
Abstract
Background:
Few studies have examined the impact of persistent symptoms of schizophrenia, especially with respect to patient-reported outcomes (PROs), carer burden and health economic impact.
Aims:
Analyse data relating to burden and severity of illness, functional impairment and quality of life for patients with persistent symptoms of schizophrenia.
Methods:
A cohort of stable outpatients with persistent symptoms of schizophrenia across seven countries were assessed in a multicentre, non-interventional, cross-sectional survey and retrospective medical record review using PRO questionnaires, clinical rating scales and carer questionnaires.
Results:
Overall, 1,421 patients and 687 carers were enrolled. Approximately two-thirds of patients had moderate/mild schizophrenia with more severe negative symptoms predominating. Patients showed impaired personal/social functioning and unsuitability for work correlated with various patient factors, most notably symptom-related assessments. Quality-of-life assessments showed 25% to ⩾30% of patients had problems with mobility, washing or dressing. Carer burden was also considerable, with carers having to devote an average of 20.5 hours per week and notable negative impact on quality-of-life measures. Healthcare resource utilisation for in-hospital, outpatient and other care provider visits was significant.
Conclusion:
These results demonstrate the significant burden of schizophrenia for patients, carers and society and highlight the need for improved treatment approaches.
Introduction
Schizophrenia contributes substantially to mental health burden and societal expenditure globally (van Os & Kapur, 2009). Of note, the severity and duration of illness and functional impairment all reduce overall quality of life (Csernansky & Schuchart, 2002; Doering et al., 1998; Milev, Ho, Arndt, & Andreasen, 2005; Novick, Haro, Suarez, Vieta, & Naber, 2009; Postrado & Lehman, 1995). In this respect, persistent symptoms account for much of the poor functional outcome of patients with the disease (Milev et al., 2005). Approximately two-thirds of patients with schizophrenia experience significant persistent positive symptoms after 1 year of treatment, with one-third continuing to experience them after 6 years (Caspi, Davidson, & Tamminga, 2004; Menezes et al., 2006; Novick et al., 2007, 2009; Robinson, Woerner, McMeniman, Mendelowitz, & Bilder, 2004; van Os & Kapur, 2009). As a result, even in the remitting phases of schizophrenia, patients can show incomplete recovery (Altamura, Velonà, Curreli, Mundo, & Bravi, 2002; Andreasen et al., 2005). In addition, negative symptoms reduce patients’ ability to live independently, perform activities of daily living, engage in social activity, maintain personal relationships and participate in work or study (Harvey et al., 2012; Novick et al., 2009; Rabinowitz et al., 2012; White et al., 2009). Recent estimates indicate that one or more negative symptoms are present in nearly 60% of patients with schizophrenia (Bobes, Arango, Garcia-Garcia, Rejas, & CLAMORS Study Collaborative Group, 2010). However, currently available antipsychotics have limited impact on negative symptoms (Erhart, Marder, & Carpenter, 2006; Miyamoto, Miyake, Jarskog, Fleischhacker, & Lieberman, 2012), with many patients continuing to experience persistent negative symptoms during the course of their illness (Chue & Lalonde, 2014; Haro et al., 2015; Stahl & Grady, 2004; Suzuki et al., 2012).
Patient-reported outcomes (PROs) are widely used in the assessment of patients with schizophrenia and, together with other specific instruments, can provide an understanding of patient perceptions of their condition, treatment and outcomes (Miller et al., 2014). There are few studies pertaining to persistent symptoms of schizophrenia, particularly with respect to PROs, and also the related areas of carer burden and health economic impact. As such, there is a need to understand and to quantify better the impact of persistent symptoms (Buckley & Shendarkar, 2005; Chakos et al., 2006; Haro et al., 2003). Consequently, this study was conducted to assess the impact of persistent symptoms on patient functioning, carers and society.
Methods
Study design
This was a multicentre, non-interventional, cross-sectional survey and retrospective medical record review of a cohort of stable outpatients with persistent symptoms of schizophrenia across seven countries (Australia, Czech Republic, France, Italy, Russian Federation, Spain and Turkey). Countries were selected based on the relevance of this study in terms of the need for such national data as identified by the study sponsor. Patient care and treatment followed routine clinical practice and were at the discretion of the investigator. Informal carers were also invited to participate. Cross-sectional data were collected during one routine outpatient clinic visit using PRO questionnaires, clinical rating scales and carer questionnaires, to analyse data relating to symptoms and severity, functioning, health-related quality of life (HRQoL), carer burden and medical resource utilisation (Table 1).
Study assessments conducted at a single study visit.
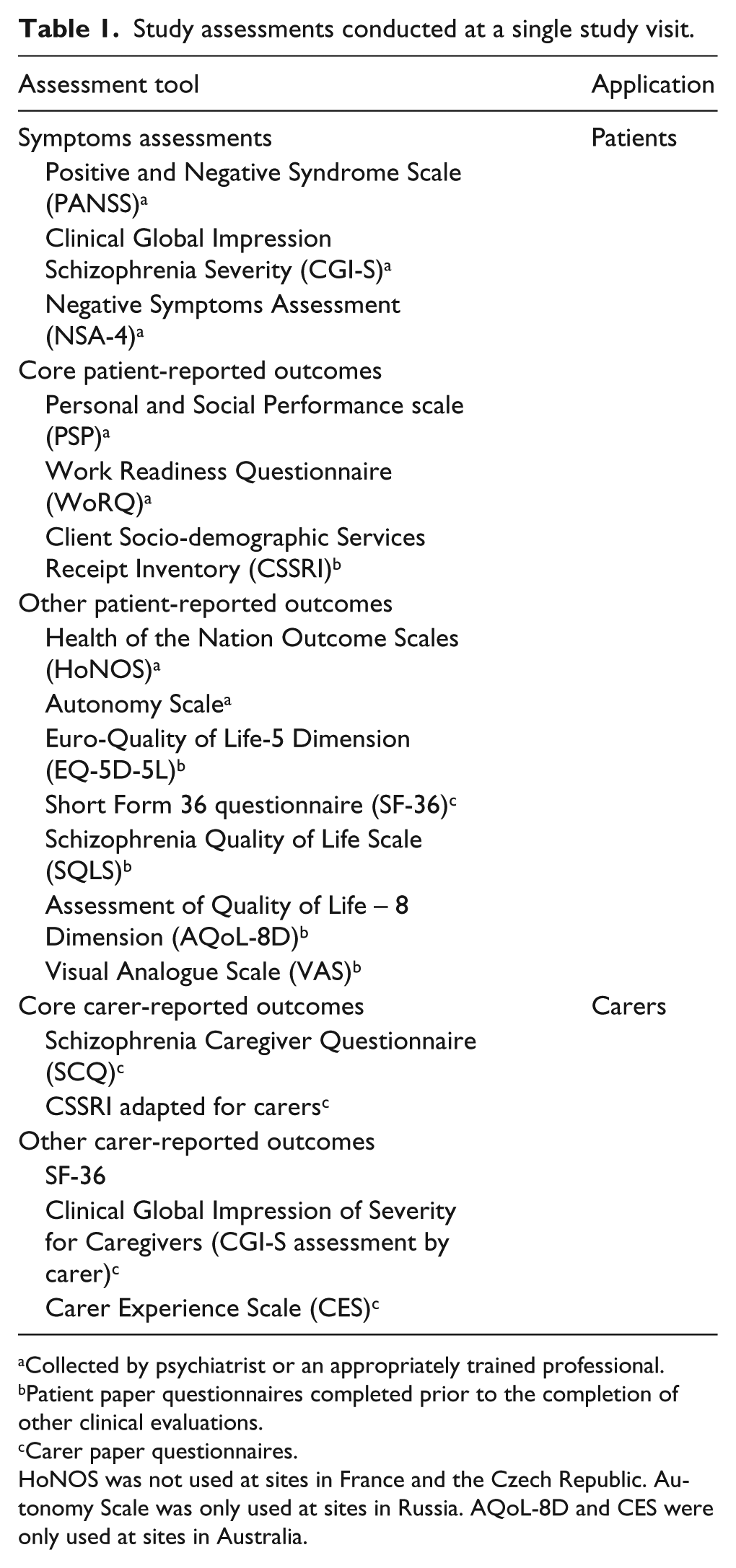
Collected by psychiatrist or an appropriately trained professional.
Patient paper questionnaires completed prior to the completion of other clinical evaluations.
Carer paper questionnaires.
HoNOS was not used at sites in France and the Czech Republic. Autonomy Scale was only used at sites in Russia. AQoL-8D and CES were only used at sites in Australia.
Participants
To maximise generalisability of study results to the whole population of non-acute patients with persistent symptoms of schizophrenia, minimal entry criteria were applied regarding treatment history, comorbidity, history of substance abuse, poor compliance with treatment, history of treatment resistance or symptomatic remission.
Adult patients diagnosed with schizophrenia (Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR) or International Classification of Diseases, 10th revision), presenting at psychiatric outpatient clinics/facilities, within the normal course of care, were enrolled. Key inclusion criteria were age ⩾18 years, persistent symptoms of schizophrenia for ⩾3 months prior to enrolment and prescribed adequate doses of antipsychotics for ⩾3 months prior to enrolment. Participants were excluded if they had an acute exacerbation of schizophrenia within 3 months prior to enrolment or were enrolled in an interventional study. To assess carer burden, carers aged ⩾18 years acting in an informal or unpaid capacity (e.g. family member, relative or friend), who spent at least 4 hours a week with the participant, and who consented to complete the survey, were asked to provide information regarding caring tasks and burden. Having a carer was not mandatory for patient inclusion. All participants provided informed consent and the study was approved by an independent ethics committee.
Study assessments
A series of validated questionnaires was used to assess the current clinical status of schizophrenia (symptom severity, symptom persistence, clinical and functional outcomes), burden of schizophrenia (quality of life, carer burden, resource utilisation), medication use and comorbidities during the single study visit (Table 1). Only ‘core’ assessments listed in Table 1 are covered in detail herein. Additional information on healthcare resource utilisation were derived from a retrospective chart review of psychiatric records (and, if applicable, review of primary care medical records) covering ⩾3 to 12 months prior to inclusion.
Statistical analysis
The Patient Analysis Set comprised all recruited patients who fulfilled all of the inclusion criteria and did not fulfil any of the exclusion criteria and this population was used for the main patient health outcome and resource utilisation data analyses. The Carer Analysis Set comprised all recruited carers who fulfilled all the eligibility criteria and did not fulfil any of the exclusion criteria.
The statistical analysis was exploratory and primarily made use of descriptive methods. Based on precision considerations concerning the estimates of relevant outcomes (resource utilisation, clinical outcome measures) and the need for an adequate number of patients for statistical modelling, approximately 1,600 patients were required, as well as a target of 200 patients per country for local data analysis. In particular, the 95% confidence interval around the mean Positive and Negative Syndrome Scale (PANSS) total score was expected to have a half-width of 0.49 points; for the estimated number of outpatient visits over a period of 3 months, the precision was expected to be 0.65 visits (Knapp et al., 2002).
An analysis of influence of severity and type of symptoms on patients’ social and occupational functioning was performed using multiple linear and logistic regression models adjusting for factors such as country and disease characteristics. Multiple regression models were fitted and refined using a backward selection procedure (p ⩽ .15 to stay in the model) to establish those factors significantly associated with the Personal and Social Performance (PSP) and Work Readiness Questionnaire (WoRQ) scores. All statistical tests were carried out at the 5% significance level without adjustment for multiplicity.
Results
Participant disposition and characteristics
This study was conducted between May 2013 and April 2014. Of the 1,421 patients who provided informed consent, 1,420 fulfilled the study criteria and were included in the patient analysis (Table 2). A further 687 carers, who provided informed consent, were also included in the carer analysis (Table 3). Participant demographic characteristics were similar across the seven countries (Table 2). Overall, patients were predominantly male (65.1%) and White (81.5%), with a mean age of 40.5 years. The majority of patients (73.8%) were single or unmarried and almost half of patients (47.2%) lived with their parents (Table 2). Patients were most commonly not working, being either retired or unemployed (30.7% and 26.8%, respectively). The mean age at diagnosis of schizophrenia was 27.5 years, and the overall mean duration of persistent positive and negative symptoms was 8.7 and 10.5 years, respectively (Table 2).
Participant characteristics.
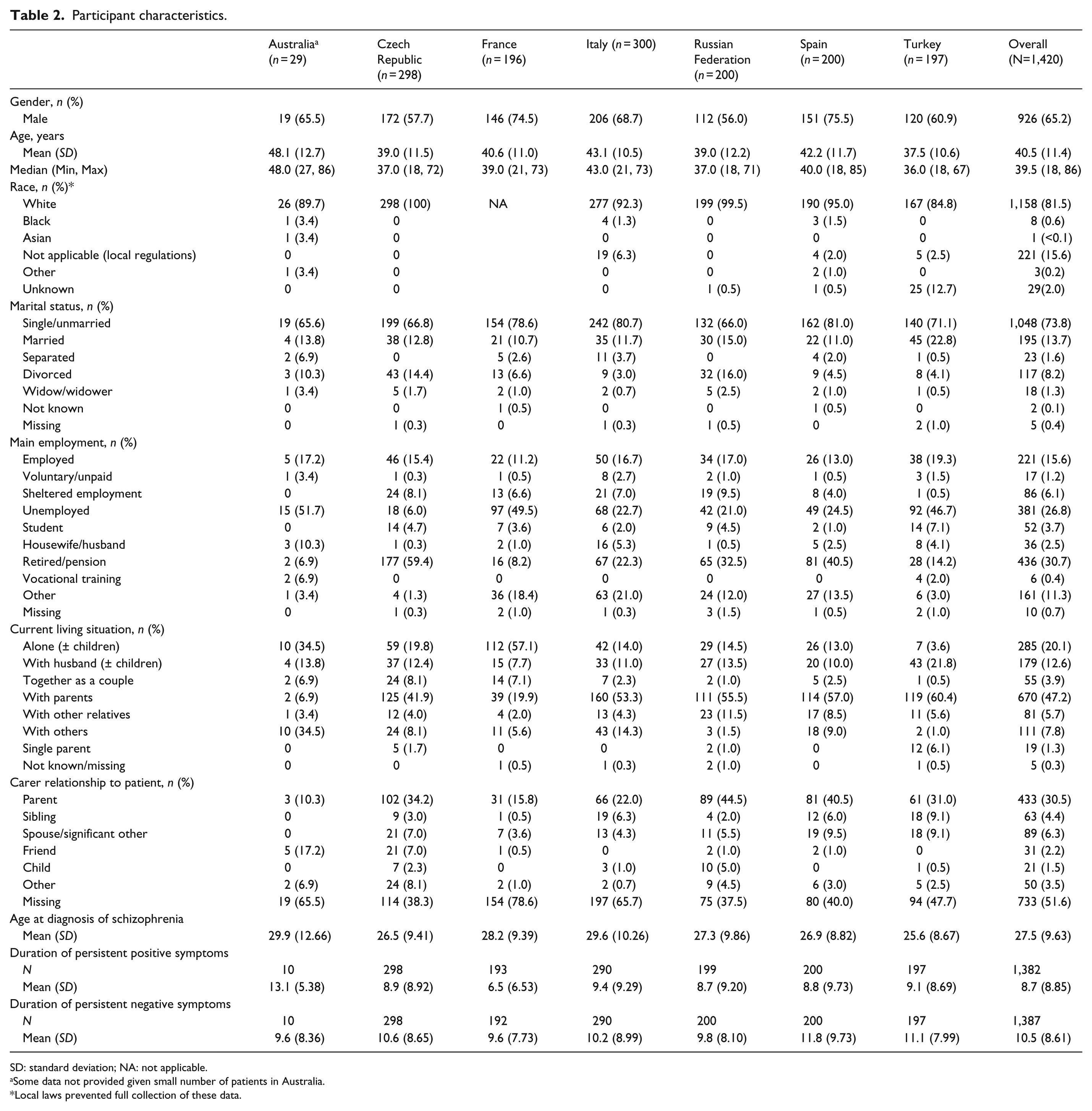
SD: standard deviation; NA: not applicable.
Some data not provided given small number of patients in Australia.
Local laws prevented full collection of these data.
Carer characteristics.
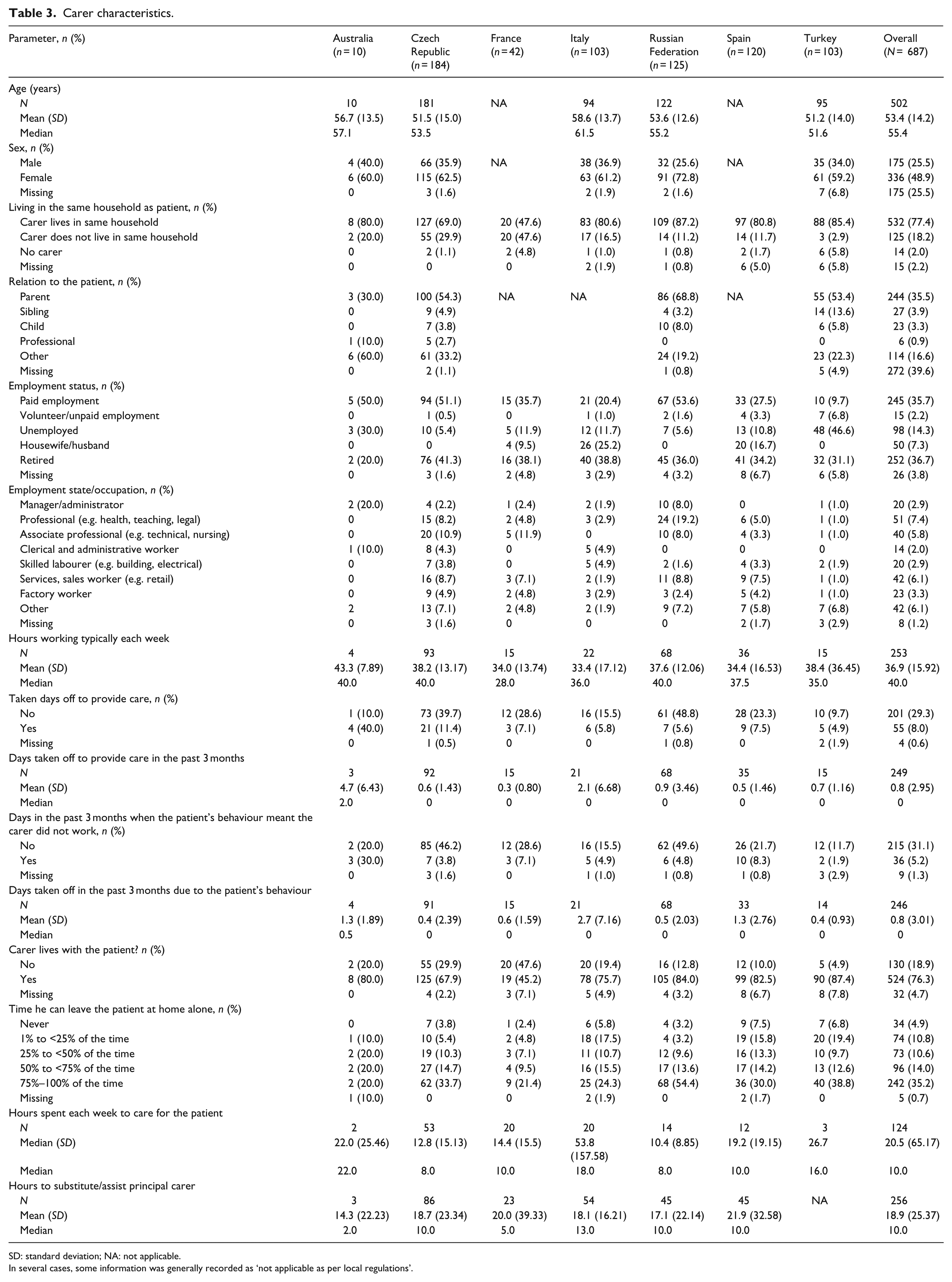
SD: standard deviation; NA: not applicable.
In several cases, some information was generally recorded as ‘not applicable as per local regulations’.
Non-psychiatric comorbidities were common and occurred in a similar pattern across all countries (data not shown). The most common comorbidities were obesity (18.6% of 1,420 patients), elevated blood lipids (11.1%) and glucose metabolism disturbances (5.9%; the majority (59%) were associated with diabetes mellitus type II). The majority of patients were either a current (48.4%) or previous (11.0%) smoker; 4.6% declared a current drug habit and 18.9% a previous drug habit. Of the 1,407 patients (99.1%) currently taking medications, most were prescribed one or two antipsychotics (62.3% and 29.2%, respectively), while 41.8% were receiving other concomitant medications.
Level of severity and type of persistent symptoms on patient social and occupational functioning and health-related quality of life
Severity and type of persistent symptoms
The mean PANSS negative symptoms factor score was 20.7 and the positive symptoms factor score was 18.7. The overall severity of schizophrenia, as assessed by the Clinical Global Impression–Severity (CGI-S), demonstrated that patients were most commonly either moderately ill (37.5% of patients) or mildly ill (29.8%), with fewer patients being markedly or minimally ill (16.9% and 11.1%, respectively). The negative symptoms of schizophrenia were generally of greater severity (36.9% and 27.0% of patients being moderately and mildly ill, respectively) than the positive symptoms (19.9% and 23.4% of patients, being moderately and mildly ill, respectively).
Health-related quality of life and functional questionnaires
The mean PSP scale score for all patients was 55.9, with most patients (76.0%) having an overall score between 31 and 70, indicating varying degrees of difficulties in personal and social functioning in the past month (Figure 1). The following factors had a significant negative association with the PSP score in the multiple regression model: duration of negative symptoms, smoking status (current), PANSS positive symptoms factor score, PANSS negative symptoms factor score and CGI-S for schizophrenia score (adjusted R2 = .6016).
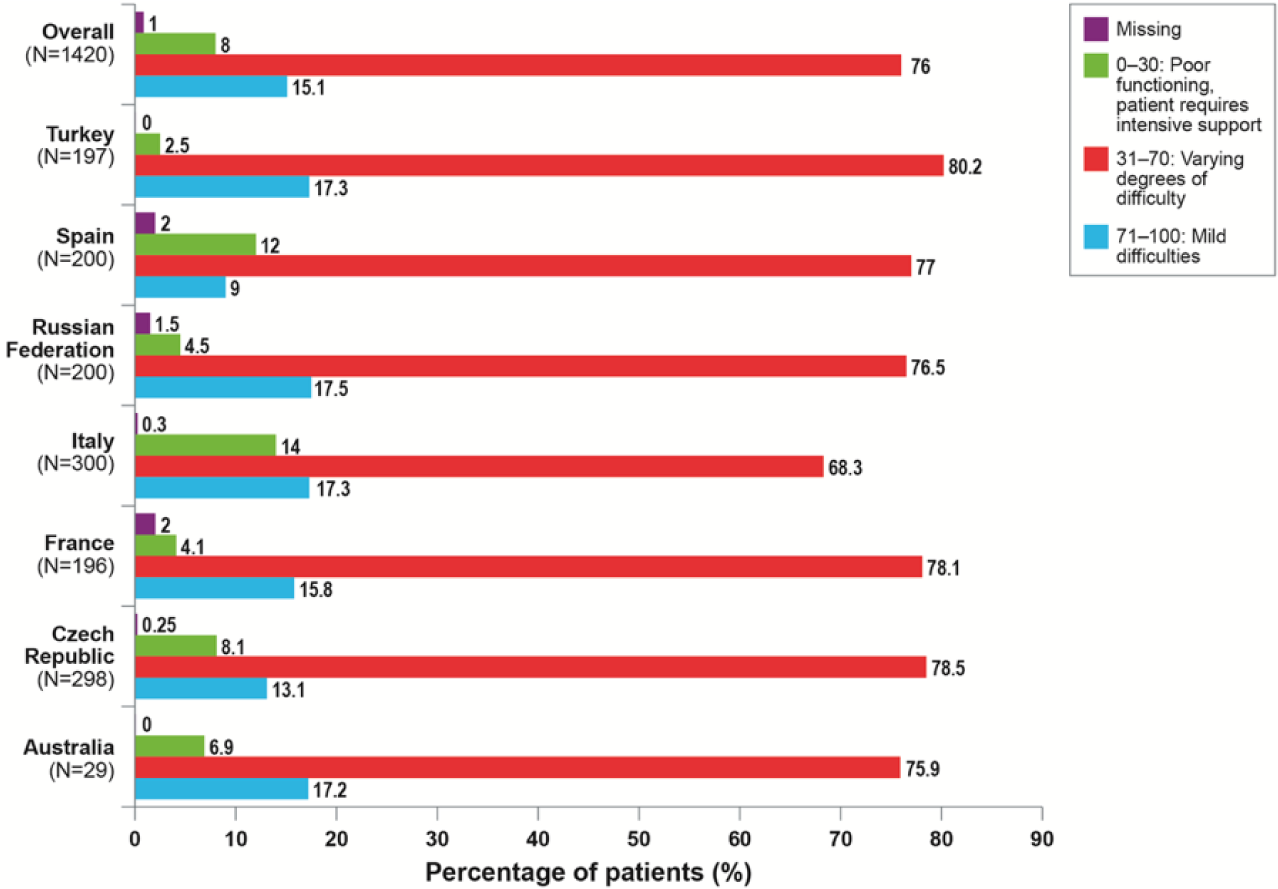
Results from the Personal and Social Performance scale for the patient population (N = 1,420).
Based on clinical judgement from the WoRQ, 64% of patients (n = 920) were not considered ready for work (Figure 2). The following factors had a negative association (5% level of significance) with WoRQ in the logistic regression model: PANSS positive symptoms factor score, PANSS negative symptoms factor score and disturbance of glucose metabolism (adjusted R2 = .3990). The Euro-Quality of Life-5 Dimension (EQ-5D-5L) questionnaire demonstrated that ⩾30% of patients had problems with mobility and one in four had problems with washing or dressing (Figure 3).
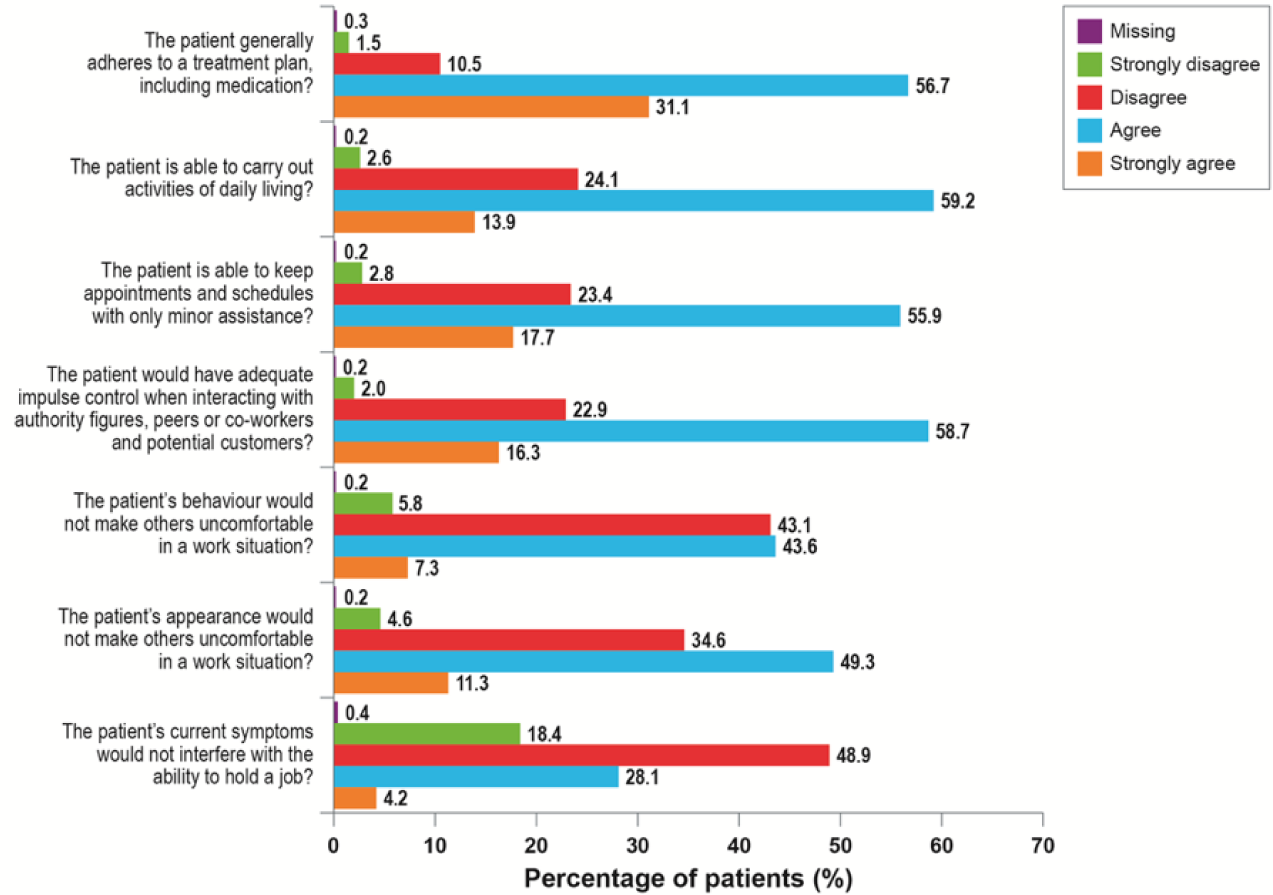
Results from the clinician’s rating Work Readiness Questionnaire for the patient population (N = 1,420).
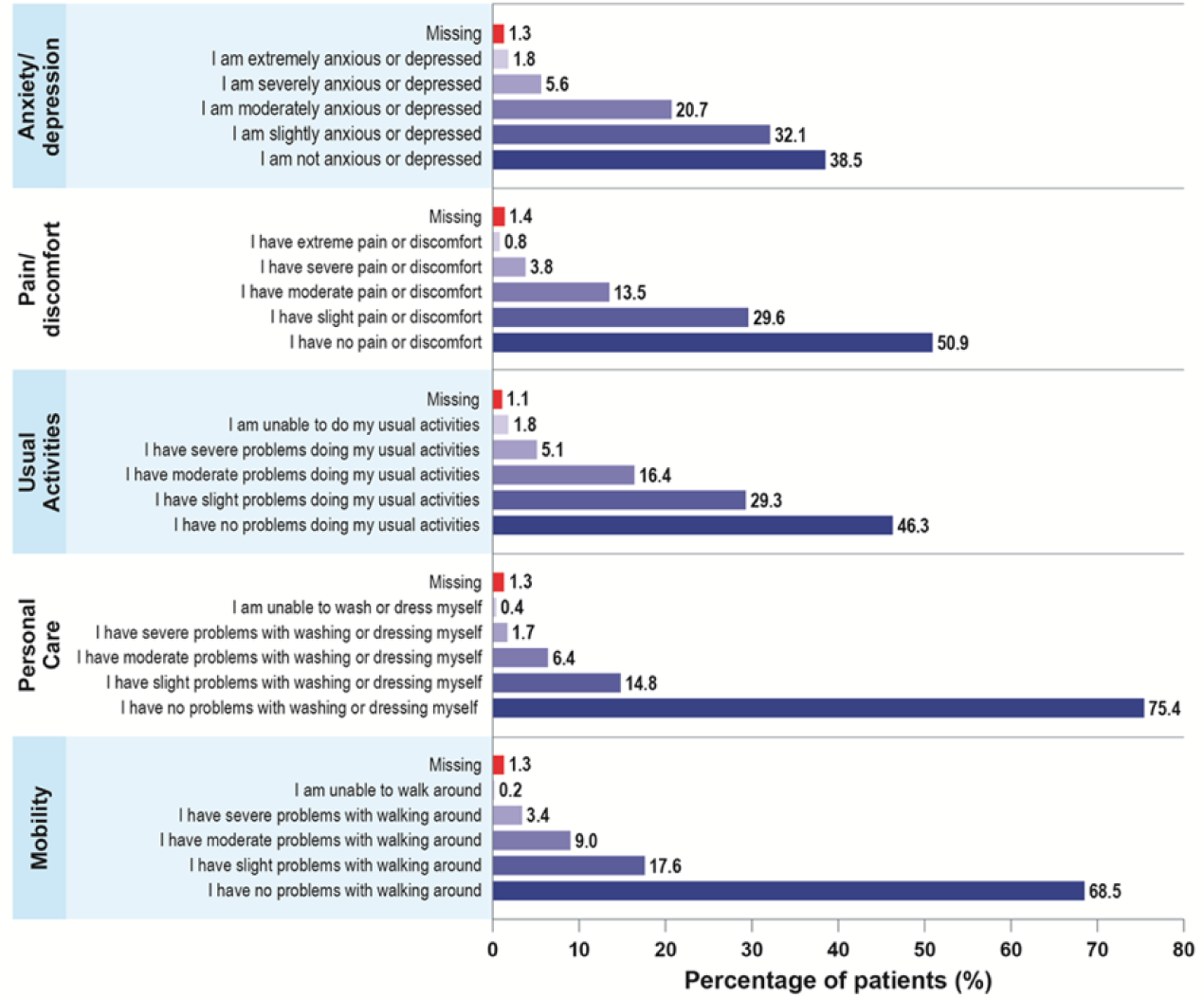
Results from the patient-rated Euro-Quality of Life-5 Dimension questionnaire (N = 1,420).
The mean Visual Analogue Scale (VAS) score for the patient’s current health state overall was 69.3 on a scale of 0–100 (100 equals the best imaginable health state and 0 equals the worst imaginable health state). Overall, mean scores for the Short Form 36 questionnaire (SF-36) domains for patients were greatest (over 70) for physical functioning at 77.6 and bodily pain at 71.3, whereas the SF-36 scores were lowest (below 60) for vitality at 52.6 and general health at 56.5 (Figure 4). The mean score for the Schizophrenia Quality of Life Scale (SQLS) was 2.50 for the psychological scale, 2.68 for the motivation and energy scale and 2.28 for the symptoms and side effect scale. These results indicate that the symptoms for each scale occurred either rarely (score of 2) or sometimes (score of 3).
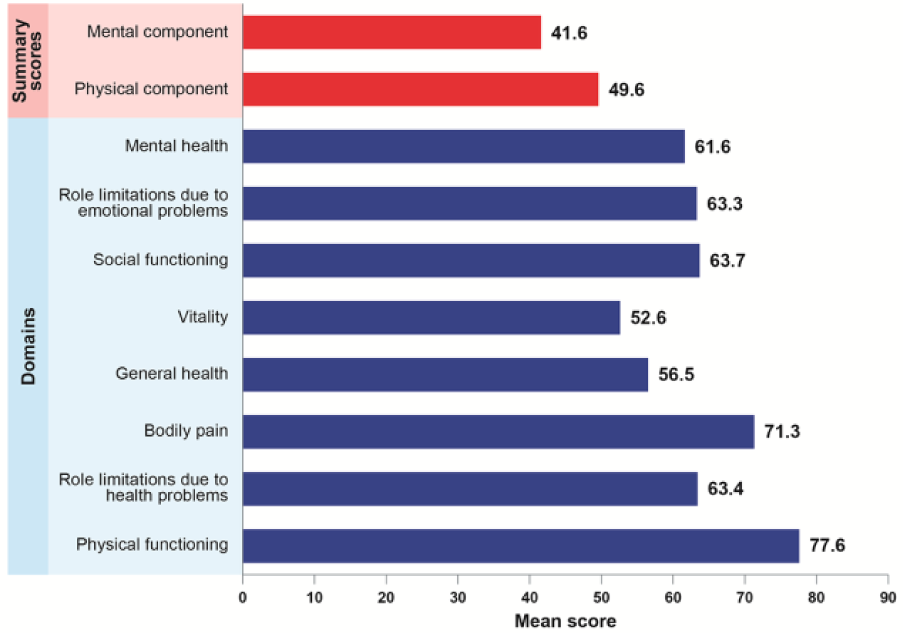
Results from the Short Form 36 questionnaire for the overall patient population (N = 1,420).
Carer burden for patients with persistent symptoms of schizophrenia
Socio-demographic information for the carer, as assessed by the Client Socio-demographic Services Receipt Inventory (CSSRI), is presented in Table 3. The mean age of the carers was 53.4 years; of patients with a carer, the carer was most commonly a parent of the patient (58.9%). Nearly one-third of carers (30%) had concerns with regard to leaving the patient home alone. The mean number of hours carers spent each week caring for the patient was estimated to be 20.5 hours; an additional 18.9 hours (mean) were spent by persons unknown substituting or assisting the carer. Of the carers assessed, 45.4% had had an illness during the past 3 months or had visited a doctor; of these, 4.8% took time off work due to their own illness (ranging from 1 day to 2 months), with 2.5% needing to stop work completely. The mean scores for the SF-36 domains for carers were greatest (>70) for physical functioning at 76.7, social functioning at 72.5 and role limitations due to emotional problems at 70.3. For the Schizophrenia Caregiver Questionnaire (SCQ), the mean scores given by the carers for the individual questions were generally towards the lower end of the scale (ranging from 1.4 to 3.0 on a scale of 10). However, for 4 of the 32 SCQ questions, mean scores of >3 were achieved.
Medical resource utilisation: psychiatric records review
Of the 1,420 patients in the patient analysis, the psychiatric record review covered the past 12 months for 61.3%, a minimum of 3 months for 16.8% and 6 months for 9.8% of patients. The review showed that 28.6% of patients had inpatient hospital visits equating to a mean of 0.7 visits/year. The most common inpatient hospital visits were made to an acute psychiatric ward (13.0% of patients; mean of 1.8 visits/year) which involved a mean stay of 12.1 days (ranging from 1.7 in Turkey to 39.8 in Russia). All other inpatient hospital-based services (psychiatric rehabilitation ward, long-stay ward, emergency crisis centre, general medical ward and ‘other’) were reported for ⩽2.3% of patients.
The vast majority of patients (92%) had visits to outpatient hospital- and community-based services during the review period (range, 1–313 visits), with 20.3 mean visits/year (ranging from 7.2/year in Turkey to 38.8/year in France). The most common outpatient visit was attending a psychiatrist (75.5% of patients; mean 10.9 visits/year), followed by visits to a community mental health centre (14.8% of patients; mean 20.2 visits/year). Against this background, patients made a mean of 27.2 visits/year to primary and community care contacts (varying from 9.6/year in Turkey to 52.7/year in France). A total of 95.2% of patients visited a psychiatrist (mean 14.2 visits/year) while 15.9% of patients visited a community psychiatric nurse (mean 35.3 visits/year), 11.2% a general practitioner (mean 6.5 visits/year) and 10.2% a psychologist (mean 16.9 visits/year). All other outpatient hospital- and community-based services and primary and community care contacts were visited by <10% of patients.
Discussion
Results from this cross-sectional survey and retrospective analysis provide real-world data on outpatients with persistent symptoms of schizophrenia and show a high burden of disease despite apparent adequate antipsychotic therapy. Indeed, persistent symptoms were associated with a considerable adverse impact not only on the patient’s health and well-being but also on their carers, family members and wider society.
Approximately two-thirds of patients in our analysis were classified as having moderate or mild schizophrenia with more severe negative symptoms predominating. As a consequence, patients faced varying degrees of difficulties in personal and social functioning (PSP scale) in the past month and physicians judged that almost two-thirds of patients were not ready for work (WoRQ), both measures being correlated with a variety of patient factors, most notably symptom-related assessments. These findings were corroborated by quality-of-life assessments showing that ⩾30% of patients had problems with mobility and one in four had problems with washing or dressing. The burden on carers (most often parents) was also considerable, with carers and substitute carers having to devote 19–21 hours per week in this role, with high levels of concern recorded about leaving the patient alone and notable negative impact on quality of life measures.
In the past 50 years, a shift towards community care and the increasing deinstitutionalisation of psychiatric patients has resulted in transferring of responsibility and day-to-day care to family members, with recent studies indicating that carers of those with schizophrenia experience a heightened humanistic and economic burden (Caqueo-Urízar, Rus-Calafell, Urzúa, Escudero, & Gutiérrez-Maldonado, 2015; Csoboth, Witt, Villa, & O’Gorman, 2015). Indeed, results from a recent cross-sectional study reported that 19.5% of family carers of individuals with schizophrenia experienced significant depressive symptoms, with 65.5% perceiving themselves to be in poor physical health (Thunyadee et al., 2015). The data from more than 687 carers in this study provide further confirmation on the burden of caring for a person with schizophrenia, and with over half of carers (58.9%) in the study being family members, further confirms the shift in burden in the past 30 years from institutions to families and society.
The economic impact of schizophrenia on medical resource utilisation was also found to be substantial, covering both inpatient and outpatient hospital-based services and community-based services. There was a higher resource use of outpatient hospital-based services compared with inpatient services; the majority of patients had visits to outpatient services whereas only a small minority of patients visited the inpatient services, a finding that may be explained by the stable patient population with no acute symptoms and the fact that many patients with long-term psychiatric disabilities now reside with family members (Martens & Addington, 2001; Saunders, 2003). There was also a vast range in the frequency of visits to healthcare services across countries, likely due to differing local service availability and accessibility as a result of national healthcare systems, policies and priorities, including resource allocation to mental health services that are beyond the examination of this article (Knapp et al., 2002; Roick et al., 2007).
This study complements two recently completed large-scale registries in schizophrenia – the multinational registry (PATTERN), which was designed to evaluate the burden and course of schizophrenia across eight countries (Argentina, Brazil, Canada, France, Germany, Italy, Spain and the United Kingdom), and the US-based Management of Schizophrenia in Clinical Practice (MOSAIC) disease-based registry, which was undertaken to address important gaps in understanding the impact and burden of schizophrenia and to provide insight into the current status of schizophrenia care in the United States (Haro et al., 2015; Nasrallah et al., 2015). In the PATTERN study of 1,379 patients with schizophrenia, the majority of participants had moderately severe disease, persistent symptoms despite apparently adequate therapy, and predominantly negative symptoms associated with poor functioning (Haro et al., 2015). Similarly, in MOSAIC, the 550 patients evaluated again had a high level of persistent symptoms despite apparent adequate treatment, with approximately two-thirds of patients having mild to moderate schizophrenia and negative symptoms predominating. Patients required help with performing everyday tasks while negative symptoms persisted over the 2-year assessment period (Nasrallah et al., 2015). In line with these investigations, our findings once again underscore the severity of illness and the persistence of symptoms despite being adequately treated. The predominance of negative symptoms and the negative impact of symptoms on functional deficits are particularly worthy of note, highlighting that there continues to be a great need for improvement in the treatment of schizophrenia.
There are several limitations to this study, which are inherent to such cross-sectional and retrospective studies. The population of patients in this study were those followed in outpatient clinics/facilities for routine care and may not represent the entire population of patients with persistent symptoms of schizophrenia. There are variations in standard of care and medical information databases between countries, although the data collection procedure was standardised by the use of an electronic case report form for participating sites. Health economic data were only reported in terms of resource utilisation; it was therefore not possible to compare the costs across countries. It is also difficult to make comparisons between countries in relation to healthcare resource consumption due to differences in the healthcare systems, a finding highlighted by the large variations between countries in the use of inpatient hospital-based services.
Conclusion
Results from this international cross-sectional evaluation and retrospective survey in a real-world outpatient setting describe both the clinical status of patients with schizophrenia and that of their carers, while highlighting the societal and economic impact of schizophrenia across countries. Overall, the findings of this analysis demonstrate the significant burden of schizophrenia for both patients and carers and the high level of resource utilisation for this severe mental illness.
Footnotes
Acknowledgements
The authors received editorial support from inVentiv Medical Communications, which was funded by F. Hoffmann-La Roche, Ltd. The authors would like to thank Laura Alberti and Paul Gandi for their support with this study.
Conflict of interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.-L.N., D.T., and J.L. are all employees of F. Hoffmann-La Roche Ltd. C.G.B. is an employee of Genentech (a member of the Roche group). C.B. is a contractor of F. Hoffmann-La Roche Ltd.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was sponsored by F. Hoffmann-La Roche, Ltd.