
Abstract
Background:
The individual placement and support (IPS) intervention supports persons with severe mental illness in achieving competitive employment. Although the IPS intervention is labelled a recovery-oriented intervention, little is known about how participants experience IPS to influence recovery. The aim was to investigate how IPS and employment influence recovery in persons with severe mental illness.
Material:
A qualitative phenomenological hermeneutic study of experiences of 12 participants in IPS.
Discussion and conclusion:
IPS and competitive work have an impact on personal recovery, may influence work functioning and decrease depressive symptoms, but do not seem to have an impact on psychotic symptoms.
Keywords
Introduction
Employment is a frequently stated life goal among persons with severe mental illness (SMI) (Bengtsson-Tops & Hansson, 1999; Ramsay et al., 2011). In spite of the desire to work, employment rates among persons with SMI are low (Greve & Nielsen, 2013; Lerner & Henke, 2008; Marwaha, Durrani, & Singh, 2013; Marwaha & Johnson, 2004). One way to address this problem is through the evidence-based, recovery-oriented individual placement and support (IPS) intervention which helps persons with SMI achieve competitive employment (Bond, Drake, & Becker, 2008; Kinoshita et al., 2013). IPS is labelled recovery-oriented intervention and the guidelines of IPS (e.g. zero exclusion, attention to participant preferences and time-unlimited individualized support) foster hope, self-determination and social integration (Bond, Salyers, Rollins, Rapp, & Zipple, 2004; Schneider et al., 2009). However, in general, knowledge of the influence of IPS is sparse when measured by recovery outcomes including mental health symptoms, level of function and self-esteem (van Rijn, Carlier, Schuring, & Burdorf, 2016). On the other hand, the main target of IPS, namely, competitive employment, has significantly been associated with an increase in level of function and self-esteem (Charzynska, Kucharska, & Mortimer, 2015; Michon et al., 2014). The important question is whether it is the IPS intervention itself or its main target, competitive employment, which promotes recovery?
One branch of the recovery literature distinguishes between clinical and personal recovery (Davidson, Lawless, & Leary, 2005; Roe, Mashiach-Eizenberg, & Lysaker, 2011; Slade, 2010). Clinical recovery is understood as an outcome, measured by symptom reduction and increased level of function. Personal recovery is seen as a process defined by the individual, not necessarily in terms of symptom reduction, but rather by what helps the individual move beyond the role of being a patient with mental illness. The CHIME framework describes the personal recovery as a process including five elements: Connectedness, Hope and optimism, Identity, Meaning and purpose in life and Empowerment (Leamy, Bird, Le Boutillier, Williams, & Slade, 2011). In this study, recovery is seen as the product of both clinical and personal recovery. In other words, the authors had a predefined concept of recovery, which may differ from how participants perceive recovery. In addition, the multidisciplinary team of authors – psychiatrists, sociologists and nurses – including the perception of the IPS model constitute our pre-understanding. To gain new insights from participants’ experiences, our pre-understanding was attempted to be bracketed (Dahlberg, Dahlberg, & Nyström, 2001). Former qualitative studies have investigated how IPS and employment influence participants but do not use a pre-understanding of recovery (Areberg, Bjorkman, & Bejerholm, 2013; Boyce et al., 2008; Boycott, Akhtar, & Schneider, 2015; Johnson et al., 2009; Koletsi et al., 2009; Lexen, Hofgren, & Bejerholm, 2013).
The aim of the study was to describe how IPS and employment may influence recovery as experienced by persons with SMI.
Method
Design
A qualitative phenomenological hermeneutic research design was employed including a reflective lifeworld approach focusing on how the world is experienced by humans (Dahlberg et al., 2001; Malterud, 2011). Through interviews, IPS participants unfolded their experiences of how IPS and employment influenced their recovery.
Study setting
The qualitative study was conducted from December 2015 to March 2016, simultaneously with a randomized controlled trial (RCT), with the purpose of investigating efficacy of the IPS method in Denmark (Christensen et al., 2015). The qualitative study rose during data collection in the RCT. Since supplement of a qualitative study would not in any way interfere with the original RCT design, there were no methodological contradictions in including the qualitative part in this post-protocol way. The IPS intervention was provided by the employment specialist (ES) and followed ‘place and train’ philosophy. Main focus was individualized search for competitive employment based on participant’s preferences, avoiding prevocational training. The intervention was integrated within the mental health services and included ongoing job support and benefit counselling (Drake, Bond, & Becker, 2012). In general, before entering IPS, participants had regular mandatory contact with local vocational authority (job centres), depending on what kind of benefits they received. Often, participants had undergone vocational rehabilitation at job centres in accordance with ‘train and place’ philosophy, with a focus on prevocational training, for example, sheltered employment or internships.
Participants
Participants of the IPS intervention were residents of Copenhagen, assigned to community mental health services and diagnosed with SMI, defined as: schizophrenia, schizotypal or delusional disorders (F20–F29); bipolar disorder (F31); or severe depression (F33), according to WHO International Classification of Diseases version 10 (World Health Organization, 1993). Furthermore, all IPS participants expressed a clear desire for competitive work.
In order to recruit interviewees for the study, a poster was placed in the IPS office waiting area to encourage IPS participants to sign up as interviewees. This way, recruitment of participants was unaffected by IPS staff and mental health personnel. In the data collection period, 175 participants were assigned to the IPS RCT in Copenhagen. A total of 12 signed up for the qualitative study. The diagnoses within the group fell into the categories F2, F31 and F33. Male/female ratio was 9/3, and age range was 28–59 years. Three participants were employed, seven were under education and two were neither working nor taking education during their participation in IPS. Sample size for the study was found sufficient to allow for identification of general themes and followed the concept of information power, as described by Malterud, Siersma, and Guassora (2015). Accordingly, the chosen sample size depended on degree of study aim specificity, sample specificity, use of established theory, quality of dialogue and analysis strategy. The study aim was neither categorized as narrow nor broad rather somewhere in between. In addition, the sample specificity of the study was neither characterized dense nor sparse, rather intermediary. The study used well-established theory from recovery literature; the quality of dialogue was strengthened by three pilot interviews, and the interviewer was an experienced psychiatrist used to perform interviews with the target group.
Data collection
The qualitative interview was found to be a viable mean of acquiring knowledge embedded in participants’ lifeworld (Kvale, 2007). Individual semi-structured interviews were deemed suitable for acquiring an understanding of how IPS and employment influenced recovery. The semi-structured interview guide contained themes related to participants’ reflections regarding (1) Entering IPS; (2) Which elements of IPS were found to be important? (3) Did IPS contribute to personal changes? (4) How and to what extent IPS and work were found to be important to recovery? Prior to data collection, three pilot interviews were performed. Questions were asked in a way that invited participants to describe their experiences. All interviews were performed, audio-recorded and transcribed verbatim by first author. Interviews lasted from 45 to 90 minutes.
Data analysis
Interviews were analysed using Armedio Giorgi’s (1997) phenomenological analysis method, adopted by Kirsti Malterud (2011), consisting of four steps: (1) preliminary themes were identified; (2) preliminary themes formed the foundation for identifying meaning units into different codes; (3) each code contained a number of sub-codes, illuminating different aspects of the code; and (4) essences of codes were summarized generating general categories (see Table 1) and hermeneutic interpretive review of participants’ lived experiences formed part of the discussion.
Coding process.
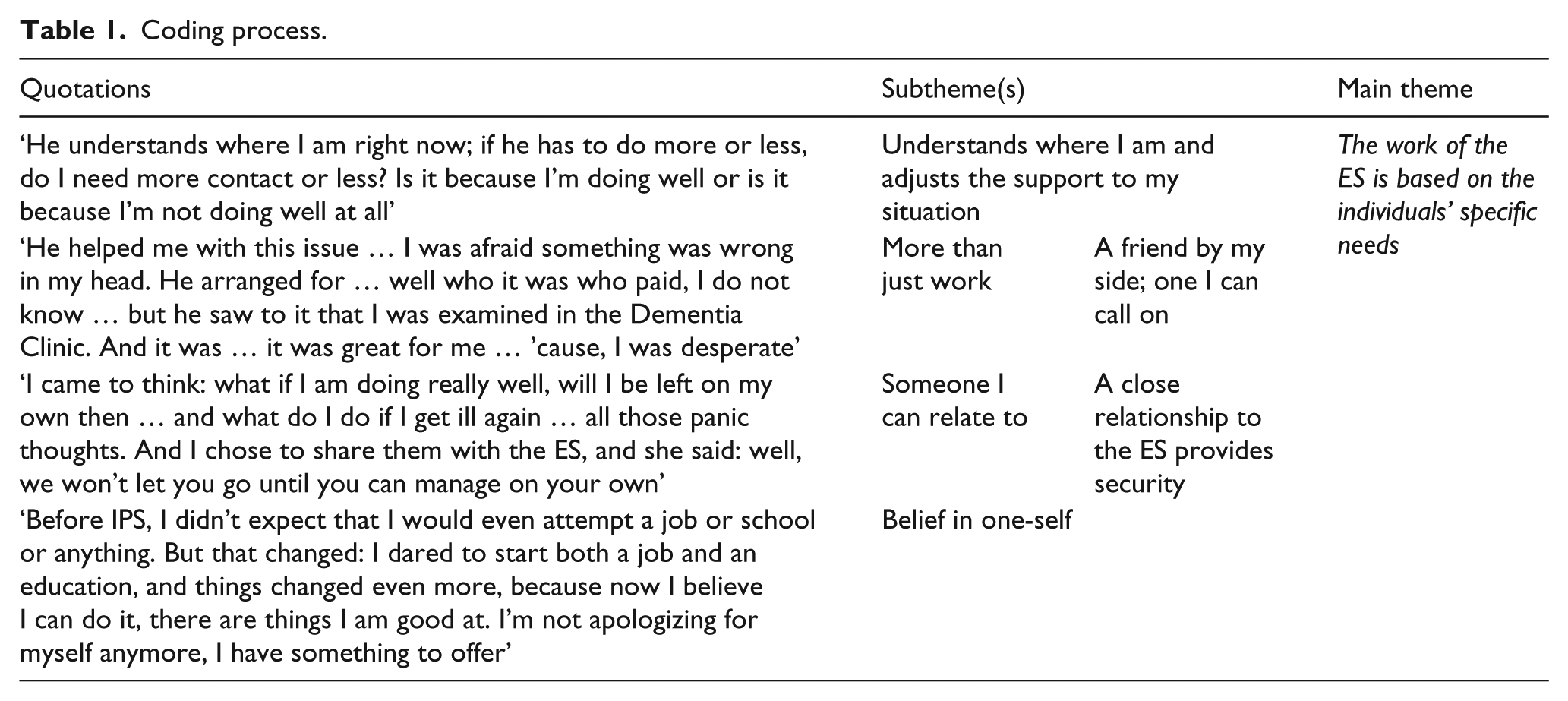
Throughout the research process, authors critically discussed emerging codes and categories. These reflective discussions continued until consensus was reached. Analysis was supported by NVivo 11.0 software.
Ethics
The project is registered with the Danish Data Protection Agency (j.no. 2008-58-0035) and with the Danish Ethical Committee (j.no. S-20152000-163). All participants were thoroughly informed about the study and gave written consent. All direct references to individuals and all quotations have been anonymized.
Results
The study aimed to describe how IPS and employment might influence participants’ recovery. Overall, for the participants, the ES personified the IPS intervention. The ES was viewed as a supportive, understanding and reassuring person who was able to initiate stalled employment processes and provided an assertive service with close and frequent contact with the IPS participants. According to some participants, recovery was influenced by the IPS intervention through interactions with the ES leading to an increase in self-esteem and skills to change life patterns. Others credited employment with being most influential to their recovery and recognized IPS as an important component in its achievement.
Four main themes of the participants’ experiences emerged: (1) participants hoped IPS improved their job-seeking situation; (2) the work of the ES is based on the individuals’ specific needs; (3) employment considerably impacts everyday life and future plans; and (4) self-esteem, new skills and employment contribute to recovery.
Participants hoped IPS improved their job-seeking situation
When participants described IPS they contrasted it with meetings they had had at job centres, where they were allocated to different case workers. This procedure led to impersonal and unproductive relationships with case workers. Participants described situations where meetings with case workers about their job situation led nowhere:
Well, nothing really happened. When they don’t know, what was decided on at the last meeting and the meeting before that, then obviously, the meeting with them is a waste of time. With IPS we meet more often … they are friendly compared to the job centre […] they do these follow-up meetings all the time, so there is progress.
In other situations, case workers communicated in a condescending way and did not listen to the participants or made no effort to try to understand them:
… he began to provoke me, saying he knew my type and I was just lazy and I was just … and when I picked him up on these statements, I was accused of being psychotic.
Meetings at job centres were described as stressful and contributing to either persistence or aggravation of mental illness. Participants’ expectations of the IPS intervention were dominated by hope of improving their job-seeking situation which they felt was stuck. As well, the opportunity of being assigned to one single ES instead of a variety of case workers was found important.
The work of the ES is based on the individuals’ specific needs
The ES was by participants experienced as a person providing an assertive service, ensuring a close and frequent contact. Participants described a variance of situations where they experienced the ES met their individual needs:
He understands where I am right now; if he has to do more or less, do I need more contact or less?
Participants described the ES as a person who was able to initiate processes in the field of employment but also in other areas where issues seemed to hamper getting into employment. For example, participants experienced psychological support from the ES in situations involving loss of close relatives or crisis with spouse or children. As well, the ES took charge in cases where participants felt shelved by the system:
He helped me with this issue … I was afraid something was wrong in my head. He arranged for … well who it was who paid, I do not know … but he saw to it that I was examined in the Dementia Clinic. And it was … it was great for me … ’cause, I was desperate.
These examples illustrate how the ES temporarily set aside the job-seeking process in order to concentrate about solving aggravating issues important to participants.
The ES encouraged participants to take initiatives and supported them in the job-seeking process, for example, in writing job applications or visiting potential future employers. In those situations, participants felt responsible and in charge as the ES stayed in the background. This was described as crucial to the participants as it contributed to the feeling of being able to handle and control such situations. Participants described the ES as committed and serious about helping them back on track. The ES made them feel trust and security. Other qualities highlighted by the participants when they described how the ES met their needs were openness and honesty:
I came to think: what if I am doing really well, will I be left on my own then … and what do I do if I get ill again … all those panic thoughts. And I chose to share them with the ES, and she said: well, we won’t let you go until you can manage on your own.
Participants described how collaboration with the ES made them feel that they were no longer ‘just a number in the system’. They felt they had someone who listened to them, took them seriously and treated them properly. Being approached in this manner made participants feel that the ES met their needs of being treated respectfully.
The ES influenced participants’ ways of thinking. They felt affirmed by the ES, who made them feel valuable and important. This affirmation was experienced as necessary to participants in order for them to continue to make progress in their job-seeking process:
Before IPS, I didn’t expect that I would even attempt a job or school or anything. But that changed: I dared to start both a job and an education, and things changed even more, because now I believe I can do it, there are things I am good at. I’m not apologizing for myself anymore, I have something to offer.
Being met as a person with individual needs; supported, both in the job-seeking process and in other situations; encouraged and treated respectfully made participants feel acknowledged by the ES. According to participants, this acknowledgement promoted changes in their self-perception and self-esteem. Mental barriers to employment were broken and they developed positive attitudes towards themselves, their decisions and their actions. Participants’ self-perceptions of being capable of succeeding with employment grew during IPS.
Employment considerably impacts everyday life and future plans
To work, to contribute and to have a role in society were important to participants. The fact that other people appreciated the work they did, and depended on it, mattered a great deal. Employment added stability and normality to participants’ everyday lives:
I’m not good at doing nothing. Then I fade away; smoke too much marihuana and stuff. Whereas when I’m out there doing my job, my life gets normal.
The IPS intervention and the employment opportunities generated by it made it easier for participants to fulfil goals and dreams. They realized that life consisted of more than being mentally ill. Employment was connected with being able to buy things without having to turn every penny, travelling abroad or starting a family. Some participants doubted whether they should pursue their dreams:
When it comes to my illness and my diagnoses I’m very much in doubt; should I have children? If they grew up to be exactly like me, it would be unbearable … then it would be my fault. But to have children and to have my own family – that’s the goal of my life.
Employment influenced participants’ ways of thinking and behaving. They found that employment influenced the structure of their day. Getting up in the morning, having to shop and prepare dinner had for some participants not been part of their everyday lives before employment. Participants also talked about the importance of having colleagues to chat to and build relationships with. Social aspects such as colleagues saying ‘Good morning’, showing concern for them and asking them ‘how their weekend had been’ contributed to a feeling of inclusion. One participant described how he managed to turn the strict hierarchy at work, the ‘you won’t be spared’ mentality, into something useful:
It runs from the top and down, and the person lower down is the one who takes all the crap … You won’t be spared […] But I choose to look at it positively … it teaches me to be able to handle things … to face the world the way it is.
The psychological working environment influenced participants’ feelings of fellowship and helped them adapt to workplace mentality.
Self-esteem, new skills and employment contribute to recovery
There were nuances in the ways in which participants attributed to IPS influence on recovery. Some participants considered increased self-esteem and skills to change life patterns as components involved in recovery. They perceived those components as having been positively influenced by IPS:
IPS changes the way I look at myself … when other people look at me in a positive way … I don’t feel I’m a burden or inadequate … it makes me feel human. […] actually, it’s atypical for me to handle conflicts at work like this […] I simply chose not to respond to anything they were accusing me of … just letting people calm down.
Others specified employment as most influential to their recovery and recognized IPS as an important component in gaining it. Employment contributed to daily structure, financial flexibility, shared fellowship with colleagues, feelings of being part of society and getting closer to realizing dreams and goals.
Others, who understood recovery as correlated to reduction in mental health symptoms, did not attribute to IPS or employment any influence over their recovery:
IPS doesn’t eliminate the symptoms plaguing me all of the time … I can’t walk down the street without getting the feeling that the cars are about to hit me or that the sound of people’s talk is getting too loud for my ears.
Recovery was variously understood by participants, which explains the discrepancy of views on how IPS and employment influenced recovery. To some, IPS contributed to recovery by promoting self-esteem and skills to change life patterns. To others, IPS contributed indirectly to recovery through generated employment opportunities. And to others again, neither IPS nor employment contributed to recovery since the intervention failed to reduce mental health symptoms. Those who shared the last opinion were plagued by psychotic symptoms, whereas those who took the previous two viewpoints experienced negative and depressive symptoms, and none or milder intermittent psychotic symptoms.
Discussion
The study results emphasize the acknowledging approach used by the ES, which encouraged participants’ initiatives, increased self-esteem and influenced the skills to change life patterns. The ES was confidence-inspiring, serious in helping participants back on track and respectful in the support. Employment influenced structure of the day, expanded participants’ network and brought them closer to realizing goals and dreams. The study presents reasonable explanation of how IPS and employment may influence participants’ personal and clinical recovery.
Personal recovery
The five elements of achieving personal recovery described by CHIME: Connectedness, Hope, Identity, Meaning and purpose in life and Empowerment (Leamy et al., 2011) are reproduced in the study. Participants spoke of being part of society and having supportive, collaborative relationships with professionals as important to recovery. These elements are captured by CHIME’s connectedness category. The hope category entails dreams and aspirations. Both IPS and employment contributed to realization that life amounted to more than being mentally ill. Dreams of being able to travel outside the country or start a family were no longer thought of as unrealistic. The acknowledging approach adopted by the ES which promoted participants’ self-esteem is in line with CHIME’s identity category where a re-definition of a positive sense of identity is key to recovery. This category also embraces professionals’ treatment of consumers as individuals, which participants valued in as much as they felt that the ES listened, treated them properly and seriously. CHIME’s meaning and purpose in life category includes having meaningful social roles. While the IPS intervention in itself does not support this category, the employment opportunities generated by it does. Employment contributed to habits of getting up in the morning, sharing fellowship with colleagues and feelings of being part of society. The empowerment category entails personal responsibility. IPS participants felt responsible and in charge when writing job applications and visiting potential future employers. In those situations the ES stayed in the background, still supportive but without taking the lead. Judging from participants’ experiences, IPS and employment contain elements which can be identified by the five personal recovery processes described by CHIME.
Clinical recovery
The study found nuances in how IPS and employment were perceived to have influenced clinical recovery. Participants suffering from psychotic symptoms were clearly of the opinion that neither IPS nor employment influenced symptom severity. Even though they were capable of finding and keeping a job, they did not consider themselves as being in recovery or having recovered. They identified recovery solely in terms of reduction of mental health symptoms which neither IPS nor employment improved. In contrast to this, participants suffering from negative symptoms or depressive symptoms described how employment helped them get up in the morning and structure the day. Furthermore, fellowship with colleagues was found to be important. Without these elements, the participants explained, they could easily decline into social withdrawal and isolation.
Participants were capable of seeking and maintaining jobs with help and support from the ES. Hereby their level of function increased. However, the study does not give us insight into whether participants reached a level of work function where they could dispense with continuous support or whether the higher level of work function remain dependent on constant job support.
Both Koletsi et al. (2009) and Lexen et al. (2013) report participants experiencing employment distracted them from mental health symptoms. This partly contradicts this study where some participants credited neither work nor IPS with any influence on psychotic symptoms. Participants suffering from psychotic symptoms did neither seem to pay attention to elements of personal recovery as they solely equated recovery with the reduction of mental health symptoms which belong within the category of clinical recovery. These results may suggest that psychotic symptoms could inhibit the personal recovery process. If this is the case, it would imply an existence of an interaction between clinical and personal recovery. In contrast, participants suffering from negative or depressive symptoms felt to a marked degree that being employed influenced their recovery. They credited employment with remedying symptoms of social withdrawal and isolation. CHIME’s Meaning and purpose in life category includes fellowship with colleagues and being able to get up in the morning. These elements of personal recovery influenced the severity of negative and depressive symptoms and hence clinical recovery. This might be a further instance of interaction between personal and clinical recovery and correlates with results from another study investigating the influence of IPS on empowerment (Bejerholm & Bjorkman, 2011). This study found negative correlations between depressive symptoms and empowerment. Davidson et al. (2005) suggested using clinical and personal recovery as complementary concepts for different purposes. Our results may show that IPS and work impact both personal and clinical recovery. Additionally, important interactions between personal and clinical recovery may exist. In order to understand recovery and further develop recovery-oriented interventions, we suggest that future studies focus on the interactions between personal and clinical recovery.
Limitations
Participants of the study were residents of Copenhagen. The study would benefit from the inclusion of IPS participants from other cities or rural districts since culture and mentalities differ in small localities compared to metropolitan centres. Therefore, IPS participants from other locations might have different experiences of job centre case workers and IPS consultants than the participants in Copenhagen. The recruitment strategy, where a poster encouraged IPS participants to sign up as interviewees for a qualitative study, was to avoid selection of a certain participant subgroup. Nevertheless, the interviewees ended up being participants who favoured IPS which should be taken into account when discussing the transferability of findings. To provide a more differentiated picture of participants’ experiences, the ES were asked to encourage critical IPS participants to sign up as interviewees. A longer inclusion period and inclusions of participants from other locations might have led to a more comprehensive account of experiences.
Conclusion
This study indicates that IPS and competitive work might have an impact on personal recovery, may influence work functioning and decrease negative and depressive symptoms, but does not seem to have an impact on psychotic symptoms. The study shows important interactions between personal and clinical recovery.
Footnotes
Acknowledgements
The authors thank the IPS participants. They also thank Bent Nielsen for co-operation and feedback during the research of the study.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by grants from the Region of Southern Denmark and the TRYG Foundation.