
Abstract
Background:
Suicide is a major worldwide public health issue. Various studies showed that individual attitudes toward suicide change in a region with high suicide rate. Attitudes are one of the components of a global and complex system: social representations (SRs).
Aims:
In France, the Brittany region has an abnormally high death rate due to suicides. Our research focuses on the SRs of suicide in this region. The hypothesis underlying this project is that suicide SRs are different between an area with a high suicide rate and a region less affected by suicide.
Method:
A comparative study between the Brittany and Alsace regions, with the latter showing a statistically much lower suicide rate. The persons polled responded to a three-word free-association task around the question ‘For you, suicide is …?’ An analysis of word frequency and evocation rank was then carried out.
Results:
In confirmation of our hypothesis, SRs were different between Brittany and the control region.
Conclusion:
The study’s results open new avenues of research, specific to Brittany, in terms of the collective or individual effects of suicides, in terms of psycho-pathological conditions – essentially on depression, and in terms of training, on the stereotypes associated with suicide.
According to the World Health Organization (WHO), suicide reached the dreadful figure of 804,000 deaths throughout the world in 2014. The Organization then advocated for the necessity of making suicide prevention a major worldwide public health goal.
The multifactorial nature of suicide is now widely accepted (WHO, 2014; Wingate, Joiner, Walker, Rudd, & Jobes, 2004). As such, it concerns various fields of knowledge including sociology and psychology. End of the 19th century, in the United States with N. Triplet and in France with G. Le Bon, those two disciplines met each other via the creation of social psychology, a comprehensive framework notably interested in attitudes, stereotypes, opinions of population about social objects such as money, unemployment, drugs and so on.
Till date, no study has been carried out about the collective view of suicide in social psychology. Various studies exist in psychiatry and argued that we also have to be concerned by the attitudes and opinions toward suicide (Gibb, Andover & Beach, 2006) because of their impact on one’s behavior (Segal, Mincic, Coolidge, & O’Riley, 2004).
Since the Mc Intosh, Hubbard and Santos (1985) seminal study on opinion toward suicide that was carried out in the United States, attitude, opinions and stereotype regarding suicide have become a worldwide field of research. An important number of questionnaires dealing with suicide-related attitudes and opinions were developed, such as the Suicide Opinion Questionnaire (Domino & Leenars, 1989; Domino, Moore, Westlake, & Gibson, 1982), a touchstone in the analysis of suicide-related attitudes within the general population. This document served as a basis for the following questionnaires: the Suicide Attitude Questionnaire (SUIATT) (Diekstra & Kerkhof, 1988), the Suicide Behavior Attitude Questionnaire (SBAQ) (Botega et al., 2007), Semantic Differential scale Attitudes towards Suicidal behavior (SEDAS) (Jenner & Niesing, 2000), Attitude Towards Suicide (ATTS) (Renberg & Jacobsson, 2003) and so on.
Thanks to these assessment tools, several correlates have been put forward of attitudes toward suicide. The research works show differences according to region, sex and age, personal experience of suicide (suicide of a close relative, past history of suicide attempt), and also according to the respondent’s profession, the suicide rate of the area, and so on (Beautrais, Horwood, & Fergusson, 2004; Gagnon & Hasking, 2012; Gibb, Andover, & Beach, 2006; Kocmur & Dernovsek, 2003; Kodaka, Inagaki, Postuvan, & Yamada, 2013; Renberg, Hjelmeland, & Koposov, 2008; Reynders, Kerkhof, Molenberghs, & Van Audenhove, 2015; Segal, 2000; Segal et al., 2004; Westefeld, Sikes, Ansley, & Yi, 2004).
Most of these studies converge to point out the negative effect of both suicide rates on a collective level and of a personal history of suicide attempt on the individual level regarding attitudes toward suicide. It causes an alteration of general attitudes, in terms of rationalization or stigmatization (Beautrais et al., 2004; Renberg et al., 2008; Renberg & Jacobsson, 2003; Reynders et al., 2015), permissiveness (Gibb et al., 2006), and the tendency not to ask for medical care (Reynders et al., 2015).
Those studies highlighted the correlation between the individual and collective effects of suicide. As Freud (1921) proposed, the individual psychology is also straightaway and simultaneously a social psychology. Thus, it is important to analyze how both dimensions work together and influence each other. One of the most important French social psychologist, Moscovici (2013), argued that attitudes cannot be disentangled from another important concept: social representations (SRs). An SR is a form of knowledge, elaborated and shared within a society, having a practical objective, utility and contributing to the construction of a shared reality for this social unit (Jodelet, 1989, p. 53). Moscovici brought this notion back into fashion, inspired by the works on collective representation of the French school of sociology (Durkheim, Halbwachs, Levy-Bruhl). He distances himself from Durkheim (1960) in respect that, according to him, the individual and collective are not two distinct fields. On the contrary, the SRs are the bridge between the individual and the social worlds and are always ‘in the making’.
However, no research in suicidology or social psychology has yet taken an interest in the SR of suicide.
Attitudes, opinions and SRs
Opinions and attitudes are already second-stage mental constructions, in that they attempt to evaluate both a social object and the stereotypes qualifying the individuals linked to this social object. Underlying these secondary constructions are the SRs of the social object. Moscovici (2013) states that SR is what links the unknown and the familiar. The unknown generates lacks of communication within a group, modifies the linguistic codes and deconstructs the relations with others. According to Doise (1992), in order to become familiar with this unknown, people try to embed these unknown perceptions in the pre-existing SR and thus modify SR. Suicide is something that generates unknown, anxiety, distress, and may generate silence, trauma and so on.
SR is therefore a knowledge based on common sense – not necessarily opposed to scientific knowledge, and not necessarily less accurate, because it is also founded, at least partly, on exact knowledge shared by the individuals belonging to the group. The representation exists both psychologically and socially (Jodelet, 1989; Mannoni, 1998) and is developed through a dynamic, interactive and transversal process. It can be generated by an individual who develops, in and of himself, an infra-linguistic mental image of an object according to their sensations (Cyrulnik, 1995), to their personal experience, and according to what they hear or see produced in reaction to this object; the representation is shaped according to this individual’s relationship to others through education, culture, tradition, and collective attitude.
Because the individual is embedded in social interactions and networks of communication, his mental representation is progressively shared. They circulate through attitudes, are transmitted in the family, social and cultural speeches by means of the language, in other words in the inter-personal communication, broadcasted in media messages and images, and crystallized in behavior, in the socio-cultural practices (Costalat-Founeau, 1995; Jodelet, 1989; Perreira de Sá, 1994). In such a way, SRs weave social ties between members of a group. They create a sense of belonging through the experience of shared thinking and acting respective of a specific object. Acting as a feedback function, the social attitude regarding a common object is mentally integrated by the individual: A flow, a permanent mobility and permeability would seem to exist between the social and personal mental worlds within a cultural sphere, which supposes the existence of a two-way sharing, in the course of which mental elaborations are created; then from this material, social representations are built up. An individual can only create these elaborations from the mental material acquired within his reference group, and any member of the group can easily share and make them his. (Mannoni, 1992, p. 16)
It can also be postulated that these representations can be by more than one generation (Mannoni, 1992) because the relationships within the common sphere are shared by different age groups, particularly within the family unit.
However, interpretation of SR should carefully take into account temporal and spatial considerations, because they largely depend on social, historical, political and economic contexts in which they find their roots. Individual psychological contingencies can also make them unsteady: in some situations, representation becomes impossible, for example in traumatic circumstances. And thus SRs are not consensual.
As a consequence, methodological rigor would require studying a social object – suicide in the present case – under both individual and collective scopes, as this object, the manner in which it is built up, and the way it exerts its influence, alter the group’s relationship to this object (Guimelli, 1993; Lin, He, Jin, Tao, & Zhongli, 2013). The common sense varies according to the society in which the individuals evolve (Moscovici, 2013). These factors justify a local analysis of SR.
Aims
The Brittany region has the highest suicide rate in France: +65% above the national average (Observatoire National du Suicide (ONS), 2016). For Renberg et al. (2008), variability in the prevalence of suicide can be understood thanks to the group’s cultural and normative dimensions. The aim of this study, through the analysis of the SRs of suicide, was to identify possible ways of facilitating the social group’s access to prevention messages, actions and to medical care in case of suicidal crisis. The object of this study was to confirm whether the social object ‘suicide’ was perceived equally in two areas differently impacted by suicide. Our hypothesis was that the SR of suicide would be different. And if the representation of suicide in Brittany is different, in what way and what is the link with the collective knowledge, attitudes, behavior and the possibility to develop new field of research and prevention initiatives?
Methods
Participants
In an attempt to account for suicide rates, previous studies performed in Brittany (Barbançon, 2002; Benjankhar, 2014; Broudic, 2008; Carrer, 2007; Carrer, Houzel, Le Bechennec, Meyer, Vedeilhie, & Violette, 1986; Kress, 1984; Montplaisir, 2003; Observatoire Régional de la Santé Bretagne (ORSB), 2013, 2014a) have pointed out the socio-historical factors strongly affecting the Breton population at various points of its history: the trauma of World War I (WWI) and the resulting weakening of family structures and roles within the family; the widespread depression in mothers; the linguistic trauma of having been forced to speak and write in French instead of in the Breton language; the loss of religion; a transitory loss of cultural references with long-term psycho-pathological effects such as verbal inhibition (Kress, 1984; Houzel, in Carrer et al., 1986), alcoholism and suicide.
For purposes of comparison, we chose a French region with a fairly similar historical–cultural experience: a strong regional identity, a regional language that is both spoken and claimed as a significant identity marker, and a location about the same distance from the capital – but with a lower suicide rate than both Brittany and the national average.
The Alsace region fulfills all these criteria. Suicide rate in Alsace is 10.7/100,000 habitants versus 15.1 in the whole country (ONS, 2016). The history of Alsace in the 19th and 20th centuries includes a succession of wars, in which the men were forced to fight in the German army against their own homeland. The regional language also has a chequered history, both in relation to French language and through its linguistic similarity with the German language. Some studies highlight that both regions have an important religious background (Institut Français d’Opinion Publique (IFOP), 2006; Schlegel, 2010; Tranvouez, 2014).
Alsace is however dissimilar in terms of geographical extent, population density, socio-economic level and accessibility. The last two variables are probably linked with the region’s history, its location and its post-war development. Alsace could be said to be the reverse image of Brittany: more geographically isolated, with disparities in population density and socio-economic development (Alsace has built up trade along its border with Germany).
We chose to focus on the historical, cultural and geographical variable, since these components are the ones which are most frequently brought forward (Barbançon, 2002; Broudic, 2008; Carrer et al., 1986; Carrer, 2007) in Brittany to explain the population’s difficulties.
Means
A questionnaire 1 was created to study the SR of suicide with a three-word free-association task with simple directives. The free-association word task is a classic tool in SR studies (Bergamaschi, 2011; Fontaine & Hamon, 2010; Walchelke, 2008, etc.). It calls upon the latent content of the representation (Abric, 2011; Salès-Wuillemin, Galand, Cabello & Folcher, 2011), opening a way to the semantic field of the social object under study through the spontaneous and projective dimension of the task (Abric, 2011).
We also asked for socio-demographic characteristics, but we could not explore religious affiliation because of French rules and regulations.
Procedures
Questionnaires were made available on a numeric platform for four consecutive months. Invitation to access this platform was spread through local media of the two regions under study: the weekly or daily papers (in their print editions and their social network pages), by radio, and also by word of mouth through public health organizations, and so on.
We chose this because of the sensitive nature of the study’s theme. Social psychology studies (Flament, Guimelli, & Abric, 2006; Guegan, Moliner, & Vidal, 2013) have suggested that, faced with issues charged with relatively high psychological impacts, or involving the respondents’ emotions, the results obtained with face-to-face questionnaires were distorted by a masking mechanism of SR: face to face with a living person, respondents do not tend to express what they really think.
Sample
The questionnaire was designed for adults (aged over 18 years) with no upper age limit.
Selection criterion was that the respondents should reside in one of the two regions under study, whether or not they were natives of that region. The respondents’ consent to the use of the data for research was requested at the beginning of the questionnaire.
Type of study
In accordance with Abric’s theories, we considered an SR to be made up of a stable, ‘non-negociable’ central core (CC) (Valence, 2010, p. 46) including one or more elements, which structures and generates the meaning of the whole representational field under consideration (Valence, 2010, p. 46), and a more flexible peripheral system (PS), more labile and also more likely to alter and adapt to the context (Wagner, Valencia, & Elejabarrieta, 1996).
Starting from a three-word free-association task answering the question ‘For you, suicide is?’, we used Vergès’ (1992) method, a double analysis of the evocation rank, to study the structure of the SR. It is an analysis of the frequency with which a word of a given lexical field appears, correlated with its rank of occurrence. It gives an indication of the central position of an element within the SR (Abric, 2011, p. 83) and gives an initial approach and description of the representation’s internal structure (Walchelke, 2008) (Table 1).
Analysis of the structure of a social representation through a cross-comparison of frequency and evocation ranks.
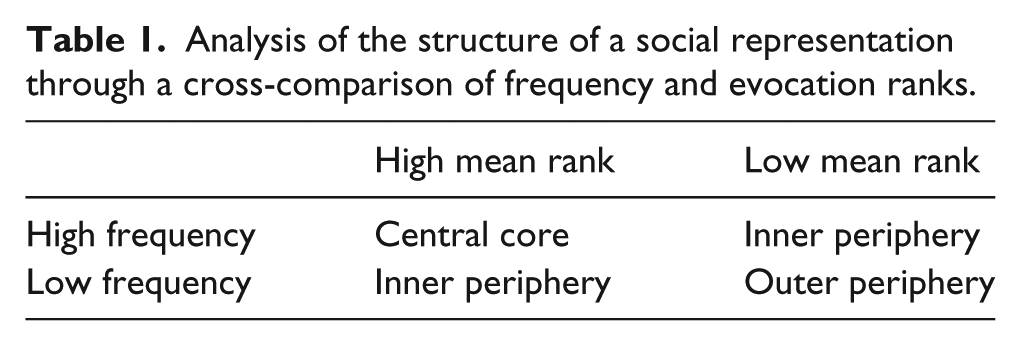
In this way, based on the words used by the respondents, we attributed to each word a rank of 1–3, according to its evocation rank. We also noted the number of times each word appeared. We then performed a lexical and semantic grouping procedure. For the purposes of our analysis, we selected words or semantic fields used by at least 5% of respondents per region under study. This threshold of 5% was chosen according to the methodology used by Salès-Wuillemin et al. (2011): in a free-association word task of 10 words maximum, this study selected the words used by at least 10% of respondents.
This selection method gave us Table 2.
SR analysis in Brittany and Alsace.
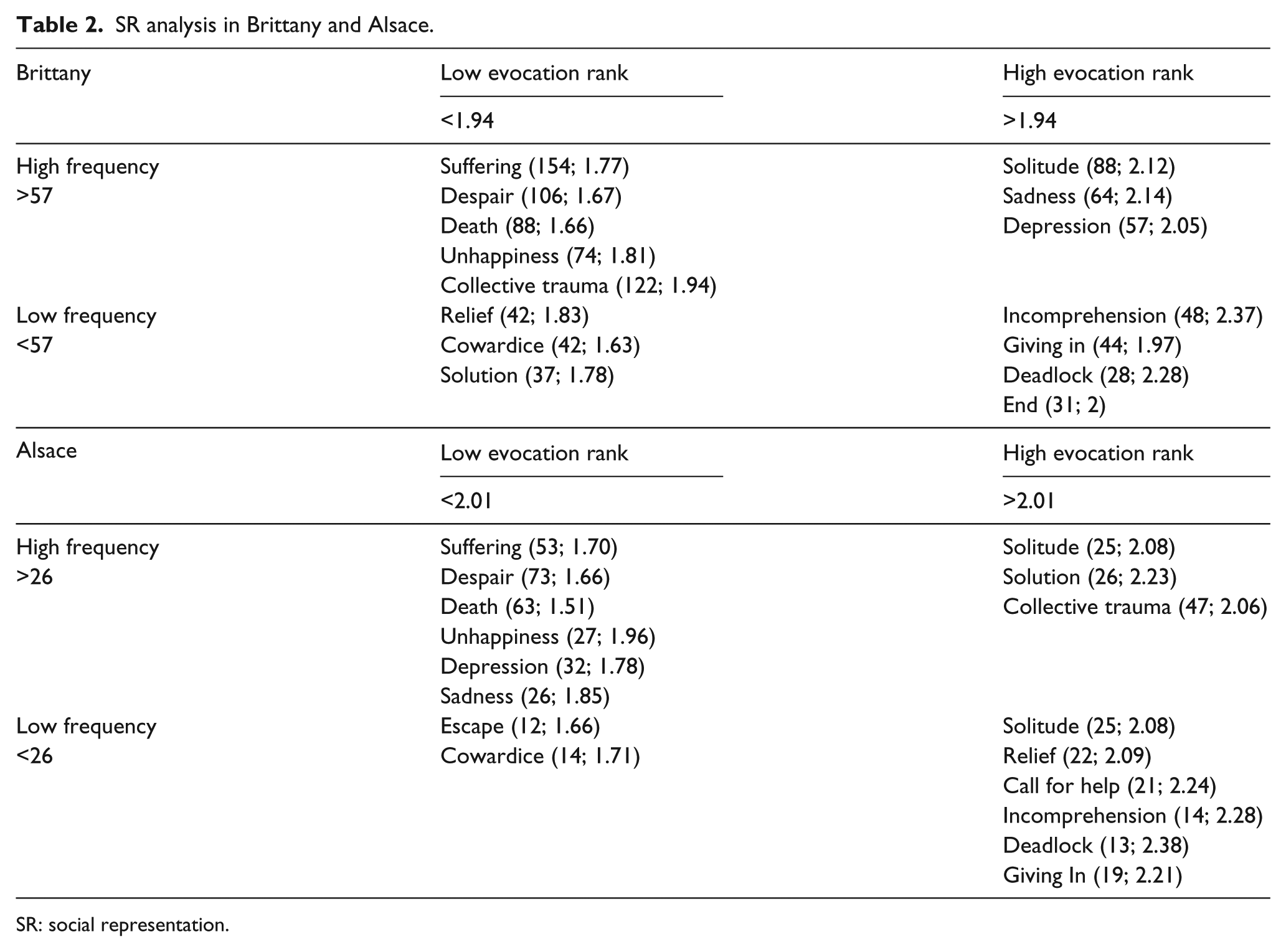
SR: social representation.
For the socio-demographic analysis, we performed a chi-square test. Significant differences are highlighted by an asterisk and p-values are specified.
Results
Groups
During the study period, 545 participants from Brittany and 241 from Alsace completed the questionnaire. The socio-demographic characteristics of the two groups are shown Table 3. Overall, the two groups are similar regarding sex ratio, ages and family structure. Some differences appeared significant: in Alsace, more people with a high educational level answered the questionnaire; there were more children per family in Brittany; there were more people living in houses in Brittany. The latter result can be explained by the density of the population in Alsace and the living area being less important than in Brittany. Another link is about isolation (measured according to the closest neighbor living less than 100 m away): in Brittany, there are more large free areas, while in Alsace, the life in close community reduces this aspect. The Institut National de la Statistique et des Données Economiques (INSEE) explains that there are few little municipalities (<500 habitants) in Alsace and that 25% of the Alsacian population is gathered in the three biggest cities: Strasbourg, Mulhouse and Colmar (INSEE, 2010, 2016a), while in Brittany, 82% of the municipalities are less dense but host 53% of the population, for a global density of population of 119 habitants/km2 (INSEE, 2016b) versus 219 in Alsace.
Socio-demographic analysis.
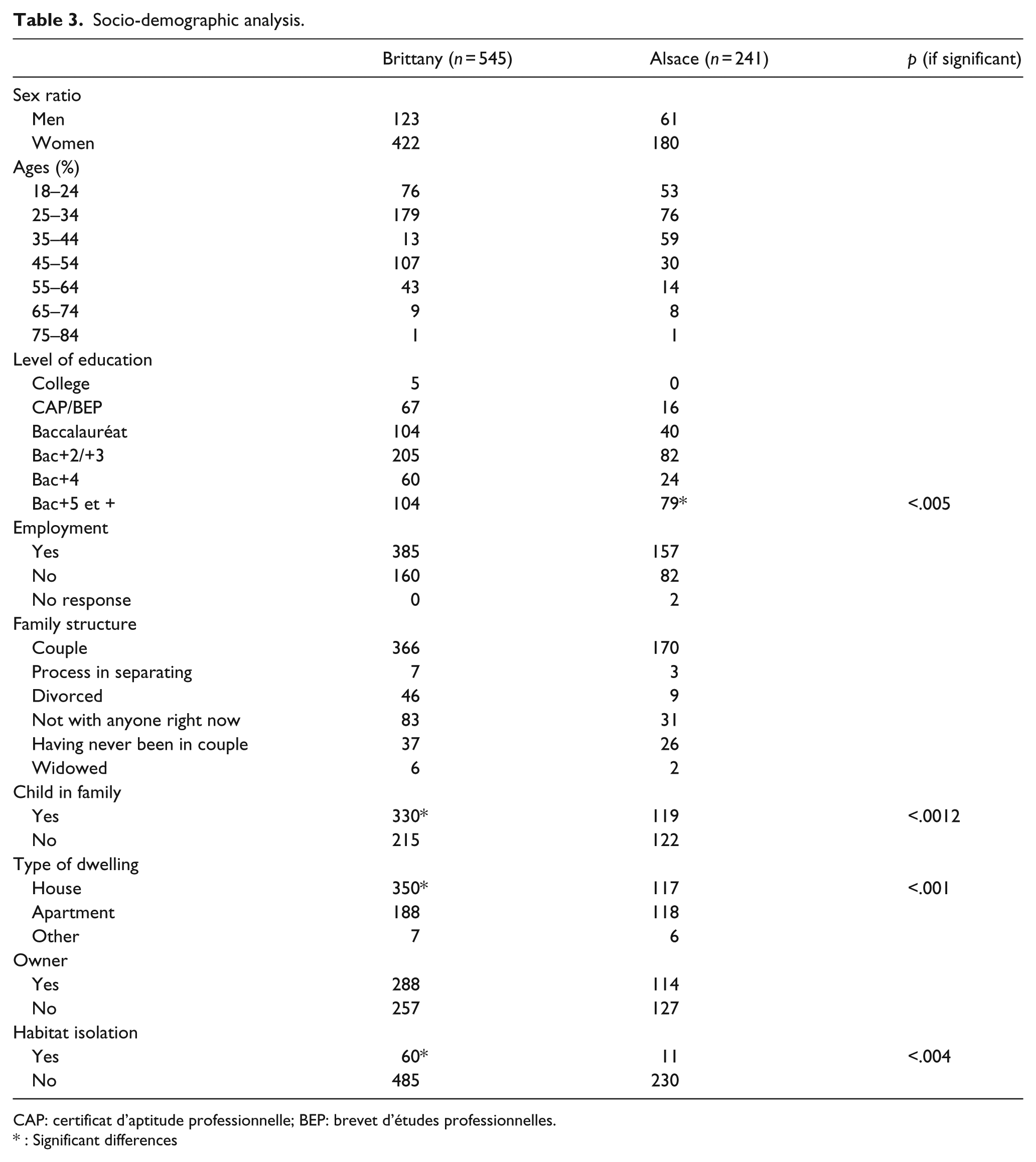
CAP: certificat d’aptitude professionnelle; BEP: brevet d’études professionnelles.
: Significant differences
Another important point is that we can compare the two groups in terms of suicide awareness (Figure 1, Table 4). We could have expected differences in Alsace because of lower suicide rates. The people who responded to our survey were people concerned by the thematic.
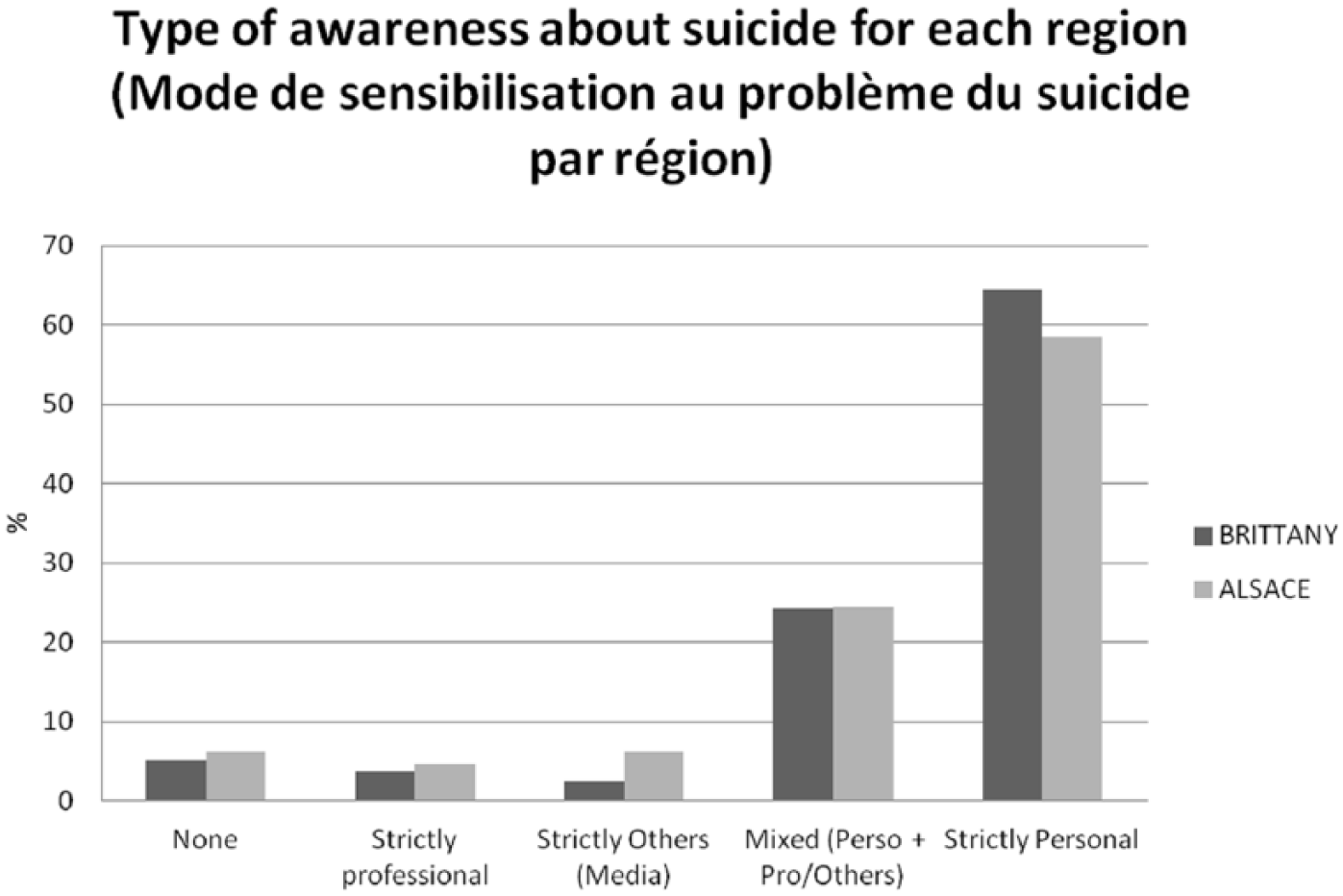
Type of awareness about suicide in each region.
Type of awareness about suicide and suicide attempt.
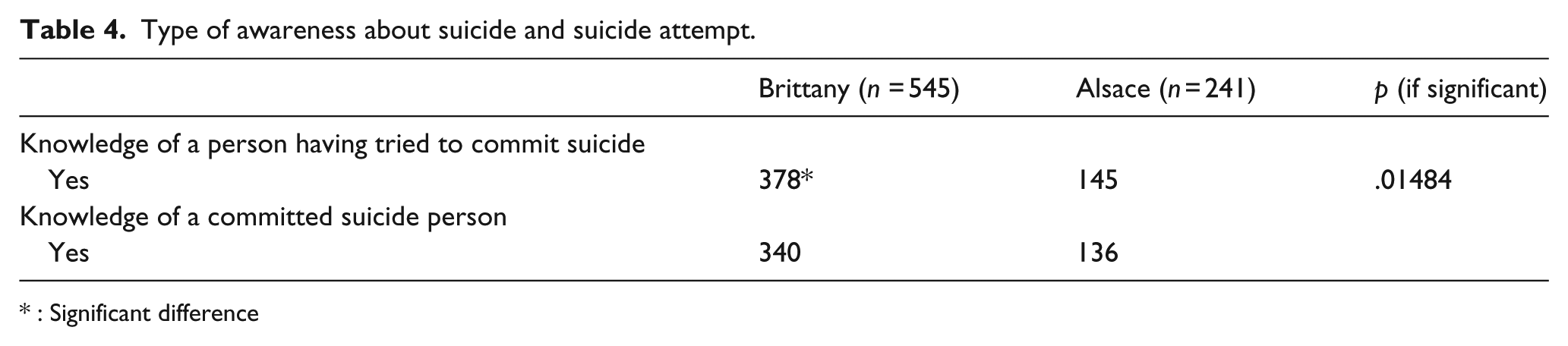
: Significant difference
General analysis
A total of 82% of elements were shared by the two populations under study (Figures 2 and 3). A common set of four terms cited by the participants as an explanation for suicide was found in both CCs. For both populations, suicide is a death following a state of unhappiness and suffering associated with despair. On this point, common sense coincides with the expert’s vision.
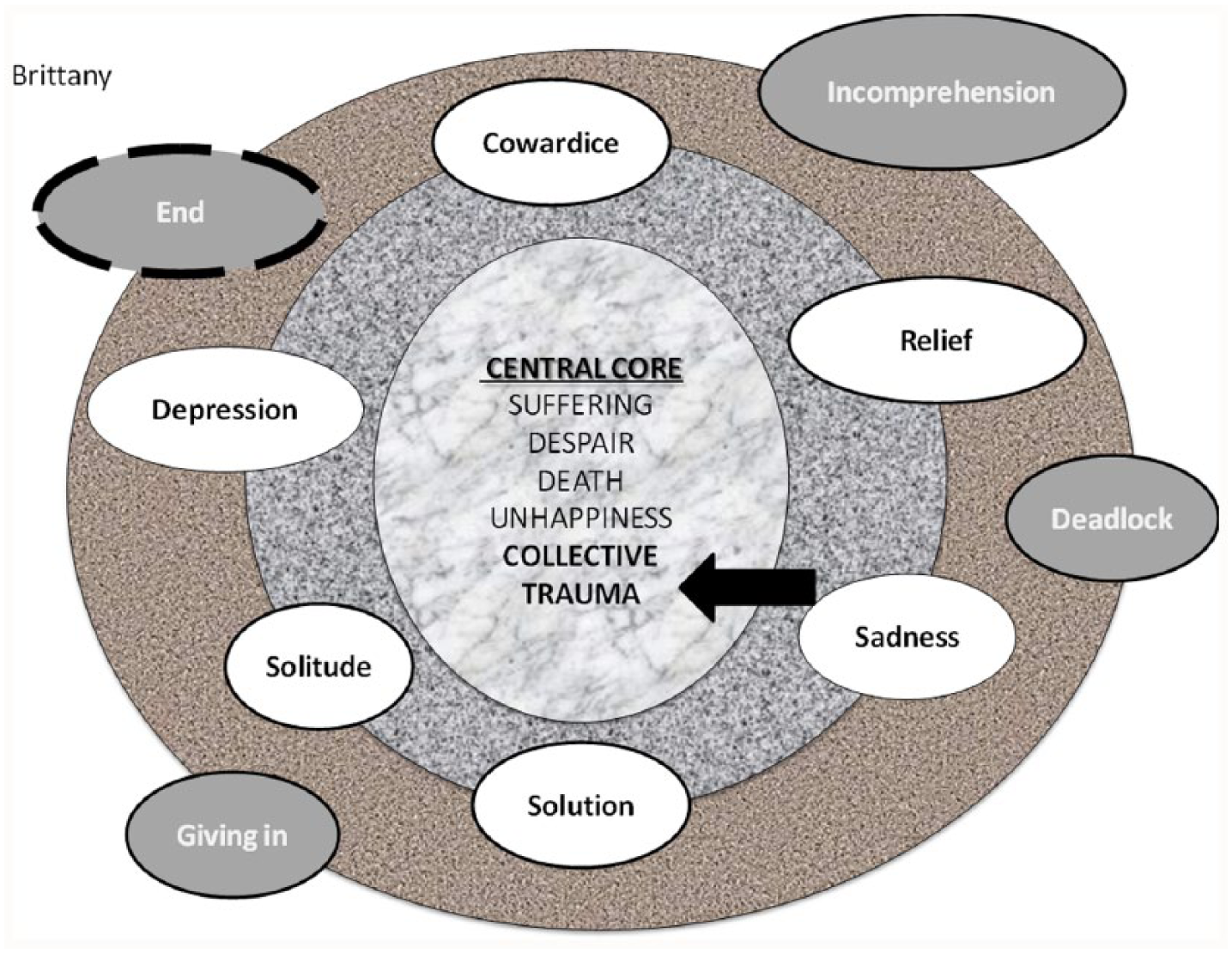
Social Representation System of suicide in Brittany.
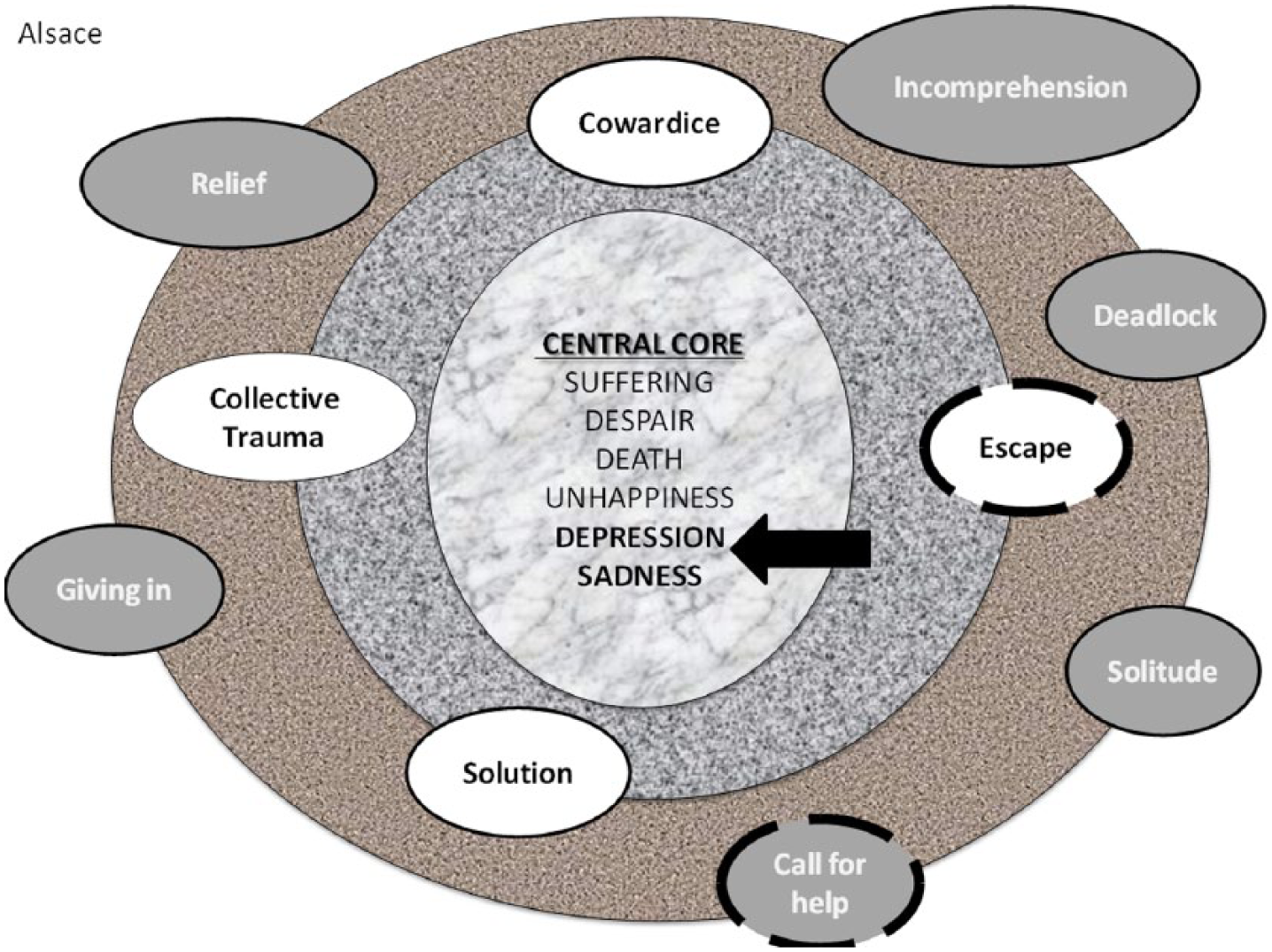
Social Representation System of suicide in Alsace.
CC analysis
Although the major part of the elements was shared, the central component in Brittany was more focused on the traumatic effect of suicide on the social group: on the living. On the contrary, Alsacian participants were rather centered on the sadness and depressive components.
PS analysis
Moreover, only two unshared items appeared in the SR: suicide as a goal and an end in Brittany, while in Alsace, it was perceived as a call for help and an escape from one’s problems.
Discussion/perspectives
… social representation acts as a guide for people’s actions by integrating people’s collective memories with their individual experiences. (Lin et al., 2013, p. 1931)
The aim of this study was to search for differences between SR of suicide in Brittany, which is a region with a high suicide rate, and SR of suicide in Alsace, where the suicide rate is low, in order to explain the collective effects of suicide in Brittany as well as the collective brakes. We can say that SR of suicide is different in Brittany compared to Alsace (Moliner, 1994), although most parts of the elements are shared between the two systems of representation. Three important points already emerge from this work.
Collective traumatic dimension
First of all, in Brittany, collective significance of suicide lies in its traumatic aspects. Yet, Valence (2010) posits that the CC is one of the elements that reflect collective consciousness. Has the population’s confrontation to suicides and suicide attempts, either personal or made by close friends or family, gradually had a collective traumatic effect? Is this collective effect continuing and self-sustaining itself today? How do those traumatic effects translate in terms of behavior? According to Reynders et al. (2015), this could result in stigmatization, lack of distress calls and early access to medical care. Repeated exposure to suicide could also lead to what is more typically described in clinical terms as a traumatic state, including distress, avoidance, detachment, sideration, that can alter the ability of a person to recognize someone else’s or one’s own suffering. This aspect of the data would give us indications on what approach to take in terms of postvention, on the prevention of the psychological trauma, so it neither repeats nor becomes commonplace, and also on the possibility of involving the social group in prevention actions. Reynders et al. (2015) explain that in a region with high suicide rate, as in Brittany, people with a suicidal past develop feelings of shame, depreciation, self-stigmatization and are less inclined to seek for help.
When speaking about prevention, it is necessary to consider not only targeted actions, but also universal measures, in order to bring a collective answer in terms of prevention initiatives. Yet a reluctance to speak about suicide at collective levels in Brittany remains in politics and the media. For example, we were not allowed to publish the survey in free access public newspapers from regional and local authorities.
Individual dimension and link with depression
A second element that was noteworthily evidenced by our study is the place of the depression in suicide SR in Brittany and Alsace: depression was not perceived as a central aspect of the suicide representation in Brittany. Yet, a large corpus of scientific research points out depression as being closely associated with suicide (Bhar, Ghahramanlou-Holloway, Brown, & Beck, 2008; Bradvik, 2003; Chapman, Specht, & Celluci, 2005; Lee, Wong, Chow, & McBride-Chang, 2006; Swan & Potter, 2001 etc.). The study ‘Santé Mentale en Population Générale (Mental Health in the General Population) SMPG’, showed that the term ‘depressive’ is associated, for 75% of respondents, with sadness, isolation and suicide (Roelandt, Caria, Defromont, Vandeborre, & Daumerie, 2010).
In Brittany however, depression is only associated with suicide in the PS. Conversely, does Alsace’s lesser exposure to suicide result in suicide remaining a more individual event, more personal and more specifically associated with depression?
If we look closely at the items found in the SRs of suicide, it may be that the Alsace population has a more global view of the nature of depression and of some of its symptoms: sadness, despair, unhappiness, suffering. As a consequence, we could postulate that Alsacian population is more ready to identify depression, which might facilitate access to health-care services for people suffering from depression. This hypothesis is supported by the presence of the item ‘call for help’. In Alsace, the romantic literary is an important heritage. The poet Johann Wolfgang Von Goethe (1999) described an individual’s progress toward suicide in his very famous ‘Sorrows of the Young Werther’. Romanticism offered a standardized figure of despair and depression, readily available for individual and collective representations. And when elaboration is possible, there is less trauma.
Another specificity of Alsace is the psychiatric and psychoanalytic tradition, partly due to the proximity of Germany, Swiss and Austria that are the home countries of Japsers, Kraepelin, Bleuler, Piaget, Rorschach, Jung, Freud and so on.
It is possible that the collective consciousness in Alsace is still pervaded by this cultural heritage so that depression and psychic care are more accessible and thinkable in Alsace than in Brittany.
The Breton population apportion the same symptoms on different levels: central for suffering and despair, peripheral for sadness and depression.
One way of approaching this could be by understanding how depression is perceived in Brittany, what the word means to the population. Notably, such an exploration could be relevant for the improvement of access to medical care. It seems important to explore the SR of mental illness, psychological suffering and access to medical care, along the same lines as Jodelet (1989) when he was working on madness. The culture in Brittany is of Celtic origin and we can see a traditional idea of health and sickness that pervades today’s collective conception of health care. As a rather caricatural example, we could cite the announcement made by a village, in order to have their despair noticed, that for lack of a general practitioner, a druid would have to take the function upon himself. 2 It was a joke intended to draw the attention on the situation of the village, but it still says something about the conception of medicine and care. Those representations of care and by extension of mental illness are to be studied in Brittany.
Educational and preventive dimensions
Generally speaking, behaviors related to a social object are mainly guided by peripheral representations. In this study, we identified elements that provide hints about how people represent themselves suicide. Resulting prejudice and attitudes may inhibit the comprehension of prevention messages. Regarding attitudes, the professional training method developed by Monique Séguin and Jean-Louis Terra for the Plan National de Prévention du Suicide (National Plan for the Prevention of Suicide), initiated in 2000, calls upon ‘conventional wisdom’ to correct the trainees’ opinions on suicide, making prevention easier. In every region in which a training session takes place, the same stereotypes are used, for instance, ‘suicide is a choice’, ‘killing yourself takes courage’, ‘suicidal people have decided to die’, ‘suicide is hereditary’ and so on. We did not find such concepts among the most frequently cited notions in the two populations (they were in fact mentioned, but not frequently: in Brittany, courage held the 17th place in the number of occurrences, the call for help the 18th, selfishness the 19th, personal choice the 21st, and genetics and heredity were not associated with suicide but only mentioned, in a minor way, among the causes associated with suicide). The current research could be completed by a study of the SRs among groups of people trained to identify and intervene in suicidal crises according to the Séguin/Terra model, using the same instructions as in the two groups (Brittany and Alsace). The aim would be to check whether the training modifies the representation system.
Adapting the content of training sessions to the trainees’ representations could be an important step forward. A spontaneous evocation task, followed by some work on the items named, could be useful. To alter representations, however, it is necessary to modify not only the PS, but also and especially the CC: … the central core controls the meaning and the organization of the entire representation field. It is for this reason that the whole representation is transformed in a radical way if the central core is affected by a change of the meaning or a change of nature (Abric, 1987). Consequently, it is important to find methodological means to ensure its systematic identification. (Guimelli, 1993, p. 556)
Limitation
The extent of the study, although being rather consequent compared to other’s SR studies, is not wide enough to draw definitive conclusions. We carried out a descriptive study of the SR at a time t (Rouquette, 1997). But a logical and statistical analysis of SR is not enough to explain the phenomenon. More studies are needed using narrative contents (interviews, media content analysis, etc.) to go further in the exploration of the SR of suicide (Laszlo, 1997).
Conclusion
The WHO recommends adapting prevention campaigns to the context and culture of each region. Our study has highlighted the relevance of taking into account the territorial dimension in suicide prevention campaigns. Adapting prevention initiatives to an area requires familiarity with its context. This implies collaboration between various disciplines, such as sociology, anthropology, psychiatry and ethno-psychiatry, psychology and so on, and between the research teams.
In Brittany, the high rate of suicide already implied different recommendations for prevention for the different areas of prevention (primary, secondary and tertiary), for instance, to ‘give a positive image of mental health’ (Reynders et al., 2015, p. 10), to undertake more cross-disciplinary studies, to train the general practitioners and other health professionals to spot depressions (Rutz et al., 1989) and suicidal crises (Scouarnec, Kopp-Bigault, Audouard-Marzin, Jaffrelot, & Walter, 2016), to study attitude on suicide and suicide prevention initiatives in Brittany specifically (Brunero, Smith, Bates, & Fairbrother, 2008). We can improve the care of suicidal people, before or after a suicidal attempt (Berrouiguet et al., 2014) and decrease the stigmatization, auto-depreciation, shame and so on.
Our purpose with this study was to open a new field of search in suicidology on the SR of suicide and to keep taking an interest in and questioning what takes place in Brittany, as well as in other regions. Furthermore, we aimed to catch the interest of other research teams in order to further our multidisciplinary approach.
Footnotes
Acknowledgements
Thanks to the Bureau de Traduction Universitaire from the Université de Bretagne Occidentale (UBO) that helped us with the translation. Thanks to Professor Eva Louvet, PhD, Professor of social psychology at Strasbourg University (Unistra) for her precious help. Thanks to Professor Guy Beauchamp, PhD, Professor at the department of psychology and psychoeducation at Université de Québec en Outaouais (UQO) for his help with statistical analysis. This article expands on the poster presented in June 2015 at the International Association of Suicide Prevention World Congress in Montreal (Canada).
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Groupement d’Etudes et de Prévention du Suicide (GEPS). The Bureau de Traduction Universitaire from the Université de Bretagne Occidentale (UBO) was funded by EA 4686 (UBO).