
Abstract
Background:
Despite its efficacy and safety, electroconvulsive therapy (ECT) is underutilized, in part due to stigma associated with the treatment.
Aims:
The aim of this study was to test the hypothesis that experiencing ECT has an impact on associated stigma, as measured by patient and family knowledge of and attitudes toward ECT.
Methods:
A comprehensive literature search was conducted using MEDLINE, EMBASE and PsycINFO. Studies with cross-sectional and/or longitudinal designs were identified. Studies were further categorized into subcategories based on participant type (patients or patient family members) and outcome domain (knowledge or attitudes). Effect size (Cohen’s d) was calculated for each study and then integrated into each subcategory (participant type by outcome domain) using a random effect model.
Results:
Eight studies were identified as being eligible for analysis. Two studies were cross-sectional, five were longitudinal and one incorporated both designs. Analysis of the longitudinal studies indicated that experiencing ECT both increased knowledge of and improved attitudes toward ECT in patients; in family members of patients, analysis showed significant positive change in knowledge of ECT, but no significant change in attitudes toward ECT.
Conclusion:
Experience with ECT may have a positive impact on knowledge of and attitudes toward ECT. However, the quality of evidence of included studies was low; further research is required in order to clarify the relationship and to identify information of use to individuals considering ECT as a treatment option.
Introduction
The efficacy of electroconvulsive therapy (ECT) has been established for a number of psychiatric disorders (reviewed in Trevino, McClintock, & Husain, 2010). In addition to its efficacy, ECT may work faster than medication (Spaans et al., 2015) and is used as a primary treatment for some psychiatric conditions (reviewed in Higuchi, 2010). However, ECT may be one of the most stigmatized therapies in the field of psychiatry (Payne & Prudic, 2009) and may be underutilized despite its demonstrated efficacy and safety (Dowman, Patel, & Rajput, 2005; Surya, McCall, Iltis, Rosenquist, & Hogan, 2015).
Stigma derives from problems of knowledge, attitudes and behavior (Thornicroft, Rose, Kassam, & Sartorius, 2007). In terms of treatments in psychiatry, the act of treatment in and of itself changes patient knowledge of and attitudes toward the treatment. In other words, patients with serious psychiatric conditions may have less positive attitudes toward, or knowledge of, a treatment before it is performed, but the experience of treatment has a positive impact on the patient’s attitudes toward and/or knowledge of the treatment. ECT is a prototypical example of this phenomenon, since it is generally administered to patients with more severe conditions, and could potentially rapidly change their mental status. Given that post-ECT mental status is presumed to be better than status pre-ECT, it is important to answer the question of whether experiencing ECT mitigates stigma associated with ECT. If the experience of ECT does, indeed, mitigate stigma, it would be important for this information to be shared between physicians, patients and patient family members, as it could facilitate more informed decisions with regard to administration of ECT. In spite of the importance of this question, however, no systematic review has yet assessed the association between the experience of ECT and knowledge of and attitudes toward ECT.
Given its efficacy and safety, we hypothesized that the experience of ECT would have a positive impact on knowledge of and/or attitudes toward ECT among patients and their family members (Chakrabarti, Grover, & Rajagopal, 2010; Lasalvia & Tansella, 2008). In this context, we conducted a systematic review and meta-analysis of studies to investigate whether and how the experience of ECT influences knowledge of and/or attitudes toward ECT.
Methods
We conducted screening of studies and synthesis of databases in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement (Moher, Liberati, Tetzlaff, Altman, & PRISMA Group, 2009).
Selection criteria
Studies were included in the present review if they
Were peer-reviewed. Studies without peer review were not included because peer review is a fundamental process to ensure that the study is methodologically sound. This is consistent with the recommendations by the Cochrane Collaboration (Higgins & Green, 2008).
Utilized quantitative measurements to examine attitudes toward and knowledge of ECT. We did not limit analysis to any specific ECT procedure. We found no studies examining behavior related to ECT.
Were of cross-sectional and/or longitudinal design. In the case of cross-sectional design, we included studies that compared quantified information about attitudes toward or knowledge of ECT between patients or family members of patients who had experienced ECT (‘ECT group’) and those who had not experienced ECT (‘non-ECT group’). In the case of longitudinal design, we included all study designs, including randomized controlled trials, controlled before and after studies, and pre–post designs with no control group. A pre–post design denotes studies that compared the potential influence of the experience of ECT on knowledge of and/or attitudes toward ECT by requiring participants to answer questionnaires before and after undergoing ECT.
Data sources and selection process
Studies that examined knowledge of and/or attitudes toward ECT, as described above, were identified using Ovid databases (Ovid MEDLINE®, EMBASE Classic + EMBASE and PsycINFO) (Ando, Yamaguchi, Aoki, & Thornicroft, 2013; Aoki, Cortese, & Tansella, 2015). The syntax used in this systematic screening is shown in Appendix 1. A Google search was also conducted, using the same keywords as for the Ovid search. Finally, reference lists of included studies were reviewed. After deleting duplicates, the titles and abstracts of all studies were evaluated to determine relevance for this review. Final screening was conducted on 4 August 2015. Two reviewers independently identified potentially relevant studies. These potentially relevant studies were then divided into two groups, and the full text of each study obtained. For each group, two reviewers independently examined studies to determine eligibility for the present review. In case of disagreement between these two reviewers, a final determination was made after discussion by all four reviewers. There was no language restriction applied in the process of study selection. The process of selection is shown in a PRISMA flow diagram (Figure 1) (Moher et al., 2009). We also contacted two international organizations (the International Society of ECT and Neurostimulation and the European Forum for Electroconvulsive Therapy), in an effort to ensure that we had not overlooked any eligible studies.
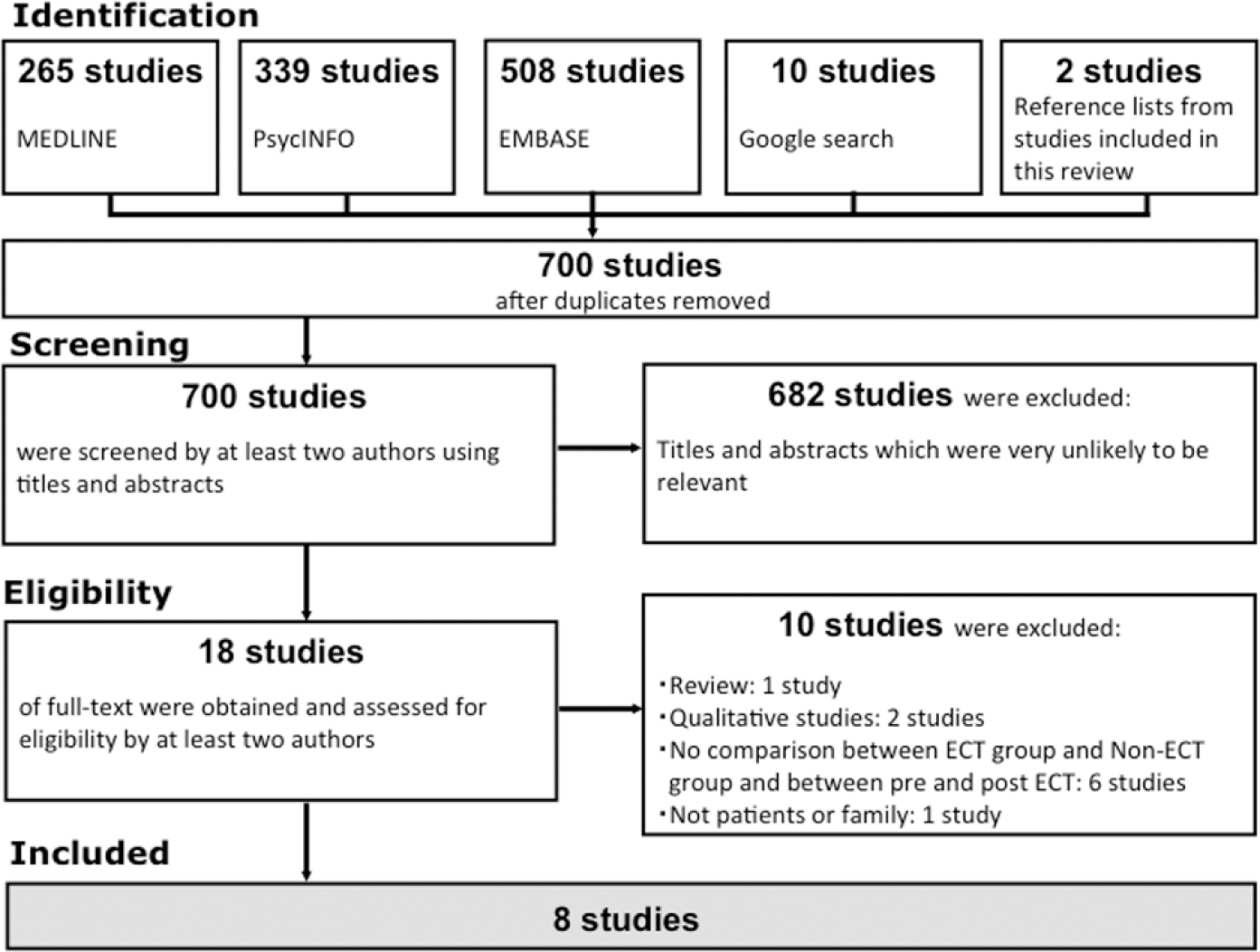
Selection of included studies.
Data extraction
Two authors independently extracted the following data for studies included: (1) name of first author, (2) year of publication, (3) study design (i.e. cross-sectional or longitudinal), (4) number of participants, (5) characteristics of participants, (6) details related to ECT, (7) outcome domain (e.g. knowledge of and/or attitudes toward ECT), (8) results of the outcome evaluation and (9) results of analyses to assess potential associations between knowledge of/attitudes toward ECT and clinical response.
Risk of bias
We assessed risk of bias in cross-sectional studies and longitudinal studies separately, using an assessment tool for methodological quality developed by Gyorkos and colleagues (1994). We employed this assessment tool as it is reported to be the only tool that can evaluate both cross-sectional and longitudinal studies (Sanderson, Tatt, & Higgins, 2007).
With regard to longitudinal studies, the tool has six criteria: (1) strategy for allocating longitudinal and control participants, (2) blinding of subjects, (3) completeness in measurement of intervention, (4) soundness of outcome assessment, (5) blinding of observers and (6) completeness of follow-up. If a criterion was not applicable to a study, the rating ‘Not Applicable (N/A)’ was given. Where each criterion was applicable, the risk of bias was rated as follows: No (no risk of bias), Minor (minor risk of bias) or Major (major risk of bias). Since the tool developed by Gyorkos and colleagues does not specify a minimum standard for these three categories, we used criteria based on a previous study that used the same tool, which is shown in Box 1 (Yamaguchi et al., 2014).
Rating methods and respective criteria for risk of bias.
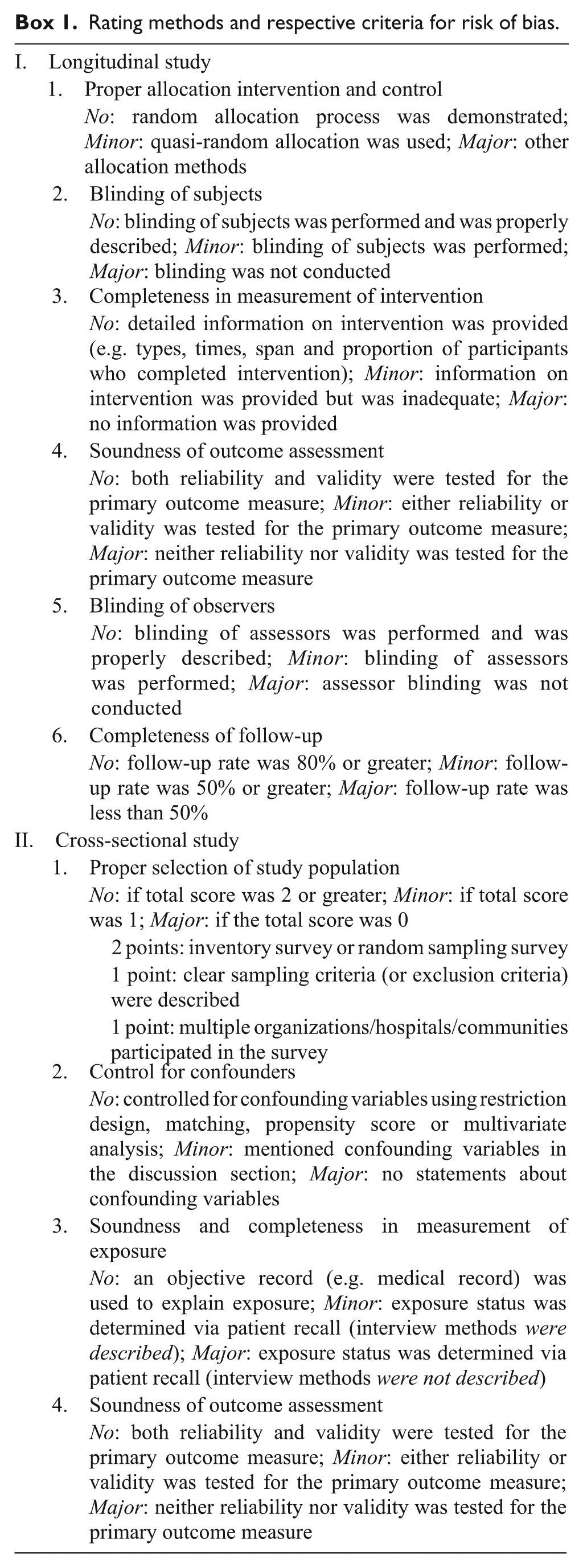
In the case of cross-sectional studies, the assessment tool focused on the following four criteria: (1) proper selection of study population, (2) control for confounding factors, (3) soundness and completeness in measurement of exposure and (4) soundness of outcome assessment. The rating method was similar to that used with the longitudinal studies. Criteria and standards for the three categories of bias risk (No, Minor, Major) are shown in Box 1. With regard to the second criterion (control for confounding factors), since there is no established confounding factor for stigma associated with ECT, it was not possible to assess this criterion. Thus, all studies were classified ‘N/A’ for this criterion.
Data synthesis and statistical analysis
Since the studies included in the present review employ a wide variety of methods for reporting their results, it was not possible to compute standardized mean difference. Thus, we first computed the d for each outcome in individual studies via a Web site (Practical Meta-Analysis Effect Size Calculator) designed by the Campbell Collaboration (Wilson, n.d.; Wilson & Lipsey, 2001). Then, using a random effect model with appropriate formula, the d from individual studies was synthesized to estimate effect size in each outcome domain (knowledge or attitudes), participants (patients or family members of patients) and study design (cross-sectional or longitudinal) (Cooper, Hedges, & Valentine, 2009). When only item-level results of a questionnaire were available, we calculated the d of individual items. We then integrated the d of each item to estimate the d of the questionnaire, using a random effect model.
In terms of associations between knowledge of/attitudes toward ECT and clinical response, the studies included lacked sufficient data to statistically synthesize evidence. Therefore, we narratively reported the relationships between changes in knowledge of/attitudes toward ECT and clinical response (e.g. depression and side effects) when included studies examined those topics.
Results
Selection process
A comprehensive literature search comprising the three databases previously described, a Google search and a hand search identified 700 studies. After initial screening of titles and abstracts, 18 potentially relevant studies were selected for full-text screening. Of these, 10 were excluded for the reasons listed in Figure 1, and eight studies (total number of participants = 774) were included in the present review (Figure 1) (Baxter, Roy-Byrne, Liston, & Fairbanks, 1986; Brodaty, Berle, Hickie, & Mason, 2003; Calev et al., 1991; Goodman, Krahn, Smith, Rummans, & Pileggi, 1999; Grover, Chakrabarti, Khehra, & Rajagopal, 2011; Malekian, Amini, Maracy, & Barekatain, 2009; Pettinati, Tamburello, Ruetsch, & Kaplan, 1994; Szuba, Baxter Liston, & Roy-Byrne, 1991).
Description of eligible studies
Tables 1 and 2 summarize characteristics and outcomes of the studies included in this review. Two are cross-sectional studies (Goodman et al., 1999; Grover et al., 2011), while five are of longitudinal design (Brodaty et al., 2003; Calev et al., 1991; Malekian et al., 2009; Pettinati et al., 1994; Szuba et al., 1991). One study incorporates results from both cross-sectional and longitudinal designs (Baxter et al., 1986); this study is included in the descriptions and tables for both cross-sectional and longitudinal studies.
Description of cross-sectional studies included in the review.
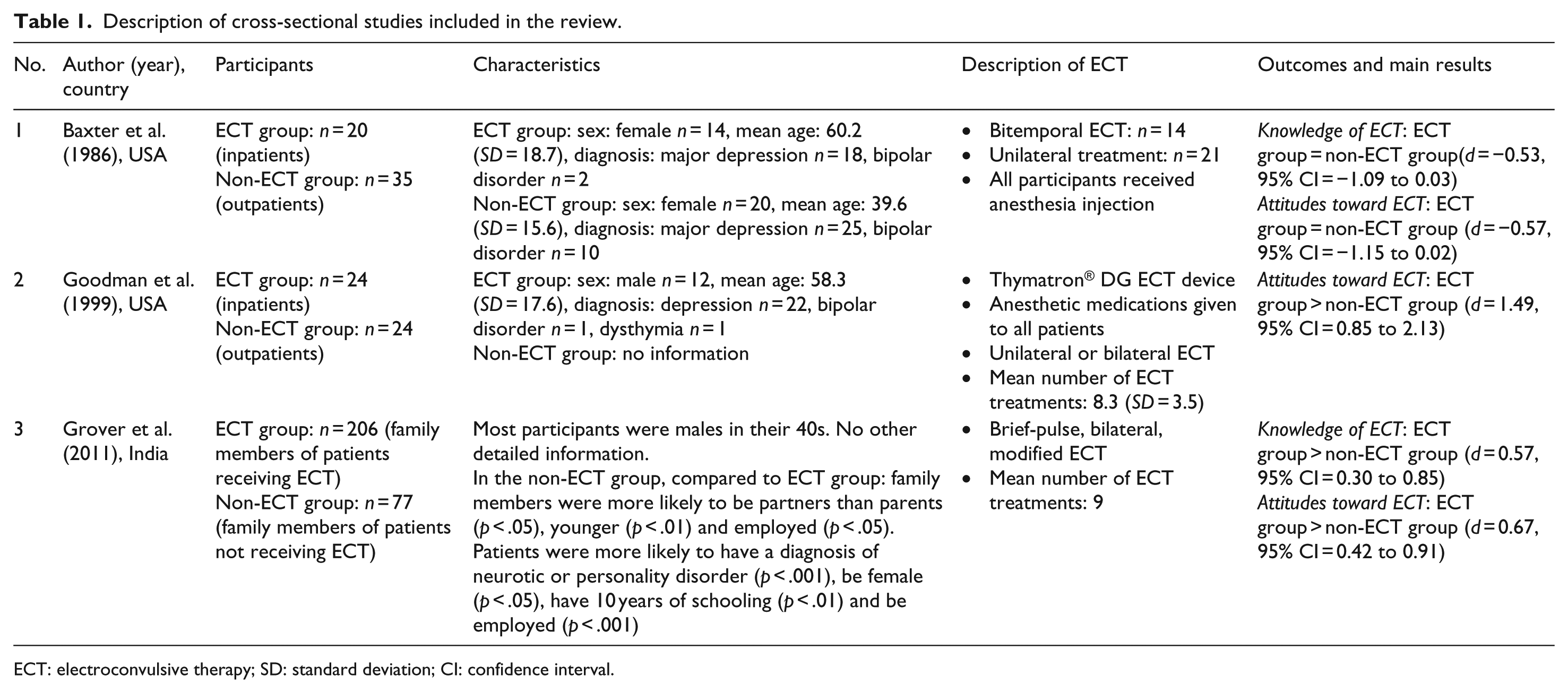
ECT: electroconvulsive therapy; SD: standard deviation; CI: confidence interval.
Description of longitudinal studies included in the review.
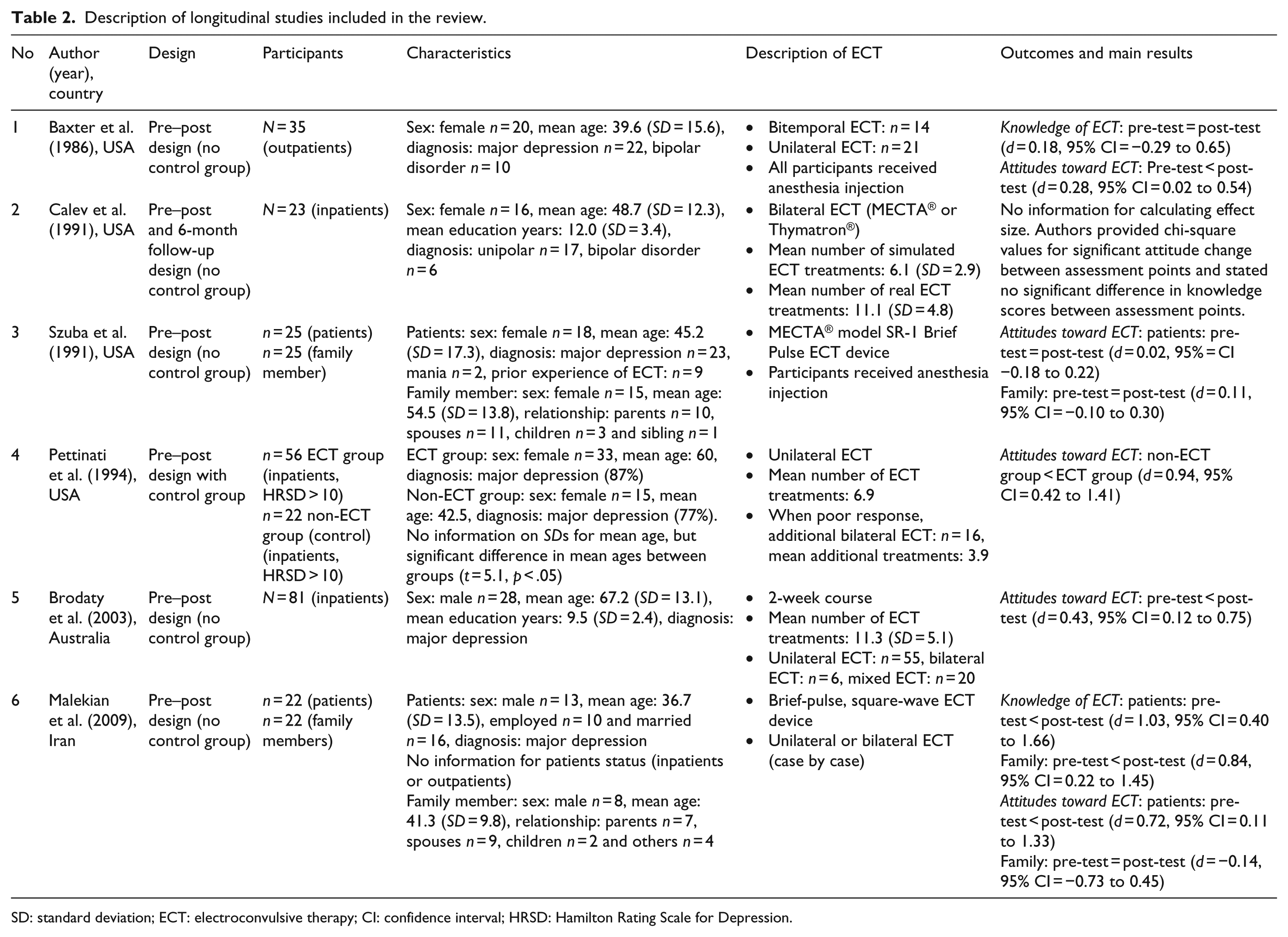
SD: standard deviation; ECT: electroconvulsive therapy; CI: confidence interval; HRSD: Hamilton Rating Scale for Depression.
None of the longitudinal studies used a randomized controlled methodology. Only one longitudinal study featured a control group (non-ECT group) to assess the effect of the ECT experience on attitudes toward ECT (Pettinati et al., 1994). Five studies were conducted in the United States (Baxter et al., 1986; Calev et al., 1991; Goodman et al., 1999; Pettinati et al., 1994; Szuba et al., 1991); the remaining three were from Australia (Brodaty et al., 2003), India (Grover et al., 2011) and Iran (Malekian et al., 2009). In most studies, bilateral ECT was administered. Five studies included only patients as participants (Baxter et al., 1986; Brodaty et al., 2003; Calev et al., 1991; Goodman et al., 1999; Pettinati et al., 1994), two studies included both patients and their family members (Malekian et al., 2009; Szuba et al., 1991) and one enrolled only family members of patients (Grover et al., 2011).
Risk of bias
With regard to the cross-sectional studies, only one (Goodman et al., 1999) had clear inclusion and exclusion criteria (classified as ‘minor’ risk of bias in terms of proper selection of study population) and used objective records to identify exposure status of patients (‘no’ risk of bias in terms of soundness and completeness in measurement of exposure). It should be noted that no cross-sectional studies used established measures to assess patient knowledge of or attitudes toward ECT (Table 3). For the longitudinal studies, three of the six criteria for risk of bias were not evaluated, as none of the studies were randomized controlled trials (Table 4). Three studies provided sufficient information on ECT procedure and number of ECT treatments (Brodaty et al., 2003; Calev et al., 1991; Pettinati et al., 1994). All but one of the longitudinal studies had no established outcome measures; Malekian et al. (2009) used outcome measures from a previous study. All studies followed up with more than 50% of participants.
Risk of bias table for cross-sectional studies.
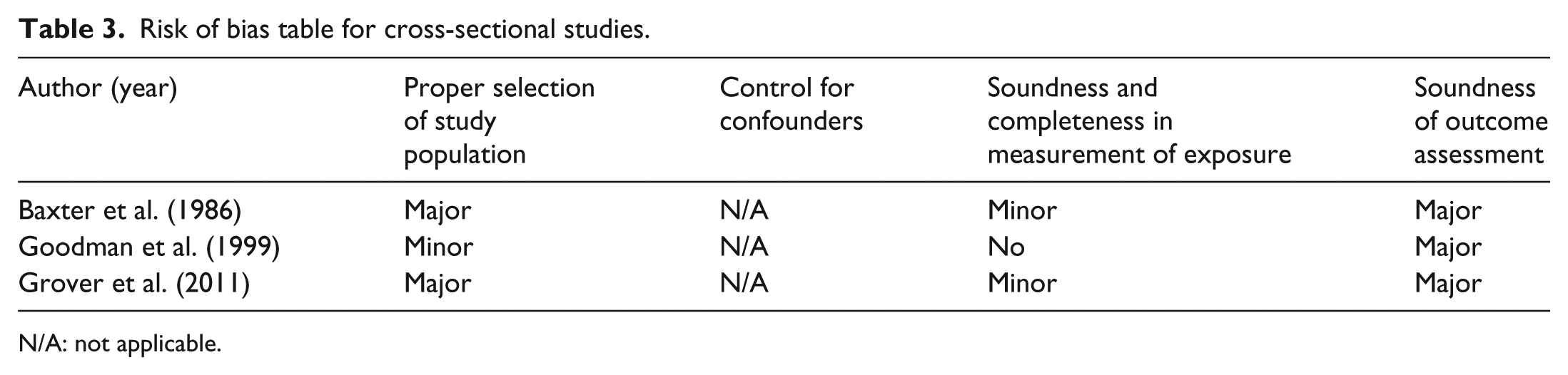
N/A: not applicable.
Risk of bias table for longitudinal studies.
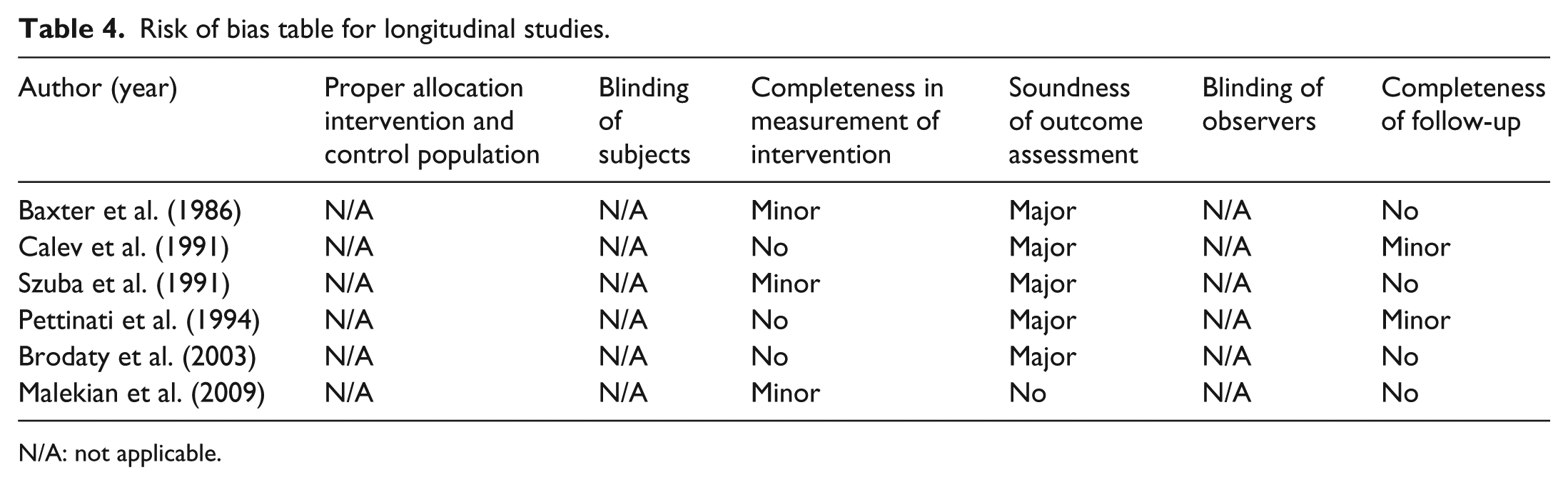
N/A: not applicable.
Effects of ECT experience on knowledge of and attitudes toward ECT
Effect sizes for each domain are shown in Table 5. Analysis of cross-sectional studies showed no significant difference in knowledge of or attitudes toward ECT between patients who had experienced ECT and patients who had not experienced ECT (Baxter et al., 1986; Goodman et al., 1999). However, a relatively large cross-sectional study (Grover et al., 2011) found significantly better knowledge of ECT (d = 0.57, 95% confidence interval (CI) = 0.30 to 0.85) and more favorable attitudes toward ECT (d = 0.67, 95% CI = 0.42 to 0.91) in family members of patients who had experienced ECT compared to family members of patients who had never experienced ECT.
Effects of ECT experience on knowledge and attitudes, among eligible studies.

ECT: electroconvulsive therapy; CI: confidence interval.
Two longitudinal studies (Baxter et al., 1986; Malekian et al., 2009) assessed patient knowledge of ECT both before and after ECT, and analysis showed significant improvement in their knowledge of ECT (d = 0.53, 95% CI = 0.04 to 1.02). In addition, analysis of four studies (Baxter et al., 1986; Malekian et al., 2009; Pettinati et al., 1994; Szuba et al., 1991) demonstrated that patients held more positive attitudes toward ECT after experiencing ECT compared with attitudes before ECT (d = 0.36, 95% CI = 0.09 to 0.64). One study (Malekian et al., 2009) suggested that family members’ knowledge of ECT also improved after administration of ECT (d = 0.84, 95% CI = 0.22 to 1.45). However, family members’ attitudes toward ECT did not show significant improvement (Malekian et al., 2009; Szuba et al., 1991).
One longitudinal study (Pettinati et al., 1994) with a control group also reported a significant improvement in attitudes between a post-ECT group and a non-ECT (control) group (d = 0.94, 95% CI = 0.68 to 1.20).
Associations between knowledge/attitudes and clinical response
Three studies examined the relationship between changes in knowledge of or attitudes toward ECT and clinical outcomes (Table 6). Two studies reported potential associations between positive changes in attitudes (or attitude improvement) toward ECT and improvement in depression, as measured by the Hamilton Rating Scale for Depression, and with side effects (Brodaty et al., 2003; Calev et al., 1991). In contrast to this, the third study did not find any significant relationship between those variables (Szuba et al., 1991).
Associations between knowledge of/attitudes toward ECT and clinical outcomes.
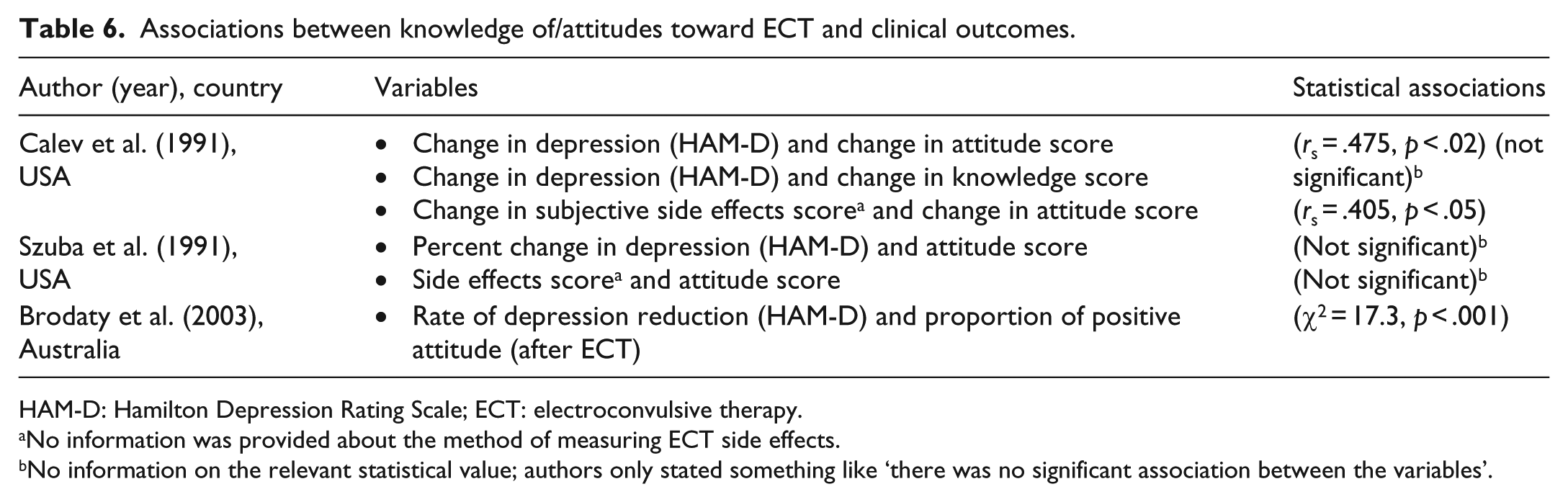
HAM-D: Hamilton Depression Rating Scale; ECT: electroconvulsive therapy.
No information was provided about the method of measuring ECT side effects.
No information on the relevant statistical value; authors only stated something like ‘there was no significant association between the variables’.
Discussion
Summary of findings
Two longitudinal studies with patients who had experienced ECT showed significant improvement in knowledge of ECT, although one cross-sectional study did not demonstrate any significant difference in knowledge of ECT between patients who had experienced ECT and patients who had not. Longitudinal studies involving patients, including one with a control group, also showed significant improvement in attitudes toward ECT post-treatment. However, cross-sectional studies with patients did not demonstrate any significant difference in attitudes toward ECT between those who had experienced ECT and those who had not.
Response to ECT and attitudes toward and knowledge of ECT
Changes in attitudes toward ECT may be related to the response to ECT. In other words, in the case of longitudinal studies, responders may be in better psychiatric condition post-ECT than they were pre-ECT. People with greater response to ECT may appreciate the treatment more than those who had negative experiences with ECT. Furthermore, responders may also have greater cognitive ability to increase their knowledge of ECT.
In the case of cross-sectional studies, it is reasonable to assume that, for both patients and their family members, response to ECT is seen as a successful experience, which in turn provides a foundation for better attitudes and increased knowledge. However, due to insufficient information, in the present review it was not possible to assess the potential relationships between response to ECT and attitudes toward ECT. Future studies with large sample sizes, and sufficient data, are warranted.
Potential relationships between knowledge and attitudes
Our interpretation that experiencing ECT may decrease stigma associated with ECT would be supported if we were able to identify a coincidence of increased knowledge of, and improvements in attitudes toward, ECT. While it was not possible to statistically assess this relationship in the present review, we did observe such a tendency. For example, in one cross-sectional study, Baxter and colleagues found no differences in either knowledge of or attitudes toward ECT in ECT and non-ECT groups, whereas Grover and colleagues found both increased knowledge of and improved attitudes toward ECT in participants who received ECT versus those in the non-ECT group (Baxter et al., 1986; Grover et al., 2011). However, in the case of longitudinal studies, the relationship between knowledge and attitudes is not clear. Malekian and colleagues reported both increased knowledge of and improved attitudes toward ECT in the context of pre–post testing, while Baxter and colleagues identified improvements in attitudes toward ECT, but no change in knowledge of ECT (Baxter et al., 1986; Malekian et al., 2009). It is very important that future studies examine these relationships in more detail, in both cross-sectional and longitudinal contexts.
Knowledge/attitudes toward ECT and clinical outcomes
Potential associations between knowledge of/attitudes toward ECT and clinical outcomes, including depressive conditions and side effects, appear to be still inconclusive due to discrepancies in results and insufficient data (Brodaty et al., 2003; Calev et al., 1991; Szuba et al., 1991). In addition, the three studies noted assessed these associations in different ways. For example, one examined the correlation between attitude change and depression improvement over time, while another compared the rate of depression reduction with the proportion of patients reporting positive attitudes toward ECT treatment. Further discussion on appropriate standard methods of testing the association between knowledge of/attitudes toward ECT and clinical outcomes is needed.
Between-study heterogeneity and evidence level of studies included in this review
It should be noted that the included studies have high between-study heterogeneity. However, the number of included studies is too small to quantitatively assess between-study heterogeneity. For example, the included studies utilized a variety of in-house questionnaires that had not been shown to be reliable or replicable. In addition, all the cross-sectional studies, and one longitudinal study with a control group, lacked sufficient information about participant characteristics and/or the characteristics of the ECT and non-ECT groups. In the longitudinal studies, the results of post-ECT questionnaires were compared with those obtained before ECT treatment. However, given the nature of ECT, it is impossible to conduct a study that provides high-quality evidence, such as a double-blind, randomized controlled trial, or to perform ECT simply to examine changes in knowledge of and attitudes toward ECT. Thus, despite their low quality of evidence, we integrated the results of these studies in order to test our hypothesis.
Difference in results between longitudinal and cross-sectional designs
Analysis of longitudinal studies showed that experiencing ECT increased knowledge of and improved attitudes toward ECT, except in the case of attitudes of family members. On the other hand, cross-sectional studies did not show any significant differences in knowledge of or attitudes toward ECT between patients, regardless of the presence or absence of experience with ECT. There are two possible explanations for this inconsistency. First, the number of cross-sectional studies and their participants was smaller than the number of longitudinal studies and their participants, although the cross-sectional studies did have more heterogeneity in participant characteristics than longitudinal studies. The cross-sectional studies may have been too small and lacked the statistical power needed to achieve significance. Second, the effect of the ECT experience on reducing stigma associated with ECT, as seen in improved knowledge of and/or attitudes toward ECT, might not last long. Although it was not explicitly stated in the included studies, it is apparent that longitudinal studies examined knowledge of/attitudes toward ECT shortly after ECT treatment, while cross-sectional studies recruited patients who had experienced ECT long before the questionnaire.
Potential implications for future clinical practice and research
Some of the present results may be interpreted in the context of the recent recommendations on ECT usage offered by Coffey and Coffey (2016). For example, the authors wrote, ‘Patients have unfettered access to their own medical information. Referring providers receive treatment updates on the same day of the patient’s ECT visit’. Coffey and Coffey also state, ‘Family members and loved ones are invited to participate in every step of the ECT visit, including the actual ECT treatment, and thus become allies for quality and safety of ECT care’. These statements emphasize knowledge, as does this study. The present results suggest that before receiving ECT, patients may enhance their knowledge by observing ECT equipment, or talking with patients who have already received ECT. Further, as Coffey and Coffey recommended, ‘patient-centered ECT’ is essential in the context of shared decision making between clinicians and patients (Duncan, Best, & Hagen, 2010).
The results of this study may also prove to be a useful addition to information on the efficacy of ECT (reviewed in Trevino et al., 2010) and its subjective side effects (Fisher, 2012; Frank Koopowitz, Frank Koopowitz, Chur-Hansen, Reid, & Blashki, 2003; Rose, Fleischmann, Wykes, Leese, & Bindman, 2003). However, this study also revealed the currently low evidence level for the potential effects of receiving ECT on knowledge of and attitudes toward ECT. From this, we can say that three types of studies are needed in the future. First, it is necessary to develop validated measures that can objectively assess knowledge, attitudes and behavior related to ECT. Second, longitudinal studies with substantially large sample sizes and demographically matched control groups are needed to clarify the effects of receiving ECT on knowledge of and attitudes toward ECT. Finally, the potential association between knowledge/attitude improvement and clinical outcomes of ECT should also be explored.
Limitations
There are a number of limitations to the present systematic review and analysis. First, although there is no ‘gold standard’ method for evaluating stigma associated with ECT, the quality of evidence was not high. Second, only a small number of studies were included, and these had high between-study heterogeneity, although we did utilize a random effect model in an attempt to integrate them. Third, the studies analyzed were published over a 25-year period, from 1986 to 2011. In light of the changes in public attitudes toward psychiatry and psychiatric treatment in general during this time, there may be accompanying changes in attitudes toward and/or knowledge of ECT. However, due to the small number of included studies, it was not possible to examine this potential chronological change.
Conclusion
Experience with ECT treatment may have a positive impact on knowledge of and/or attitudes toward ECT, which may then contribute to reducing stigma associated with ECT. Few relevant studies were found, however, and the quality of evidence was generally low. Further study of this issue is necessary.
Footnotes
Appendix 1
Acknowledgements
The authors are deeply grateful to Prof. Pascal Sienaert, the European Forum for Electroconvulsive Therapy and the International Society for ECT & Neurostimulation for their kind assistance with identifying potentially relevant research studies. Yuta Aoki and Sosei Yamaguchi contributed equally to this study.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported, in part, by the Japan Society for the Promotion of Science (Y.A.).