse, a theme echoed by Browne and Hemsley (2010) in their exploration caregivers’ views on housing and living with a mental illness. Improved holistic interventions for MHSU which include protective, supportive structures for community and caregivers can go a long way towards easing the burden on caregivers (Awad & Voruganti, 2008). A positive caregiving experience proved to reinforce the role for the caregiver, while supportive community structures such as the church emerged as a supportive resource. This has been noted in other research where, in addition, supportive family relationships were shown to add to caregiver satisfaction, as was structural health system support (Kartalova-O’Doherty & Tedstone Doherty, 2009).
Poor levels of mental health knowledge emerged as a concern for our participants. While some experienced the psychoeducation component of the main study positively, there remained a clear need for reinforcement. Sin et al. also found the impact of psychoeducation inconclusive, while Gutiérrez-Maldonado found family psychoeducational intervention reduced burden in caregivers of MHSUs with schizophrenia (Gutiérrez-Maldonado & Caqueo-Urízar, 2007; Sin, Jordan, Barley, Henderson, & Norman, 2015). Yesufu-Udechuku et al. (2015) found that the impact of psychoeducation on psychological distress was delayed and was not appreciable immediately postintervention. This suggests that much still needs to be done to ascertain the most effective approach to deliver appropriate and useful psychoeducation for the caregivers of MHSU.
Previous research has suggested that caregivers may have to negotiate harsh environments in the course of caregiving. Caregivers and treatment partners in our study had to contend with a high burden of care, as well as environments ridden with violence, substance abuse and food insecurity. It has been suggested that caregivers may view MHSU with a history of violence in a negative light, especially where violence was directed towards the caregiver (Onwumere et al., 2014). The result maybe be low self-esteem among caregivers. Prior research have indicated that lay health workers working with MHSUs with extreme social difficulties or alcohol-related problems had particular difficulty where interventions seemed unable to address their specific needs, while these factors have been correlated with increased emotional distress and burden among caregivers (Pereira, Andrew, Pednekar, Kirkwood, & Patel, 2011; Vaddadi, Gilleard, & Fryer, 2002). The increased burden placed by substance use on family relationships has the impact of reducing the amount of support they give, while there is a suggestion that, in fact, direct family support may help reduce or eliminate substance use in people with mental illness (Clark, 2001; Clark & Drake, 1994). Yesufu-Udechuku et al. (2015) also noted that support interventions and problem solving had a sustained beneficial effect.
Socioeconomic factors have a clear impact on the caregiving relationship. Caregivers sometimes need to relocate to areas where employment might be more easily obtained. This, in addition to factors around their own mental illness, and burden of other responsibilities, directly impacts their availability to provide support to the MHSUs (Ae-Ngibise, Doku, Asante, & Owusu-Agyei, 2015). The issue of food insecurity also emerged from the MHSUs who found it challenging to adhere to their medication when they experienced chronic hunger. Kartalova-O’Doherty and Tedstone Doherty (2009) found that carers with a higher socioeconomic status experienced more satisfaction in their caregiving role.
A number of limitations to the study deserve emphasis. This component was not designed as an interventional study where we could compare the experimental and treatment-as-usual groups. The study was designed as a qualitative study to explore multiple perspectives of how these participants experience care and participation in the intervention. We are therefore unable to comment on whether the intervention resulted in a different experience of factors impacting caregiving for those in the intervention group versus those in the control group. The sampling was purposive rather than representative. We had to use an interpreter for our Xhosa-speaking participants which may have biased the results. Psychiatric hospitals in South Africa, however, tend to depend on the use of interpreters to gain perspectives of care from multilingual MHSU (Kilian, Swartz, & Joska, 2010).
Nevertheless, this study has helped highlight some of the important considerations for adherence-focused interventions designed around caregiving. Obligation to provide care and total care burden may contribute to mental health caregiver burden and availability to provide care, thus negatively impacting the caregiving role, along with MHSU factors such as aggression and limited insight. Further contributors may be socioeconomic issues such as food insecurity, environmental issues such as violence, substance abuse and peer pressure. Factors enabling caregiving could include caregiver resilience, accessed available support and knowledge of mental illness. Psychoeducation is yet to show sustained outcomes for MHSU as well as caregiver. Further work is required in exploring how best these interventions can be tailored to the needs and circumstances of MHSU and caregivers especially in environments where caregiving can be significantly compromised by these factors.
Footnotes
Appendix
Interview guide.

| Interview Guide | |
| Steps |
|
|
|
|
| Can you tell me about your diagnosis | |
| What do you think has made you sick? | |
| What medication are you on? | |
| Have you been taking your medication regularly? | |
| If yes, what has helped you with taking your medication? | |
| If no, what has stopped you from taking your medication? (Probe for side-effects and social stressors) | |
| I’d like to ask you a few questions about your discharge from Valkenberg Hospital 3 months ago. | |
|
|
|
| What information were you given about your diagnosis before leaving the hospital? | |
| What information were you given about the clinic visits following your discharge? | |
|
|
|
| Were the sms reminders helpful with remembering to attend the follow up appointments at the clinic? | |
| Were they sent often enough? | |
| Should it be more often? | |
| Should it be less often? | |
| What is the best time of the day to receive an sms notification? | |
| Let’s discuss the session when your treatment partner came to the hospital for a meeting with the doctor (investigator) before you were discharged | |
| What information did you get about your diagnosis? | |
| What information did you get about your treatment? | |
|
|
|
| What information did you get about your follow up after discharge? | |
| Was having a treatment partner helpful with taking medication? | |
| If so, how? | |
| If not, why not? | |
| In what ways could the treatment partner support you better? | |
|
|
|
| I’d like to ask you a few questions about your experience at the clinic/day hospital. | |
| Is the clinic easy to get to? | |
| Do you know where to go when you arrive at the clinic? | |
| How long did you wait when you arrived for your appointment? | |
| Was this waiting time acceptable? | |
| Let’s talk about your interaction with your clinic staff. | |
| Were they easy to talk to? (interviewer can probe further about the attitudes of the staff) | |
| Was the correct medication available for you at your appointment? | |
| If there was a problem with availability was the problem solved to your satisfaction? | |
| Is there anything else that you would like to tell me about your clinic visits? | |
|
|
|
| Is there anything else you would like to tell me, which was not covered in the questions above? | |
|
|
|
|
|
|
| I would like to ask a few questions about how the patient took his treatment and attended clinic reviews | |
| Has the patient been taking his treatment regularly? | |
| Has the patient been attending clinic review appointments regularly? | |
| What has helped him/her to continue to take their treatment and attend clinic reviews? | |
| What has prevented him/her from taking their treatment and attending clinic reviews? | |
| Was the clinic helpful? | |
| Can you tell me more about that? | |
| How can visiting the clinic be made a better experience? | |
|
|
|
| I would now like to ask you a few questions about the specific areas we looked at in our investigation/study | |
|
|
|
| How often did you receive the sms notifications? | |
| Were they clear and easy to understand? | |
| At what time of day did they arrive? | |
| Is this an acceptable time? | |
| Were they helpful? How so? | |
|
|
|
| Were they sent often enough? | |
| Should they be sent less often or more often? | |
| Has being part of this intervention changed things for you and the patient? How? | |
|
|
|
| Let’s discuss the session when you came to the hospital for a meeting with the doctor (investigator) before the patient was discharged | |
| What information did you get about the patient’s diagnosis? | |
| What information did you get about the patient’s treatment? | |
| What information did you get about the follow up after discharge? | |
| Was this session helpful? In what way? | |
| In what way can a session like that be improved? | |
|
|
|
| What has it been like to be the patient’s treatment partner? | |
| Which parts of it were good? | |
| Which parts of it were difficult? | |
| How did you make contact with the patient? | |
| How often did you make contact with the patient | |
| What helped you in your role as a treatment partner | |
| What could have helped you be a better treatment partner? | |
|
|
|
| What was more helpful in reminding the patient to take his treatment and attend clinic appointments? The sms notifications, the psycho education session with the doctor or having a treatment partner? (Probe the carer to rank in order of impact) | |
| Is an intervention of this sort a good idea? | |
|
|
|
Conflict of interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: G.S. is supported by PhD Scholarship from the South African Medical Research Council. P.M. is the Head of Clinical Services at Valkenberg Hospital in Cape Town under joint appointment by University of Cape Town and the Provincial Government of the Western Cape in South Africa. D.J.S. has received research grants and/or consultancy honoraria from AMBRF, Biocodex, Cipla, Lundbeck, National Responsible Gambling Foundation, Novartis, Servier and Sun. He is supported by the South African Medical Research Council. H.T. is a consultant psychiatrist working in the acute admission unit at Valkenberg Hospital and is jointly appointed by the University of Cape Town and the Provincial Government of the Western Cape. H.T. has received a speaker’s honorarium from Pharma Dynamics. S.M. is supported by a Harry Crossley postdoctoral research fellowship. C.L. is supported by the PRogramme for Improving Mental health carE (PRIME), funded by the Department for International Development (United Kingdom). The views expressed in the article do not reflect the views of the funders, the South African Medical Research Council (SAMRC) or University of Cape Town (UCT).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.