
Abstract
Objective:
In Northern Malawi, the duration of untreated psychosis (DUP) is longer than that in high-income countries. The reasons for the delay in help-seeking are not known, although studies show multiple reasons. This research was conducted to establish health care help-seeking behaviours and identify barriers that exist between service users and health care providers. The study also intended to establish the beliefs that clients and family members have regarding the causes of mental illness which profoundly shape help-seeking, care giving process and outcomes.
Methodology:
The study employed the exploratory phenomenological method, utilizing focus group discussions (FGDs) in the sampled population. The Health Belief Model and Disease Explanatory Models were conveniently chosen a priori by researchers to develop guide questions to explore clients’ and carers’ perceptions of the illness and their health care help-seeking behaviours.
Results:
Results show a bio-psycho-social inclination of disease causation and help-seeking behaviour. Causes of mental illness are understood in three categories, namely: physical/biological, psychological and socio-cultural. The majority of participants attributed mental illness to socio-cultural factors, with witchcraft, spirit possession and curses as main determinants. Causal perceptions also influenced help-seeking pathways. Many participants reported consulting traditional healers first, for diagnosis and to know who was responsible.
Conclusion:
In this study, it has been found that help-seeking is influenced by the understanding of the source of the illness – which has a bio-psychosocial inclination. The socio-cultural explanation of witchcraft and spirit possession is dominant and a determinant of help-seeking behaviour. While participants noted benefits to hospital treatment, barriers and bio-psychosocial in nature were also noted. Guardians and not clients hold the key to choice of treatment modality and therefore a potential ally in all treatment interventions promotive, preventive and curative. There is need for strengthening of a bio-psychosocial intervention model in the treatment of mental illness.
Keywords
Introduction and background
Psychotic disorders such as schizophrenia, mood disorders, substance abuse and dementia are the number one contributors to the worldwide burden of non-communicable diseases (Mathers & Loncar, 2006; Murray et al., 2012); according to World Health Organization [WHO] (2003), they contribute about 13% of the global burden of disease. Despite this burden, there still remains a treatment gap in that a large proportion of people with mental illness either delay to access modern mental health services or avoid it all together opting for alternative healing methods (Chilale, Banda, Muyawa, & Kaminga, 2014; MacGlashan, 1999; Marshal, Lewis, Lockwood, Drake, & Joneson, 2005). According to the multicentre survey conducted by WHO, 76%–85% of people with serious mental health problems had received no formal treatment in the duration of 12 months; and for those who did receive treatment, this was most often inadequate (WHO, 2003).
Literature suggests that help-seeking behaviour is also often associated with perceived disease causation (Bartholomew, Parcel, Kok, & Gottlieb, 2006; Haley, Drake, Bentall, & Lewis, 2003; Ilechukwu, 1988; Jones & Bartlett Publishers, 2010; Mbwayo, Ndetei, Mutiso, & Khasakhala, 2013; Rawlett, 2011; Saravanan et al., 2007). Disease causality within health belief and explanatory models has a bio-psychosocial perspective (Caqueo-Urízar, Breslau, & Gilman, 2015; Ilechukwu, 1988); beliefs clients and family members possess regarding the causes of illnesses significantly shape the care giving process (Caqueo-Urízar, 2015; Saravanan, David, Prince, Bhugra, & Jacob, 2005; Saravanan, Jacob, Prince, Bhugra, & David, 2004; Saravanan et al., 2007). Factors that have been linked to both the delay in seeking of help and underutilization of modern health care systems include the belief and explanation that mental illness is caused by spirit possession and witchcraft (Saravanan et al., 2005); stigma, lack of insight and early age of onset (O’callaghan, Turner, Renwick, Jackson, & Sutton, 2010); poor access to services (Broonstra et al., 2012; Mbwayo et al., 2013;); negative symptoms (DeHaan, Van Der Gaag, & Wolthaus, 2000), as well as cognitive barriers (Leong & Lau, 2001). Developing countries are said to be high in socio-cultural attribution of mental illness, that is, spirit possessions, witchcraft, breaking of taboos and curses (Assad et al., 2015; Saravanan et al., 2005).
In Northern Malawi, the duration of untreated psychosis (DUP) has been found to be longer than is the case in high-income countries and the reasons for the delay are not known (Chilale et al., 2014). Thus, this study was conducted to identify health care help-seeking behaviours and possibly identify barriers that may exist between service users (clients and their carers) and health care providers. The study of patients’ and caregivers’ beliefs about the causes of schizophrenia are important because beliefs can influence help-seeking, adherence to treatment, disease management and clinical outcomes (Clark, Whitty, Browne, McTigue, & Kamali, 2006; Marshal et al., 2005; Saravanan et al., 2007); most importantly, delay in help-seeking significantly prolongs suffering and distress to patients and their families, so that examining the help-seeking behaviours for people with an emerging psychotic disorder and their carers would improve our knowledge on mental health care seeking behaviours and offer intervention insights. One way of achieving this is using theoretical models proposed to explaining health care help-seeking behaviours: the Health Belief Models (Bartholomew et al., 2006; Haley et al., 2003; Rawlett, 2011) and the Disease Explanatory Models (Saravanan et al., 2005, 2004).
Health belief model
According to the Health Belief Model, beliefs influence health behaviours and have been shown to influence both health care help-seeking behaviours and outcomes (Haley et al., 2003; Jones & Bartlett Publishers, 2010; Rawlett, 2011). The theory focuses on the experience, attitudes and beliefs of individuals based on the understanding that a person will take a health-related action, for example, seek hospital treatment, only if that person feels or believes that the problem will be alleviated or has positive expectations using this cue (Jones & Bartlett Publishers, 2010). So far, biological, psychological and socio-cultural beliefs are the major known in literature to influence illness attribution and help-seeking (Bartholomew et al., 2006; Haley et al., 2003; Ilechukwu, 1988; Jones & Bartlett Publishers, 2010; Mbwayo et al., 2013; Rawlett, 2011; Saravanan et al., 2005, 2004) There are suggestions that people from developed nations are much more likely to attribute their illnesses to biological and psychological causes while those in developing and collective cultures to supernatural and socio-cultural causes (Assad et al., 2015; Caqueo-Urízar, 2015). Ethnic background has been known to play an important role in the formation of beliefs regarding the causes of schizophrenia (Caqueo-Urízar, 2015). The belief systems of many African people include a major component of the supernatural; this is particularly so in ideas about the causation of psychiatric illness (Saravanan et al., 2007). Thus, to what extent these notions influence treatment choice, when modern psychiatric facilities and Primary Health Workers competent for detection and referral are available, should be a concern to mental health service provision in the developing countries and Malawi in particular.
Much recent work suggests that besides modern health systems, traditional healers are still the most consulted for the treatment of mental illness (Assad et al., 2015); help-seeking behaviour for traditional medicine in developing countries is restricted not only to mental health conditions but also to medical conditions (Abubakar et al., 2013). At least 80% of the people in Africa are estimated to use traditional medicinal sector as their first port of contact for all types of mental and physical health problems (Atindanbila & Thompson, 2011). Usually besides being an important source of support in many parts of the world, including Africa, traditional healers are consulted more because they reinforce a parallel system of beliefs to conventional medicine regarding disease origins and therefore treatment (Mbwayo et al., 2013).
Disease explanatory model
As is the case with attitude and belief formation, different cultures have different ways of understanding and explaining illness; again, these are usually multiple, diverse and often even contradictory (Das, Saravanan, Karunakaran, Manoranjitham, & Ezhilarasu, 2006; Saravanan et al., 2005, 2004) With this diverse ways of understanding illness, this suggests that help is sought from a range of different sources in different cultures. It was therefore imperative that we have a good understanding in this culture on how the service users explained mental illness and what they do when they get ill. In Northern Malawi for example, although primary health services are well established, more than three quarters of patients and their families delay to access mental health services; most will prefer alternative sources of care (Chilale et al., 2014).
Main objective
The main objective of this study was to identify factors that influence health care help-seeking behaviours and possibly identify barriers that may exist between service users and service providers.
Specific objectives
Determine what the clients and carers perceived causes mental illness;
Establish where help is sought first and why;
Establish the cues or benefits to seeking help in a western type hospital;
Establish the barriers, threats and fears to seeking help from the hospital.
Methodology
This research was conducted in compliance with the National Health Sciences Research council of Malawi (NHSRC). The study was conducted in September 2014 through April 2015 among the population where DUP had been found to be 51.7 months (Chilale et al., 2014). The district has relatively homogeneous cultural beliefs.
The study purposively sampled clients recovering from mental health problems (schizophrenia, bipolar affective disorder), recruited from the initial research on the DUP in Northern Malawi (Chilale et al., 2014) and their guardians. There were a total of six homogeneous groups from two respective study zones of the district; three of the groups were formed from the clients and three from the carers in each of the zones, respectively. The groups had a maximum of eight (8) participants. Both male and female clients and their carers aged 18 and above were sampled. Only clients who have a diagnosis of psychosis, who at the time were mentally stable and able to be involved in a discussion were included. A baseline mental status examination was done.
Focus group discussions (FGDs) were conducted once in the sampled population followed by an in-depth probing questions based on the health belief and disease explanatory models on which the guide questions were based. An interview guide was developed in English and then translated into the local language (chiTumbuka) by a group of mental health nurses. The responses from these discussions were written down by the researchers in notes fashion as group members discussed; proceedings were also audio-recorded. These recorded proceedings were later transcribed into chiTumbuka verbatim. The transcribed version of the discussions was later translated into English from which themes were generated using thematic analysis.
Results
There was a male–female client ratio of 1:1 in the FGDs; however, the number of female guardians outnumbered that of males. The majority of the clients were young to middle-aged group whereas the guardians were predominantly female above 40 years of age. The highest educational level attained for both clients and guardians was primary school.
Disease explanation
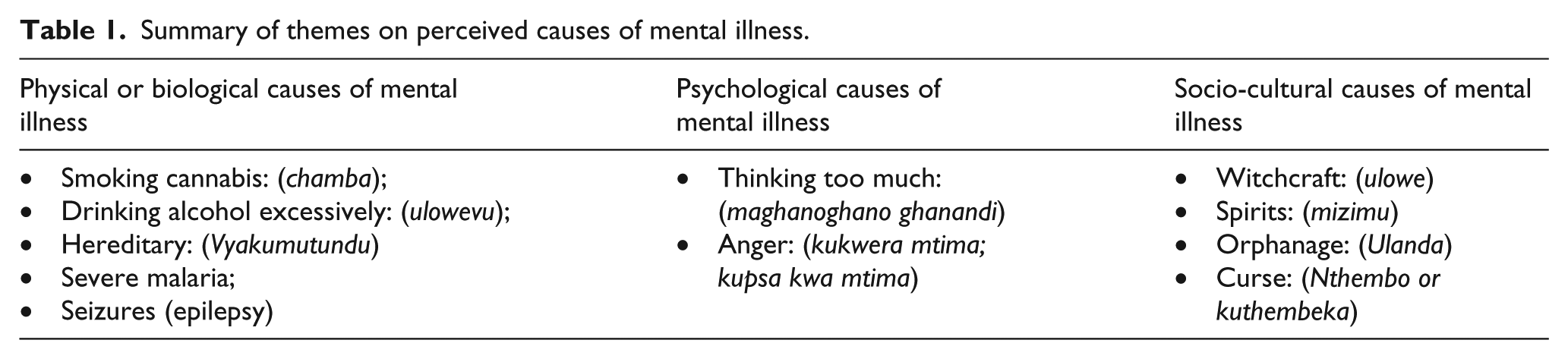
It was clear that participants had multiple versions of what caused mental illness which had influence on where help was sought. Participants’ attributions were summed into three distinct categories as follows: physical or biological, psychological and socio-cultural causes. Physical/biological causes were those attributable to changes in the body and brain functioning; psychological causes were those attributable to changes in thought processes and socio-cultural causes were those attributable to interpersonal and cultural beliefs related to illness causation. The socio-cultural attribution of witchcraft as a cause of mental illness dominated. The summary of the causes of mental illness, from both participants, is presented in Table 1.
Summary of themes on perceived causes of mental illness.
Perceived social-cultural causes
Witchcraft (ulowe)
Witchcraft was attributed by both Clients (C) and Guardians (G) as a main cause of mental illness as is in the quotes below:
… although the government says there is no witchcraft, but people always think of it and tries traditional healers who are believed to be the only people to treat or reverse any illness caused by witchcraft. (G) … he stepped on a trap which was put by someone through witchcraft who wished her bad luck so that something evil happens. (G) … when I felt sick, they took me straight to the traditional healer; this is an indication that when you get sick, it is obvious that someone has bewitched you. (C)
Spirits possession (Mizimu or vinthenda)
Spirit possession was another concept commonly associated with the onset of a mental illness as was indicated in the quotes below:
… mental illnesses are sometimes spirits from unhappy ancestral family members who possess the victim; when that happens, one dances to drums at a traditional healer for healing. (G) Most mentally ill people are considered to be possessed by evil spirits, which the traditional healer tries to reverse or treat by playing drums, so when the patients dance to the tune of these drums then the healing process takes place. (G) Mental illness and spirit possession are associated; if the illness does not show signs of improvement after dancing to drums then this is usually madness (mental illness) and not spirit possession and only then will the patient go to try hospital medicines. (G)
Orphanhood (Ulanda)
Orphanhood was perceived to cause mental illness because it led to having no support which then leads to thinking too much, a trigger of mental illness.
Curse (Nthembo or kuthembeka)
Participants also cited curses to be among the supernatural causes of mental illness where the sick or their relatives are perceived to have broken the taboo or not followed instructions for a particular life event; the quotes below are an example:
Arguing or picking quarrels with your parents is not culturally appropriate and if that happens, you can be cursed because parents are your second ‘god’ so when you disrespect them then you can be cursed. (C) There are people who would like to get rich and they go to medicine men to seek for medicines which should help them get rich or be lucky in whatever way, so if you confuse instructions given to you by the medicine man (traditional healer), the medicine can backfire and turn against one’s own family, causing different kinds of illnesses, which is like a curse. (C)
Perceived physical/biological causes
Smoking cannabis: (chamba) and drinking alcohol excessively (ulowevu)
Smoking cannabis and drinking alcohol excessively were also cited as other causes of mental illness. The quote below is indicative of this:
Some of these mental illnesses are caused by smoking cannabis and drinking alcohol excessively; we know that too much of these cause damage to the brain which lead to one suffering from mental illness. (G)
Severe malaria and epilepsy
Severe malaria and epilepsy were cited by the participants as other causes of mental illness. The quotes below are indicative of this:
Sometimes when you suffer from malaria, it comes too strong and gets into the brain and makes one mad. (C) When the patient has a seizure which throws him or her onto the fire, that one is difficult to heal and makes the patient to behave abnormally, like a mad person. (G)
Running in the family (Vyakumutundu)
Some participants indicated that there are some illnesses, including mental illness, that run in the family (vyakumutundu); however, while the explanation was socio-cultural, that is, curses (nthembo), the authors were of the view that this implied a hereditary or genetic predisposition.
Perceived psychological causes
Thinking too much (maghanoghano ghanandi)
Thinking too much was linked to mental illnesses through negative life events – for example, thinking too much about one’s poverty, domestic problems, sickness or death of a loved one (grief) were all linked to onset of mental illness.
Anger (kukwera mtima; kukwiya)
Anger was also attributed to mental illness. This was described in the same breath as thinking too much; it is the type of anger that was related with failure for a person to let go of the pain of abuse or injustice.
Too much intelligence (mahara ghanandi)
Thinking too much or being too intelligent was associated with mental illness usually common in those people who are perceived to be reading too much, as is in the following quote: ‘When one studies continuously without resting, one is likely to develop a mental illness’ (C).
Where help was sought and justification
Concerning help-seeking, guardians were influential in making decisions; this was evident in both interviews. It was clear that help-seeking was driven by the understanding of what had caused the illness. Many participants reported consulting traditional healers first, as this participant comments,
in the villages when someone gets mentally ill, people just say he has been bewitched or he has been possessed by spirits of his ancestral family; so the traditional healers are consulted to have the illness explained, whether this person is bewitched, possessed by spirits or whether it is natural cause. (C)
One participant called the whole reaction to falling mentally ill and going to traditional healers as a conditioned response in villages,
‘a generational learned response’ (chizgobi); people are just accustomed to go to traditional healers as a way to react when one gets mentally sick. When one gets sick, people usually think he has been bewitched, so there is need to know who has done it and how to treat it. People are usually reluctant to go to the hospital because there is a belief that hospitals cannot cure illness that is due to bewitchment or spirits. (G)
This seemed to augur well with yet another participant who cited social influence as playing a very big role in choosing where people go first … ‘in villages, one will always have people coming in to advise where treatment must be sought and almost always traditional healers are chosen for the treatment of mental illness’ (G).
Barriers to seeking help from hospitals
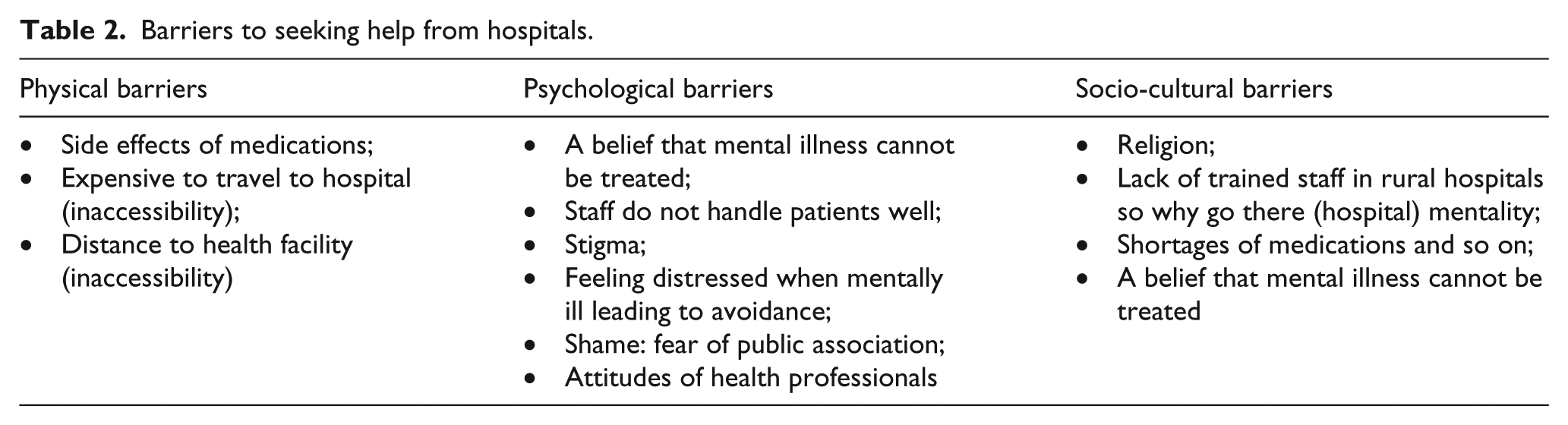
There were several factors that contribute to preventing participants from seeking help from hospitals, which were also categorized as physical, psychological and socio-cultural in nature (see Table 2).
Barriers to seeking help from hospitals.
Participants indicated inaccessibility of services as the number one barrier, as this participant said,
… if you have no money, then you are in trouble as you will have to walk long distances in bushy paths especially during rainy season. Sometimes even after travelling for long distances when you reach at the hospital late you find that the hospital has closed and you have to find somewhere to sleep which is costly; while traditional healers are in every village, you do not have to travel long distances to find one and they do not demand money immediately sometimes you are told to pay when you recover from illness and payments are usually in a form of exchange with domestic animals e.g. a goat, a cow or a chicken which are available and affordable. (C)
Other barriers included religion as this participant said, ‘There are other churches that do not allow their members to go to hospital and this is a big challenge to seeking treatment’ (G).
Poor social support
Other barriers included luck of support at home to be taken to the hospital; as one participant claimed,
the nature of the illness always requires that you have a good support system to be able to be taken to the hospital; but if people who know you well do not take you to hospital then it becomes a challenge, since, as a patient you barely know what is going on. (C)
Side effects as a barrier
Participants pointed out some side effects of medicines as being another barrier to seeking help from hospitals. For example, one participant said, ‘… the medication from hospital gives one very big appetite and makes the patient eat too much, gains a lot of weight and yet he becomes inactive “literary one swells up”’ (C).
Undependable services
Participants also indicated that the services in health centres were undependable and acted as a barrier to seeking help. For example, they cited health centres not opening in good time and scarcity of medications to treat mental illness as major challenges.
Attitude of health workers
Most participants described some health workers as a hindrance to help-seeking and effective treatment in health centres. They cited examples where health workers had been drunk or been unavailable due to alcohol; in other instances, health workers had not paid attention to patients because they are living with a mental illness; they did not take enough time to actively listen to their complaints and sometimes producing prescription even before the patient finishes explaining their complaints. This is exemplified by the quotes below:
Sometimes we come to the hospital and we are told the health worker is not here; and when they show up sometimes they are drunk. (C) Patients with mental illness are not regarded as people; when you come to the hospital there is still this thought that you are sick all the time; you see it from the health workers the way you are treated. (C)
However, besides what were considered systemic barriers, it was also found that some barriers were psychological where participants equally played a role. For example, a belief that spirit possession do not go along with western medication was seen as a socio-cultural barrier feeding into a cognitive spectrum of participants to create a health-seeking barrier. As one of the participants said, ‘My spirits do not accept pills or medication from hospitals’ (C).
Further in the results was the indication that besides external perceived discrimination, some participants seemed to develop self-stigma and discrimination which then became a barrier to help-seeking from the hospital – as is cited in the following quote, ‘sometimes you ask yourself, why should I go to hospital anyway where I am made to feel useless?’ (C)
Benefits of seeking help from hospitals
There are several factors which were viewed as benefits of seeking help from hospitals as follows: reduction of symptoms, improved sense of judgment, social acceptance and peace in the family, looking after one self and participation in the community’s activities.
Reduction of symptoms
As this participant said,
when my husband was sick, he was very violent, he was breaking things in the house, was chasing us out of the house, we were sleeping in the maize garden even during the rainy season. We were living like animals, but now that he is on medication, the symptoms are no longer there and we live together in the house, he is not violent any more. (G)
Another participant had this to say about treatment, social acceptance and re-integration, ‘Other families were afraid of him and us too, but now he has been re-integrated into the family and community’ (G).
Discussion
This study results reveal that there is a mixture of beliefs regarding the causes of mental illness and how these have influence on where help is sought first. A bio-psychosocial explanatory model can be observed in which the socio-cultural representation is dominant consistent with Abubakar and colleagues (2013). In the study, the choice of where to go when one gets sick was highly dependent on guardians influence who opted for one of the forms of treatment and where this did not appear to be working, they switched to the other. Participants consulted western and traditional medicine simultaneously for different reasons as is already alluded to by Assad et al. (2015) and WHO (2003); it was clear, however, from the consensus of participants that there still exists a high preference for traditional healers; this is consistent with other studies (Assad et al., 2015; Chilale et al., 2014; Ngoma, Prince, & Mann, 2003; Sorketti, Zuraida, & Habil, 2012; WHO, 2003). Of interest here is that results indicate complementarity of the two systems and may imply that the efforts to improve access for mental health services in this context cannot ignore traditional health systems.
Factors that played as barriers to seeking help from western hospitals included distance, money for transport, lack of medicine in hospitals, drug side effects and attitude of both service users and health workers. Barriers like distance, poverty, money and lack of medicines are consistent with other studies (WHO, 2003). Service users’ attitudes about health workers being a barrier are considered to be either experiential or as a result of learned negative experiences from other users, which leads to the development of cognitive barriers to seeking hospital services. These attitudes, however, may also be social cognition outcomes emanating from day-to-day interactions within the particular culture about accessibility, affordability, credibility and efficacy of a particular health system (Assad et al., 2015). This may imply that deliberate action be put in place to improve the image of health services.
In this study, it was clear that the burden of responsibility for care was dominated by women. This is consistent with the gender role segregation within the study population, which makes women active in domestic labour and child care with men occupied in dealing with the external world. However, although it was obvious that women took a leading role of carers, it would be interesting to understand whether they are the primary decision makers on where help is sought. In a study in Primary Health Care setting in Mombasa Kenya, fathers were found to be the ultimate decision makers in relation to where help is sought (Abubakar et al., 2013).
Study limitation
The study only used FGDs as a method of data collection. There is need for triangulated methods in future studies. However, the probing during discussions increased face validity of both the data and conclusions. The study only sampled a rural-based population; it would be significant to conduct the same study with an urban-based population. In the study, the majority of the participants had a primary school education and although there has been a positive correlation between low education and traditional healers’ consultation (Razali & Najib, 2000), this is not known among the ‘educated’ in Malawi.
Conclusion
In this study, it has been found that help-seeking is influenced by the understanding of the source of the illness – which has a bio-psychosocial inclination. The socio-cultural explanation of witchcraft and spirit possession is dominant and a determinant of help-seeking behaviour to traditional healers for both diagnosis and treatment. While participants noted benefits to hospital treatment, barriers and bio-psychosocial in nature were also noted. Guardians and not clients hold the key to choice of treatment modality and therefore a potential ally in all treatment interventions promotive, preventive and curative.
Recommendation
Besides clients, there is a need for improvement of mental health services at a community level aimed at family, the primary health care workers and the traditional healers. An approach where mainstream health care systems and contemporary healing systems complement each other may be the most efficient and cost-effective way to meet the huge need for mental health care. While others have advocated integration or collaboration of the two systems, we propose education for all stakeholders for both referral and appropriate decision making. More research is needed about the relationship between traditional healing and mental health in Malawi.
Footnotes
Acknowledgements
The authors acknowledge the contribution of the following: The Saint John of God Research Grant Scheme in Stillorgan, Dublin, Ireland. The Director and management of Saint John of God Mzuzu, Ireen Mithi and Manson Msiska for helping with data collection and transcription and the clients and caregivers who are the owners of these results.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.