
Abstract
Aim:
Three southern provinces of Thailand, Pattani, Yala and Narathiwat, have been involved in a long period of unrest due to differences between the population in the provinces and the Thai government with regard to language, culture and governance. The objectives of this article are to examine the effects of everyday stressors due to the conflict, including economic stress and migration, as well as the effect of religiosity on the reporting of psychiatric symptoms among adults in the three provinces.
Methods:
Data were drawn from a survey conducted in 2014. The survey included a probability sample of 2,053 Muslim adults aged 18–59 years.Mental health was assessed using World Health Organization’s (WHO) Self-Reporting Questionnaire (SRQ) of 20 questions. Multilevel models were estimated to examine the influence of economic stress due to the conflict, as well as community and individual aspects of migration and religion on mental health.
Results:
The data showed that migration from the household and the community and the economic effects of the unrest were associated with reporting of more psychiatric symptoms among adults in the southern provinces. Religion was related to reporting of fewer psychiatric symptoms at the individual and the community levels.
Conclusion:
The study documented increased reporting of psychiatric symptoms among persons reporting perceived household economic stress due to the conflict and the migration of family members.
Three southernmost provinces of Thailand have been involved in a long period of unrest due to differences between the population in the provinces and the Thai government with regard to language culture and governance. The objective of this article is to examine the effects of everyday stressors due to the conflict, including economic stress and migration, as well as the effect of religiosity on reporting of psychiatric symptoms among adults in the three Thai southern provinces of Pattani, Yala and Narathiwat.
Background
Conflict, economic depression and mental health
Exposure to traumatic events has been found to increase risk of posttraumatic stress disorder (PTSD) as well as depression and other mental disorders (Axinn, Ghirmire, Williams, & Scott, 2013; Miller & Rasmussen, 2010). However, direct exposure to violence has been found to explain only a small part of psychiatric symptoms (Miller & Rasmussen, 2010). In addition to stress due to direct exposure to conflict, everyday tensions related to the conflict such as economic depression and migration of family members may also increase the level of symptoms of mental health including depression, anxiety and other issues (Miller & Rasmussen, 2010). This research focused on the effect of daily stressors on the mental health of people in conflict and post-conflict settings (Miller & Rasmussen, 2010). While direct exposure to conflict may affect mental health, stressful social and material conditions, such as economic hardships caused or worsened by conflict, may also affect mental health.
Migration of family members and mental health
The economy of the provinces in this study has been weakened by the conflict, often leading to the migration of family members. There has been a long tradition of migration for work from these communities, particularly to destinations in Malaysia. This migration may have increased due to the unrest in the area (Jampaklay, Ford, & Chamratrithirong, 2015). Migration has been shown to increase the incidence of psychiatric symptoms of adults left behind in communities (Lu, 2012; Lu, Hu, & Treiman, 2012; Wilkerson, Yamawaki, & Downs, 2009). The tension in a household over economic or other factors that lead to a migration and worry about a household member who is far from home may lead to stress. Migration can also be considered a form of family disruption. In the context of migration of a family member, the absence of key family members may lead to a loss of social support and heightened stress (Lu, 2012). Migration of a family member may diminish reciprocal social support of the kind that may produce positive social and emotional experiences (Cohen & Willis, 1985; Jones, 2015). While many earlier studies of the impact of migration on the household left behind focus on children (Hildebrandt & McKenzie, 2005; Jampaklay & Vapattanawong, 2013) or the elderly (Abas et al., 2013), this study focuses on working age adults who serve as providers for the young and the elderly (Lu, 2012). Furthermore, most studies have looked at the effect of migration at the household level but not at the community level and this study will expand research in this direction.
Religion and mental health
Most villages in the three provinces contain a majority of members who are Muslim and the presence of masjids and practice of the Muslim religion is strong. Religion may be a protective factor for positive mental health due to the benefits received from faith in the religion and the support of the Muslim community. Most of the earlier research on religion and mental health has focused on Christian and Jewish religions and shown inconclusive results. Religion may increase, decease or not affect levels of daily stress (Schieman, Bierman, & Ellison, 2013). Some reviews have posited that the effect is mainly beneficial (Seybold & Hill, 2001). Studies have looked at the effect of religion mainly at the individual and not the community level. One of the positive mechanisms linking religion and mental health may be through social networks (Hill & Butter, 1995; Seybold & Hill, 2001). Religious communities provide opportunities for companionship and involvement in formal social programs that may provide support that may reduce stressors. A religious commitment may also affect lifestyle behaviors leading to better choices for health.
Conflict in the southern provinces
The majority of the population (80%) of the three southernmost provinces of Pattani, Yala and Narathiwat is Muslim. In the 18th century, these provinces had become a center of Islamic learning and commerce (Forbes, 1988/1989). Since these provinces became part of Thailand in the late 19th century, there have been times of relative tension and cooperation with the Thai government (Chalk, 2008; Croissant, 2005; Forbes, 1988/1989). The tension has been related to assimilation to the Thai culture, autonomy and governance, development and other issues. In 2004, there were several attacks by security forces including a major incident at Tak Bai, Narathiwat province. Since then, the unrest has escalated to large-scale violence in all three provinces. In the 8 years after 2004, the area experienced more than 5,500 deaths and 10,000 injured. Chronic violence has remained prevalent in these communities (Chalk, 2008; UNICEF, n.d.).
Hypotheses
This study examines the influence of religion, economic stress and migration on the reporting of psychiatric symptoms of adults in three southern provinces of Thailand. We posit that (1) perceived economic stress caused by the unrest may increase reporting of psychiatric symptoms, (2) migration of household members may increase reporting of psychiatric symptoms among adults left behind, (3) migration at the community level may increase the reporting of psychiatric symptoms of adults left behind, (4) the religious practice of the individual may reduce the reporting of psychiatric symptoms and (5) the religious practice of the community may reduce the reporting of psychiatric symptoms of adults.
Data and methods
Data
This analysis is based on baseline data from an ongoing longitudinal project on Women Migration and the Unrest in the three southernmost provinces (Jampaklay et al., 2015). The survey is a probability sample of Muslims in the three southernmost provinces of Pattani, Yala and Narathiwat. Households were selected using a probability proportional to size (PPS) framework. The survey completed Round 1 data collection in May 2014. The study sample includes Muslim households with at least one woman aged 18–59 years. For the baseline round, in total, 1,102 households were interviewed, covering 5,823 individuals of all ages listed on household rosters. Both an adult woman (N = 1,100) and an adult man (N = 953) were interviewed in households that included adults in the age range of 18–59 years. Informed consent was obtained from all individuals participating in the study. An ethical approval of study procedures was obtained from the human subjects committee of Mahidol University.
Measurement of variables
Dependent variable
Mental health
Mental health was measured using the Self-Reporting Questionnaire (SRQ-20) (World Health Organization, 1994). This is a 20-item measure that has been used in many international studies, including in Thailand (Jampaklay & Vapattanawong, 2013). The questions in the study cover include the domains of depression, anxiety, somatization and other neurotic illnesses. The 20 items used are shown in Appendix 1. The questions were administered by personal interview.
The basic questionnaire was written in Thai language. The SRQ-20 has been administered previously in Thai language, and we used the Thai questions that were used in earlier studies. The people of the southern provinces speak the Melayu and the Thai languages. Interviewers were required to speak both languages. In pretesting, we found that both languages were needed to explain the questions in the interviews. In the interviewer training, we conducted discussions how to explain the questions in both languages, especially the questions about psychiatric symptoms.
Item responses were recorded as binary (yes = 1, no = 0) and cover a 30-day recall period. The items were summed to create a total score (Giang, Allebeck, Kullgren, & van Tuan, 2016; Qadir, Khan, Medhin, & Prince, 2011). In some studies (Harpham et al., 2003; Richardson et al., 2010), a score of eight items has been used as a threshold for treatment although the cut-off point has varied with locale and type of setting (hospital vs community) (Giang et al., 2016). Caution should be used in interpreting the results that use a cut-off score because a cut-off score for this purpose has not been validated for this population.
Independent variables
Village and individual practice of Muslim religion
Respondents were asked how strictly they practice their religion on a 4-point scale from very strictly (4), fairly strictly (3), not very strictly (2) to not strictly at all (1). This first variable was used as a measure of individual religious practice. A second measure, village religious practice, was created by estimating the mean of the individual practice variable within each village.
Village migration level
The number of current migrants from the household per household was coded regardless of destination. We define migration as leaving the home of origin for at least 1 month. This measure ranged from 0 to 5. The village migration level was then estimated by taking the mean of the number of migrants per household within each village. This second measure, the mean of the number of migrants per household, was divided into 10 groups ranging from 0 to 9.
Household migration and remittances were coded using two dummy variables. The reference variable was no migrant from the household:
Migrant with remittances. This variable was coded 1 if the household had at least one migrant and reported some remittances, 0 otherwise.
Migrant with no remittances. This variable was coded 1 if the household reported at least one migrant and did not report remittances, 0 otherwise.
Perceived economic stress due to the unrest
Respondents were asked if the unrest had an effect upon the financial well-being of the household. Responses were coded from 1 to 4 for no effect (1), a little (2), some (3) and to a lot (4).
Total wealth of the household
This is an asset-based measure of household wealth derived from a principal component analysis (Filmer & Pritchett, 2001). The results were divided into 10 groups ranging from 0 to 0 to ease interpretation.
Secular education
Secular education was measured by the number of years completed.
Islamic education
Islamic education was coded with a set of dummy variables including preprimary, primary and lower secondary or higher education, education in a traditional pondok school or informal education. Informal Islamic education was used as the reference category.
Health
The health of each household member was assessed with the question ‘How is the health of this person?’ on a scale from 1 = very poor to 5 = very good.
Gender of respondent
Gender of respondent was coded as 1 = male, 0 = female.
Age of respondent
Age of respondent was coded in single years.
Marital status
Marital status was coded as married with spouse present, married with spouse absent, widowed, divorced or separated, or single. Single was used as the reference category.
Statistical methods
Poisson regression was used because the mental health measures are counts of symptoms. A two-level multilevel framework was used with a random slope at the village level and robust standard errors (Rabe-Hesketh & Skrondal, 2005). Results are presented in terms of incidence rate ratios (IRRs). A result was considered significant if the p value was less than or equal to .05.
Results
Descriptive data
Table 1 shows mean values of variables included in the model by gender of the respondent. The SRQ summary mean was 2.6. On average, females reported more symptoms than males (females 3.09, males 2.21, p < .01). Using an 8-item cut-off, about 8.2% of respondents were in need of treatment (10.4% of women, 6.1% of men). Village religious practice averaged 3.16 and village migration level averaged 4.65. There were no significant gender differences in these variables nor in the presence of a migrant with or without remittances, perceived economic stress due to the unrest, household wealth, secular education, age and strictness of practice. There were gender differences in Islamic education: fewer women than men attended a pondok and more women than men had Islamic education at the lower secondary level or higher. On average, respondents were reported to be in good health, with men reporting slightly better health. Both men and women averaged about 40 years of age. Although most of the sample reported their status as married, spouse present, there were small gender differences in the sample. Most notably, more women reported being widowed (9% women, 1.5% men).
Means of variables included in models.
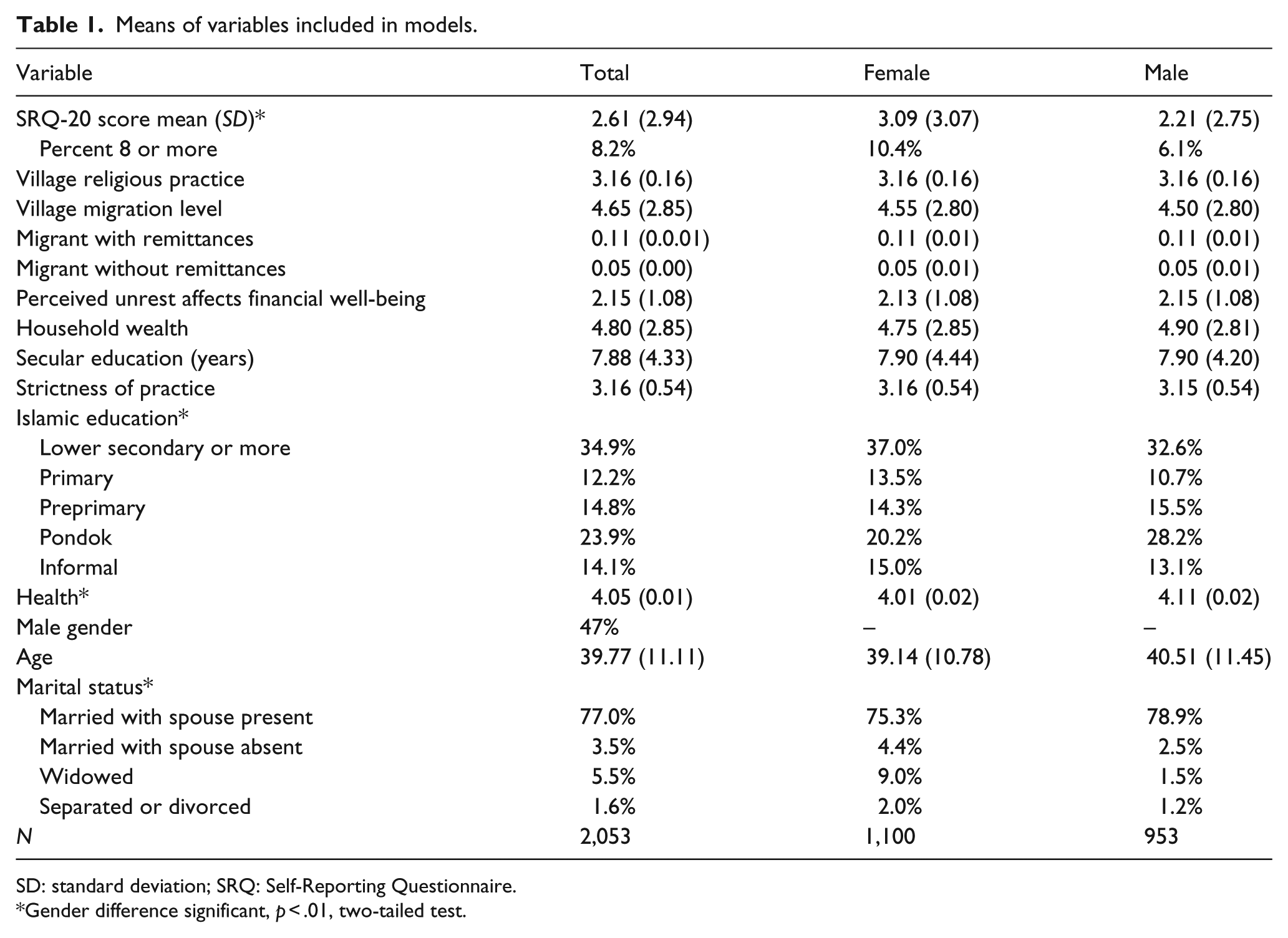
SD: standard deviation; SRQ: Self-Reporting Questionnaire.
Gender difference significant, p < .01, two-tailed test.
Model results for total SRQ-bivariate models
Table 2 shows the results of bivariate Poisson models of the relationships between the independent variables and the SRQ total sum for the total, female and male respondents. Village religious practice had a negative relationship with the SRQ sum though it was significant only for females (IRR = 0.45, 95% confidence interval (CI) = 0.24, 0.83, p = .01). The village migration level was positively associated with the reporting of psychiatric symptoms for the total population (IRR = 1.05, 95% CI = 1.01, 1.10, p = .01) and the female population, but not for the male population. Having a current migrant sending remittances compared to not having a current migrant was associated with reporting more symptoms for the total (IRR = 1.24, 95% CI = 1.15, 1.35, p = .00) as well as both the male and female populations. Having a current migrant and not receiving remittances compared to not having a migrant was also associated with reporting of more symptoms for the total (IRR = 1.33, 95% CI = 1.19, 1.47, p = .00) as well as the female and male populations. Perceived unrest affecting financial well-being was also positively related to the reporting of symptoms for the total (IRR = 1.14, 95% CI 1.06, 1.23, p = .00) as well as both the male and female populations. Increased household wealth was significantly associated with a reduced number of symptoms for the total and female populations. Secular education was associated with a reduced number of symptoms for the male population.
Bivariate Poisson models of factors related to total SRQ-20 score.

IRR: incidence rate ratio; SRQ: Self-Reporting Questionnaire; CI: confidence interval.
Strictness of practice of the Islamic religion was not associated with reporting of symptoms. Many of the Islamic education variables were not significantly related to reporting of symptoms. However, primary Islamic education was related to an increased reporting of symptoms and the pondok to a decreased reporting of symptoms for the total population. Male gender was associated with reporting of fewer symptoms (IRR = 0.69, 95% CI = 0.65, 0.73, p = .00). Good health was associated with a reduced reporting of symptoms for the total, male and female populations. Marital status was also associated with reporting of symptoms only for males. In the male population, being married with spouse absent compared to being single was associated with fewer symptoms.
Table 3 shows the results from multivariate Poisson regression models with the total SRQ score as the dependent variable. Looking first at the model for all respondents, the level of religious practice in the village was negatively related to reporting of psychiatric symptoms. The IRR was 0.42 (95%CI = 0.21, 0.81, p = .01). This variable was significant for females and for males. The village migration level was related to an increased reporting of symptoms (IRR = 1.06, 95%CI = 1.02, 1.11, p = .00) in the model for all respondents. In the models for males and females, the result was only significant for females. If the household had a current migrant, more symptoms were reported for households receiving remittances (IRR = 1.22, 95% CI = 1.12, 1.32, p = .00) and for households not receiving remittances (IRR = 1.29, 95% CI = 1.16, 1.44, p = .00) than for households without a migrant. This migration result was significant for all respondents as well as for both males and females. If the household reported that the unrest had affected the financial well-being of the household, more symptoms were reported in the model for all respondents. The IRR was 1.14 (95% CI = 1.11, 1.17, p = .00). This result on financial well-being was significant for all respondents as well as for both males and females. Household wealth had a small significant negative effect on the reporting of symptoms for all respondents. This result on household wealth was significant for females but not for males.
Multivariate Poisson regression model of factors related to the summary SRQ-20 score by gender.
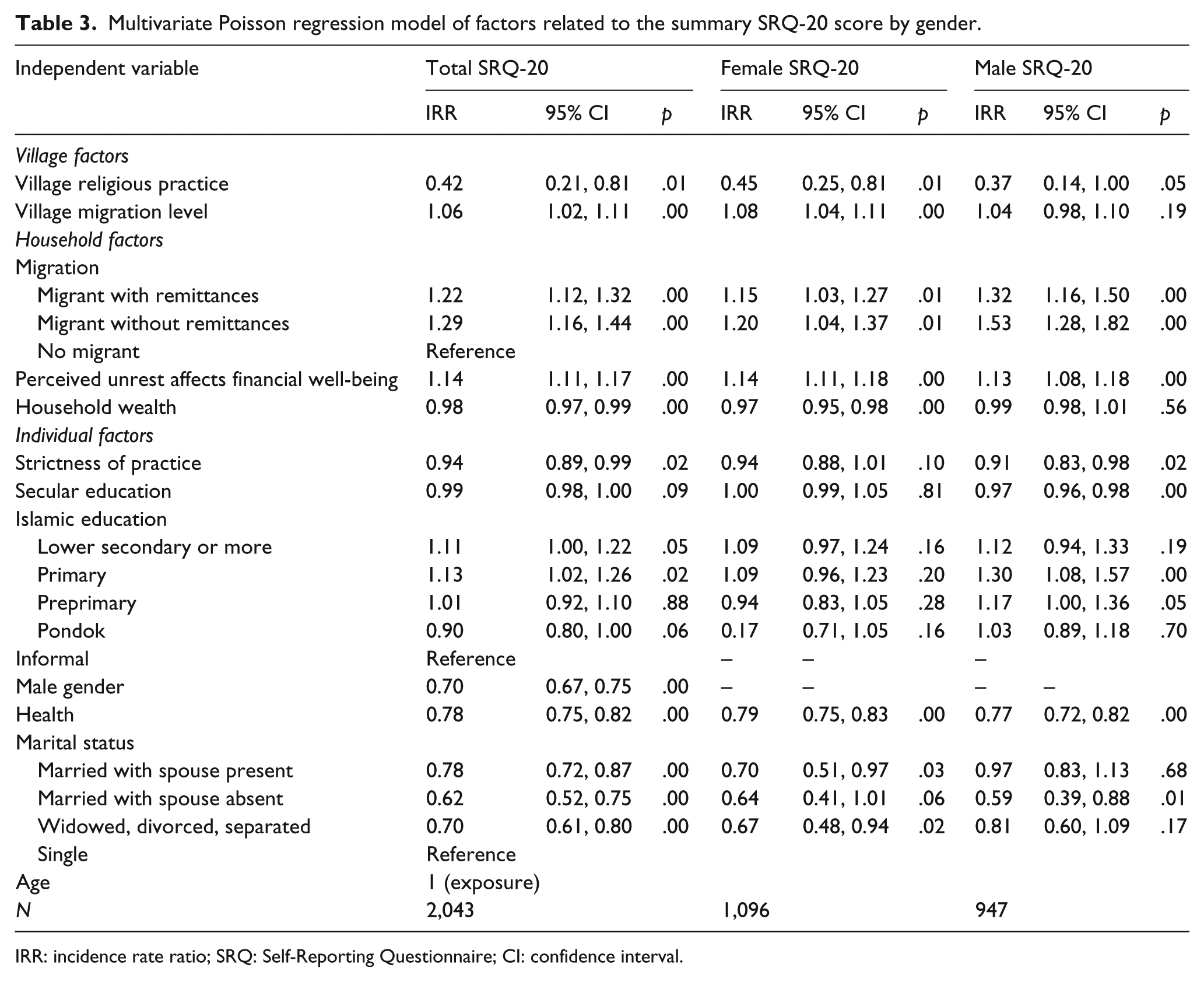
IRR: incidence rate ratio; SRQ: Self-Reporting Questionnaire; CI: confidence interval.
Considering the individual factors, the strictness of individual religious practice was associated with a reduced reporting of symptoms (IRR = 0.98, 95% CI = 0.91, 0.99, p = .00) for all respondents, though this result was significant for males but not females. Secular education was negatively related to the reporting of symptoms for males, but not for female or for all respondents. Lower secondary and primary Islamic education were related to an increased reporting of symptoms for all respondents. None of the Islamic education variables were significant for females, although primary and preprimary Islamic education were related to an increased reporting of symptoms for males. Those with better health (both males and females) and male respondents reported fewer symptoms of mental illness. Fewer symptoms were also reported among all respondents by those married with spouse present, married with spouse absent and those who were widowed, separated or divorced compared to those who were single.
Discussion
In this analysis of factors related to mental health, we found some evidence that migration from the household and the community has affected the reporting of psychiatric symptoms among adults in the southern provinces. An insight from this research is the influence of migration both at the community and the individual levels on mental health. More symptoms of mental illness were reported by persons living in villages with higher levels of migration as well as from households with a current migrant. The experience of losing a household member to migration increased the reporting of symptoms of mental health, regardless of the receipt of remittances. The absence of household members as well as other members of the village may affect the levels of social support in the household and the village leading to increased psychiatric symptoms. This work adds to earlier studies in China, Indonesia and Mexico that showed detrimental effects upon the mental health of adults remaining at home in migrant households (Jones, 2015; Wilkerson et al., 2009; Lu, 2012; Lu et al., 2012).
Although the effect of having a current migrant from the household was related to an increased reporting of symptoms among both male and female respondents, the village level effect was stronger for women. This suggests that women’s lives may be more affected by the absence of community members than males’ lives.
This research also adds to the large international literature on religion and mental health. While studies of religion have shown mixed effects on individual health, most have focused on Christian or Jewish religions. This study examined the effects of the practice of the Muslim religion at both the individual and the community levels, providing theoretical insight into how religion can affect mental health. The strictness of practice in the village had a positive effect on mental health. This relationship was found for the total SRQ-20 score for both genders. The village level effect may reflect a greater closeness of social networks and social support within the villages that benefits both men and women.
Strictness of practice at the individual level had a significant effect on reporting of psychiatric symptoms for the models for all respondents and for males. Male Muslims in the southern provinces gather weekly for a Friday prayer while females may practice their religion more as an individual or a family. This weekly gathering of males may increase the psychological benefits they receive both from the individual prayer and from the increased social support they may obtain from their weekly Friday prayer.
If the respondents reported that the unrest had affected the financial status of the household, more psychiatric symptoms were reported. This was true for the total SRQ score for both genders. Hence, perceived daily economic stressors due to the unrest were related to an increase in the number of psychiatric symptoms reported. The living conditions created by conflict, in addition to the effects of direct exposure to violence, can affect the mental health of a population (Miller & Rasmussen, 2010).
Although secular education did not have a significant effect upon the SRQ total or factor scores for the total population, we did find a positive effect of secular education for males but not females on the total score. Secular education can give an individual an advantage in the Thai labor market. This advantage may have had a stronger effect for males. The multivariate results were not consistent for different levels of Islamic education. Those who were married with spouse present, married with spouse absent, widowed, divorced or separated reported fewer symptoms than those who were single.
One limitation of this study is that it is a cross-sectional sample. This limits our ability to control for unobserved differences between households with different migration statuses. We also do not have direct measures of stress or social support or information on how these factors may change over time. Needed are further studies with longitudinal designs.
Nonetheless, the study has documented some negative consequences for the presence of psychiatric symptoms from perceived economic depression due to the conflict and the migration of family members. The effects of migration and religion were seen at the village and the individual levels. This finding provides insight into the possible effect of these processes on mental health. Migration of family members for work is a common occurrence in Asia and many parts of the developing world. Further longitudinal studies should be conducted in international settings to examine the influence of migration on the mental health of adults in the communities left behind.
Footnotes
Appendix
SRQ-20.

| Yes | No | ||
|---|---|---|---|
| SRQ1 | Do you often have headaches? | 1 | 0 |
| SRQ2 | Is your appetite poor? | 1 | 0 |
| SRQ3 | Do you sleep badly? | 1 | 0 |
| SRQ4 | Are you easily frightened? | 1 | 0 |
| SRQ5 | Do your hands shake? | 1 | 0 |
| SRQ6 | Do you feel nervous, tense or worried? | 1 | 0 |
| SRQ7 | Is your digestion poor? | 1 | 0 |
| SRQ8 | Do you have trouble thinking clearly? | 1 | 0 |
| SRQ9 | Do you feel unhappy? | 1 | 0 |
| SRQ10 | Do you cry more than usual? | 1 | 0 |
| SRQ11 | Do you find it difficult to enjoy your daily activities? | 1 | 0 |
| SRQ12 | Do you find it difficult to make decision? | 1 | 0 |
| SRQ13 | Is your daily work suffering? | 1 | 0 |
| SRQ14 | Are you unable to play a useful part of life? | 1 | 0 |
| SRQ15 | Have you lost interest in things? | 1 | 0 |
| SRQ16 | Do you feel that you are a worthless person? | 1 | 0 |
| SRQ17 | Has the thought of ending your life been on your mind? | 1 | 0 |
| SRQ18 | Do you feel tired all the time? | 1 | 0 |
| SRQ19 | Do you have uncomfortable feeling in your stomach? | 1 | 0 |
| SRQ20 | Are you easily tired? | 1 | 0 |
Acknowledgements
The authors wish to express their gratitude to all respondents who were willing to share their information with us and their views albeit having to struggle through the unrest on a daily basis. The authors cannot thank them enough.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Mahidol University under the fiscal year 2014 budget, contract number 70.