
Abstract
Background:
Knowledge about subjective perceptions and explanatory models has the potential to inform clinical evaluation and lead to development of patient-friendly treatment models in medically unexplained physical symptoms (MUPS).
Aim:
To collect qualitative data about explanatory models in MUPS.
Methods:
A cross-sectional observational study was done among patients with MUPS presenting over a 2-year period to a specialty psychosomatic clinic. The Short Explanatory Model of Illness interview was used to gather qualitative data about explanatory models which were subsequently recoded using standard manuals.
Results:
A total of 123 subjects were evaluated. The nature of symptoms was most commonly reported as ‘non-specific’ (n = 102, 82.9%) but of moderate to severe intensity (n = 87, 73.8%). Getting cured or showing improvement was the most common expectation from treatment (n = 58, 47.9%). Moderate to severe impact of symptoms was reported on work output (n = 100, 84%), emotional life (n = 85, 71.4%) and physical mobility (n = 59, 49.1%). A considerable proportion was either dissatisfied (n = 61, 50%) or frankly unhappy (n = 38, 31.4%) with treatment received.
Conclusion:
There is a need to re-calibrate the clinical approach to people with MUPS to enhance treatment satisfaction. Our findings could assist in evolving culturally sensitive conceptualizations of illness and in developing patient-centred models for therapy in MUPS patients.
Keywords
Introduction
Somatic symptoms, without adequate medical explanation, constitute a significant percentage of cases seen in both primary and specialist care settings (Burton, 2003; Kroenke, 2003; Reid, Wessely, Crayford, & Hotopf, 2001). These cases, referred to as medically unexplained physical symptoms (MUPS) often turn chronic, lead to significant disability and poor quality of life and are associated with disproportionately higher consumption of limited health care resources (Barsky, Orav, & Bates, 2005; Edwards, Stern, Clarke, Ivbijaro, & Kasney, 2010; Gureje, Simon, Ustun, & Goldberg, 1997; Hiller, Fichter, & Rief, 2003). The existing system of psychiatric classification and treatment has largely failed to provide satisfactory results in managing them adequately (Kroenke et al., 1997; Mayou, Kirmayer, Simon, Kroenke, & Sharpe, 2005). Partly, the problem lies in the inability of the conventional classificatory systems to capture many of these individuals, especially those who do not have co-morbid mood or anxiety disorders but nonetheless experience significant distress and burden (Dimsdale, Patel, Xin, & Kleinman, 2007; Smith et al., 2005).
Another major limitation in managing this condition is the lack of consonance between the patient’s underlying belief about the symptoms (such as their nature and origins) and the explanations offered by the biomedical model (Butler, Evans, Greaves, & Simpson, 2004; Simon, Gater, Kisely, & Piccinelli, 1996). This may be a reason for the high perceived levels of dissatisfaction with services among patients with MUPS (Dirkzwager & Verhaak, 2007). Evidence suggests that this lack of satisfaction is mutual with physicians experiencing frustration and a sense of powerlessness when patients come back repeatedly with inadequate improvement (Mathers, Jones, & Hannay, 1995). Though it may seem counterintuitive, studies have shown that many patients with MUPS less frequently request somatic interventions than many physicians may offer (Ring, Dowrick, Humphris, & Salmon, 2004). On the other hand, what a sizeable proportion of them desire and may benefit from is emotional support and a culturally acceptable and convincing explanation for their symptoms (Peters, Stanley, Rose, & Salmon, 1998; Salmon, Ring, Dowrick, & Humphris, 2005). The common sense model, proposed by Diefenbach and Leventhal (1996), is one such alternative model that also incorporates explanatory models in its treatment paradigms.
Explanatory models, as defined by Arthur Kleinman (1980), refer to ‘notions about an episode of sickness and its treatment that are employed by all those engaged in the clinical process’. In other words, it represents the individual’s internal representation about the happenings in his/her body when he/she is experiencing physical or psychological symptoms. Explanatory models are known to correlate with the decision to seek consultation, continuation of symptoms and incurred disability (Kessler, Lloyd, Lewis, & Gray, 1999; Sensky, MacLeod, & Rigby, 1996). These may have many distinct but related dimensions such as the illness label, presumed aetiology, feared consequences and perceived dysfunction among others (Haidet et al., 2008; Horne, 1997; Leventhal, Diefenbach, & Leventhal, 1992; Mayou, 1991). Knowing the culturally prevalent explanatory models will assist clinicians in formulating coherent and convincing theoretical frameworks for physical complaints. This information can also be used to articulate the treatment rationale as well as for specific therapeutic techniques used in MUPS treatment such as reattribution and cognitive-behaviour therapy. It will help in transforming these psychological interventions into those of a more patient-friendly nature and potentially improve retention rates. To date, however, limited information is available from the Indian setting on explanatory models in MUPS.
Hence, we carried out the present research with the objective of collecting qualitative data about explanatory models among subjects with MUPS. The qualitative data collected were recoded using standard manuals for easier interpretation and analysis. Through this, we aimed at eliciting patient perceptions and understanding about the nature and impact of their symptoms.
Methods
Setting and design
This was a cross-sectional exploratory study carried out at the psychiatry outpatient department of a teaching cum tertiary care hospital in South India for 2 years (January 2014–December 2015). The hospital, which is attached to a centrally funded autonomous university, is located in an urban area of the Union Territory of Puducherry, but also caters to patients from neighbouring districts of the state of Tamil Nadu. It has all the specialty and super specialty departments functioning within a single campus. Most of the service users are patients who directly walk-in, prepare a case file and seek desired services. About 30% of patients constitute referral cases from nearby as well as faraway centres. All cases presenting to the psychiatry outpatient department are first evaluated by a senior resident (qualified psychiatrist equivalent to a registrar) for psychiatric morbidity. Those who are deemed to satisfy case definitions for MUPS are given an appointment for detailed evaluation in the weekly specialty psychosomatic clinic within the outpatient premises of the department of psychiatry. The patients are asked to come with a reliable informant on the day of appointment and a detailed evaluation of symptoms is performed by a junior resident (psychiatrist-in-training), following which the case is discussed with the consultant psychiatrist in-charge of the clinic (V.M.) and a detailed diagnosis and management plan is formulated. All psychiatric diagnoses are made in accordance with International Classification of Diseases-10 (ICD-10) (World Health Organization, 1992).
The specialty psychosomatic clinic was primarily started by the Department of Psychiatry to cater to the special needs of people with MUPS. The team manning the clinic comprises of a consultant psychiatrist, a senior resident qualified psychiatrist, a junior resident (psychiatrist-in-training) as well as a dedicated social worker. The management comprises of both pharmacological and a broad array of psychosocial strategies depending on the nature and relevance for individual clients. Further information on the scope and workflow of the clinic is detailed elsewhere (Menon, Sarkar, & Thomas, 2016).
Subjects and methods
For this study, subjects were included if they had single/multiple physical symptoms for at least 3 months duration and basic/ordered investigations within normal limits following which the symptoms are deemed to be medically unexplained by the treating physician. The patients had to have referral letters from their physicians stating explicitly the medically unexplained nature of their symptoms. We excluded patients not having proper referral letters as well as those above the age of 65 in order to avoid including spurious cases. We also excluded patients who presented with psychotic symptoms as well as those with intellectual/language or hearing impairment and pregnant women or those who have delivered in the last 1 year. Consecutive patients satisfying the above inclusion and exclusion criteria were prospectively recruited for the research. A total of 154 patients were screened during this period out of which 123 were found to satisfy inclusion and exclusion criteria and their data are reported here. The reasons for excluding others are mentioned in Figure 1.
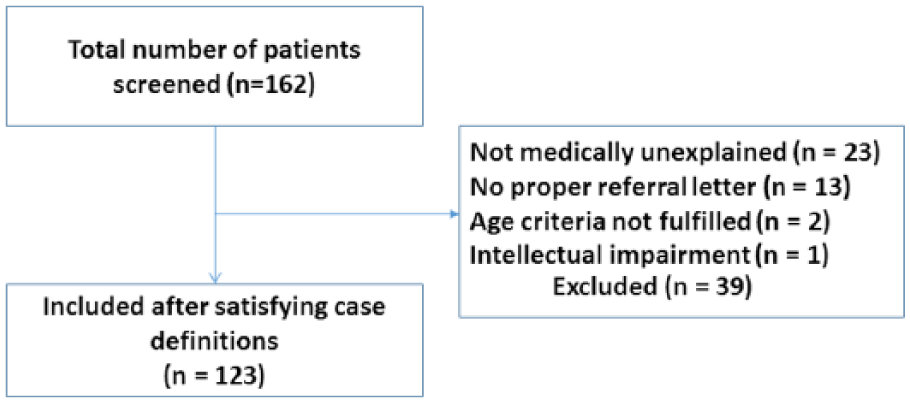
Screening and inclusion of cases.
Ethical approval
Prior approval to carry out this research was obtained from the Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER) Scientific Advisory Committee and Institutional Human Ethics Committee of JIPMER, Puducherry. Study procedures were explained in the local language and written informed consent was obtained from all the consenting participants.
Assessments
Recruited patients were assessed cross-sectionally on the Short Explanatory Model of Illness (SEMI) interview, version 3.1 (Lloyd et al., 1998): this is a short interview with multiple sections designed to elicit various dimensions of explanatory models related to assumptions, beliefs and causes of symptoms, fear of consequences, perceived dysfunction and satisfaction with services received. As these sections are standalone, it allows for flexibility in administration by the interviewer. The interviews on an average took about 20 minutes each. It has been previously used in research on MUPS (Sumathipala et al., 2008). A trained resident administered the interview and responses were recorded verbatim. Inter-rater comparability of responses was checked by another psychiatrist (B.S.) who carried out the same interview with 15 randomly selected patients. Subsequently, two psychiatrists (A.B.A. and J.S.T.) independently coded these verbatim responses at regular intervals during the period of study and these were compared. Any disagreements were sorted out through mutual discussion and consensus. Recoding was done using the original coding manual in order to convert verbatim responses into meaningful categories.
Data analysis
Descriptive analysis was primarily carried out for this study. Mean, standard deviation, frequencies and percentages were used for representing the data. The responses on SEMI items were categorized and frequencies of those categories were represented. Missing value imputation was not done and the percentages were drawn from the denominator of those subjects which provided at least some responses. Inferential statistics were not used for assessing the relationship between demographic and clinical characteristics and the responses on SEMI.
Results
The mean age of the sample was 37.3 (±10.0) years, with a range of 14 to 60 years. The demographic characteristics of the sample are shown in Table 1. Just more than half of the sample comprised of females. The sample was largely married, educated up to 10th grade and belonged to Hindu nuclear families.
Demographic characteristics of the sample.
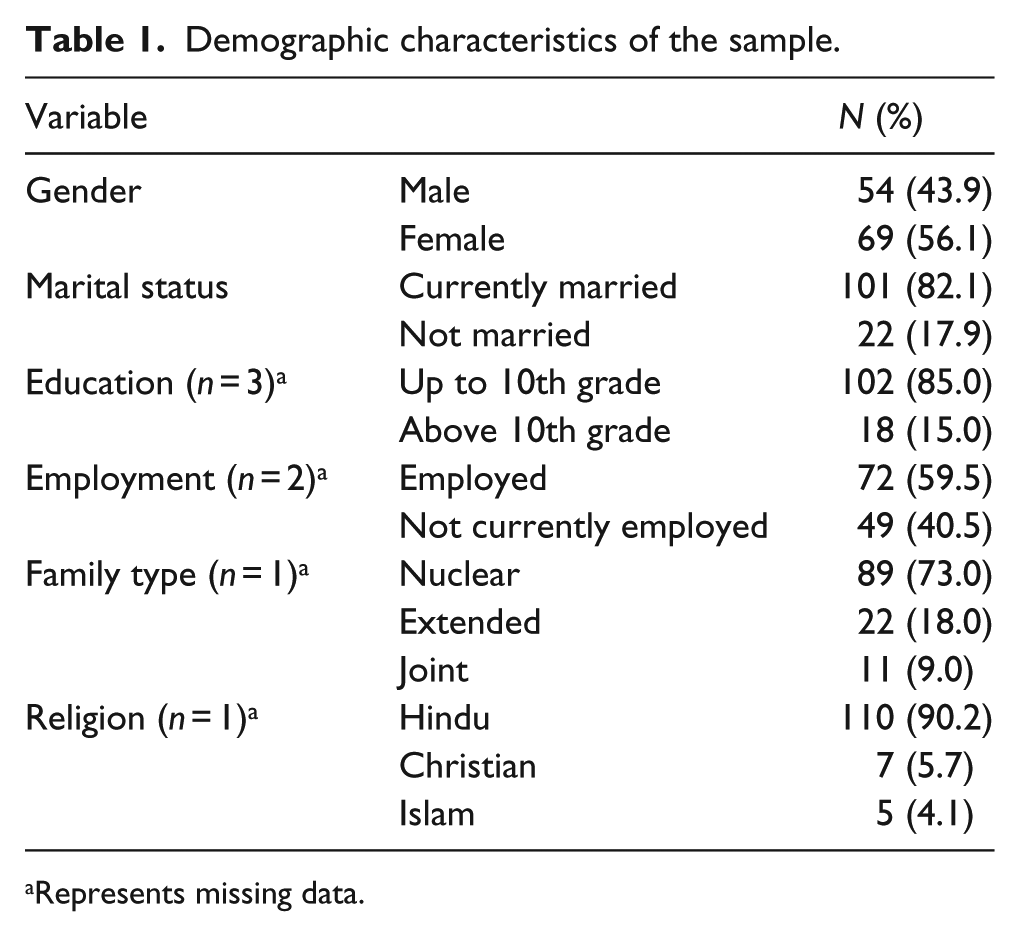
Represents missing data.
Patients had made a median of 10 visits (inter-quartile range of 6–17 visits) prior to consultation at our centre. The information about the health problems that necessitated health care seeking is shown in Table 2. A large majority of the patients reported the nature of problems as ‘non-specific’, that is, neither physical nor of psychological nature. The duration of problems was more than 1 year in about two-thirds of the participants. The reason of the problem was considered internal by about half of the participants and the severity was largely considered moderate to serious. The perceived fear of the problems was most commonly reported as fear of a serious illness, followed by fear of death. About three-fourths of the patients endorsed that coming for seeking help was their own decision, while others reported advice from others as the reason of coming. ‘Internal’ reasons were reported most commonly as the exacerbating factor, while treatment and visits to doctor were the most common relieving factor.
Health problems necessitating treatment seeking.
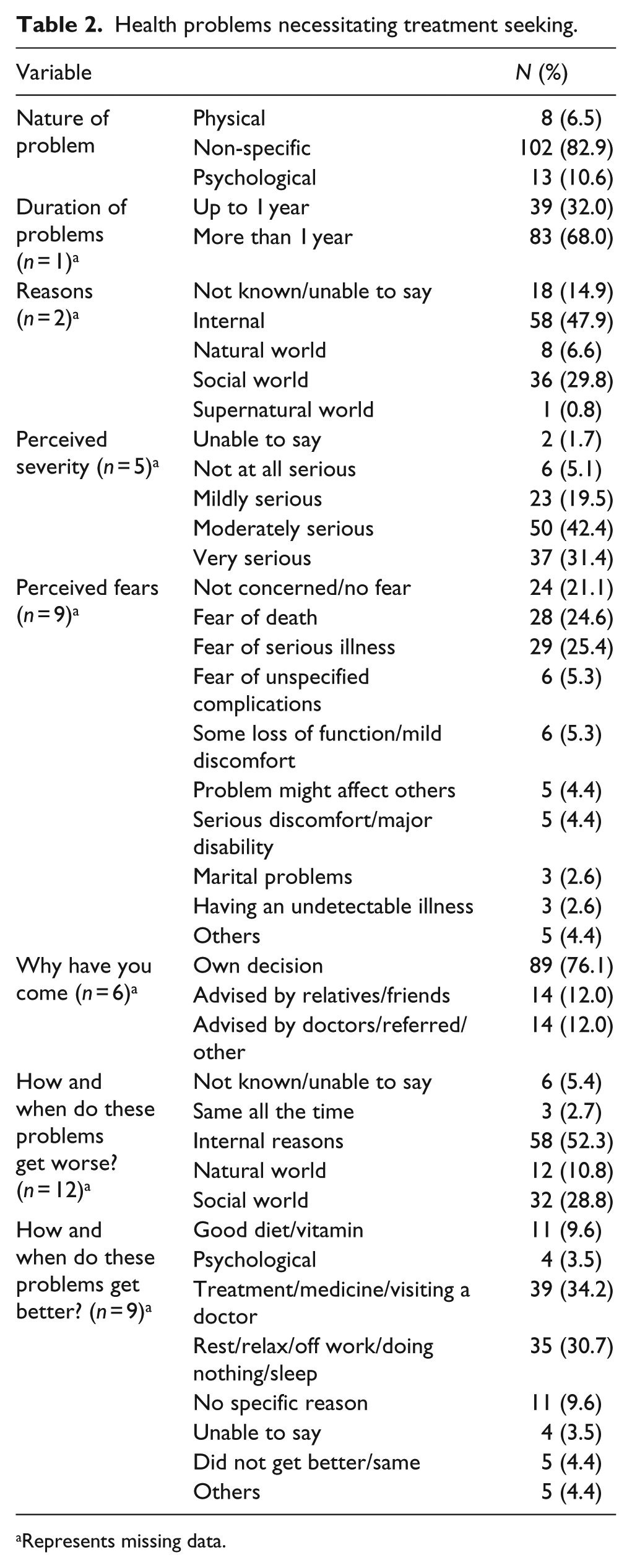
Represents missing data.
The perceptions of treatment are depicted in Table 3. Getting cured and reducing symptoms were most common expectations of treatment, and a lower proportion admitted further examination and investigations as their expectations. About a fourth of the patients reported that their doctors did not say anything about the illness. Medication and treatment were the most common courses of action taken by the physicians. A considerable proportion of the patients were dissatisfied or unhappy with the treatment.
Patient perceptions of treatment.
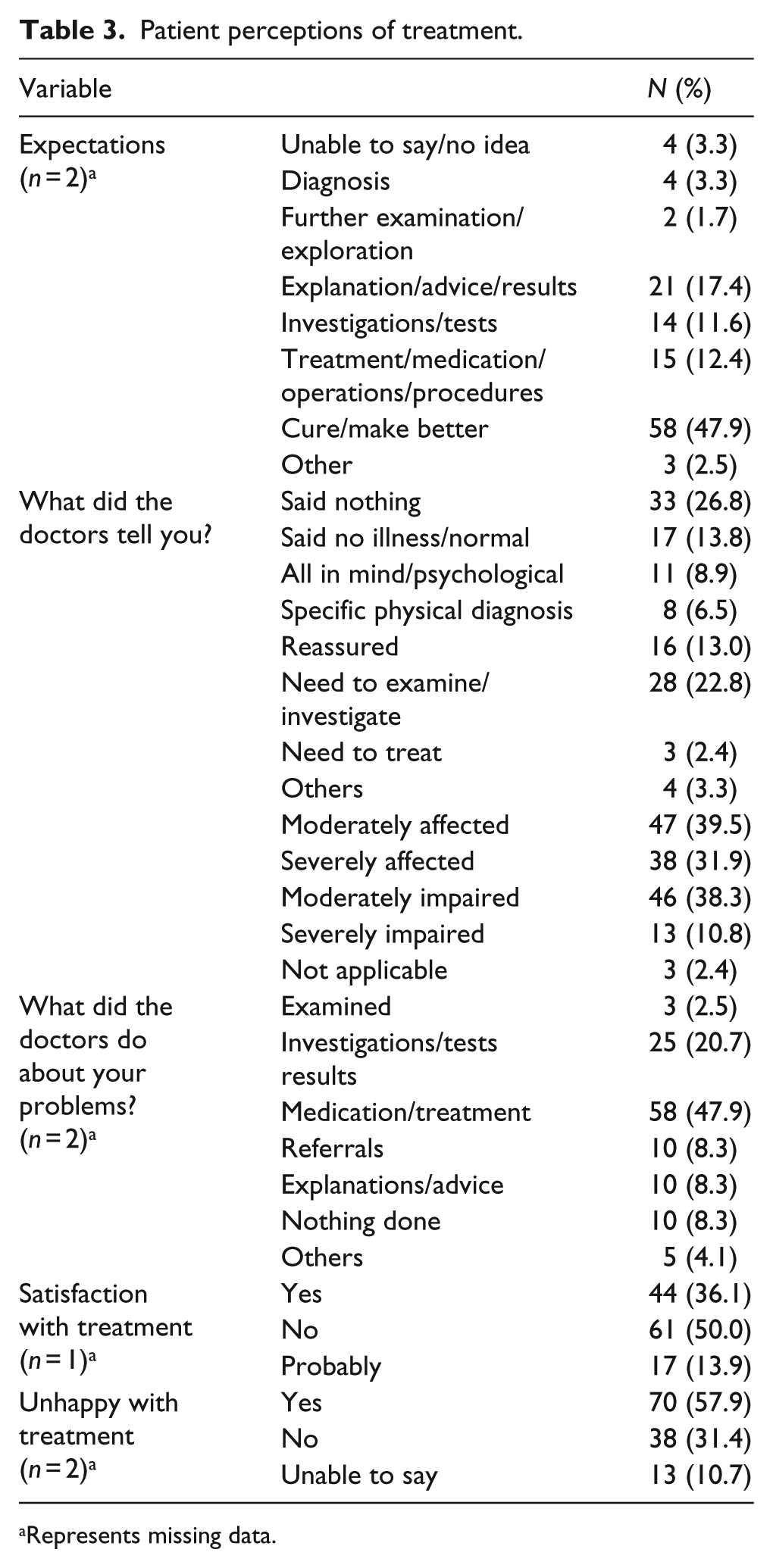
Represents missing data.
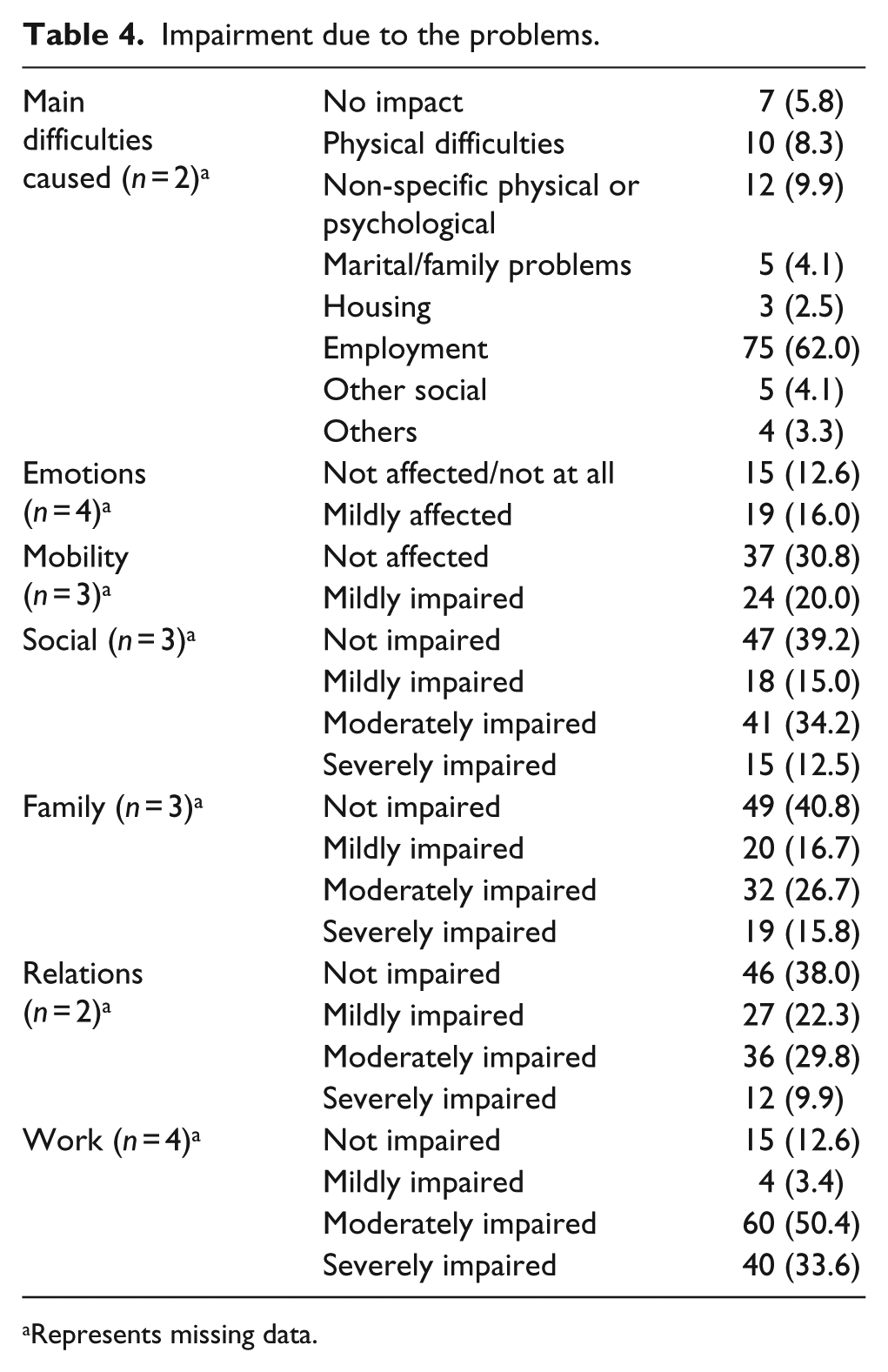
The impairments due to the problems as reported by the patients are shown in Table 4. The most significant impairment was noted in relation to employment by the participants. While the emotions, mobility and work were mostly ‘moderately’ affected; social, familial and relational functioning were largely reported as unaffected.
Impairment due to the problems.
Represents missing data.
Discussion
This study shows that most patients with MUPS are not able to give specific explanations regarding the identity or causality of their symptoms, yet considered them to be very serious and potentially life threatening. This is concurrent with the findings of an earlier Sri Lankan study (Sumathipala et al., 2008), in a setting culturally very similar to ours, that most MUPS patients neither offer scientifically feasible nor culturally acceptable explanations for their symptoms. Concerns about the consequences of symptoms have been shown to be uppermost in the minds of sufferers with MUPS in a previous Indian study too though, in this sample, a higher percentage of sufferers believed in the physical nature of their symptoms (Nambi et al., 2002). The fact that most patients had spent more than a year and passed through numerous health care providers before visiting our centre may indicate a delay in proper diagnosis as well as dissatisfaction with services. Early identification and educating the patients regarding the non-threatening nature of symptoms and strategies to alleviate their fears and concerns appear to be immediate areas that clinicians should focus upon when dealing with suspected MUPS patients.
The predominant single response regarding the expectations from treatment was to get cured or get better. A substantial minority (24%) desired further tests/investigations/medications pertaining to their symptoms. This figure is higher than that reported by Sumathipala et al. (2008); but numerous other studies have shown that expectations about a diagnosis are common in such a cohort of patients with MUPS (Dwamena, Lyles, Frankel, & Smith, 2009; Jackson & Kroenke, 2001). This difference in expectation could be correlated with duration of symptoms. Early on in their presentation, patients may search for a valid diagnosis that resonates with their internal representations about the illness; but as the symptoms become chronic, the focus shifts more towards disabilities and dysfunction. In our sample, the mean duration of symptoms was less than that noted in the Sri Lankan cohort (Sumathipala et al., 2008) and therefore this explanation may hold good. Nevertheless, our findings seem to suggest that many of them thought of a physical explanation for their underlying symptoms. But going by the responses of other sections where the vast majority were unable to reduce their symptoms to physical systems upon direct probing, it appears that the responses need to be viewed holistically as varied manifestations of distress and possible disillusionment with services than distinct or watertight categories. Notably, nearly half of the patients (49.6%) mentioned that doctors either offered no explanation about their condition or ordered further testing without adequate explanation. Both these approaches are those among various iatrogenic factors linked to symptom maintenance in MUPS patients and hence assume clinical significance (Kouyanou, Pither, Rabe-Hesketh, & Wessely, 1998; Kouyanou, Pither, & Wessely, 1997). This may also have contributed to the high levels of overall dissatisfaction reported with treatment (57.9%). Hence, effective communication is vital and clinicians should take the patient into confidence regarding the use of tests and investigations. A recent review succinctly summarizes the spectrum of explanatory models available in the literature and many of them may be useful in daily practice (Van Ravenzwaaij et al., 2010).A judicious use of diagnostic tests can assist in enhancing the quality of the therapeutic relationship and make the approach more patient-centred as has been suggested earlier (Dwamena et al., 2009; Nunes, Ventura, Encarnação, Pinto, & Santos, 2013).
With regard to disruptive impact of symptoms on various domains of activity, an overwhelming majority (84%) reported significant impairments in the work domain followed by emotional and physical mobility domains. A similar profound impact on work output and employment have been noted by earlier researchers too (Hiller et al., 2003; Martin, Rauh, Fichter, & Rief, 2007; Nambi et al., 2002). The impaired domains may be inter-related and the emotional fallout can be explained, at least to an extent, by the lack of productivity and feeling of being unable to contribute adequately to household matters. Considerable evidence also links MUPS with syndromes of affective dysregulation and more specifically, alexithymia (De Gucht & Heiser, 2003; Duddu, Isaac, & Chaturvedi, 2003; Waller & Scheidt, 2006). That only a fewer proportion of patients reported disruptions in family relations may indicate the good social and familial support that sufferers enjoy in this part of the world which is definitely advantageous to the patient. This support may be properly harnessed by care providers to facilitate the recovery process of patients. Earlier observations have suggested that emphasizing on resuming work, in a graded manner, may break the vicious cycle of activity avoidance leading to symptom maintenance (Deale, Chalder, & Wessely, 1998).
Strengths and limitations
This study has explored patient’s perceptions and explanations about MUPS about which there is limited literature globally. The sample is sizeable and the qualitative approach has, doubtless, elicited maximum possible information as opposed to, say, a checklist-based interview. Such an approach of exploring patient’s views can be routinely adopted by clinicians when evaluating MUPS which will reduce the need for a clinician to take a polarizing stand on MUPS such as the presence or absence of physical illness which is anyway difficult to judge (Eisenberg, 1977). This can also inform management and development of patient-friendly and cognitive-behaviour therapy models which may see improved retention and possibly efficacy rates. Obvious limitations of our work include the setting of a tertiary care hospital and the non-random sampling used which may have introduced an element of sampling bias considering that many patients with MUPS do not get referred for specialist care (Röhricht & Elanjithara, 2014). It could also be argued that there was loss/inaccuracy of information when it was recoded but to reduce this, we had two psychiatrists independently do the process of recoding and mutual discussions to sort out discrepancies. Many questions relied on the patient’s ability to recollect details and hence, some recall bias in a study of this kind is unavoidable. The possibility of a medical explanation for some of the symptoms, with a longer duration of follow-up, cannot be categorically ruled out though the 3-month criteria that we have used to determine MUPS were based on prior studies in the field (Nimnuan, Hotopf, & Wessely, 2001; Simon & VonKorff, 1991). Nevertheless, with the above limitations, the study findings assume significance due to the paucity of such qualitative studies in MUPS patients and their potential to transform the way we currently approach and manage these patients.
Conclusion
Most patients with MUPS are unable to offer explanations about the identity of or localize their symptoms to the physical or psychological domains. Yet, they harbour significant concerns about the consequences of their symptoms. Often, they perceive as inadequate the explanations given by treating doctors and remain dissatisfied with services provided. While significant impairments in work and emotional domains are experienced, family relations continue to be harmonious among most sufferers. Clinicians need to approach MUPS keeping these points in mind and should focus on immediate and practical needs of the patients in management. Early identification, explanation, reassurance about the non-threatening nature of symptoms and encouraging patients to resume work early within the supportive framework of the family may facilitate recovery in this group.
Footnotes
Acknowledgements
The authors thank all the participants for their support and valuable time. V.M. conceptualized and designed the work, did the literature review, drafted the protocol, obtained the necessary approvals, co-ordinated data collection and wrote the first draft of the manuscript. B.S. was involved in drafting the study protocol, carried outpatient interviews and gave inputs to write the manuscript. A.B.A. and J.S.T. were involved in recoding the qualitative data, maintaining the records and revised the manuscript for intellectual content. N.S. was involved in patient interviews and contributed to the literature review. S.S. co-conceptualized the work, performed data analysis and gave inputs to revise the manuscript. All authors read and approved the final version of the manuscript. The authors are happy to share the trial protocol upon request. Please contact the corresponding author for the trial protocol.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.