
Abstract
Background:
Mental disorders have been associated worldwide with human rights’ violations. Controversially, many occur in mental health facilities.
Aim:
This work aimed to assess the rights of people with mental disorders in healthcare facilities in Tunisia.
Methods:
A cross-sectional study, using the World Health Organization (WHO) quality-rights toolkit, assessed the human rights levels of achievement in Elrazi Hospital, the only psychiatric hospital in Tunisia, in comparison with the National Institute of Nutrition (NIN). The framework was the Convention on the Rights of Persons with Disabilities (CRPD). The assessment was carried through observation, documentation review, and interviews with service users, staff, and family members. The sample was composed of 113 interviewees.
Results:
In Elrazi Hospital, three out of the five evaluated rights were assessed as only initiated: the right to an adequate standard of living, to exercise legal capacity and to be free from inhuman treatment. By comparison, these rights were partially achieved in the NIN. The right to enjoyment of the highest attainable standard of health was partially achieved and the right to live independently and to be included in the community was not even initiated. These last two rights were at the same level of achievement in the NIN.
Conclusion:
Significant improvements are needed to adapt the practice in Elrazi Hospital to comply with human rights, especially since the achievement level of these rights is lower than in a non-psychiatric hospital. Our study emphasizes the importance of spreading the CRPD as a standardized framework.
Research in context
The close relationship between health and human rights is now well established. Human rights violations do affect health, and one’s health status may also affect his or her enjoyment of his or her rights.
Mental health appears to be one of the health components that affect human rights the most. In the writings of Locke, Kant and Mill, considered as sources of liberalism and of the modern concept of rights, those suffering from mental disorders were excluded from people qualifying for rights without justifications, and throughout the human history, they have experienced atrocious violations of their rights.
Therefore, the promotion and protection of the human rights of people with mental disorders ought to be in the core agenda of global mental health, and one of the two principles for the services scale-up priority. Thus, increasing attention is being given to the fulfillment of human rights in mental healthcare facilities. An assessment toolkit was developed by the World Health Organization with the Convention on the Rights of Persons with Disabilities (CRPD) as a framework, within a bigger project: the Quality Rights project aiming to improve the quality and human rights conditions in inpatient and outpatient mental health and social care facilities worldwide.
This close established relationship between mental health and human rights, and the growing recognition that international human rights law imposes duties on all social actors and not just states, are bringing new responsibilities to physicians to bring human rights into healthcare through their practice and advocacy as they are, with the service users, the direct witnesses of the abuses and violations. It also brings new opportunities to enhance the value and the effects of mental health work, as bringing a human rights perspective positions mental health in the scope of the struggle for human dignity, as a collective, multi-dimensional responsibility of a wide range of social and political stakeholders.
Adding a human rights perspective to mental health starts with the evaluation of the current situation. Such an evaluation has not been performed yet in Tunisia. Hence, this work aims at assessing the rights of people with mental disorders in healthcare facilities.
A comprehensive inventory of the realities is a necessary first step toward identifying the problems in existing healthcare practices. This step can help the different stakeholders plan effective actions to ensure that the services are of a good quality and respectful of human rights. No actions can be planned before the concrete problems are identified.
This assessment of rights, underlying human rights violations in our health facilities, can also be used by civil society actors and human rights defenders as the basis of advocacy actions, to ensure a better achievement of the rights, standards and criteria framed in the CRPD that Tunisia signed and ratified.
Introduction
Mental disorders were, and are still, associated worldwide with human rights’ violations (Drew et al., 2011). Controversially, psychiatric institutions and mental health services are among the environments in which these violations are most likely to take place (Drew et al., 2011; Funk & Drew, 2012; Kleinman, 2009).
The international framework of human rights of people with mental disorders is the Convention on Rights of Persons with Disabilities: CRPD (United Nations, 2006). Tunisia signed the CRPD in 2007 and ratified it in 2008 (United Nations Treaty Collection, 2017). However, the Tunisian mental health law was last updated in 2004 (République Tunisienne, 2004). The same applies to the disability law that was stipulated in 2005 and was not modified afterward. This may suggest that the CRPD standards are yet to be translated into national laws.
This work aimed to check the realities and assess the respect of the rights of people with mental disorders in mental healthcare facilities of a University Psychiatric Hospital in Tunisia and also to introduce the practice of assessing the respect of the rights of people with mental disorders in mental healthcare facilities.
Methods
Study design and instrumentation
This is a descriptive and analytical cross-sectional study. The only university psychiatric hospital in Tunisia, Elrazi Hospital (World Health Organization and Ministry of Health, 2008), was compared to a non-psychiatric hospital in the same city (Tunis), in order to determine the accountability of ‘mental illness’ in the human rights’ quality in healthcare facilities.
The assessment of the rights of persons with mental disorders had the CRPD as framework and was conducted according to the criteria elaborated by the World Health Organization in its Quality Rights toolkit to assess and improve quality and human rights in mental health facilities (Funk & Drew, 2012).
The toolkit covers five themes: the right to an adequate standard of living and social protection (Article 28 of the CRPD); the right to enjoyment of the highest attainable standard of physical and mental health (Article 25); the right to exercise legal capacity and the right to personal liberty and the security of person (Articles 12, 14); freedom from torture or cruel, inhuman or degrading treatment or punishment and from exploitation, violence and abuse (Articles 15,16); and the right to live independently and be included in the community (Article 19).
Each of the themes outlined above was broken down into standards, which were further broken down into criteria. The criteria form the basis of the rights assessment. Assessment of corresponding criteria determined whether a particular standard was met. The standards, in turn, helped to determine whether the overarching theme was met (Figure 1).
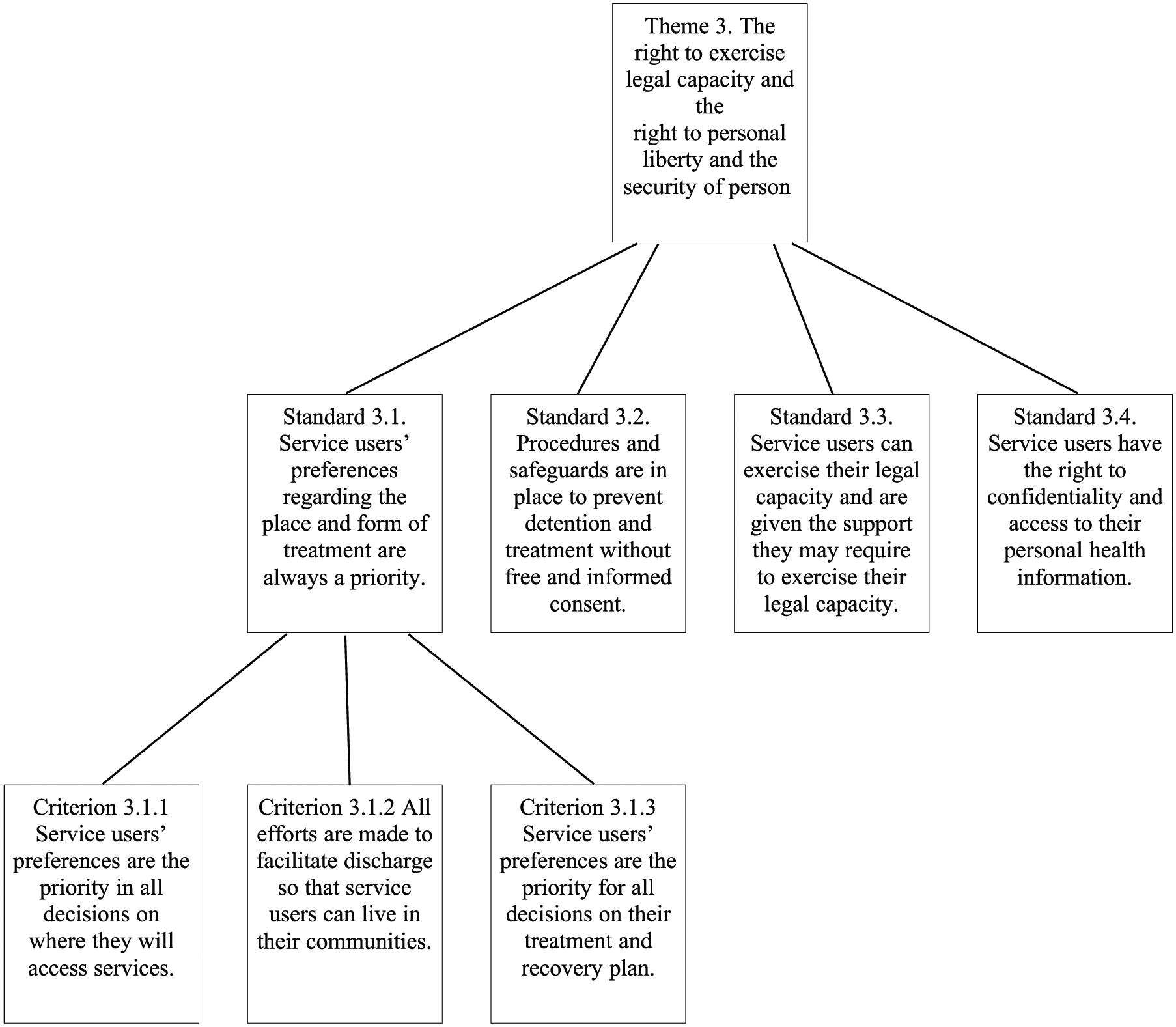
Example of division of the themes into standards and criteria (Theme 3. The right to exercise legal capacity and the right to personal liberty and the security of person).
The assessment had a four-level scoring scale: fully achieved, partially achieved, achievement initiated and not initiated. It was conducted, as recommended by the toolkit (Funk & Drew, 2012), through interviews of service users, caregivers and staff members, observation of the facility, and the documentation review.
Population and sampling
The assessment was conducted in Elrazi Hospital, Tunis, Tunisia, including the seven inpatient adult psychiatry units. The forensic psychiatry and the child psychiatry units were not included in this study as both had their specific legislation and organization.
The population was composed of service users of Elrazi Hospital, their family members and the staff. A control study was conducted in a non-mental health university hospital: the endocrinology department in the National Institute of Nutrition and Food Technology (NIN), assessing the rights of people with diabetes (types 1 and 2). The choice of the control group was based on the location (same city as Elrazi Hospital, Tunis), on their status of specialized University Hospitals and on the chronicity of both illnesses.
The control population was composed of patients with diabetes, hospitalized in this department, their family members and the staff. A stratified random sampling was used and followed the recommendations of the toolkit (Funk & Drew, 2012). A total of 113 interviews were conducted, distributed as the following – in Elrazi: 35 service users, 18 family members and 35 staff members; and in the endocrinology department, interviews were conducted with 10 service users, 10 staff and five family members.
Procedure and time frame
The assessment was conducted during the period between March 2014 and February 2015. The Ministry of Health, the hospital administration and the heads of the departments were informed about the study without previous announcement of the visits dates. Visits were carried out at the rate of one to three per week according to the availability of the team members, at different times of the day.
The team was composed of two evaluators (the first and the second authors (M.R and A.B.H), who shared the assessment in the different units, conducting the interviews and observing the facilities. The documentation review was performed by M.R. The two evaluators practiced together how to use the toolkit: the interview and the observation guidelines, and the Clinical Global Impression scale, coached by the supervisor (last author). They also conducted four pilot interviews before the beginning of the study.
A minimum Clinical Global Impression score of 4 was one of the inclusion criteria for the service users, along with a 5-day minimum duration of hospitalization, and a diagnosis of a chronic psychiatric disorder.
Ethical considerations
All interviewed participants were asked for their consent before the interview. They had the right to ask questions and to decline to be interviewed, before, or at any time during the interview. They also had the right to refuse answering some questions.
All interviews were conducted in closed spaces, which ensured privacy. The interviews were conducted with the exclusive presence of the interviewer and the interviewee. Neither staff member nor other persons were allowed to be present.
Signed consent forms were kept in a safe place by the interviewer, separately from the anonymous interview forms. The study was approved by the ethical committee and the permissions to collect the data were received from the administration of Elrazi Hospital and from the head of the endocrinology department in the NIN.
Statistical analysis
The assessment scores were determined from the combination of the interviews findings, the observation and the documentation review. The team (composed of the evaluators and the supervisor) decided on a score for each criterion, combining the mean of the interviews’ answers, the observation of the facilities and the documentation review, based on the levels of achievement. In the majority of items, the scores from the interviews (the rounded means) were concordant with the scores from the observation and documentation review, and when it was not the case, the lower score was considered.
The rights’ achievements in both facilities were compared qualitatively based on all findings and quantitatively based exclusively on the interviews results, using the chi-square test for the criteria and the Mann–Whitney test for the themes. All statistics had 95% confidence intervals.
Results
Rights assessment in the mental health facility
The achievement of the right to an adequate standard of living in Elrazi was initiated, with six standards and only one partially achieved (standard 1.4: service users are given food, safe drinking-water and clothing that meet their needs).
The right to health was partially achieved. Two standards scored below this average as they were only initiated (standards 2.2 and 2.3, respectively, related to skilled staff and good-quality health services and to treatment, psychosocial rehabilitation and links to support networks).
The right to exercise legal capacity, to personal liberty and to security was initiated. One standard was partially achieved (standard 3.4 related to the right to confidentiality and access to their personal health information), while two standards were initiated (standards 3.1 related to the respect of service users’ preferences regarding the place and form of treatment and 3.3 related to the exercise of legal capacity). The standard 3.2 related to safeguards and procedures preventing detention and treatment without free and informed consent was not even initiated.
The freedom from torture or degrading treatment was also initiated: standards 4.3 and 4.4 related to the non-abuse of electroconvulsive therapy and to the scientific experimentation were partially achieved. Standards 4.1 and 4.5 related to the right to be free from abuse and neglect were initiated, while the standard 4.2 related to the use of alternative methods in place of seclusion and restraint was not even initiated.
The achievement of the right to live independently and to be included in the community was not initiated as none of its standards was (Table 1).
Assessment of the themes according to the different standards in the mental health facility.

A/F: fully achieved; A/P: achieved partially; A/I: achievement initiated; N/I: not initiated.
Rights assessment in the mental health and the general health facilities.
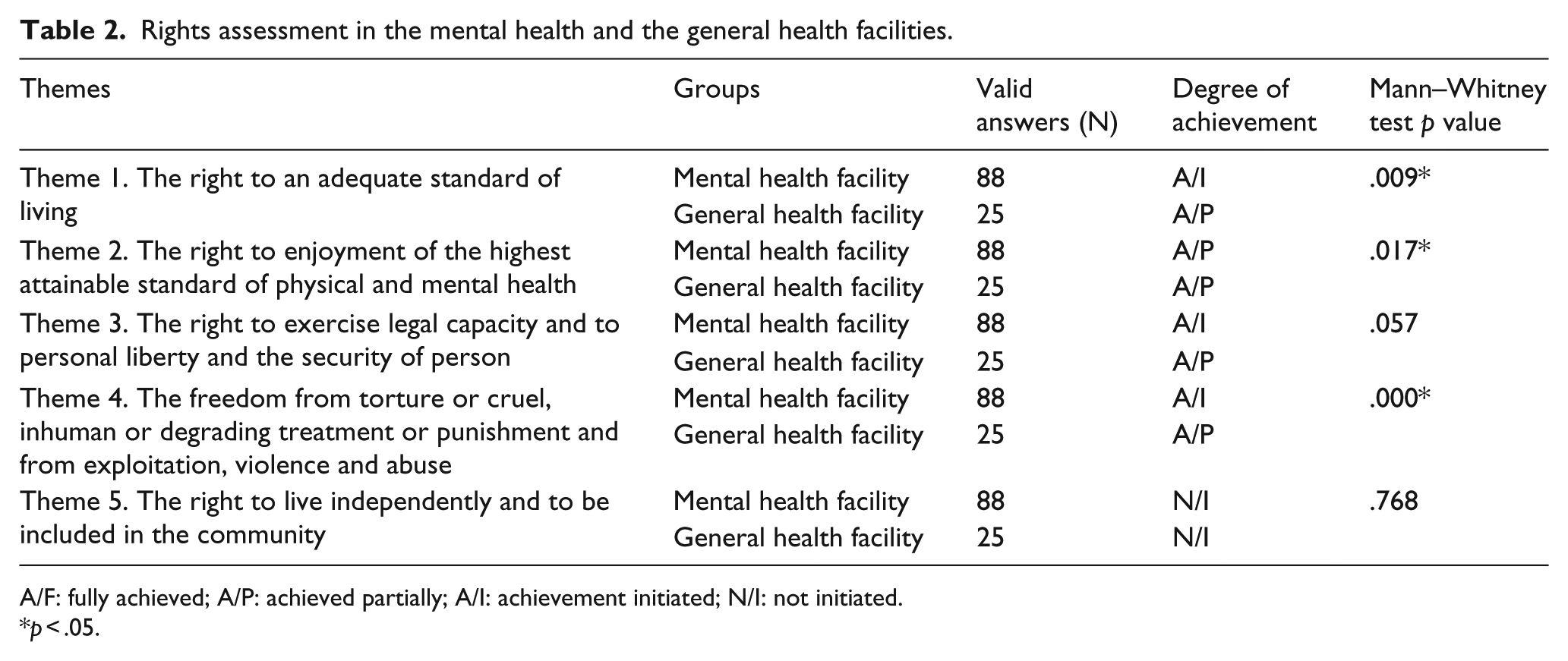
A/F: fully achieved; A/P: achieved partially; A/I: achievement initiated; N/I: not initiated.
p < .05.
Comparison to the non-mental health facility
In the NIN, four rights were partially achieved. Only the right to live independently and to be included in the community was not initiated. It was also the one, with the right to health that was assessed at the same level of achievement in the two facilities, while the other three rights scored lower in Elrazi (Table 1).
Significant differences were found in the scores collected through interviews between the two facilities, with better achievement in NIN, in three themes: the right to an adequate standard of living, the right to health, and the freedom from torture or degrading treatment (Table 1).
Discussion
In Elrazi Hospital, three out of the five evaluated rights were assessed as only initiated: the right to an adequate standard of living, to exercise legal capacity and to be free from inhuman treatment. The right to enjoyment of the highest attainable standard of health was partially achieved and the right to live independently and to be included in the community was not even initiated. These last two rights were at the same level of achievement in the NIN, while the first three ones were lower scored than the NIN.
Rights assessment in the mental health facility
In Elrazi, the assessment showed difficult living conditions, poor hygiene, and lack of decent bedding and privacy. Service users were wearing uniforms, denied personal possessions, individual space, as well as the smallest choices like the time to wake up, to eat or to sleep, in a typical picture of institutional personhood removal (Bakalović & Lee, 2011). The social environment was as difficult: service users were denied the opportunity to communicate with the outside world, except the few who were receiving visits from families. They were experiencing excruciating boredom, with neither intellectual nor physical stimulation; the most common daily activity was wandering between corridors. Furthermore, if impoverished living conditions in mental hospitals were since decades associated with anti-therapeutic effects (Goffman, 1961), conditions in Elrazi were even suspected to be among the factors of premature excess mortality among young service users (Zgueb et al., 2014).
The right to health was the most highly scored; evidence that it is the priority for which most efforts are deployed, although some failures were noticed and improvement is needed. There is a lack of mental health human resources, considered as one of the limitations to the services scaling-up in low- and middle-income countries (Saxena, Thornicroft, Knapp, & Whiteford, 2007). Thus, there is no regularly provided psychosocial rehabilitation, which is also related to a lack of training on global mental health skills, also common in these countries (Eaton et al., 2011). Another limit to high-quality mental health services was the absence of the recommended recovery orientation (Funk & Drew, 2012) and the predominance of the medical-based model. This predominance can also be seen through the use of medication: majority of the patients were on antipsychotic poly-pharmacy and/or high doses of antipsychotic not following the international recommendations (Gardner, Murphy, O’Donnell, Centorrino, & Baldessarini, 2010; Humber NHS Foundation Trust, 2012; Royal College of Psychiatrists, 2014; Vital Durand & Le Jeunne, 2013), with the patients neither informed of the side effects of these medications nor asked for their consent.
While tackling the right to exercise legal capacities, it was clear that even if the legal admission procedures were respected, involuntary admissions were the most frequent, and even increasing (Rafrafi et al., 2013). Involuntary admissions are regulated in detail by the Tunisian mental health law (République Tunisienne, 1992, 2004). But if the existence of this legal framework is an asset, having it limited to persons with mental disorders is in contradiction with the non-discrimination principle as this was mentioned in the recommendations made to Tunisia by the CRPD Committee (Committee on the Rights of Persons with Disabilities, 2011). According to the CRPD, any criteria for involuntary admission must be non-discriminatory and disability neutral (Szmukler, Daw, & Callard, 2014), examples to be followed can be the new ‘Fusion laws’, combining mental health and incapability laws (Dawson & Szmukler, 2006). Moreover, the supported-decision making model is still an unusual practice in Elrazi, and the need was expressed that health professionals should take the lead introducing it and engaging their patients in the decisions concerning them (Duncan, Best, & Hagen, 2010).
The limitations of the freedom from torture or degrading treatment were probably not surprising, as ill-treatment and neglect are common in mental healthcare facilities throughout the world (Drew et al., 2011; Gostin, 2008). In Elrazi, there was evidence that service users were undergoing abuse and neglect since slaps, humiliating words and punishments seemed to be part of their daily routine and 20 out of 35 service users reported being subject of such maltreatment. One patient, hospitalized for a bipolar disorder described the way they were treated by the staff by saying, ‘We are not treated like humans, barely like animals and no one is caring about us more than giving us the pills and the meals’. This may let us question the sense of healthcare as it overlaps here with ill-treatment if not with torture (Office of the High Commissioner for Human Rights, 2004).
Another common practice in Elrazi that falls under the definition of ill-treatment was the large use of restraint. It was even considered as a regular and acceptable ‘therapeutic’ option to address acute agitation and was practiced against the recommendations (United Nations, 1991). This may be explained by the lack of resources, which is already known to be a main factor (Freeman, Pathare, Drew, & Funk, 2005), but it is equally related to the lack of knowledge and training about alternatives (Champagne & Stromberg, 2004; Donat, 2005; Gagnon, Desmartis, Dipankui, Gagnon, & St-Pierre, 2013; Kontio et al., 2012).
The right to live independently in the community was absent from the facility mission, and there were no services aiming to provide, support or facilitate the access of persons with mental disorders to the full range of support needed for autonomy and inclusion. Housing support was almost absent, and many patients were ‘living’ in the hospital because of homelessness, which is similar to the situation in other countries (Hillman, 2007; Hillman et al., 2004). One of the main reasons to homelessness was unemployment, with high rates among persons with mental disorders documented in the literature, due mainly to the prejudice that mental disorders impede the work capacity even though there is evidence that enabling people to retain or gain employment has a positive effect on more life domains than almost any other medical or social intervention (Boardmann, Grove, Perkins, & Shepherd, 2003; Marwaha & Johnson, 2004).
The healthcare facility seemed completely isolated from the community, which impoverished the care quality and limited the scaling-up possibilities (Selamu et al., 2015). This isolation was contributing to the exclusion of people with mental disorders, who are already considered as among the most marginalized in societies (Mathias, Kermode, San Sebastian, Koschorke, & Goicolea, 2015), this exclusion limited the access to care, leading to a vicious circle (Sartorius, 2007).
The same assessment was carried in the psychiatric clinic of the Serres general hospital in Greece where it was very similar to Elrazi’s with three rights out of five at the same achievement level (Nomidou, 2012), while the assessment carried in the seven mental health hospitalization units in the principality of Asturias in Spain revealed better scores (Marco Moreno, Gonzalez Quintana, Lama Carter, & Fernández Chur, 2012). However, compared to the situation of the Hargeisa group hospital in Somalia where none of the rights was initiated (Curie, 2012), there was evidence of steps taken in Tunisia toward fulfilling the rights of people with mental disorders despite deficiencies.
Comparison to the non-mental health facility
The comparison with other countries seems to be well described as an image where ‘the details may differ, but the situation of neglect and abuse is not so different’ (Kleinman, 2009). In fact, comparison between mental health and general health facilities in the same country may be more useful, as the national context and resources are the same and closing the gap between mental and general health services quality is the least that can be implemented.
The difference in the right to an adequate standard of living between the two facilities may indicate the failure of the de-institutionalization of Elrazi: even though it has been a university hospital since 50 years ago (Ammar, Douki, Taktak, & Ben Zineb, 1998), the conditions remain those of an asylum. This was also reflected by the second right: if no significative difference was found in the overall right, differences were noted in the standards related to overmedication and treatment without consent, as in the mental health facility, treatment seems to be provided for the general order not only for the best interest of the patient.
The right to legal capacity had also lower score in Elrazi because of involuntary admissions and the lack of interaction between the staff and the patients regarding their preferences and decisions. Is it an amalgam between mental illness and incapability? Another spread amalgam, this time with dangerousness and unpredictability (Sartorius, 2007), was reflected through the fourth right: freedom from degrading treatment and torture.
The right to live independently and to be included in the community was initiated in none of the facilities as a consequence of the narrow understanding of healthcare limited to the biomedical model, although it is important to underline that the lack of support for autonomy provided by the health facilities has different consequences on the two populations, thus the right is unequally enjoyed, as people with mental disorders are much more vulnerable to exclusion and marginalization (Funk et al., 2010; Mathias et al., 2015).
Limitations
Study setting
The assessing team was only composed of health professionals, and this was because of resource constraints, which limited the possibility to recruit service users or family members to join them. In fact, the study would have benefited from a more participatory approach. Though, a special attention was given so none of the investigators assessed a department where they were working or interviewed service users who were also their patients, in order to limit the biases.
Rights’ assessment
Two major limits faced the rights’ assessment in this study; the first was inherent to the combination of quantitative and qualitative methods in the assessment, so that the interviews, observation and documentation review findings were combined in order to produce scores. In fact, the translation of the findings in scores limited the possibility of reflecting all the diversity and specificities of the different answers. Moreover, even if the scoring was made after discussions among the team, and based on specific criteria developed in the WHO toolkit under each standard and right, subjectivity cannot be completely neutralized. The second limit is the fact that the seven departments were assessed together and the findings were averaged which may dilute them: even if no significant differences were found while comparing the five themes achievement between the seven departments, separate assessments of the departments may still have been more valuable in providing more precise findings, but would have probably needed larger samples.
Awareness raising
One of the initial objectives of this study was to raise awareness about the rights of people with mental disorders, but only a small sample was concerned and no tool was developed to assess the awareness after the interviews even if some spontaneous impressions were collected.
Mental illness, disability and the CRPD
This assessment of the rights of persons with mental disorders was conducted according to the international framework of standards defined by the CRPD, as it is accepted by the Committee on the Rights of Persons with Disabilities that people with a ‘mental illness’ (referred to as having a ‘psychosocial disability’) fall under the Convention. But whether all people with a ‘mental illness’ are appropriately considered as having a ‘disability’ is a rough question that raises larger philosophical and sociological issues.
Conclusion
Even though the complete fulfillment of the rights of people with mental disorders depends on different factors and protagonists, many of these rights can be influenced by health professionals. Thus, the role of mental health professionals includes assessing, respecting, protecting Human Rights and advocating for them. The CRPD, mainly if ratified by the country, can be the legal framework offering the standards to implement and the objectives to reach so that people with mental disorders enjoy their well-being.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.