
Abstract
Background:
Self-harm (defined here as an act of intentionally causing harm to own self, irrespective of the type, motive or suicidal intent) is one of the strongest antecedents of suicide in youth. While there have been a number of studies of youth self-harm in low- and middle-income countries (LMICs), there is currently no systematic review of studies of prevalence rates and risk and protective factors.
Aim:
To systematically review the evidence relating to the prevalence rates and forms of self-harm in youth in LMICs and its relationship to family economic status, family functioning, relationship with the peer group, social relationships and academic performance.
Methods:
Electronic searches of three databases, MEDLINE, PsycINFO and Scopus, were performed. In total, 27 school-, community- and hospital-based studies evaluating self-harm in LMICs with youth focus (with participants between 12 and 25 years) were included.
Results:
The self-harm was divided into suicidal and non-suicidal depending on the nature of self-harm. The 12-month prevalence rates of non-suicidal self-harm varied from 15.5% to 31.3%, and the range of suicidal behaviour rates was from 3.2% to 4.7%. Banging and hitting were the most common in the community-based studies, followed by cutting, scratching and wound picking. Self-poisoning with pesticides was most commonly reported in hospital-based studies. Risk factors for self-harm were family conflict, peer groups with members indulging in self-harm, truancy and school absenteeism. Protective factors were having an understanding family, having friends and higher school competence. Risk factors for suicidal thoughts and attempts were lack of close friends and history of suicide by a friend.
Conclusion:
The 12-month prevalence rates of youth self-harm in LMICs are comparable to high-income countries (HICs). The profile of risk and protective factors suggests that family-based interventions could be useful in treatment and prevention. Future studies should aim for greater consistency in assessment methods and the constructs under evaluation.
Background
Suicide in youth is a major public health concern in low- and middle-income countries (LMICs; McKinnon, Gariepy, Sentenac, & Elgar, 2016; Sidhartha & Jena, 2006). It is the second biggest cause of death in those aged 15–29 years in India (Patel et al., 2012), the world’s largest democracy and the home to its largest adolescent population. Self-harm is defined as an act of intentionally causing harm to own self, irrespective of the type, motive or suicidal intent (Hawton et al., 2003; National Collaborating Centre for Mental Health, 2012). Self-harm predicts an elevated risk of future suicide by 30–100 times as compared to the general population in the following year (Cooper et al., 2005; Hawton et al., 2015; Whitlock et al., 2013). The studies in adults suggest that the risk persists beyond the first year with 1 in 15 dying by suicide after 9 or more years following the self-harm attempt (Owens, Horrocks, & House, 2002). The risk increases with the number of self-harm episodes and is more prominent in those aged 10–24 years as compared to older age groups (Zahl & Hawton, 2004).
Various terms are used to describe self-harm such as self-harm behaviour (Washburn et al.), self-injurious behaviour, deliberate self-harm (DSH), self-mutilatory behaviour (SMB) and suicidal behaviour. Sometimes suicide intent is used to make a dichotomous separation between suicidal and non-suicidal self-harm. Non-suicidal self-injury (NSSI) is one such term defined as a deliberate direct destruction or alteration of body tissue without a conscious suicidal intent (Whitlock et al., 2013). The substantial overlap of suicidal and non-suicidal self-injurious behaviours, with the dimensional quality of suicidal intent makes this classification arbitrary (Kapur et al., 2013). Thus, many standard guidelines focus on self-harm irrespective of the intent (Hawton et al., 2003; Hawton, Saunders, & O’Connor, 2012; National Collaborating Centre for Mental Health, 2012; Swahn et al., 2012).
Our understanding of self-harm in youth and its relationship with suicide is based on mostly the research conducted in high-income countries (HICs) (Muehlenkamp, Claes, Havertape, & Plener, 2012). About 10% of adolescents in the community harm themselves at some point (Hawton, Rodham, Evans, & Weatherall, 2002; Moran et al., 2012). The risk factors for self-harm and suicide in youth include socio-economic disadvantage and psychiatric illnesses such as depression, anxiety disorders and substance use problems (Hawton et al., 2012; Skegg, 2005). Other important individual- and family-related risk factors include adverse childhood experiences, interpersonal difficulties, parental separation, divorce or death, parental mental disorder and family history of suicidal behaviour (Hawton et al., 2012). Additionally, characteristics related to self-harm that are associated with suicide include male gender, self-harm attempt requiring a hospital presentation and onset of self-harm early in life (Hawton et al., 2012).
A longitudinal study exploring the relationship between NSSI and suicidal behaviour (suicidal-plan and -attempt) in young adults (baseline average age of 20.3 years) found having parents as confidants was protective against transition from NSSI to suicidal behaviour (Whitlock et al., 2013). A good social support, confiding relationship with the family members, religious affiliations, cultural norms and optimistic outlook are some of the other protective factors against self-harm.
The paucity of evidence in this area in LMICs impedes our understanding of origin, purpose and forms of self-harm in youth. Additionally, the societal and cultural differences between LMICs and HICs could have a significant impact on the overall presentation and course of self-harm in youth (Amitai & Apter, 2012; Muehlenkamp et al., 2012). This is important as the role of overarching culture and specific transcultural factors such as the media environment and family structure in self-harm is becoming increasingly clear. There is growing evidence that some cultural factors offer protection from self-harm (Skegg, 2005). For example, the suicide rates are lower in some Catholic and Islam countries where it is strongly disapproved (Skegg, 2005). Furthermore, identifying and addressing the context-specific risk and protective factors are likely to improve the effectiveness of interventions that aim to reduce self-harm.
With this background, we systematically reviewed the current available evidence on self-harm in youth in LMICs with the aim of answering the following research questions:
What is the prevalence of self-harm in youth in LMICs and is it different from HICs?
What are the most common forms of self-harm in youth in LMICs, and in particular, what proportion is suicidal self-harm?
What is the relationship between family economic status, family functioning, peer group, social relationships, academic performance and self-harm in youth in LMICs?
This article is focused on self-harm in 12–25 years old. We chose this age range for a number of reasons, including the lengthening of the period of adolescence with the earlier onset of puberty and the delay in the social transitions related to adulthood such as marriage (Patton et al., 2016). The age range of the current review is broad enough to capture the developmental trajectory of this developmental phase and includes mid-adolescence, a period of higher prevalence of self-harm (Patton et al., 2007). This age range also ensures developmental consistency, as young adults are relatively close in age to older adolescents (Hawton et al., 2012). In most LMICs, young people of this age are still financially dependent on their family members (Lai, 2011). We have included the research articles published in Turkish language to make the review more comprehensive. To our knowledge, this is the first review of its kind.
Method
A systematic search of bibliographic electronic databases, such as MEDLINE, PsycINFO and Scopus, was performed in August 2015. The Covidence software that is used as a primary screening, and data extraction tool for Cochrane authors was used to assist in the production of the systematic review. The following terms formed the basis of the search strategy: ‘self-harm’ OR ‘deliberate self-harm’ OR ‘DSH’ OR ‘self-injurious behavior’ OR self-injury OR ‘self-inflicted wounds’ OR ‘suicide attempt’ OR ‘suicidal behaviour’ AND ‘low middle income country/ies’ OR ‘an individual country from LMIC list (WHO Classification, 135 countries)’. Further papers were identified through hand searching the references of all subsequently included studies and relevant reviews (Figure 1).
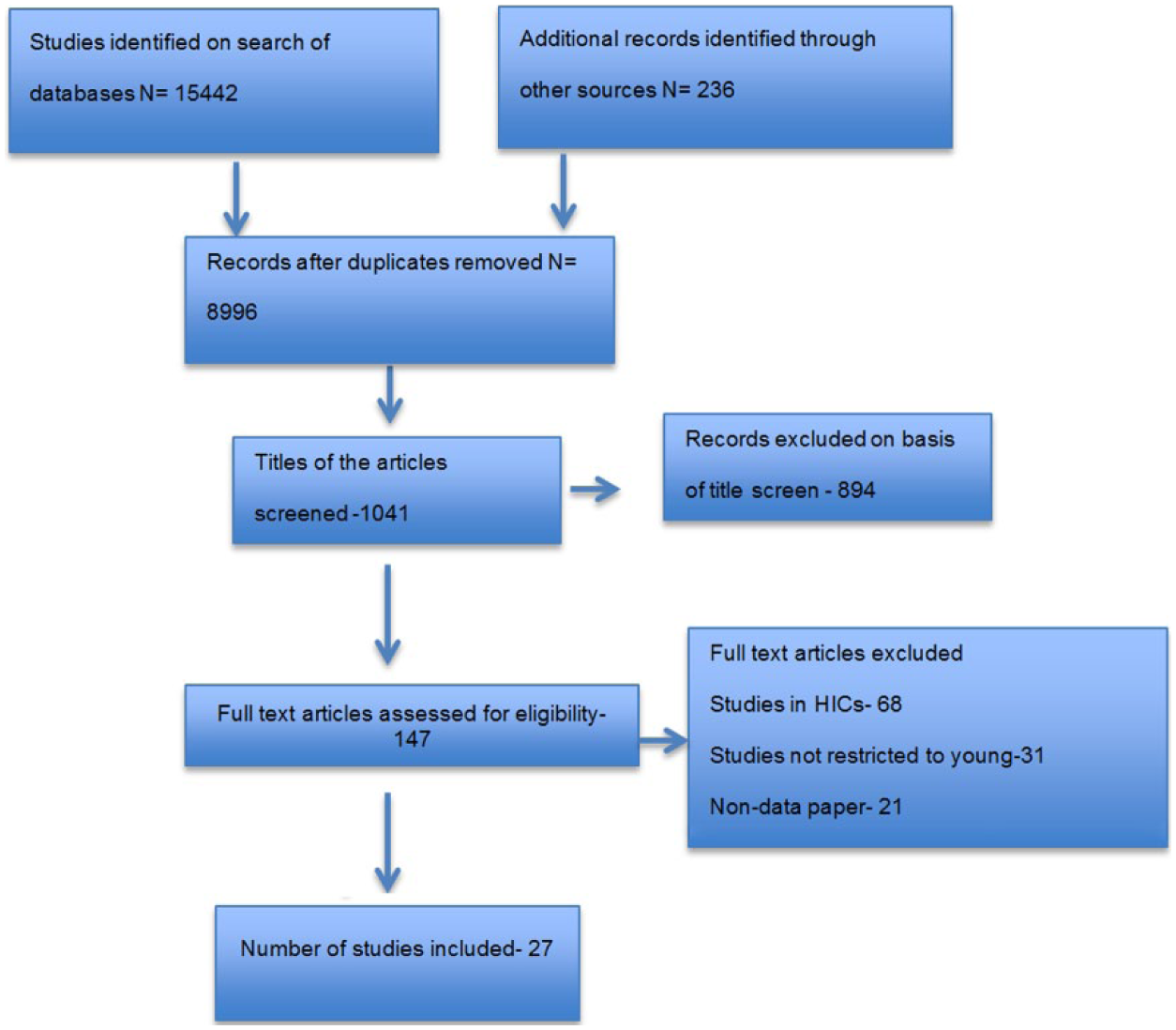
PRISMA study selection flow chart.
Two authors, including the first author, independently screened the titles of all retrieved articles and then conferred to resolve any differences of opinion. Thereafter, the same authors assessed the relevance and appropriateness of the selected articles by screening the abstracts. The full text versions of potentially relevant articles after screening were assessed for inclusion in the review. The first author and a co-author classified all studies independently, and disagreements were resolved through discussion in person. The nature of the self-harm (suicidal vs non-suicidal) was decided by the description provided in the study and discussed by the two authors to reach a joint consensus. For example, the construct of DSH has been used to describe both suicidal and non-suicidal self-harm in different studies (Sidhartha & Jena, 2006; Wan, Hu, Hao, Sun, & Tao, 2011).
Inclusion criteria
Cross-sectional, case–control and longitudinal studies were included if they were conducted in a school, community or a hospital setting targeting self-harm or suicidal behaviour, in youth in LMICs. All the included studies had a youth person focus. There were no participants over 25 years of age in any of the studies included.
Exclusion criteria
The following studies were excluded:
Systematic reviews, correspondence, personal viewpoints, brief reports and other non-data articles;
Studies in specific populations in which self-harm is a comorbid condition and not the primary concern or the presenting problem, for example, self-harm in psychosis;
Studies in which the sample mainly consisted of the older adult population with a small proportion of adolescents.
The review conforms to the recommended guidelines by PRISMA 2009 checklist. The quality assessment was performed using the following scales: Newcastle–Ottawa Scale adapted version for cross-sectional studies, Newcastle–Ottawa Scale for case–control studies and quality assessment tool for systematic reviews of observational studies (QATSO) scale for longitudinal studies (Modesti et al., 2016; Wells et al., 2000; Wong, Cheung, & Hart, 2008).
Results
In total, 27 studies were included in the review. Of these, 16 were conducted in the school or community setting and 11 were hospital-based studies. In total, 14 studies were from Turkey and 4 each from China and India. There was one study from Albania, Lithuania, Pakistan, Seychelles and Zambia that met the inclusion criteria (Table 1).
Type of studies and countries.

Prevalence of self-harm
Results showed considerable variation in 12-month prevalence rates of self-harm rates in youth in LMICs. Comparing the prevalence rates between studies is complicated by large variations in methodology including differences in the constructs under evaluation and in the ages of the included populations (Appendices 1–4). Eight studies assessed self-harm prevalence rates over the previous 12 months (Table 2). One study evaluated both non-suicidal and suicidal self-harm separately and tried to explore the relationship between them (Tang et al., 2011). All the others focused on either suicidal or non-suicidal self-harm (Evren, Evren, Bozkurt, & Can, 2014; Kharsati & Bhola, 2015; Muula, Kazembe, Rudatsikira, & Siziya, 2008; Sidhartha & Jena, 2006; Somer et al., 2015; Wan et al., 2011; Wilson, Dunlavy, Viswanathan, & Bovet, 2012).
12-month prevalence (school and community based).
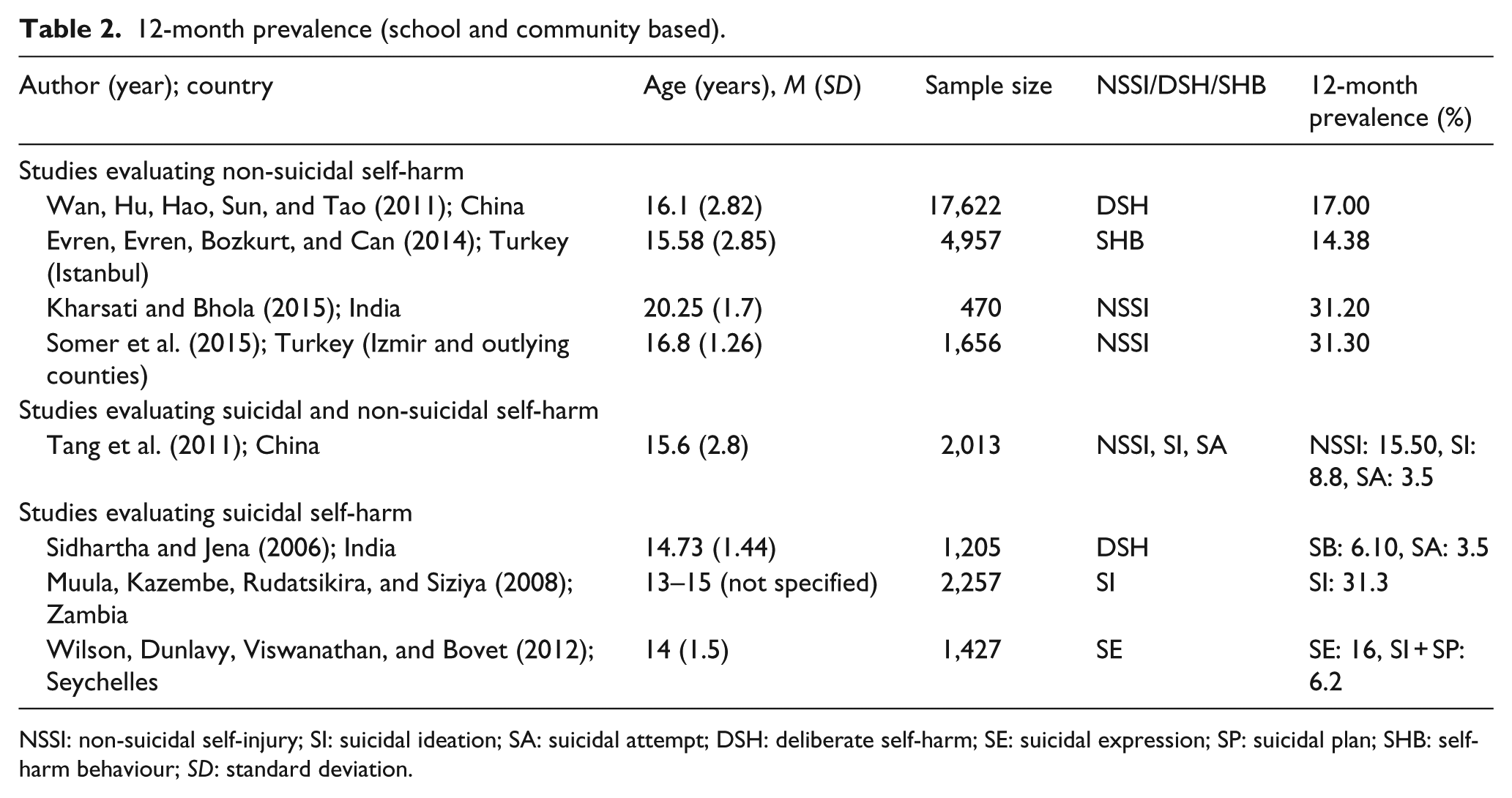
NSSI: non-suicidal self-injury; SI: suicidal ideation; SA: suicidal attempt; DSH: deliberate self-harm; SE: suicidal expression; SP: suicidal plan; SHB: self-harm behaviour; SD: standard deviation.
The rates of non-suicidal self-harm varied from 15.5% to 31.3% (Table 2). The variation is partly been explained by the method of assessment. For example, the rates were higher in the cross-sectional surveys with standardized scales as compared to the interview-based studies or those using branched assessment method (evaluation of self-harm using a single question followed by exploratory questions to ascertain the nature of self-harm in case of an affirmative response; Evren et al., 2014; Kharsati & Bhola, 2015; Somer et al., 2015; Wan et al., 2011).
There was a very little variation in the rates of suicide attempt in the studies. However, the rates of suicidal thoughts in adolescents in Zambia were much higher as compared to China and India (Muula et al., 2008; Sidhartha & Jena, 2006; Tang et al., 2011; Table 2).
Form of self-harm
In total, six school- and community-based (Aktepe, Çalişkan, & Sönmez, 2014; Kharsati & Bhola, 2015; Somer et al., 2015; Tang et al., 2011; Wan et al., 2011; Zoroglu et al., 2003) and nine hospital/clinic-based studies reported on the forms of self-harm (Akdemir, Zeki, Ünal, Kara, & Çetin, 2013; Akin & Berkem, 2012; Çelik et al., 2011; Fidan, Ceyhun, & Kirpinar, 2009; Fidan & Kirpinar, 2009; Gökçen & Köylü, 2011; Grover, Sarkar, Chakrabarti, Malhotra, & Avasthi, 2015; Kola, Kola, Petrela, & Zaimi, 2013; Soylu, Taneli, & Taneli, 2013; Syed & Khan, 2008). Banging and hitting were the most common form of self-harm in the community-based studies, followed by cutting, scratching and wound picking (Aktepe et al., 2014; Kharsati & Bhola, 2015; Somer et al., 2015; Tang et al., 2011; Wan et al., 2011; Zoroglu et al., 2003). Burning and use of chemicals were the least common forms of self-harm (Wan et al., 2011; Zoroglu et al., 2003). In the hospital-based studies, self-poisoning was the commonest method (Akin & Berkem, 2012; Çelik et al., 2011; Fidan et al., 2009; Fidan & Kirpinar, 2009; Gökçen & Köylü, 2011; Grover et al., 2015; Kola et al., 2013; Soylu et al., 2013; Syed & Khan, 2008). Pesticides were a common choice of poisoning (Grover et al., 2015; Kola et al., 2013; Syed & Khan, 2008; Tables 3 and 4). The details of the measurement tools used in the various studies are shown in the appendices.
Form of self-harm (school/community-based studies).
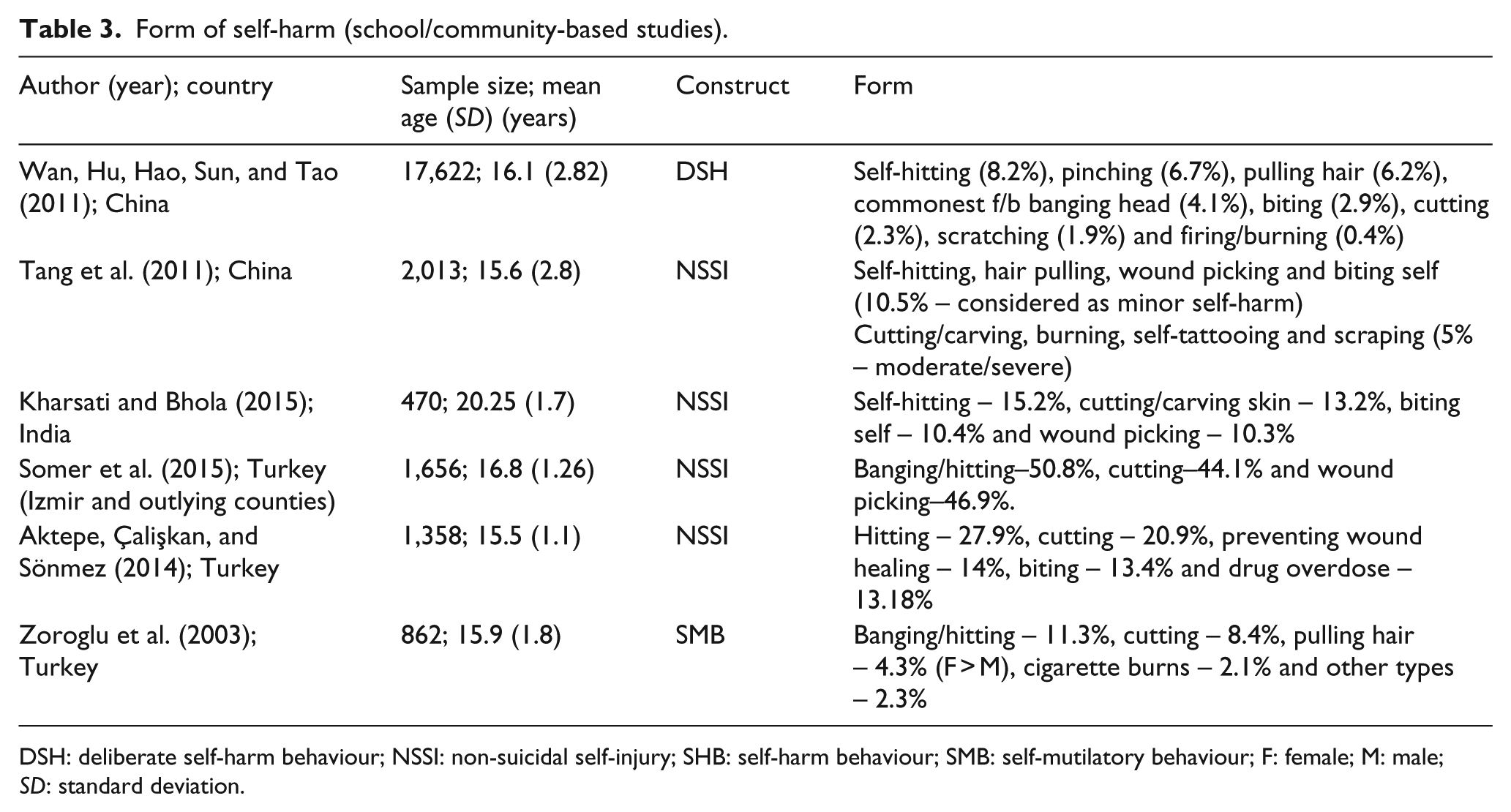
DSH: deliberate self-harm behaviour; NSSI: non-suicidal self-injury; SHB: self-harm behaviour; SMB: self-mutilatory behaviour; F: female; M: male; SD: standard deviation.
Form of self-harm (clinic/hospital-based studies).
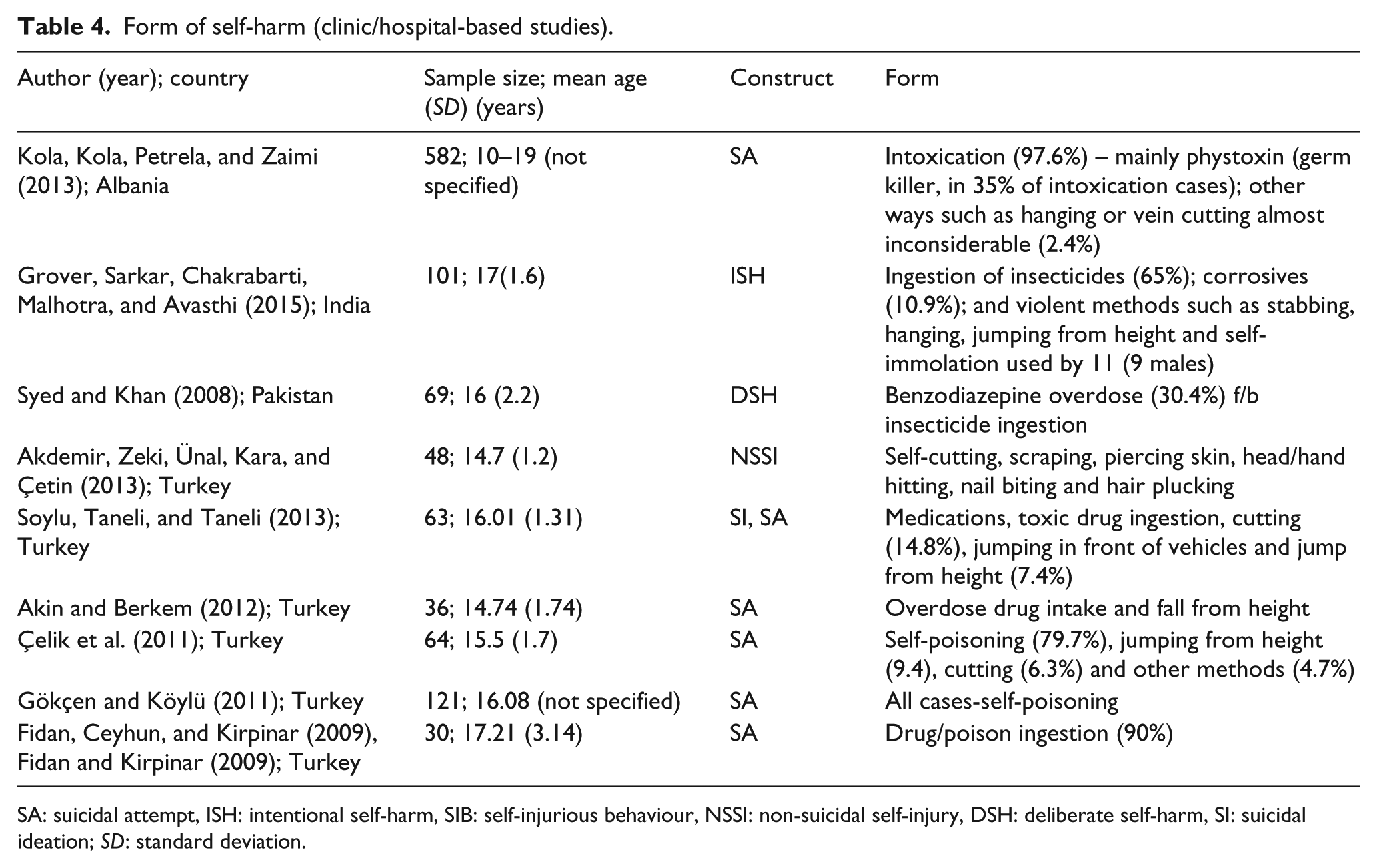
SA: suicidal attempt, ISH: intentional self-harm, SIB: self-injurious behaviour, NSSI: non-suicidal self-injury, DSH: deliberate self-harm, SI: suicidal ideation; SD: standard deviation.
Risk and protective factors
We classified the risk and protective factors into three domains, that is, family-related factors, peer-related factors, and school-related factors (Table 5). We have focused on the school- and community-based studies exploring the risk factors for self-harm for a period of up to 12 months preceding a self-harm episode for the conclusions to be generalizable and the association to be most relevant.
Risk and protective factors for self-harm (school/community-based studies).
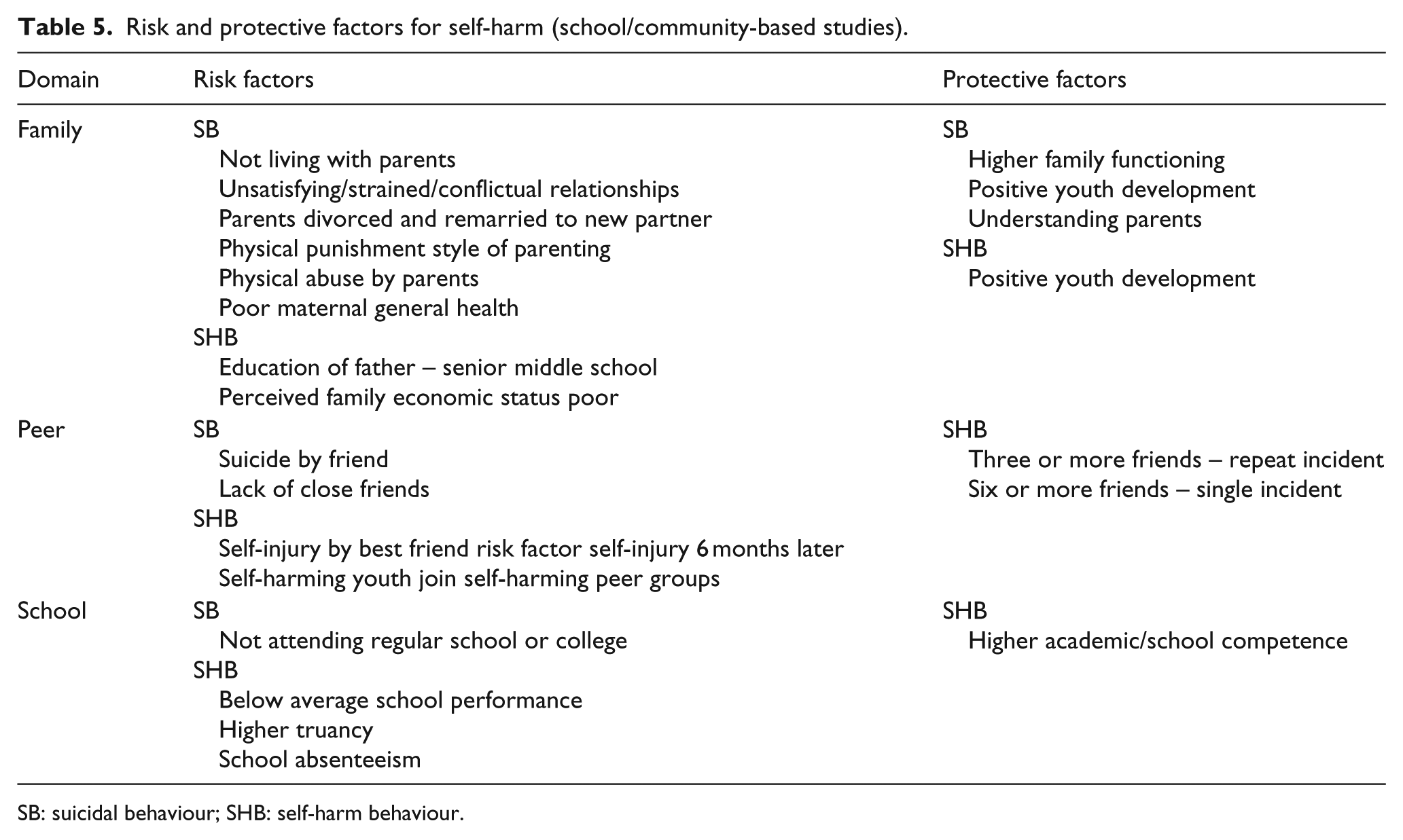
SB: suicidal behaviour; SHB: self-harm behaviour.
Family-related factors
A couple of studies found higher family functioning to be protective against self-harm (Law & Shek, 2013; Shek & Yu, 2012). Additionally, two other studies established unsatisfying/strained/conflictual familial relationships, divorced parents with new partners and negative opinion of family members as risk factors for self-harm and suicidal behaviour (Pillai, Andrews, & Patel, 2009; Shek & Yu, 2012). An understanding set of parents was protective against suicidal behaviour (Wilson et al., 2012). Parental neglect, physical abuse by parents and authoritarian discipline style were the other risk factors identified for suicidal behaviour (Pillai et al., 2009; Sidhartha & Jena, 2006). Perceived and real socio-economic status of the family as poor was significantly related to self-harm (Shek & Yu, 2012; Wan et al., 2011). There was some evidence for the association of poor maternal general health with suicidal behaviour and the education level of fathers having been restricted to senior middle school with self-harm in youth (Liu, Sun, & Yang, 2008; Wan et al., 2011).
Peer-related factors
Lack of close friends (Wilson et al., 2012) and history of suicide by a friend (Sidhartha & Jena, 2006) were identified as risk factors for suicidal thoughts and attempts. In one study, having three or more friends was protective against repeated self-harm and having six or more friends was protective against a single self-harm episode (Wan et al., 2011). In another study, self-injury by the best friend was predictive of self-injury in youth 6 months later. Additionally, youth indulging in self-harm were more likely to join peer groups with self-injuring members at 6-month follow-up (You, Lin, Fu, & Leung, 2013). Also, one study found that the negative opinion of the family members of the peer group was significantly associated with self-harm in youth (Evren et al., 2014).
School-related factors
Below average school performance, truancy, school absenteeism and dropping out of school or college were significantly associated with self-harm (Evren et al., 2014; Pillai et al., 2009). Higher academic achievement and superior school competence were associated with lower incidence of self-harm (Shek & Yu, 2012). Furthermore, there were a few studies reporting a correlation between substance use and self-harm behaviours (Evren et al., 2014; Toprak, Cetin, Guven, Can, & Demircan, 2011; Table 5).
Important findings that need replication
In a large community-based study in a rural India, loss of traditional lifestyles indexed by behaviours such as premarital sex and independent decision-making was associated with increased suicidal behaviour in young women (Pillai et al., 2009).
Discussion
This review, the first of its kind to review the evidence for the prevalence rates of self-harm in youth in LMICs, as well as the associated risk and protective factors, identified 27 studies from eight countries. The prevalence rates of non-suicidal self-harm in LMICs varied from 15.5% to 31.3%. This range is comparable to 12-month prevalence rates of NSSI (7.3%–37.2%) in HICs (Moran et al., 2012; Muehlenkamp et al., 2012). Furthermore, the 12-month prevalence rates of suicide attempts of 3.2%–4.7% are similar to HICs (Cash & Bridge, 2009).
Hitting is the commonest method of non-suicidal self-harm followed by cutting, wound picking and biting (Table 5). These findings are similar to the available evidence from HICs of NSSI generally involving low lethality methods (e.g. cutting, burning and biting) as opposed to suicidal behaviour that tends to involve high lethality methods (e.g. overdose, wrist cutting and hanging; Hamza, Stewart, & Willoughby, 2012).
Self-poisoning is the commonest method of suicide attempt in youth in LMICs according to the hospital-based studies (Akin & Berkem, 2012; Çelik et al., 2011; Fidan & Kirpinar, 2009; Gökçen & Köylü, 2011; Kola et al., 2013; Soylu et al., 2013). In a large hospital-based study conducted in Sri Lanka, the authors found that most of the suicide attempts were using pesticides and were precipitated by triggers in the social environment (Konradsen, Van Der Hoek, & Peiris, 2006). There was no demarcation between suicidal and non-suicidal self-harm in a couple of studies that used constructs such as intentional self-harm and DSH to evaluate self-harm (Grover et al., 2015; Syed & Khan, 2008). Poisoning remained the commonest method in these studies. This could mean that the demarcation between suicidal and non-suicidal self-harm may be comparatively blurred in LMICs.
In many studies, the pesticides stored in the household were used for poisoning (Grover et al., 2015; Kola et al., 2013; Syed & Khan, 2008). An additional method of self-poisoning was the use of pharmaceutical drugs (Kola et al., 2013; Syed & Khan, 2008), many of which are classified as restricted in HICs requiring a doctor’s prescription. These medicines are freely available without a doctor’s prescription in LMICs. These factors become important while planning any suicide/self-harm prevention programmes by restriction of means. For example, a central pesticide storage facility was proven to be an effective measure in reducing completed and attempted suicide in Southern India (Vijayakumar et al., 2013).
There are limited studies that have explored the risk and protective factors for self-harm in youth in LMICs making the comparisons with the evidence from HICs harder. However, this review provides us with a few helpful insights into the risk factors associated with self-harm in youth in this context and what possibly could be protective towards it. The most robust finding of the current review is the importance of family-related factors such as unsatisfying/strained/conflictual familial relationships, divorced parents with new partners and childhood abuse and maltreatment as risk factors for self-harm and suicidal behaviour in youth in LMICs (Table 5). A couple of studies found an association between low paternal education and self-harm (Oksuz & Malhan, 2005; Wan et al., 2011). These associations are similar to those found in studies conducted in HICs (Beautrais, 2000; Skegg, 2005). An adequate parenting is essential for the development of social skills required for effective interpersonal functioning during adolescence, and a lack of it could result in increasing the risk of self-harm (Beautrais, 2000). The protective function of higher family functioning and understanding parents with regard to self-harm in LMICs could be attributable to dense family networks and greater reliance of youth on their family in this context as compared to many western countries (Aggarwal & Berk, 2015a). Thus, interventions with an incorporated family component could work better for self-harm in youth in LMICs. There is some evidence for the effectiveness of interpersonal psychotherapy in self-harm in young people (Washburn et al., 2012). Further research will be needed in LMICs to see how effective the existing evidence-based approaches are for self-harm and whether a family-related component could be incorporated to make them better suited to the local conditions.
Formation of peer groups and establishing friendships is an important psychosocial maturational task of adolescence. It becomes all the more important in LMICs due to the dense and proximal social networks that most of them share (Aggarwal & Berk, 2015b). Furthermore, the social networks act as reliable source of multiple types of support in LMICs (Perkins, Subramanian, & Christakis, 2015). Not participating in these social connections, being excluded from desirable groups or negative feedback from peers could result in negative impacts on the adolescent identity formation (Harter, Stocker, & Robinson, 1996). The self-harm could occur in the friendship groups by selection effects (where adolescents befriend peers already indulging in the behaviour) or socialization effects (where they start doing it to win the approval of peers and for social conformity; Prinstein et al., 2010).
Some indirect association has been found between school-related factors such as below average school performance and negative attitude towards school and school work with suicidal behaviour in studies in HICs (Evans, Hawton, & Rodham, 2004). The higher school functioning was found to be protective against self-harm in a study with poor academic performance, truancy and school absenteeism identified as risk factors for self-harm in youth in many studies (Evren et al., 2014; Shek & Yu, 2012). This could be due to the higher value placed at academic achievement in LMICs and the stress that ensues due to poor academic performance (Aggarwal & Berk, 2015b).
Conclusion
The available evidence suggests that the 12-month prevalence rates of self-harm in LMICs in youth are comparable to those in HICs. The risk and protective factors for self-harm in youth in LMICs identified in the review require further investigation due to the limited evidence and the variability in the assessment methods, as well as the constructs studied. The distinction between suicidal and non-suicidal self-harm is blurred, and these constructs are very often used interchangeably. The association between family functioning and self-harm suggests that family-based interventions could be useful for treating and preventing self-harm in young in LMICs. More research in this area could give us clarity about the mechanisms leading to and maintaining self-harm in youth, the relationship between self-harm and suicide in adolescents and young adults in LMICs and will help in devising effective intervention programmes in this setting.
Footnotes
Appendix
Hospital/outpatient clinic-based studies on self-harm (non-English language).

| Turkey (Soylu, Taneli, & Taneli, 2013) | University hospital–based cross-sectional study (June 2008–March 2009) | Social, emotional and cognitive factors leading to SI and SA in patients with MDD | 63 cases between ages 12 and 18 years Mean age: 16.01 years (SD: 1.31 years) |
Children’s Depression Inventory (CDI) State-Trait Anxiety Inventory (STAI-I, II) Beck Hopelessness Scale Coppersmith Self-Esteem Inventory Multi Dimensional Perceived Social Support Scale Strengths and Difficulties Questionnaire (SDQ) |
Prevalence: not assessed Form of self-harm: medications, toxic drug ingestion, cutting (14.8%), jumping in front of vehicles and high-jump (7.4%) Risk factors for SI: high depression and anxiety levels, hopelessness and low self-esteem. Risk factors for SA: separated family background, lower family support and conduct difficulties |
5/10, as per Newcastle–Ottawa Scale adapted for cross-sectional studies |
| Turkey (Elif and Berkem, 2013) | University hospital–based case–control study (June 2009–May 2010) | Adverse Life events in adolescent SA | 36 cases between ages 12 and18 years Mean age: 14.74 years (SD: 1.74 years) 34 controls between ages 12 and 18 years Mean age: 14.42 years (SD: 1.43 years) |
Adverse Life Events List | Prevalence: not assessed Form of self-harm: not described Risk factors: adverse life events, poor school performance, family history of mental/emotional problems, negative financial state of family, separation from significant other and school failure |
4/10, as per Newcastle–Ottawa Scale adapted for cross-sectional studies |
| Turkey (Akdemir, Zeki, Ünal, Kara, & Çetin, 2013) | University hospital–based cross-sectional case–control study | NSSI and its a/w psychiatric symptoms, identity formation, self-esteem | 48 cases between 12 and 17 years Mean age: 14.7 years (SD: 1.2 years) 49 controls between 12 and 17 years Mean age: 14.7 years (SD: 1.5 years) |
Brief Symptom Inventory (BSI) Sense of Identity Assessment Form (KDE) Rosenberg Self-Esteem Inventory (RSES) |
Prevalence: not assessed Forms of self-harm: self-cutting, scraping, piercing skin, head/hand hitting, nail biting and hair plucking Risk factors: F > M, low self-esteem, associated psychiatry behaviours such as MDD and conduct disorder |
6/10, as per Newcastle–Ottawa Scale adapted for cross-sectional studies |
| Turkey (Akin & Berkem, 2012) | University hospital–based retrospective case–control study from 2009 to 2010 | SA and its a/w anger and impulsivity | 36 cases of SA between ages 12 and 18 years Mean age: 14.74 years (SD: 1.74 years) 34 healthy subjects as controls Mean age: 14.42 years (SD: 1.43 years) |
Kiddie Schedule for Affective Disorders and Schizophrenia Present and Lifetime Version Spielberg State-Trait Anger Expression Inventory (SSTAEI) Barratt’s Impulsivity Scale (BIS) Suicide Intent Scale (SIS) Wechsler Intelligence Scale for Children–Revised (WISC-R) |
Prevalence: not assessed Form of self-harm: overdose drug intake and fall from height Risk factors: F > M, depression, ADHD, conduct disorder, anger a/w SA and impulsivity a/w SA |
4/10, NOS-A |
| Turkey (Çelik et al., 2011) | University hospital–based cross-sectional assessment | SA and its r/w self-image, domestic violence and socio-demographic variables | 64 adolescents 12–18 years Mean age: 15.5 years (SD: 1.7 years), M: 25%, F: 75% |
Offer Self-Image Questionnaire (OSIQ) Child Depression Inventory (CDI) State-Trait Anxiety Inventory For Children (STAIC) Martial Adjustment Test (MAT) Diagnosis and severity evaluated according to DSM-IV criteria and Clinical Global Impression Scale |
Prevalence: first SA (70.3%), second SA (18.8%) and third SA (10.9%) Form of self-harm: self-poisoning (79.7%), jumping from height (9.4), cutting (6.3%) and other methods (4.7%) Risk factors: mood disorders, substance use, conflict with family a/w first SA, subsequent SA a/w problems in romantic relationships and grief and loss |
4/10, NOS-A |
| Turkey (Gökçen & Köylü, 2011) | University hospital–based study from 2009 to 2010 | SA | 121 adolescents 12–18 years, mean age: 16.08 years, M: 17.4%, F: 82.6% | Hospital administered ‘Suicide Attempt Record Form’ and evaluation by the hospital ‘Psychosocial Support Unit’ | Prevalence: first SA (81.8%) and second SA (18.2%) Form of self-harm: all cases self-poisoning Risk factors: school problems (38.8%), problems with other gender (21.5%), familial problems (14%) and other (25.7%) Preponderance of female gender in sample, 23.1% treated for psychiatric disorders in previous 6 months |
|
| Turkey (Fidan, Ceyhun, & Kirpinar, 2009) | University hospital–based case–control study | SA and family functionality |
30 cases of SA between ages 11 and 22 years |
Socio-demographic Form |
Prevalence: not assessed |
4/10, NOS-A |
DSH: deliberate self-harm; SHB: self-harm behaviour; SIB: self-injurious behaviour; NSSI: non-suicidal self-injury; NFSB: non-fatal suicidal behaviour; SB: suicidal behaviour; SA: suicide attempt; SI: suicidal ideations; a/w: associated with; r/t: related to; r/w: relation with; NOS-A: Newcastle–Ottawa Scale adapted; F: female; M: male.
Conflict of interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.B. is supported by a NHMRC Senior Principal Research Fellowship 1059660. G.P. is supported by a NHMRC Senior Principal Research Fellowship 1117873. N.R. is supported by a NHMRC Career Development Fellowship 1083394.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.