
Abstract
Background:
There is a growing understanding of the importance of the social factors of posttraumatic stress disorder.
Aims:
This study expands research on association between posttraumatic stress and social factors by introducing the measure of the acceptance of social changes and evaluating possible links between posttraumatic stress disorder symptoms and acceptance of social changes.
Methods:
A general population sample (n = 778) aged from 18 to 89 years (M = 40.2) from Lithuania participated in our study, of whom 68% reported exposure to traumatic events. Posttraumatic stress reactions were measured with the Impact of Event Scale – Revised (IES-R), and acceptance of social changes was measured with the Acceptance of Social Changes Instrument (SOCHI) developed by the authors of this study.
Results:
About 8% of the participants had a potential posttraumatic stress disorder (PTSD) diagnosis. Acceptance of social changes was negatively associated with posttraumatic stress. PTSD was related to lower acceptance of social changes (d = .61). Structural equation model (SEM) revealed the mediating role of PTSD for acceptance of social changes following trauma exposure.
Conclusion:
Findings of our study indicate that the acceptance of social changes might be an important psychosocial factor of PTSD.
Introduction
There is a growing understanding of the importance of social factors of trauma and posttraumatic stress disorder (PTSD). Evidence from meta-analytic studies revealed that the lack of social support is one of the key predictors of PTSD in the populations exposed to trauma (Ozer, Best, Lipsey, & Weiss, 2003). New concepts and measures, such as social reconciliation (Ajdukovic, 2007), social acknowledgment (Maercker & Mueller, 2004) and disclose of trauma (Bedard-Gilligan, Jaeger, Echiverri-Cohen, & Zoellner, 2012) among the others, have been introduced recently, providing new research directions for exploring psychosocial predictors of PTSD. Furthermore, new social theories of trauma and PTSD, which emphasize the dynamic interaction between the individual reactions to trauma and the social context of the individual, community and societal levels, have been proposed recently (Maercker & Horn, 2013).
Humans are living in a constantly changing physical and social world, and they need to deal with the dynamic nature of social context. We can assume that some individuals would be more ready to accept social changes and others would be resistant to changes (Oreg et al., 2008). Adjustment to social changes is particularly important in the context of trauma. Large-scale traumas, such as wars, political violence, terror attacks, do shatter social structures and societies, are changed in the aftermath. Communities might be destroyed, people lose trust and may question the supportive role of others (Ajdukovic, 2007). The recovery of community after large-scale interpersonal violence and disaster might be related to significant changes in society (Epping-Jordan et al., 2015), and traumatized individuals in a post-conflict or post-disaster community might be facing difficulties in accepting changes.
We propose that acceptance of social changes is related to PTSD symptoms based on the recent research and theoretical formulations of the role of the social context of PTSD (Maercker & Horn, 2013). Acceptance of social changes differs from social support and other known social factors of trauma and PTSD in several ways. Social support research is focused on the interaction of the individual with others in a group, and measures of perceived, received or provided social support (Prati & Pietrantoni, 2010). With a focus on the interpersonal level, social support research does not capture community or social levels. Acceptance of social changes extends the list of trauma-related social factors with an appreciation that the individual is an active agent in a society and is reacting to social changes on cognitive, behavioral and emotional levels.
We could not identify an available instrument for measuring acceptance of social changes. Oreg (2003) proposed a 17-item self-report Resistance to Change Scale, which have been validated in 17 cultures recently (Oreg et al., 2008). The Resistance to Change Scale measures resistance as a dispositional personality trait, and includes emotion reaction, cognitive rigidity, short-term focus and routine seeking subscales. Resistance to Change Scale (Oreg, 2003) does not include social contextual items and thus is not suitable for research on acceptance of social changes. Considering the lack of measures in this field, we developed a brief 5-item Acceptance of Social Changes Instrument (SOCHI) for the assessment of the acceptance of social changes. This new instrument measures individuals’ social cognitions toward changes on the societal level and perceived adjustment to social changes. We aimed to explore the relationship between the PTSD symptoms and acceptance of social changes in a general population sample in Lithuania in our study. We hypothesized that acceptance of social changes might be associated with PTSD symptoms.
Methods
Participants and procedures
In total, 778 adult participants aged from 18 to 89 years (M = 40.2, SD = 17.85) from the general population in Lithuania participated in this study. The sample consisted of 58% (n = 450) women. In all, 38% (n = 295) of participants had university education. We aimed to collect data from a sample with demographic composition (age, gender, education, urban/rural) similar to the Lithuanian Housing and Population Census data from the year 2011 (Statistics Lithuania, 2013) using a quota sampling. Data were collected by 5 PhD level psychologists and 13 trained and supervised psychology students (5 undergraduates, 6 clinical psychology master’s program students and 2 PhD students) across Lithuania. Participants were approached and invited to participate in the study in a community setting: either at home or in a work place. After introduction of the study and written consent, participants were asked to fill-in self-report questionnaires in Lithuanian language. In all, 87% of invited participants agreed to participate and completed the study.
Measures
Posttraumatic stress symptoms
The Impact of Event Scale – Revised (IES-R) (Weiss & Marmar, 1997) was used to assess PTSD symptoms. The IES-R is a 22-item self-report scale widely used in a traumatic stress research. The IES-R is based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed., DSM-IV) criteria for PTSD (American Psychiatric Association, 1994). Participants were instructed to indicate experience of PTSD symptoms during the last week. High validity and reliability of the IES-R have been reported in many cultures (Weiss, 2004). Various scoring systems have been reported for the IES-R. We used a scoring system developed by Weiss and Marmar (1997) with a scale from 0 (Not at all) to 4 (Extremely) and a 5-point scale (0–4) in our study. We computed the total score of the IES-R as a mean of the responses to each item, with a range from 0 to 4. The Lithuanian language version of the IES-R scale was validated in a previous study in a sample of 403 young adults aged from 18 to 41 years from a general population exposed to various traumatic events (Kazlauskas, Gailienė, Domanskaitė-Gota, & Trofimova, 2006). Good psychometric properties of the Lithuanian version of IES-R were reported with Cronbach’s α = .93 for the total scale (Kazlauskas et al., 2006). Internal consistency was high (α = .96) in our sample for the total IES-R scale. While the authors of the IES-R (Weiss & Marmar, 1997) do not provide cutoffs for the diagnosis of PTSD, several studies provided the cutoffs for the potential PTSD identification. Participants were assigned to the PTSD group based on the cutoff of 1.5 for the total IES-R scale as it was proposed by Creamer, Bell, and Failla (2003).
Trauma exposure
The Brief Trauma Questionnaire (BTQ) is a self-report measure of trauma exposure developed by Schnurr, Iii, Vielhauer, Findler, and Hamblen (2002). Originally, the BTQ was an interview version proposed as the Brief Trauma Interview, and it was further revised into a self-report instrument for screening of exposure to lifetime traumatic events (Schnurr et al., 2002). The list of 10 traumatic events, including serious accident, war zone, disaster, sexual abuse, life-threatening illness, physical attack, abuse in childhood, witnessing an injury or death are included in the BTQ. The BTQ was used in several studies, including large population sample studies (Kubzansky et al., 2014). A Lithuanian language version of the BTQ (Kazlauskas & Želvienė, 2015) for trauma exposure screening is available. We used the BTQ to identify individuals in the sample who experienced at least one potential lifetime traumatic event, and also for assessment of accumulative lifetime traumatic events by summing up the number of experienced traumatic events for each participant. The score of the BTQ ranged from 0 to 10.
Acceptance of social changes
Acceptance of social changes was measured with a self-report SOCHI developed by the authors of this study. The proposed new instrument consists of five items (Table 1) related to a person’s attitudes toward social changes. Three items are about changes in the country, one item is about positive orientation toward the past and one includes perceived adjustment to the social changes. Participants were asked to indicate how much they agree or disagree with each item on a 5-point scale from 1 (Completely disagree) to 5 (Completely agree). The SOCHI items 2–5 were reversed and recoded from 1–5 to 5–1 scale for calculation of the total SOCHI score and further analysis. The total score of the SOCHI is a sum of all item responses and can range from 5 to 25. The higher SOCHI scores indicate that a person is accepting social changes easier, while lower scores indicate that a person is reluctant to accept social changes.
Items of the Acceptance of Social Changes Instrument (SOCHI) (n = 778).
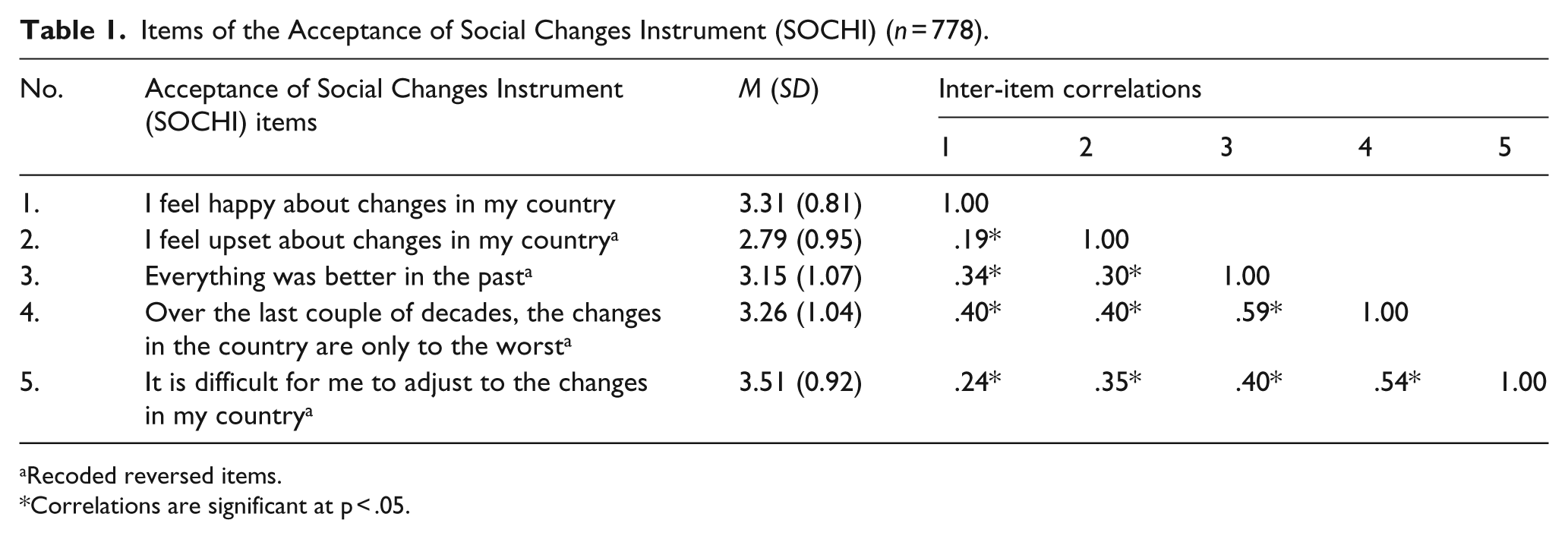
Recoded reversed items.
Correlations are significant at p < .05.
Data analysis
The Statistical Package for the Social Sciences (IBM SPSS® Statistics version 23.0) and IBM AMOS 23.0.0 software were used for data analyses. Confirmatory factor analysis (CFA) was performed for exploration of the SOCHI factor structure. Structural equation model (SEM) with PTSD as a mediating factor for SOCHI following trauma exposure was tested. Three main variables of this study were included in this model: (1) trauma exposure, (2) posttraumatic stress symptoms and finally (3) acceptance of social changes as a latent variable. Comparative fit index (CFI) ⩾ .90 and root mean square error of approximation (RMSEA) ⩽ .08 were used as goodness-of-fit indexes for model fit statistics (Kline, 2011). We report chi-square for the models, but did not use it as relevant goodness-of-fit index for CFA and SEM because of the large sample size. Missing data were handled by excluding cases with missing values in statistical analyses.
Results
Exposure to traumatic events
Exposure to at least one lifetime traumatic experience was reported by 68% (n = 529) of our sample. The average number of experienced traumatic events was 1.6 (SD = 1.63, range: 0–8). Prevalence of the potentially traumatic events in the sample was as follows: physical assault (30.1%), serious accident (27.8%), abuse in childhood (22.0%), serious injury (19.2%), witnessed serious injury of someone (14.8%), death of close family member or friend (14.1%), natural or technological disaster (11.2%), life-threatening illness (10.5%), sexual abuse (5%) and war zone experiences (3.9%). The average IES-R score in the sample exposed to lifetime traumatic events was 0.56 (SD = 0.73, range: 0–3.82).
Psychometric properties of the SOCHI
The mean score of SOCHI scale in the total sample was 16.02 (SD = 3.44, range: 5–25). Internal consistency of SOCHI was acceptable (α = .76) in our sample. SOCHI inter-item correlations were significant (p < .01) for all items and ranged from .19 to .59 (Table 1). CFA supported single-factor solution with all five SOCHI items included in one factor with a good model fit indexes χ2 (5) = 17.01, p < .01, RMSEA = .056, CFI = .99. Factor loadings for the SOCHI items ranged from .47 to .89. SOCHI scores were negatively associated with age of the participants (r = −.28, p < .001).
Associations between PTSD symptoms and acceptance of social changes
IES-R was associated with the accumulative number of lifetime traumatic events (r = .23, p < .001). Posttraumatic symptoms (IES-R) and acceptance of social changes (SOCHI) were negatively correlated (r = −.23, p < .001) in the subsample of trauma-exposed participants. The association between IES-R and SOCHI was significant controlling for age (partial correlation, r = −.21, p < .001), indicating little age effect on the strength of the relationship between posttraumatic stress symptoms and acceptance of social changes. No significant association was found between SOCHI and lifetime trauma exposure measured by the reported number of lifetime traumatic events (r = .08, p = .07).
Relationships between trauma exposure, posttraumatic stress symptoms and acceptance of social changes were further analyzed in the SEM model with PTSD as a mediating factor for acceptance of social changes included in the model. The model’s goodness-of-fit indexes supported the proposed model with good data fit (χ2 (13) = 39.59, p < .01, RMSEA = .069, CFI = .96). Trauma exposure was associated with posttraumatic stress symptoms in a SEM model (Figure 1). We also identified indirect effects of trauma exposure on acceptance of social changes in the model with a significant mediating effect of PTSD on acceptance of social changes (Figure 1).

Structural equation model of posttraumatic stress and acceptance of social changes. All parameters in the model are significant at p < .01, except ns.
Acceptance of social changes in PTSD versus non-PTSD groups
In a further exploration of an association between PTSD and SOCHI, we identified a group of participants with potential PTSD. About 8% of total sample (n = 65, 27 men and 38 women) were assigned to the PTSD group based on high PTSD symptoms scores on the IES-R scale (⩾ 1.5). The mean age of the PTSD group participants was 39.60 (SD = 17.22, range: 18–76). The PTSD group was of a similar age (t(772) = .28, p = .77) and gender composition (χ2 (1, n = 778) = 1.92, p = 1.00) to the rest of the sample. The most prevalent traumatic events in the PTSD group were as follows: serious accident (48.1%), physical assault (46.7%), serious injury (32.8%), witnessing serious injury of someone (31.4%), death of a close family member or friend (30.1%) and childhood abuse (28.4%).
IES-R score in the PTSD group was 2.07 (SD = 0.52). The average SOCHI score in the PTSD group was 14.11 (SD = 3.49), 95% confidence interval (CI): 13.22–15.00, and non-PTSD group the SOCHI was 16.18 (SD = 3.39), 95% CI: 15.93–16.44. We found that the PTSD group had significantly lower scores of the SOCHI in comparison to non-PTSD group (t(759) = 4.61, p < .00) (Figure 2). The mean difference was 2.07, 95% CI: 1.18–2.95, and the effect size for the group differences for SOCHI was medium (Cohen’s d = .61).
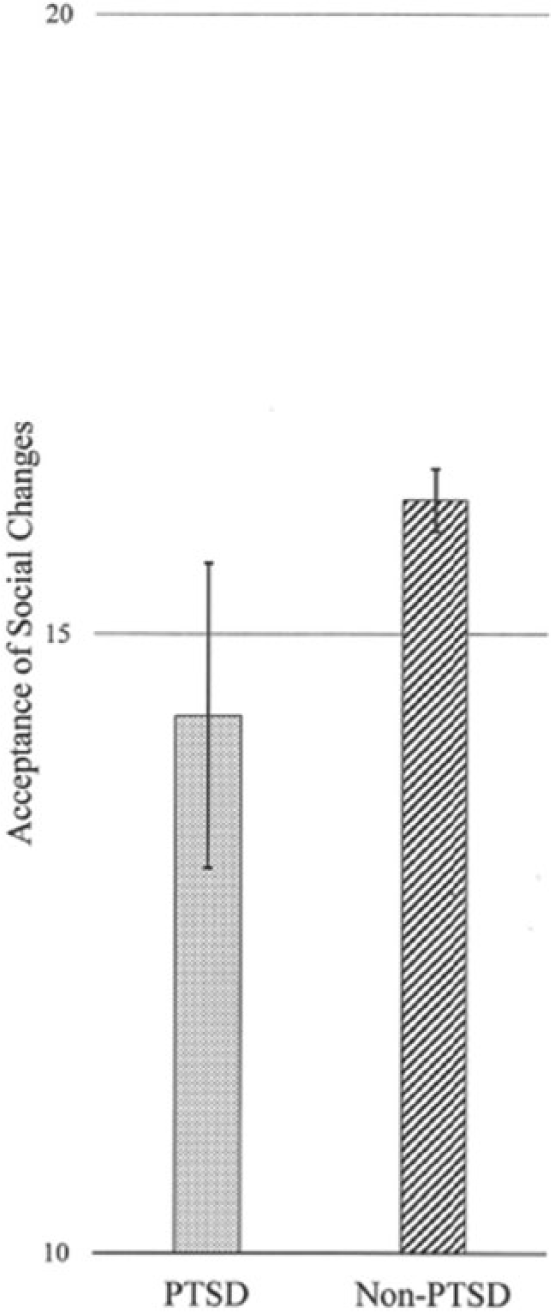
Acceptance of social changes in PTSD and non-PTSD groups.
Discussion
Our study is one of the first to analyze the relationship between posttraumatic stress and acceptance of social changes. It contributes to a better understanding of interpersonal and social factors of PTSD and is in line with research which focuses on the role of social context in mental health, and particularly in trauma and PTSD (Maercker & Horn, 2013). Our findings indicate that PTSD is linked to negative attitudes toward social changes, and thus it might be more difficult for a person with a PTSD to accept social changes in a community or society. Individuals in society are constantly challenged to adjust to social changes. Our findings demonstrate that traumatized individuals with PTSD reported lower levels of acceptance of social changes. The SEM analysis supported the idea that acceptance of social changes might be affected by the higher levels of PTSD. Furthermore, we could assume that a negative attitude towards social changes consequently might be related to adjustment problems and impaired psychosocial functioning.
The findings from our study are relevant not only as basic research results, but they also provide guidelines for clinicians who meet PTSD patients in their clinical practice. Our results show that addressing the issue of adjustment to social changes might be relevant to the individuals with PTSD. However, further studies are needed to explore the dynamics of acceptance of social changes in a process of trauma recovery and therapy. Implications of this study might be important for the post-conflict countries with high prevalence of PTSD (up to 31%) (Steel, Chey, Marnane, Bryant, & Van Ommeren, 2009). Our results suggest that traumatized individuals might not be embracing the social changes easily, and policy makers should be informed about the association between trauma and acceptance of social changes.
The idea that acceptance of social changes might be related to PTSD is originating from Lithuania. Lithuania is one of the European countries which has undergone significant social changes during the last few decades (Kazlauskas & Zelviene, 2016). Social structures, as well political systems, and legislation changed a lot after escaping from the Soviet bloc in the 1990s and integrating into the European Union (EU) in the 2000s. While we found a relationship between acceptance of social changes and PTSD in Lithuania, more research in the region, and also in other societies and cultures are needed to further evaluate this relationship.
Limitations of this study need to be addressed. We collected data using self-report measures. While self-report measures were useful for our study in approaching a population-based sample and IES-R is a widely used scale for assessment of posttraumatic stress disorder symptoms, there are limitations in diagnosing PTSD based on self-report. Potential PTSD prevalence in our sample was about 8%, consisting of about 60 individuals, and thus the PTSD group was rather small for an analysis. Although PTSD prevalence in our sample was comparable with previously reported PTSD prevalence of 2%–7% in Lithuania (Kazlauskas & Zelviene, 2016), further studies are needed to explore the relationship between PTSD and acceptance of social changes in a clinical samples. Our study design was cross-sectional and did not provide sufficient information on the causal relationship between PTSD and acceptance of social changes. Longitudinal studies are needed to get more insight on the dynamics of acceptance of social changes following trauma.
Despite the above-mentioned limitations of this study, the preliminary findings from our study extend the current understanding of psychosocial factors of PTSD and also indicate directions for future research. We developed a brief instrument for measuring acceptance of social changes that can be used in other studies and facilitate cross-cultural research. The findings of our study indicate that acceptance of social changes might be an important psychosocial factor of PTSD.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant (No. SIN-01/2012) from the Research Council of Lithuania.