
Abstract
Background:
As young Australian males are at a high risk of suicide, the identification of risk factors other than psychopathology is vital for the development of comprehensive suicide prevention measures.
Aims:
The study investigated whether there were differences in risk factors and pathways to suicide in young adult males from Queensland, Australia, with and without a diagnosable psychiatric disorder.
Methods:
A case–control, psychological autopsy method was applied using a control group of young males who had died suddenly from causes other than suicide.
Results:
Suicide cases without a psychiatric diagnosis more frequently displayed behaviours indicative of their suicidality (such as previous attempts, disposing of possessions and making statements of hopelessness) than controls without a diagnosis. Suicides without a diagnosis also displayed more ‘difficult’ personality traits, such as higher levels of neuroticism and aggression. They also experienced poorer quality of life and were significantly more likely than their controls to have experienced a recent separation from a spouse or partner.
Conclusion:
The results of this study confirmed the existence of several distinct characteristics of young males who die by suicide in the absence of any diagnosable psychiatric disorder.
Introduction
Suicide claims the lives of more than 800,000 people worldwide each year, indicating an annual global age-standardised suicide rate of 11.4 per 100,000 in 2012 (World Health Organization (WHO), 2014). Despite marked variations between regions and countries, in general suicide rates are significantly higher for males than for females. The World Health Organization (WHO) presents the global age-standardised rates for males and females as 15.0 and 8.0, respectively (WHO, 2014). Suicide is second to accidental death as the leading cause of death in young males worldwide (Pitman, Krysinska, Osborn, & King, 2012; WHO, 2014).
In Australia, despite some decrease in the male suicide rate over the past decade (Australian Bureau of Statistics (ABS), 2015), disproportionately high male-to-female suicide ratios are still observed. During the period from 2008 to 2012, males were more than three times more likely than females to die from suicide (ABS, 2015). In Queensland, Australia, between 2002 and 2011, the average age-standardised suicide rate was 3.41 times higher for males than females (22.3 and 6.5 per 100,000, respectively). In the same state, suicide rates for Aboriginal and Torres Strait Islander males were 1.49 times higher than other Australian males (Kõlves, Potts, & De Leo, 2015). Young adult males between 25 and 44 years of age have the highest suicide rates in the country (ABS, 2015). In Queensland, for 2002–2011, the rates for males aged 25–34 years and 35–44 years were 32.9 and 34.0 per 100,000, respectively (Kõlves et al., 2015).
Evidence from previous studies indicates that the majority of persons who die by suicide have a diagnosable psychiatric condition at the time of death (Conner, Duberstein, Conwell, Seidlitz, & Caine, 2001; Isometsä, 2001). A diagnosis of a mental disorder is one of the strongest risk factors for suicide, with psychiatric comorbidity (i.e. a diagnosis of more than one mental disorder) increasing the risk even further (Nock, Hwang, Sampson, & Kessler, 2010).
However, there has been much debate about the extent of contribution of mental disorders to suicide (Pridmore, 2015; Snowdon, 2015). Milner, Sveticic, and De Leo (2012) conducted a systematic review of psychological autopsy studies and found that a considerable proportion (37%) of suicide cases did not have any form of psychiatric diagnosis (i.e. Axis I or Axis II disorders). However, variations were noted in how psychiatric conditions were defined and measured between studies. The researchers concluded that the number of suicides without a diagnosable mental disorder differed between geographical contexts, most probably as a result of cultural variation (Milner et al., 2012). The dominant medical view is that in western countries at least 90% of suicides are the result of a diagnosable mental disorder (Pridmore, 2015). In developing countries such as China and India, it is thought that this percentage is much lower (WHO, 2014). In Australia, studies currently suggest that about 80% of suicide decedents had mental health disorders, with the percentage being lower in older people (De Leo, Draper, Snowdon, & Kõlves, 2013b; Snowdon, 2015).
Pridmore (2015) concurs that although suicide is often impacted by a mental disorder, it is often the result of a combination of stressors, including unemployment, relationship breakup, drug and alcohol abuse and painful emotions such as shame and guilt. An international review on suicide in young men by Pitman et al. (2012) identified specific risk factors, such as psychiatric illness, substance misuse, lower socioeconomic status, rural residence and single marital status, and population-level factors including unemployment, social deprivation and media reporting of suicide. Although a number of studies conducted in non-western populations have highlighted the importance of life events, economic and social stress as influences on suicide, there has been little research into suicides occurring in the absence of mental disorders in high-income western contexts (Milner et al., 2012).
As young adult males in Australia are at a high risk of suicide, the identification of risk factors other than psychopathology is vital for the development of comprehensive suicide prevention measures. This study utilised the psychological autopsy method to investigate whether there are differences in risk factors and pathways to suicide in young adult males (aged 25–44 years) from Queensland, Australia, with and without a diagnosed mental disorder. Specifically, the study aimed to explore the risk factors for suicide by comparing young males without a diagnosable mental disorder who die by suicide with a control group of young males who died by sudden death. In addition, the study investigated differences between suicide cases with and without a diagnosed mental disorder. To the authors’ knowledge, this is the first Australian study to examine suicidality specifically in young males with no diagnosable psychiatric disorder.
Method
Study design and data collection
A case–control study design was applied using a control group of young males aged 25–44 years who had died suddenly from causes other than suicide (e.g. myocardial infarction, accident) to compare with a group of males from the same age group who had died by suicide. Those who died in a single vehicle accident were excluded from the control group to minimise the potential overlap with suicide deaths. Psychological autopsy interviews were conducted with next-of-kin (NOK) to collect data for each of the suicide and sudden death control cases.
The recruitment procedure entailed sending NOKs a letter and information sheet introducing the study and inviting them to participate in an interview. Informants for the suicide cases were identified through the Queensland Suicide Register (QSR), an independent database maintained by the Australian Institute of Suicide Research and Prevention (AISRAP). NOKs for the suicide cases who had previously provided authorisation to be contacted for research purposes (via the Queensland Police Service) were sent letters from AISRAP. NOKs of sudden death cases were identified by and sent letters from the Queensland Office of State Coroner.
All letters were followed up by telephone approximately 2 weeks later by AISRAP researchers. On provision of informed consent, trained clinical interviewers arranged appointments for individual interviews. Telephone interviews were organised where informants considered this preferable to or more convenient than face-to-face interviews. Clinical interviewers conducted the psychological autopsy interviews with the NOKs of the deceased, which lasted between 1 and 3 hours. The semi-structured interviews applied validated scales and questionnaires to establish the presence or absence of psychopathology, as well as demographic and psychosocial risk factors for suicide.
Informants were interviewed between 6 and 12 months after victims’ deaths to allow adequate time to reduce the risk of psychological stress of the bereaved participants, while still minimising the potential for recall bias. All interviews were conducted in the time period between 2008 and 2011.
Measures
Scales/questionnaires
Quality of life was assessed using the WHO Quality of Life, Australian Version Scale (WHO, 2004). The prevalence of life events in the period of 12 months preceding death was measured using the Paykel interview for recent life events (Paykel, 1997; Paykel, Prusoff, & Uhlenhuth, 1971). The Bille-Brahe Social Support Scale (Bille-Brahe & Jensen, 2004) – which distinguishes between receiving and giving practical and emotional social support from family and friends – was applied to measure social support. The Overt Aggression Scale was used to assess levels of aggression (Yudofsky, Silver, Jackson, Endicott, & Williams, 1986), and the Barratt Impulsiveness Scale, Version 11 (Patton, Stanford, & Barratt, 1995) was used to measure impulsivity. The NEO Five-Factor Inventory (NEO-FFI) was applied to evaluate personality (McCrae & Costa, 2004). The NEO-FFI is a shortened version of NEO PI-R, a standardised tool which assesses the five major personality domains of neuroticism, extraversion, openness, agreeableness and conscientiousness.
Psychiatric diagnoses
Psychiatric disorders were determined using the Structured Clinical Interview for DSM-IV, Research Version, Non-patient edition (SCID-1-RV NP) for Axis I disorders (First, Spitzer, Gibbon, & Williams, 2002) and SCID-II for Axis II disorders (First, Gibbon, Spitzer, Williams & Benjamin, 1997). All interviews were conducted by clinical interviewers who had received prior specific training. The clinical interview data were used to obtain retrospective psychiatric diagnoses, based on the consensus between three psychiatrists (including one of the authors, D.D.L.) who used the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) Axis I and Axis II criteria to judge each case blindly (i.e. they did not know whether the cases were suicides or sudden deaths).
Subjects
Interviews were conducted for a total of 194 individual cases, comprising 126 of suicide cases and 68 sudden death cases. Response rates for NOKs of suicide cases and sudden death cases were 59.2% and 39.4%, respectively. In the suicide group, 68.3% cases had interviews performed with one informant and 31.7% with two or more informants. In the sudden death group, 80.9% of cases had an interview conducted with one informant and 19.1% with two or more informants. There were no significant differences between suicide and sudden death cases in the relationship to the deceased (spouse, parent, children, etc.).
The main methods of suicide were hanging, strangulation and suffocation (62%), exposure to organic solvents and halogenated hydrocarbons and their vapours (7.9%) and rifle, shotgun and larger firearm discharge (7%). The sudden death cases were most frequently due to diseases of the circulatory system (59.3%), followed by accidental and other external causes of death (21%) and diseases of the nervous system (10.3%).
Ethical clearance
The study was approved by the Griffith University Human Research Ethics Committee (Ethics protocol number CSR/03/05/HREC).
Statistical analysis
The statistical package IBM SPSS (version 22.0) was used to perform all statistical analyses. To analyse the predicting variables for the suicide group compared to sudden death controls, separately for the groups either with or without a psychiatric disorder, odds ratios (OR) with a 95% confidence interval were calculated. When calculating ORs or χ2 in sub-groups with small numbers (fewer than five), Fisher’s exact test was used. A probability level of .05 was employed for all statistical tests.
Results
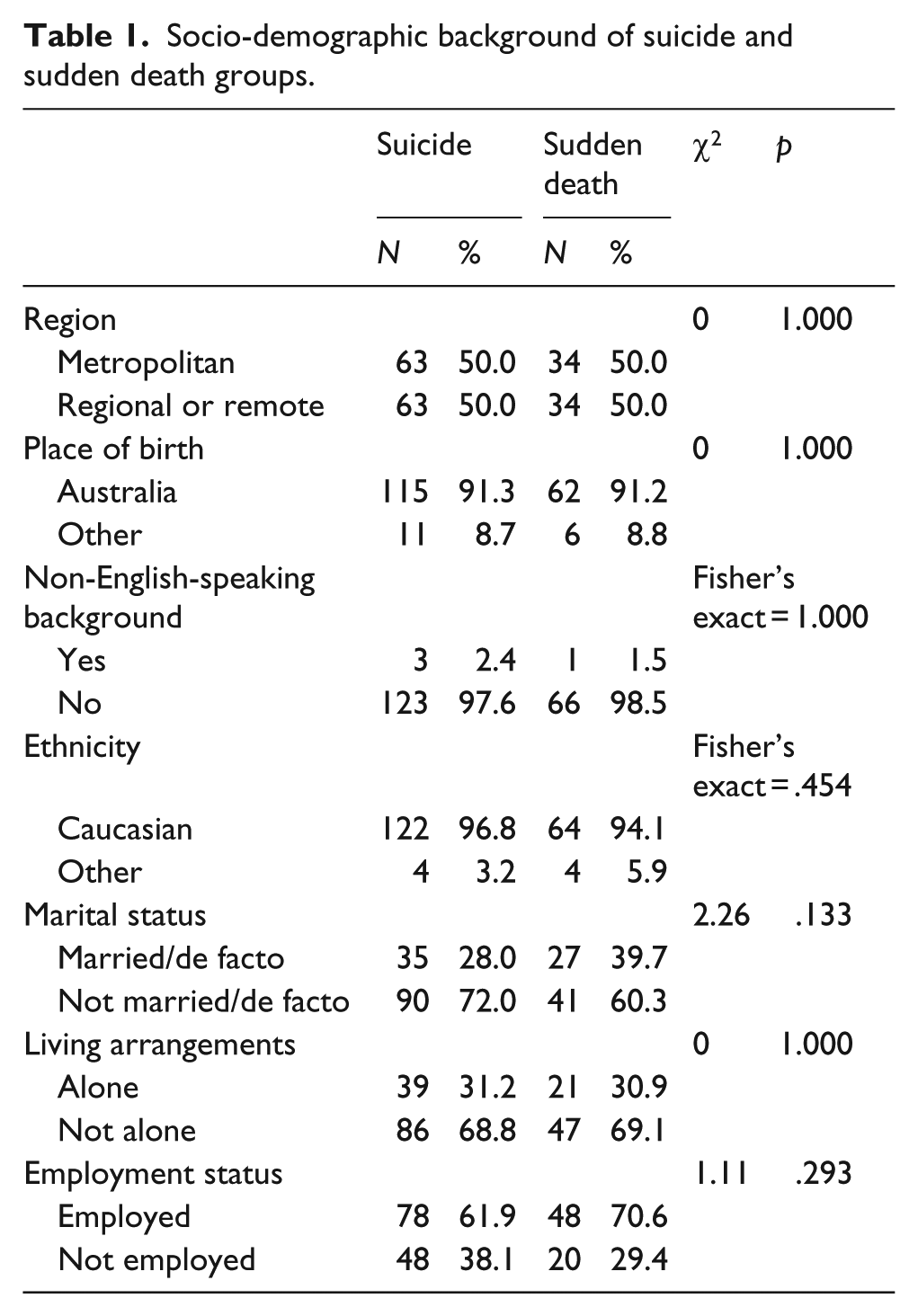
The majority of the subjects in the study were Caucasian (95.9%) and born in Australia (91.2%). Of the total sample, 2.1% comprised Aboriginal and Torres Strait Islanders (i.e. four subjects in the suicide group and two subjects in the control group). There were no significant differences between suicide and sudden death control groups on any of the demographic factors of marital status, living arrangements, employment status, region (metropolitan, regional/remote), non-English-speaking background (NESB), place of birth or ethnicity (see Table 1).
Socio-demographic background of suicide and sudden death groups.
Diagnostic profile
Of the suicide group, 20.6% (n = 26) had no diagnosable psychiatric disorder at the time of death, and 79.4% (n = 100 cases) had at least one psychiatric diagnosis. As presented in Table 2, a total of 96 suicide cases had an Axis I diagnosis (76.2%), 25 had an Axis II diagnosis (19.8%) and 21 had diagnoses of both Axes (17%). The most common Axis I diagnoses in the suicide group were major depressive disorder, mood disorders, substance use disorders and anxiety disorders. The most common Axis II diagnosis was borderline personality disorder, followed by both avoidant personality disorder and paranoid personality disorder.
Psychiatric diagnoses (DSM-IV Axis I and Axis II diagnoses at death).
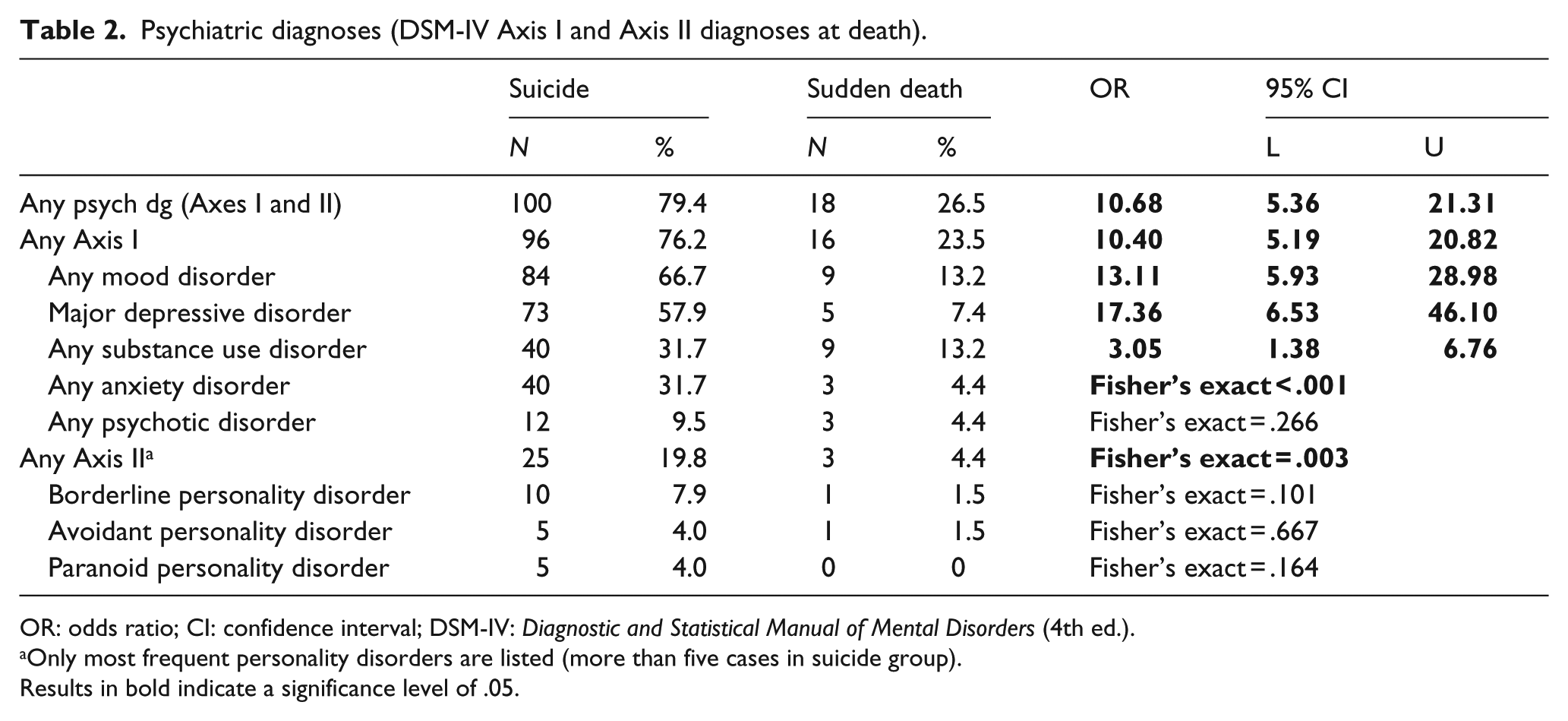
OR: odds ratio; CI: confidence interval; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders (4th ed.).
Only most frequent personality disorders are listed (more than five cases in suicide group).
Results in bold indicate a significance level of .05.
Of the sudden death control group, 73.5% (n = 50) had no psychiatric diagnosis, with 26.5% (n = 18) with at least one psychiatric diagnosis. Sixteen of the sudden death cases had an Axis I diagnosis and three cases had an Axis II diagnosis (i.e. one case each of borderline, histrionic and avoidant personality disorders). There was one case from the sudden death group with a diagnosis of both Axes. The most common Axis I diagnoses in the control group were mood disorders, substance use disorders and major depressive disorder.
No significant differences were found between suicide cases and their sudden death controls, in either those with or without a psychiatric disorder by marital status, living arrangements, employment status, region (metropolitan, regional/remote), nor NESB. However, significant differences were found on place of birth and ethnicity in the suicide group. Suicide cases with a psychiatric disorder were significantly more likely than suicides without a psychiatric disorder to be Caucasian and born in Australia (see Table 3).
Socio-demographic background of suicide and sudden death groups, with and without a psychiatric diagnosis.
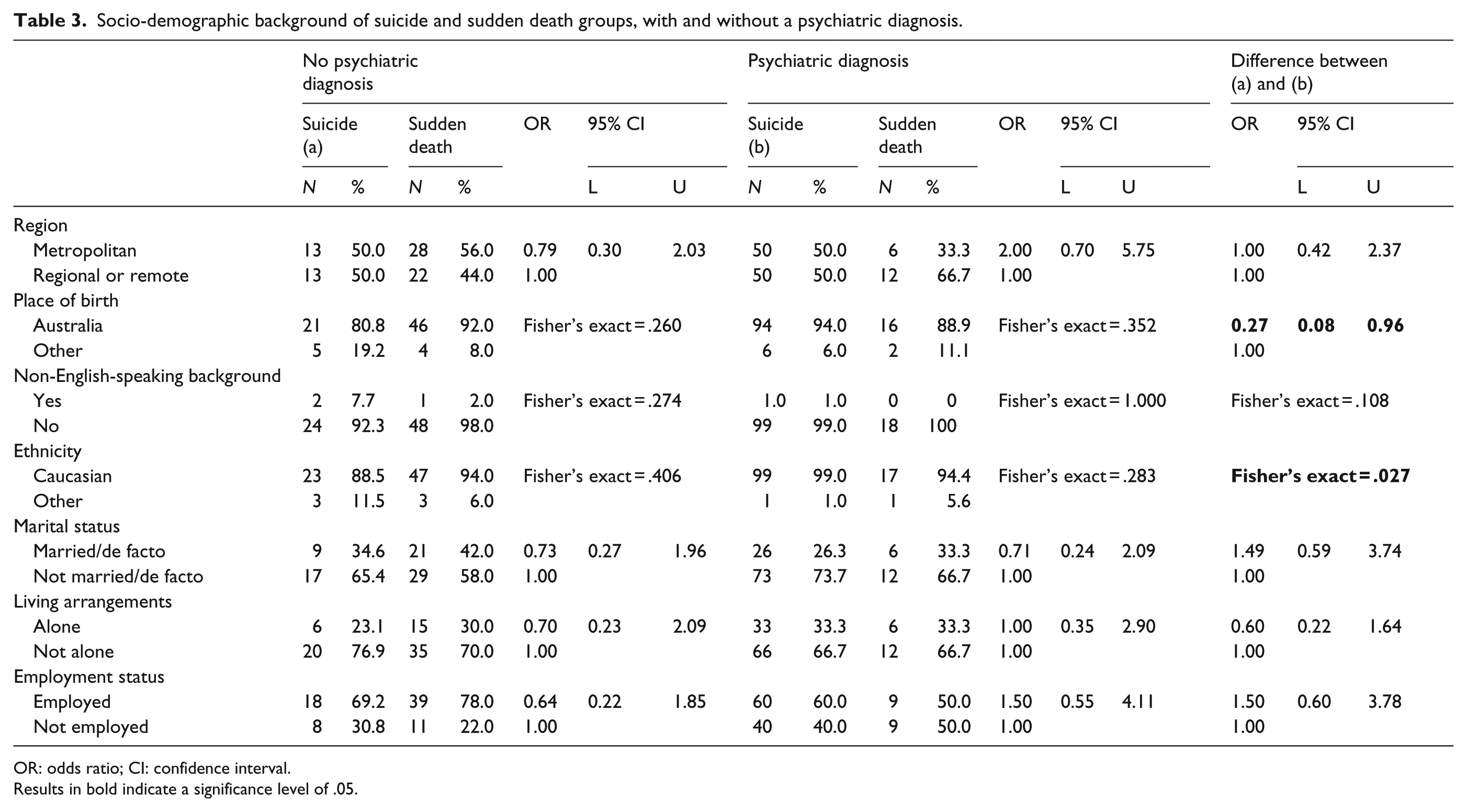
OR: odds ratio; CI: confidence interval.
Results in bold indicate a significance level of .05.
Suicidal behaviours, life events and social support
Compared to their sudden death controls, suicide cases with and without a diagnosable psychiatric disorder significantly more frequently displayed behaviours indicative of their suicidality (see Table 4). Suicides both with and without a psychiatric disorder were significantly more likely than their control groups to have had previous suicide attempts, disposed of their possessions, made statements of hopelessness and shown other suicidal behaviours or statements. In comparison to suicide cases with no diagnosis, suicides with a psychiatric diagnosis were significantly more likely to have had previous suicide attempts, made statements of hopelessness and shown other suicidal behaviours or statements.
Suicidal behaviours, life events and social support.

OR: odds ratio; CI: confidence interval; F test: Fisher’s exact test.
Results in bold indicate a significance level of .05.
Both suicides with and without a psychiatric disorder were significantly more likely than their sudden death controls to have experienced relationship and other recent life events over the last 12 months. Further analysis of the individual items comprising the relationship life event scale showed that suicides without a psychiatric diagnosis were also significantly more likely than the sudden deaths without a diagnosis to have recently experienced a separation from a spouse or partner. Suicides with a psychiatric diagnosis were significantly more likely than suicides without a diagnosis to have experienced recent significant life events involving family, financial and legal matters.
There were no differences between suicides without a diagnosis and their controls in the average number of significant life events experienced. In contrast, suicides with a psychiatric disorder experienced significantly more life events than sudden deaths with a psychiatric disorder. Suicides with a psychiatric disorder also experienced more significant life events than suicides without a psychiatric disorder.
There were no significant differences between suicide cases with and without psychiatric disorders on whether they received the level of practical and/or moral support that they needed from either family or friends. However, suicides with a psychiatric diagnosis received significantly less moral support than needed from their families than suicides without a diagnosis. In addition, sudden deaths with a psychiatric diagnosis received significantly less practical support than needed from friends than suicides with a diagnosis.
Suicides with and without a psychiatric disorder and their respective controls did not differ significantly on levels of impulsivity (see Table 5). However, suicides with a diagnosis showed significantly higher levels of impulsivity than suicides without a diagnosis. Suicide cases both with and without a psychiatric disorder showed significantly higher levels of aggression than their sudden death controls. Suicide cases with a psychiatric disorder also showed significantly higher levels of aggression when compared to those without a diagnosis.
Personality and quality of life.

M: mean; SD: standard deviation; NEO-FFI: NEO Five-Factor Inventory.
Results in bold indicate a significance level of .05.
Compared to sudden deaths with no diagnosable psychiatric disorder, suicides without a diagnosis showed significantly higher levels of neuroticism, indicating poor emotional regulation and more frequent feelings of anxiety, anger, guilt and depressed mood. There were no other significant differences between suicides with and without a psychiatric disorder and their respective controls on the other NEO-FFI measures of personality. There were, however, a number of significant differences between suicides with and without a diagnosis on NEO-FFI measures. Compared to suicides without a diagnosis, suicides with a psychiatric diagnosis also showed significantly higher levels of neuroticism, as well as significantly lower levels of agreeableness. Suicides with a psychiatric diagnosis were also significantly less extroverted than suicides without a diagnosis.
Suicide cases without a psychiatric diagnosis had poorer quality of life than their controls across the WHO Quality of Life Australian Version Scale’s domains of psychological and social well-being. Suicides with a psychiatric diagnosis had poorer quality of life than their controls across the domains of psychological and social well-being. Compared to suicides without a diagnosis, suicides with a psychiatric diagnosis also had poorer quality of life across all four domains of physical, social and psychological and environmental well-being.
Discussion
The results of this study confirmed that one-fifth of young males (20.6% of our sample) who die by suicide have no diagnosed psychiatric disorder. This proportion is lower than the 37% of cases cited in Milner et al.’s (2012) international review, but does align with current Australian figures suggesting that about 80% of individuals who die by suicide have mental health disorders (De Leo et al., 2013b). It should be noted, however, that in Australia, there seems to be a higher prevalence of suicides without a diagnosis in adults over the age of 60 years (De Leo et al., 2013b).
Although young male suicide cases without a diagnosable psychiatric condition showed fewer warning signs than those with a diagnosis, they did display some detectable behaviours that could be statistically distinguished from their controls. Suicides without a diagnosis more frequently displayed suicidal behaviours such as previous suicide attempts, disposing of possessions and making statements of hopelessness than their sudden death controls. Compared to their controls, suicides without a diagnosis also displayed more ‘difficult’ personality traits. For example, they showed higher levels of neuroticism and aggression. These results are in line with previous research as both neuroticism and aggression have been implicated in suicidal behaviour (Draper, Kõlves, De Leo & Snowdon, 2014; Hirvikoski & Jokinen, 2012).
Tellingly, suicide cases without a diagnosis experienced poorer quality of life (across both social and psychological well-being) than their sudden death controls. Although a significant difference was not found between suicides without a diagnosis and their controls in the average number of significant negative life events experienced, it is worth noting that the obtained p-value of .052 for this statistical test was only marginally above the significance level. It is possible that a statistically significant result may have been obtained had the sample been larger.
Suicides without a psychiatric diagnosis were also significantly more likely than their controls to have recently experienced a separation from a spouse or partner. This finding is consistent with research that suggests that individuals, especially males, experiencing the acute phase of marital/de facto separation may be at greater risk of suicidal behaviour compared to those experiencing long-term separation (Ide, Wyder, Kolves, & De Leo, 2010; Kõlves, Ide, & De Leo, 2010, 2012; Wyder, Ward, & De Leo, 2009). In addition, research specific to Queensland has shown that relationship separation resulted in a suicide risk at least four times higher than any other marital status and that this risk was particularly high for young males (Wyder et al., 2009). These findings have strong implications for the need for relationship and resilience training programmes for young males.
The results also revealed distinguishing features between suicides with and without a diagnosable psychiatric condition. Consistent with limited existing research (Law, Wong, & Yip, 2014), suicide cases without a diagnosis showed fewer warning signs of their suicidality and are therefore much more difficult to predict. In line with research on risk factors for suicidal ideation, suicide cases with a psychiatric diagnosis displayed higher levels of aggression, impulsivity and neuroticism and lower levels of agreeableness and extroversion (Draper et al., 2014; Hirvikoski & Jokinen, 2012; Kerby, 2003). Suicide cases without a diagnosis experienced less significant negative life events (family, financial and legal) than suicides with a diagnosis. However, it could be argued that these negative events may be indicative of difficulties experienced as a result of suffering from a mental disorder, rather than predictors of suicidality. For example, it is possible that pre-existing issues such as psychiatric illness, anti-social behaviour or poor coping skills could contribute to negative life events such as relationship breakdowns (Butterworth & Rodgers, 2008; Wyder et al., 2009). Suicides with a psychiatric diagnosis also experienced poorer quality of life than suicides without a diagnosis across all four of the physical, psychological, social and environmental domains.
Contrary to previous research (Law et al., 2014), no evidence was found for the effect of the risk and protective factors of not receiving/receiving adequate practical or moral support for suicide cases with or without a diagnosis. Given that suicide cases with a psychiatric diagnosis received less moral support from their families than those without a diagnosis, it is again possible that due to psychiatric illness or anti-social behaviour, these individuals may have had poorer relationships with their families and thus received less moral support.
Methodological considerations
A limitation of this study is the low response rate for NOKs for the sudden death group and thus the smaller than desirable sample size which limits statistical power and multivariate statistical analysis. However, this response rate for controls was slightly higher than those obtained in other recent Australian psychological autopsy studies (e.g. De Leo, Draper, Snowdon, & Kõlves, 2013a; De Leo et al., 2013b). Moreover, the absence of significant differences on demographic variables indicates that the samples are from relatively homogeneous populations. A more salient limitation of this study, however, was the under-representation of the Aboriginal and Torres Strait Islander population. Based on the QSR, Aboriginal and Torres Strait Islanders represent 5.75% of all suicides in Queensland (over twice the proportion of Aboriginal and Torres Strait Islanders represented in our sample). Given the high rates of indigenous suicide in Queensland (and Australia generally), it will be imperative for future research to obtain greater indigenous representativeness.
Care must also be taken in the interpretation of findings when using a control group of sudden deaths. De Leo et al. (2013b) have argued that the characteristics of sudden death non-suicide cases (e.g. physical health, lifestyle choices) may well differ from those who die by suicide, as well as the general population. In the case of this study, a large proportion of the controls (nearly 70%) suffered from diseases of the circulatory or nervous system which were attributable to their death, suggesting that they may differ from 25- to 44-year-old males in the general population in terms of physical health.
Although the psychological autopsy method is the most direct technique currently available for examining the relationship between specific risk factors and suicide (Cavanagh, Carson, Sharpe, & Lawrie, 2003), it has methodological limitations associated with the reliability on the accuracy of accounts from proxies, as well as potential bias from both proxies and interviewers (Hjelmeland, Dieserud, Dyregrov, Knizek & Leenaars, 2012; Milner et al., 2012). Attention also should be given to the possibility of either over- or under-diagnosing mental disorders, as well as retrospective and recall bias in suicide research using psychological autopsy methodology (Milner et al., 2012).
Conclusion
The results of this multi-dimensional and innovative research project confirmed the existence of several distinct characteristics of young males that die by suicide in the absence of any identifiable diagnosis of psychiatric disorder. The results also indicate the need for improved protocols for identifying individuals without a psychiatric diagnosis who may be at risk, as these people are often invisible to the existing health care and psychosocial services (Law et al., 2014). These findings highlight the need for researchers, policy-makers, practitioners and the general public to recognise suicide as related to a wider and complex set of social and cultural factors. Increased knowledge of risk factors for suicide among young males without a diagnosable psychiatric condition can lead to the development of evidence-based prevention and early intervention programmes for young males at high suicide risk who do not come to the attention of medical and psychiatric services.
Footnotes
Acknowledgements
The authors would like to thank Dr Hugh Simpson and Dr Darren Cowley who made the clinical diagnoses for the cases. The authors would also like to acknowledge the clinical interviewers Davina Donovan and Trudi Little and project manager Jerneja Sveticic. The authors acknowledge their industry partner in the project, the Queensland Office of the State Coroner.
Author contribution
D.D.L. designed the study and V.R. and K.K. conducted the analysis. V.R. drafted the initial manuscript and K.K. and D.D.L. contributed to the final draft. All authors contributed to and have approved the final manuscript.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by the Australian Research Council (DP0881331).