
Abstract
Background:
Community-based day centres (CBDCs) for people with mental illness are a common service for both people with an immigrant background and native Swedes.
Aim:
The aim was to compare CBDC attendees with an immigrant background with attendees who were native Swedes in terms of well-being and perceptions of everyday activities and investigate whether ethnic background could predict these factors.
Methods:
Attendees at nine CBDCs were invited to participate. In all, 56 with an immigrant background and 69 native Swedes completed self-report questionnaires that addressed various aspects of well-being and everyday activities.
Results:
Attendees with an immigrant background had a worse situation regarding perceived self-esteem, empowerment and satisfaction with everyday activities. In multivariate logistic regression analyses, ethnic background only became a significant predictor in regard to empowerment. Quality of life and activity level were of importance for satisfaction with everyday activities. Empowerment and self-esteem mutually influenced each other.
Conclusion:
Having a mental illness and an immigrant background may infer a particular risk for low empowerment. The mental health services and society at large should consider measures for adjusting the support to this group, including an analysis of how environments and contexts may act as barriers to activity enrichment and culturally congruent support.
Introduction
Engagement in everyday activities is a basic human need that is of paramount importance for health and well-being (Wilcock, 2006). It promotes personal growth and provides the individual with important feedback about the self as unique and competent (Hammell, 2004; Pooremamali, Ostman, Persson, & Eklund, 2011; Pooremamali, Persson, Östman, & Eklund, 2015). Research has found that both what people with mental illness actually do, such as time spent in various activities and the number of activities performed, and how they feel about what they do, in terms of satisfying and valued activities, are important for well-being (Eklund & Leufstadius, 2007). People experience activity well-being when they are capable of performing activities they need or desire to in an environment that allows such activities (Wilcock, 2006).
The existence of a clear link between satisfying everyday activities and well-being has been acknowledged in the planning of mental health services. In many countries, the authorities organize meaningful everyday activities for those who have a persistent mental illness (PMI) and are unemployed (Bryant, Vacher, Beresford, & McKay, 2010; Rebeiro, Day, Semeniuk, O’Brien, & Wilson, 2001; Tjörnstrand, Bejerholm, & Eklund, 2011). In Sweden, the local authorities are obliged to provide meaningful activities for people with PMI (Ministry of Health and Social Affairs, 1992), and guidelines highlight community-based day centres (CBDCs) as recommended services (National Board of Health and Welfare, 2011). People with PMI generally lack employment (Nordstrom, Skarsater, Björkman, & Wijk, 2009), and in recent years CBDCs also offer opportunities for work-oriented rehabilitation in accordance with the principles of supported employment (Bejerholm, Areberg, Hofgren, Sandlund, & Rinaldi, 2015; Bond, Drake, & Becker, 2012). Sweden is becoming an increasingly multicultural country, which is also reflected in CBDCs for people with PMI (Pooremamali et al., 2015). Research in this context shows that migration, ethnicity, mental illness, economic strain, social exclusion and communication barriers generate conditions that cause activity deprivation and have a negative influence on health, well-being and activity satisfaction and performance (Bhugra, 2004; Pooremamali, Morville, & Eklund, 2017).
A major issue in the study of occupation and well-being is whether individuals from different cultures have different conceptions of well-being, and researchers have maintained that this is the case (Diener, 2009; Suh, Diener, & Updegraff, 2008). Western individualistic cultures that emphasize individual experiences constantly direct the attention of their members to their internal psychological reaction. On the other hand, in eastern cultures where much of everyday life involves others, individuals constantly have external social indicators in focus. As a result, the view of well-being appears to differ between these two types of cultures (Suh, Diener, Oishi, & Triandis, 1998). Well-being, in the individualistic perspective, is interpreted as a realization of human potential, which is inconsistent with cultures that assume people’s well-being is dependent on their adjustment to the values and norms of their culture (Chirkov, 2009). A study among Middle Eastern immigrants with mental illness demonstrated how leading a life between two cultures increased frustration, which in turn negatively influenced their activity well-being (Pooremamali, Eklund, Ostman, & Persson, 2012).
Few studies have focused on how culture affects activity well-being (Hocking, 2009) and, to our knowledge, no study has compared well-being and perceptions of everyday activities between immigrants and native people with mental illness in Sweden. Previous research has, however, addressed well-being and activity factors separately among people with an immigrant background (Pooremamali et al., 2015) and in samples that mainly consisted of native Swedes (Argentzell, Leufstadius, & Eklund, 2012; Leufstadius, Gunnarsson, & Eklund, 2014). Since CBDCs are the mainstream alternative for meaningful daily activities for people with PMI in Sweden, a comparative study addressing people with an immigrant background and native Swedes in that context could yield important knowledge about issues of concern for the provision of better support for people with mental illness and an immigrant background.
Aims
The main aim was to compare CBDC attendees who have an immigrant background with native Swedes regarding well-being and perceptions of everyday activities. A related aim was to investigate whether ethnic background could predict well-being and perceptions of everyday activities in the sample as a whole, when also taking socio-demographic and clinical factors into account.
Methods
This study employed the principles of voluntariness and informed consent and followed the ethical guidelines stipulated in the Helsinki Declaration of 1975, as revised in 1983. It was approved by the Regional Ethical Review Board at Lund University, Reg. no. 2012/70.
The study was based on two samples, both of which consisted of people attending day centres for people with psychiatric disabilities. All day centres were located in larger cities in Sweden. The first sample was followed during implementation of a free-choice reform aimed at offering more variation and opportunities for choice of day centres and what to do there (Andersson, Eklund, Sandlund, & Markström, 2015). The participants came from four strategically chosen city districts, representing a variation in socio-economic situation and proximity to the city centre. These districts included six day centres, all of which agreed to participate. Only baseline data were used for this study. Native Swedes were in majority, and since we strove for a larger subsample with an immigrant background, a further three day centres in another major city in Sweden were included by purposeful sampling.
The study context
Day centres in Sweden are of two main types – work-oriented and meeting place-oriented (Tjörnstrand et al., 2011). The work-oriented centres offer scheduled work, and the manufacture of goods for sale and subcontract work for local companies are common activities. Services such as food catering or car washing are also common. Meeting place-oriented day centres constitute a more flexible alternative and the attendees can participate on a drop-in basis, although some may prefer to keep to a schedule. Various types of hobbies, games, eating together and socializing are typical activities.
Participants
The inclusion criteria were having a psychiatric disability and attending the day centre for 4 hours per week or more. Swedish authorities define a psychiatric disability as an enduring mental health condition (thus PMI) that prevents the person from coping with everyday life (Swedish Government Official Reports, 2006). This condition constitutes the basic criterion for being admitted to a day centre, which means that all attendees by definition fulfilled this criterion. The researchers held an information meeting at each day centre and the attendees were invited to participate. Those who wished could give their written informed consent immediately after the meeting. They could otherwise consider participation for a few weeks and hand in their written consent through the staff. The exclusion criteria were as follows: comorbidity of dementia, intellectual disability or other condition causing cognitive impairment, having substance use disorder as the main diagnosis and acute psychiatric relapse. The attendee’s primary contact among the day centre staff assessed these criteria. The data collection could be made in Swedish or Farsi, and no interpreters were used. Insufficient command of Swedish or Farsi was thus another exclusion criterion.
Immigrant background was in this study defined as being born outside of Sweden and/or having at least one parent born in another country. In two cases, there were participants who were born in a foreign country but had Swedish-born parents and had moved to Sweden as children. These were regarded as native Swedes. In all, 139 participants were recruited for the study, but data regarding ethnic background were missing for 16 individuals. The study was thus based on 125 participants, 56 of whom had an immigrant background and 69 were native Swedes. Those who had an immigrant background had been living in Sweden for between 11 and 45 years (M = 27, standard deviation (SD) = 9). In all, 15 of them were born in Sweden, but had parents born in another country. Those 56 who had an immigrant background originated from 29 different countries distributed on the Middle East (n = 19), a Nordic country (n = 14), another European country (n = 10), South America (n = 6), Africa (n = 4) and other parts of the world (n = 3).
The drop-in character of some of the day centres made it difficult to calculate the participation rate. Although no exact information was available, the participation rate was estimated to be around 50% in both samples, which is a similar rate to that found in other studies where the data collection has not been part of the regular services (Bengtsson-Tops, 2004; Eklund, Hansson, & Ahlqvist, 2004).
Data collection
The data collection took place in a private and quiet room at the day centre to ensure a relaxed atmosphere. As specified below, seven instruments were administered, each consisting of 1–12 items, and the research team was well aware of risk of exhaustion among the study participants. Therefore, breaks were inserted when needed and coffee/tea and snacks were available. Some participants completed the data collection without resting, whereas most of them wanted a break. For a few participants, the data collection had to be split on two occasions. The total time for data collection varied between 30 and 90 minutes.
A background questionnaire was used to retrieve socio-demographic data and information about day centre attendance (hours per week) and clinical data (self-reported diagnosis). The latter were later on coded by a specialized psychiatrist according to the International Classification of Diseases, 10th Revision (ICD-10) classification (World Health Organization [WHO], 1993). A previous study indicated that groups, based on the ICD-10 diagnoses generated by the coding system used here, differed logically on positive, negative and depressive symptoms (Eklund & Sandlund, 2012). The research assistant’s global assessment of the attendee’s level of functioning (Endicott, Spitzer, Fleiss, & Cohen, 1976) was also included in the background questionnaires. Further instruments are specified below.
Well-being
Four aspects of well-being were addressed in this study: self-rated health, quality of life, self-esteem and empowerment.
Self-rated health was assessed using the first item from the Medical Outcomes Study 36-item Short-Form Health Survey (SF-36; Ware & Sherbourne, 1992). The response format is a scale from 1 to 5, and a lower number indicates better health. This one-item rating of health is regarded as a reliable assessment because of a high correlation with the full scale (Bowling, 2005).
Quality of life was addressed using the 12-item Manchester Short Assessment of Quality of Life (MANSA; Priebe, Huxley, Knight, & Evans, 1999). The first item asks about the person’s present general quality of life. The remaining 11 items concern the respondent’s current satisfaction with a variety of life areas, such as work, housing, personal finances, personal safety, partner situation and physical and psychological health. The rating of these items is summarized into a composite measure of satisfaction with life domains. The response scale ranges from 1 to 7, where a high number equals better quality of life. The Swedish version used has been found to have satisfactory internal consistency and construct validity (Björkman & Svensson, 2005).
Self-esteem was estimated by the 10-item Rosenberg self-esteem scale (Rosenberg, 1965). A version with a yes/no response format was used (Oliver, Huxley, Priebe, & Kaiser, 1997). The instrument consists of five questions addressing positive and five addressing negative aspects of experienced self-esteem. The final score may range from −1 to 1, where a higher rating signifies a higher level of self-esteem. The instrument has shown good psychometric properties in terms of good internal consistency and test–retest reliability (Torrey, Mueser, McHugo, & Drake, 2000).
Perceived empowerment was assessed by the 28-item Empowerment scale, which has shown good reliability and validity (Rogers, Chamberlin, Ellison, & Crean, 1997; Rogers, Ralph, & Salzer, 2010). It uses a 4-point scale ranging from strongly agree (=1) to strongly disagree (=4). A higher rating designates stronger empowerment and the total score may range between 28 and 112. Five subscales may be discerned: self-esteem/self-efficacy, power/powerlessness, community activism and autonomy, optimism and control, and righteous anger. The subscales were used for descriptive purposes in this study, but further multivariate analyses concentrated on the overall score. The Swedish version of the Empowerment scale has shown good internal consistency and construct validity (Hansson & Björkman, 2005).
Everyday activities
The attendees’ perceptions of everyday activities were assessed by means of three self-report questionnaires and one interview-based instrument.
Engagement in the day centre activities was addressed using the self-assessed Profiles of Occupational Engagement in people with Severe mental Illness – Productive occupations (POES-P; Tjörnstrand, Bejerholm, & Eklund, 2013). The POES-P has two parts, a diary sheet and a checklist, by which an individual’s productive, work-related engagement is addressed. It was only the checklist, which consists of eight items, that was used for this study. Examples of questions are as follows: ‘I think what I do is meaningful to me’ and ‘I think I take the initiative for doing what I do’. A 5-point response scale is used, ranging from not at all (=1) to always (=5). A higher score indicates greater activity engagement. The checklist has shown good internal consistency and construct validity (Tjörnstrand et al., 2013).
Motivation for going to a day centre was assessed by a set of four questions that concern (1) participation in activities in the day centre, (2) occurrence of personal goals for what to do in the day centre, (3) any current preference for being on one’s own and (4) any current preference for having employment (Eklund & Tjörnstrand, 2013). The items reflected different facets of motivation and are not intended to form a scale. The response format is a visual analogue scale (VAS) ranging from 0 to 100. Initial content and discriminant validity have been demonstrated (Eklund & Tjörnstrand, 2013).
Satisfaction with the day centre services was assessed with an eight-item satisfaction questionnaire, inspired by Larsen, Attkisson, Hargreaves, and Nguyen (1979) but rephrased to suit a rehabilitation context. Examples of the items are ‘Did you get the support you wanted?’ and ‘Would you recommend the day centre to a friend in need of support’? The response format is a 4-point scale ranging from very dissatisfied (=1) to very satisfied (=4). The questionnaire has shown to have very good internal consistency in a rehabilitation context (Eklund & Erlandsson, 2013).
Satisfaction with everyday activities was measured by the interview-based Satisfaction with Daily Occupations (SDO) scale. The SDO has good psychometric properties in terms of internal consistency, construct validity, test–retest validity and criterion validity among people with mental disorders (Eklund, 2004; Eklund & Gunnarsson, 2007). SDO covers four aspects of daily activities: work, leisure, household chores and self-care. The original version with nine items was used. The interviewer asks whether the respondent currently performs the occupation targeted in the item. The respondent answers yes or no and then rates his or her satisfaction with that situation on a 7-point scale ranging between worst possible satisfaction (=1) and best possible satisfaction (=7).
Data analysis
Differences between attendees with an immigrant background and those who were native Swedes were calculated with the Mann–Whitney U-test for ordinal variables and the chi-square test for categorical data. Non-parametric statistics were regarded as appropriate since the instruments used produced ordinal data.
In order to shed further light on factors of importance for well-being and perceptions of everyday activities, logistic regression analyses based on the forward conditional model were performed. The well-being and activity variables for which group differences were found were selected as dependent variables for the regression analyses, and then dichotomized according to a median cut to create categorical variables. In order to obtain comparable odds ratios (ORs) based on ordinal-scale independent variables, for which the response scales varied considerably, the ordinal data were transformed to z-scores for the regression analyses. Socio-demographic, clinical, well-being and activity factors that were related to the selected dependent variable at p = .10 or below were included as independent variables in the respective regression analyses. The Hosmer and Lemeshow test was used to estimate goodness of fit, and explained variance was expressed according to the Nagelkerke R2.
Decimals are shown only for values smaller than 10 in the descriptive statistics, and p-values smaller than .05 were considered statistically significant. The software used was the IBM SPSS statistics version 22.0.
Results
Socio-demographic and clinical characteristics of the two samples
Information about socio-demographic and clinical factors for those with an immigrant background and native Swedes are shown in Table 1. Those with an immigrant background were younger and were more often married or cohabiting compared to the native Swedes, but fewer in the immigrant group reported having a close friend. There was also a group difference in education level where those with an immigrant background were over-represented both in the group with the lowest education (not finished 9-year compulsory school) and among those with a college or university education. Furthermore, those who had an immigrant background were under-represented in the group that had completed high school. The two samples did not differ on any of the clinical factors, that is, self-reported diagnosis and global functioning assessed by the research assistant.
Socio-demographic and clinical characteristics of the participants.
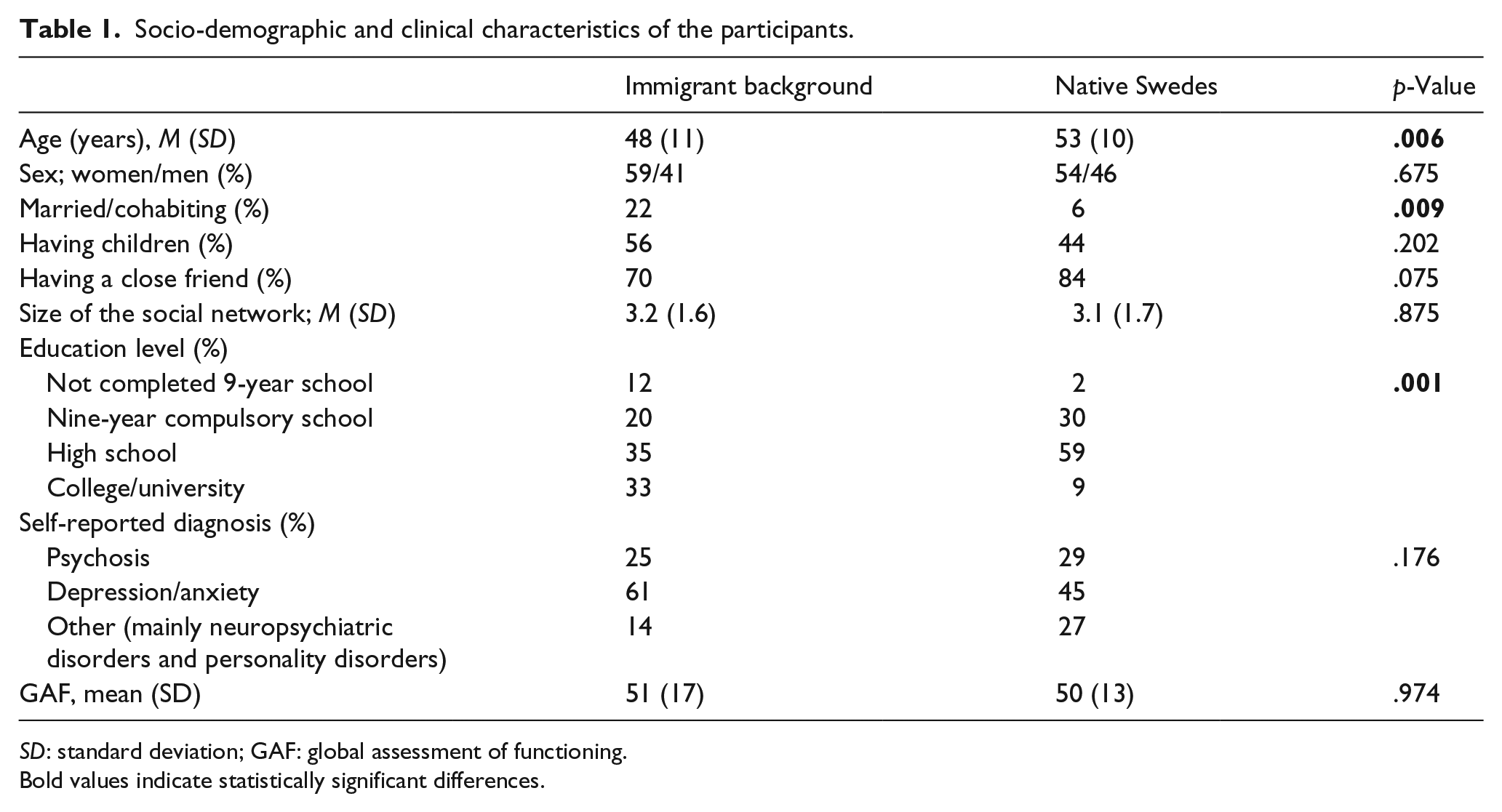
SD: standard deviation; GAF: global assessment of functioning.
Bold values indicate statistically significant differences.
Differences on well-being and activity factors
Participants with an immigrant background and native Swedes differed on several aspects of well-being (Table 2). The immigrant group scored lower on empowerment, including all the subscales, and on self-esteem. No statistically significant differences were found for self-rated health and quality of life.
Well-being and empowerment among immigrant attendees and native Swedes; M (SD).

A lower rating indicates better health.
Bold values indicate statistically significant differences.
Table 3 shows that attendees with an immigrant background were significantly less satisfied with their everyday activities. No other differences on activity factors were identified. Nor were there any group differences with respect to motivation for day centre participation or satisfaction with the day centre services.
Activity factors among immigrant attendees and native Swedes; M (SD).
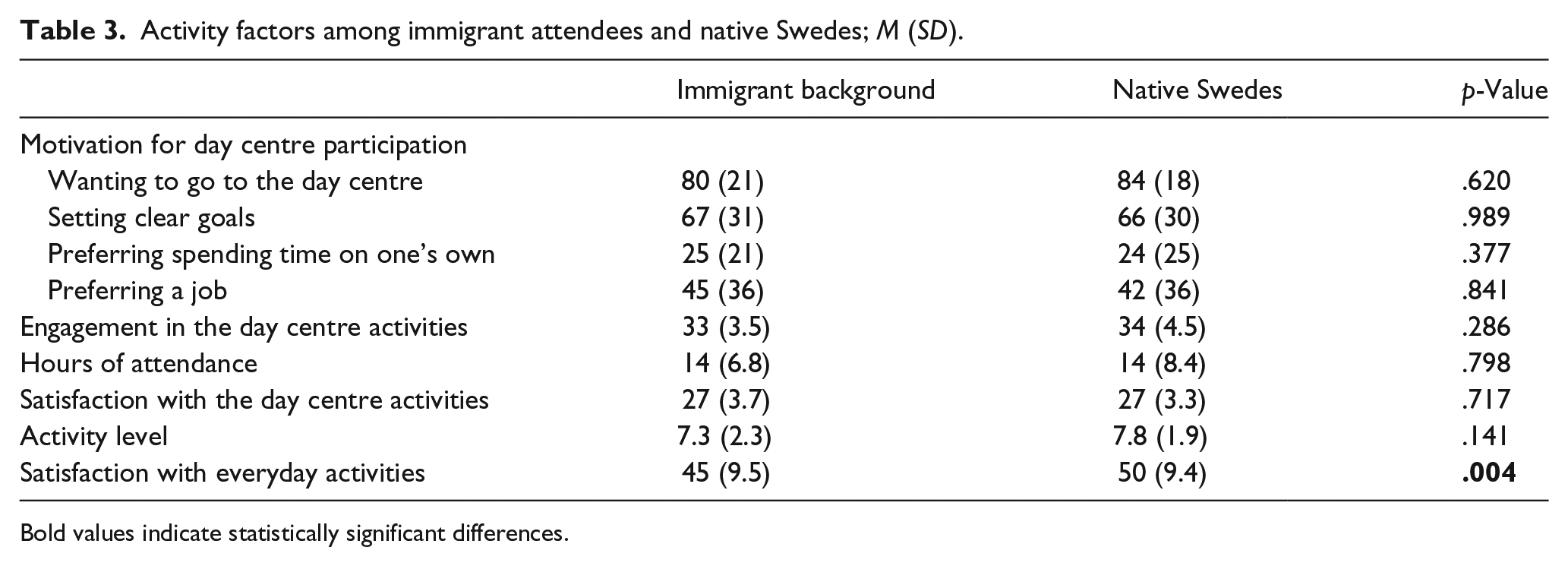
Bold values indicate statistically significant differences.
Predicting well-being and activity factors
Logistic regression analyses were performed with dichotomized self-esteem, overall empowerment and satisfaction with everyday activities as the respective dependent factors. Several independent variables showed associations at p = .10 or lower for each of these dichotomous factors (Table 4).
Associations between independent and dependent factors at p = .10 or lower.

NS: not significant.
Because of the large number of independent variables to be considered, the regression analyses were performed in four sets for each of the three dependent factors. The first concerned socio-demographic and clinical factors, the second well-being and empowerment and the third activity factors. Independent variables that became statistically significant in the respective sets were thereafter entered together in a fourth, final set (Table 5). Regarding self-esteem, Nagelkerke R2 = .52 for the final analysis indicated that empowerment together with quality of life and being married or cohabiting explained 52% of the variance. As indicated by an OR of 3.9, there was a fourfold probability of being in the high group of self-esteem for an increase of one scale step (z-score) on empowerment. An increase of one scale step on quality of life almost tripled the chance of belonging to the high group, whereas being married or cohabiting decreased that chance to 15% compared to those who were single. The Hosmer and Lemeshow goodness-of-fit index was insignificant (p = .658), indicating good model fit. The model predicted 81% of the cases into the right categories of high and low self-esteem, respectively.
Logistic regression analyses with self-esteem, empowerment and satisfaction with everyday activities as dependent variables.
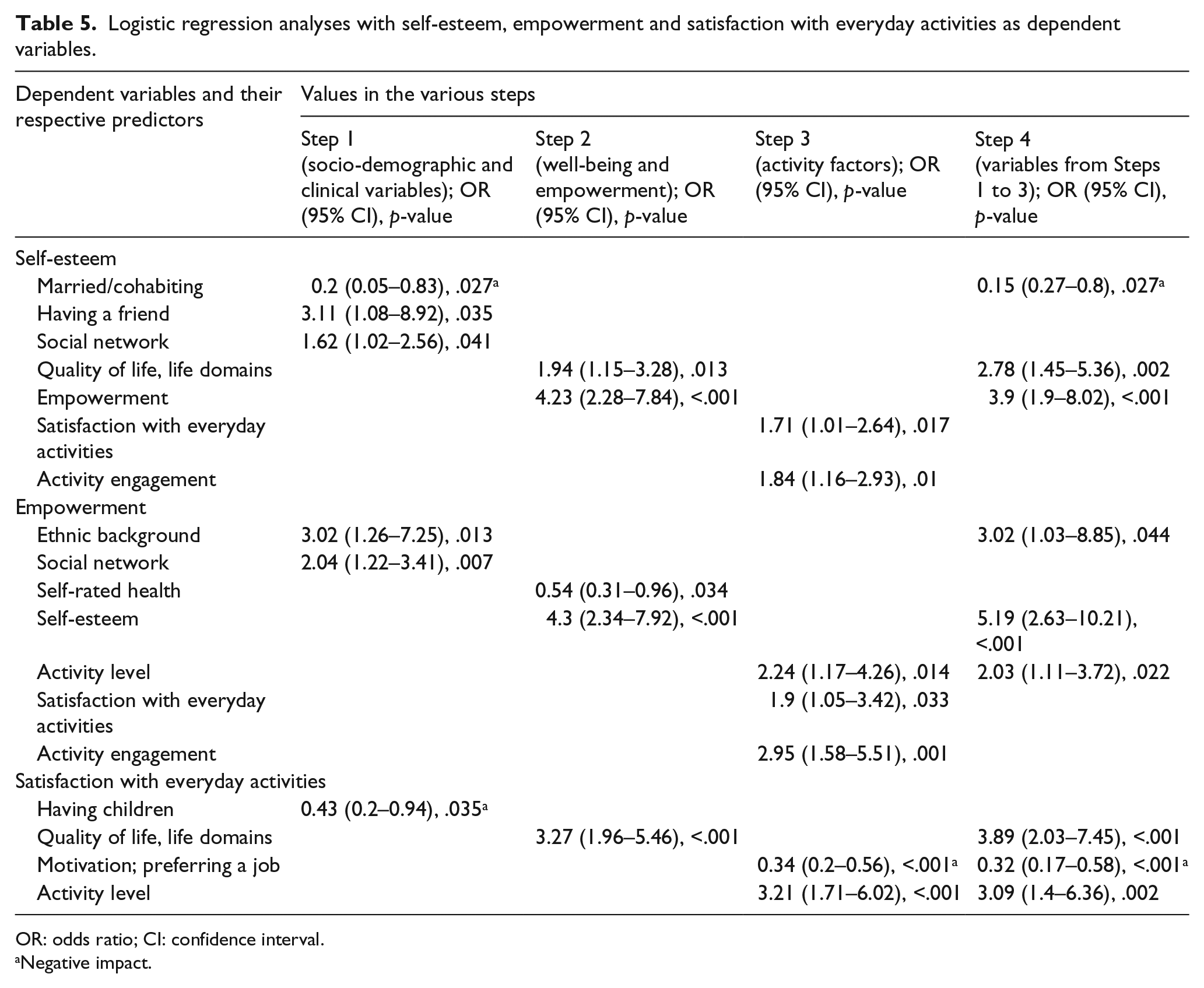
OR: odds ratio; CI: confidence interval.
Negative impact.
Self-esteem became the major explaining factor in the final analysis for empowerment, together with ethnic background and activity level explaining 57% of the variation. With an increase of one scale step (z-score) on self-esteem, there was more than a fivefold chance (OR = 5.19) of belonging to the high group on empowerment. Being Swedish-born tripled the chance of being in the high group of empowerment, compared to having an immigrant background. With an increase of one z-score on activity level, the probability of being in the high empowerment group was doubled. The p-value for the Hosmer and Lemeshow test was p = .663, suggesting satisfactory goodness of fit. The model predicted 79% of the cases into the correct groups of high and low empowerment.
With respect to satisfaction with everyday activities, quality of life, activity level and preferring a job to go to explained 55% of the variation. The strongest predictor was quality of life (OR = 3.89); thus, an increase with one z-score almost fourfolded the likelihood of belonging to the high group of satisfaction with everyday activities. A corresponding increase on activity level tripled the chance of being in the high satisfaction group. Finally, preferring work was a negative factor, and the OR of 0.32 indicates that an increment of one scale step (z-score) reduced the chance of being in the high group to about 30%. The Hosmer and Lemeshow test showed goodness of fit, p = .207. This model predicted 80% of the cases correctly.
Discussion
Those who had an immigrant background had a worse situation for perceived self-esteem, empowerment and satisfaction with everyday activities. It is interesting to note that when other potentially significant variables were further considered in logistic regression analyses, ethnic background was only significant in regard to empowerment. The double burdens of having a PMI and an immigrant background (Rew, Clarke, Gossa, & Savin, 2014) may thus infer a particular risk for a lower sense of empowerment. This is something that should be recognized and counteracted by the mental health services, since empowerment has been shown to be an important element in activity well-being (Pooremamali et al., 2015). Supportive measures that have been suggested in previous research are a strong therapeutic alliance, cultural awareness and sensitivity, involving significant others, and the use of culturally relevant community resources and activities (Pooremamali et al., 2015; Rew et al., 2014).
Some researchers have questioned whether empowerment is an appropriate phenomenon across cultures, due to differences in, for example, how autonomy, decision-making and personal development are valued (Bhugra, 2004; Bhugra & Becker, 2005; Triandis, 2001), and research has indicated that empowerment would be less relevant for people in collectivist cultures (Eylon & Au, 1999; Hui, Au, & Fock, 2004; Robert, Probst, Martocchio, Drasgow, & Lawler, 2000). This is, however, inconsistent with other research (Pooremamali et al., 2017; Pooremamali et al., 2015) showing that empowerment played a significant role in enhancing activity and mental well-being for day centre attendees originating from the Middle East, considered as representing collectivist cultures (Dwairy, 2006). Nevertheless, as concluded by Zimmerman and Warschausky (1998), there is a need to conceptualize empowerment differently depending on specific contexts and populations. This was beyond the aim of this study, but examining how empowerment intertwines with processes of acculturation is an important topic for future research.
Various factors, other than ethnic background, appeared to be important for self-esteem and satisfaction with everyday activities. Self-esteem and empowerment showed to be strongly associated, and each one was the most important factor in explaining the other. The relationship between these two phenomena is obviously strong (rs = .67 in this study). Satisfaction with everyday activities showed a different pattern with respect to explaining factors. Neither self-esteem nor empowerment was the strongest factor, although bivariate associations with these factors were statistically significant. Rating one’s quality of life at a high level and having a high level of general activity were indicative of belonging to the group with higher ratings for satisfaction with everyday activities, while preferring a job instead of going to the day centre predicted belonging to the group with lower activity satisfaction. It seems logical that activity level was related to satisfaction with everyday activities. Moreover, since very few in the targeted population have employment but many desire it (Eklund & Sandlund, 2015; Nordstrom et al., 2009), it also seems logical that preferring a job was related to reduced satisfaction with everyday activities. The findings indicate, however, that there is unused potential in the studied group of people with mental illness in that many desire employment, and that an immigrant background makes very little difference in this respect. Supported employment (Bejerholm et al., 2015; Bond et al., 2012) may thus be a suitable type of support, which should be made available to those who desire it. Since activity level also doubled the chance of perceiving a high level of empowerment, support in terms of activities seen as motivating and meaningful by the individual seems imperative. Activity should also be considered as a transactional experience, moving beyond individually based considerations to include others and the socio-cultural context as a whole (Dickie, Cutchin, & Humphry, 2006; Zur & Laliberte-Rudman, 2013). A transactional perspective might help staff and policy-makers become aware of how environments and contexts may act as barriers to activity enrichment and well-being for immigrants with PMI when these are offered culturally incongruent support and services and have limited opportunities for attachment and communication (Pooremamali et al., 2017; Pooremamali et al., 2015).
The participants with an immigrant background had been living in Sweden for a long time. This must be seen against our definition of an immigrant background, which inferred that a few who were even born in Sweden, but had one or both parents born outside Sweden, were included. Another explaining factor may be the choice of study context. People attending day centres have had a ‘career’ as mental health care users before they begin to attend a day centre. Many of the attendees with an immigrant background had thus lived in Sweden for decades, and in that respect, they have had a long period of time to become integrated into the Swedish society. This fact thus makes the differences between the attendees with an immigrant background and those who were native Swedes even more notable. Future studies should address people with a more recent immigration history and investigate whether they are even more at stake with respect to empowerment and the other well-being and activity factors at target in this study.
Methodological considerations
This was a correlational study and the direction of relationships could not be established, although the cause–effect relationship seems obvious in the case of ethnic background. Furthermore, the inclusion of various ethnic minorities in the study sample may have obscured possible differences between participants representing different cultures. Our choice of a broad definition for immigrant background may also be discussed. Studies including more ethnic homogeneity and less variety with regard to degree of acculturation would yield more specific insights, which would be a natural step following this study. Moreover, factors such as perceived stigma, discrimination and access to adequate support and resources may also differ in relation to ethnic background. The fact that stigma and discrimination were not addressed in this study constitutes a limitation, and future research should investigate the role of ethnic background in relation to perceived stigma and discrimination among people with mental illness.
Furthermore, this study was largely based on self-reports, and it has been debated whether people with severe mental illness and psychiatric disabilities give reliable responses. Research has shown that people with psychiatric disabilities produce reliable self-reports (Salzer, Brusilovskiy, Prvu-Bettger, & Kottsieper, 2014), but to avoid the risk of biased data we excluded people with comorbidities of conditions known to cause cognitive impairments. We were also careful not to exhaust the participants and inserted breaks with some refreshments. Finally, this study was performed in day centres, which limits the transferability of findings to other contexts.
Conclusion
People with a mental illness and an immigrant background experienced a lower level of well-being than native Swedes with equivalent mental health problems and the same type of support. Empowerment and self-esteem showed to mutually influence each other, and these factors and satisfaction with everyday activities were the core features that distinguished the two groups. An immigrant background was a negative factor particularly in relation to empowerment. This is alarming, and the mental health services and society at large should consider measures that can strengthen the support to this group. This should include an analysis of how environments and contexts may act as barriers to activity enrichment and well-being and to culturally congruent support. Further longitudinal studies are needed to examine how activity satisfaction and engagement develop during rehabilitation among people with mental illness and an immigrant background, and how activity factors intertwine with factors such as empowerment and various aspects of well-being.
Footnotes
Acknowledgements
The authors are grateful to Inger Thurfjell and Gunilla Wahlström Wärngård for performing most of the data collection.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Swedish Research Council for Health, Working Life and Welfare, Reg. no. 2014-4732, and the Swedish Research Council, Reg. no. K2014-99X-20067-09-4.