
Abstract
Background:
Refugees are at risk of psychiatric morbidity because of forced migration, traumatic events and resettlement in unfamiliar environments. Many live in low- and middle-income countries (LAMIC) under stressful conditions contributing to increased suicide risk.
Aims:
This study assessed the feasibility of regular contact and use of safety planning cards (CASP) by community volunteers (CVs) in reducing suicidal behaviour among Sri Lankan refugees residing in camps in Tamil Nadu, South India.
Methods:
A household survey was carried out on consenting adults in two refugee camps – one intervention and one control – randomly selected using lottery method. The primary outcome was reduction in suicidal behaviour. Experience of trauma during war and migration, depression, post-traumatic stress and alcohol use were documented. Individuals scoring >16 on Centre for Epidemiological Studies Depression (CESD) or >30 on Post-traumatic Stress Disorder (PTSD) or with active/passive suicidal ideation or a history of previous suicidal attempts were considered as high risk. CVs were trained to deliver CASP intervention to high-risk individuals. Change from baseline to follow-up was computed for intervention and control groups, and the difference between changes in suicide rates was compared using proportion test.
Results:
In total, 639 refugees from intervention and 664 from control camps participated. Of the 288 high-risk refugees in intervention camp, 139 completed the intervention. In the control camp, 187 were categorised as high risk. Prevalence of suicide attempts was 6.1%. Following intervention, differences between sites in changes in combined suicide (attempted suicides and suicides) rates per 100,000 per year were 519 (95% confidence interval (CI): 136–902; p < .01).
Conclusion:
CASP, an intervention involving contact by CVs and use of safety planning cards, is feasible to implement and can reduce suicidal behaviour among refugees. Its replication in more settings will enhance validity.
Introduction
Migration is one of the major challenges of the 21st century. Developing countries hosted 86% and the least developed countries 26% of the total number of refugees (United Nations High Commissioner for Refugees (UNHCR), n.d.). Refugees could be at excess risk of psychiatric morbidity because of forced migration, traumatic events and resettlement in unfamiliar environments (Fazel, Wheeler, Danesh, 2005; Hollifield et al., 2002). Being a refugee and asylum seeker, both directly and indirectly, can be stressful and disturbing, and such experiences are closely related to suicide and self-harm (Procter, 2004). A review on the prevalence of suicidal behaviour among refugees reported a range from 3.4% to 34% (Vijayakumar & Jotheeswaran, 2010). Goosen et al. (2011) found suicide rates of 25.6/100,000 for men and 4/100,000 for women among Dutch asylum seekers at reception centres. Procter, De Leo, and Newman (2013) reported that suicide was the leading cause of premature death among people in the Australian immigration detention network. A large number of refugees are in low- and middle-income countries (LAMIC) that are often struggling to maintain political stability and have poorly developed infrastructure and fragile health systems (Pedersen, 2002). Despite LAMIC taking on a sizeable proportion of the world’s refugees, research on this issue has largely been confined to those who have resettled in high-income countries.
Following the ethnic strife in Sri Lanka that began in 1984, a large number of refugees arrived by boats in Tamil Nadu in Southern India from where they were sent to several camps in the state. Currently, there are 111 camps hosting 67,165 refugees in the state. The refugees have been provided with accommodation, basic household articles, access to health and education facilities and a monthly allowance. They, however, face restrictions in travel, have difficulties obtaining jobs, are perceived as a security risk and, therefore, are under heightened surveillance. Concerned about the high prevalence of suicidal behaviour in these camps, the state department of rehabilitation and ‘Q’ branch which monitor these camps requested the Adventist Development and Relief Agency (ADRA, a non-governmental organisation (NGO) providing humanitarian assistance to refugees) and Sneha (a suicide prevention organisation) to address this issue, thereby providing the impetus for this study.
Randomised controlled trials conducted by World Health Organization (WHO) in multiple sites on the provision of Brief Intervention and Contact (BIC; Fleischmann et al., 2008) and other studies involving mailing supportive post cards following a suicide attempt revealed that provision of such contact was associated with a reduction in suicidal behaviour (Carter, Clover, Whyte, Dawson, D’Este, 2005; Hassanian-Moghaddam, Sarjami, Kolahi, Carter, 2011). The mental health Gap Action Planning (mhGAP manual by WHO (n.d.-a)) has recommended regular contact for those who have attempted suicide. Although a systematic review found only a weak effect (Milner, Carter, Pirkis, Robinson, & Spittal, 2015), the fact remains that such low-cost strategies are practical and feasible and, therefore, have value in resource-poor settings. Another strategy is the safety planning intervention. This comprises a concrete set of coping strategies and resources which are individualised and widely used in crisis centres and Veterans Hospitals in the United States (Stanley et al., 2016).
We adapted a combination of BIC and safety planning for our intervention. Thus, the CASP (contact and safety planning intervention) was developed which involved community volunteers (CVs) in the refugee camps making periodic visits to provide emotional support to individuals who were suicidal or depressed. The safety planning card consisted of an individualised list of coping strategies containing names and contact numbers of persons in the individual’s immediate family, social circle and health services who could be contacted during a suicidal crisis. This feasibility study aimed to assess the effectiveness and acceptability of CASP in reducing suicidal behaviour among Sri Lankan refugees residing in camps in Tamil Nadu.
Methods
Study design and participants
The study was carried out using a mixed-methods design involving a household survey and focus group discussions (FGDs). Prior to the commencement of the survey, FGDs in both camps were carried out to understand perceptions about suicidal behaviour in their camps and their attitude towards the community intervention programme. The same number of FGDs was repeated at the end of 15 months following completion of the intervention to explore issues concerning acceptability and usefulness of the intervention. The results of the FGDs are not discussed in this article. Of the 111 refugee camps located in Tamil Nadu, those having a population of 1,000 or more, which numbered 20, were considered eligible in order to have a larger population base to carry out our intervention. Using the lottery method, two camps were randomly selected from this list, one to represent the intervention camp – Kottapattu near Tiruchirapalli – and other to represent the control camp – Thoppukollai near Pudukottai. Prior to commencement of the intervention, an awareness programme on depression and suicide was carried out in the intervention camp which was then followed by a household survey in both camps. Consenting adults aged 18 years and above were approached to document their demographic information and their experience of trauma during war and migration. Assessments were also made of depression, suicidal ideation, post-traumatic stress and alcohol use. Those under treatment for mental disorders or suffered from a serious physical illness or were unable to communicate or refused to give consent were not included.
The primary outcome studied were reduction in suicide, attempted suicide and suicidal ideation. Suicidal ideation was measured using the modified 21-item Beck’s Scale for Suicidal Ideation (SSI) which was used in the WHO (n.d.-b) multisite intervention study on suicidal behaviour (SUPRE MISS) in Tamil Nadu. The scale consists of five screening items; those who indicated active and/or passive suicidal ideation were asked the additional 14 items. Depression was measured using the 20-item Centre for Epidemiological Studies Depression–Revised (CESD-R). The scale had been translated into Tamil and validated on an HIV population in Tamil Nadu and had good internal consistency (Mohanraj, 2014).
Alcohol use was measured using the Alcohol Use Disorders Identification Test (AUDIT) developed by WHO to identify hazardous or harmful use of alcohol (Babor, Higgins-Biddle, Saunders, & Monteiro, 2001). Post-traumatic stress was measured using the Post-Traumatic Stress Disorder Checklist (PCL) which had been translated into Tamil and validated in India (Rao et al., 2016).
The baseline and endline assessments were made by psychology and social work students from nearby colleges who were recruited and trained to administer the socio-demographic form and all the questionnaires. The inter-rater reliability was found to be good at .8. Those who had a score of 16 or more on the CESD-R, or presented with passive/active suicidal ideation, or had a history of previous suicidal attempts, or scored over 30 on the Post-traumatic Stress Disorder (PTSD) were categorised as high risk. Written informed consent was obtained at two time points: first, from all those who agreed to participate in the household survey at baseline and, second, from those who were classified as high risk and who consented to participate in the CASP intervention. Ethics approval was obtained from the Institutional Ethics Committee of the Voluntary Health Services (VHS), Chennai.
Sample size was calculated based on the Beck’s SSI (Beck, Kovacs, Weissman,, 1979). The mean score among suicide cases was reported to be 13.27 ± 5 units. It was decided to study at least 110 subjects in each group with 80% power, 5% level of significance and an anticipated 10% dropout with an effect size of two units across the intervention groups.
Intervention
ADRA personnel announced about the CASP intervention and the selection of CVs to deliver the intervention. Experienced volunteers from Sneha interviewed the applicants and selected nine women residing in the refugee camp as CVs from 26 applicants. They were interviewed to check on their willingness, their ability to empathise by asking them to narrate events during the war and migration, and their responses and their ability to maintain confidentiality. They underwent an intensive 20-hour training programme wherein communication skills, loss and grief, depression, suicide and empathetic offering of emotional support were communicated to them. They were also trained in obtaining informed consent and in filling the safety planning cards for each individual participant. They were given a monthly honorarium of Rs. 1,000 (~US$15). They were provided the list of individuals identified to be at high risk. Each CV was allocated a fixed number of these individuals whom they visited twice a month. During the visit, emotional support was offered and suicide risk was assessed. The CVs in consultation with each individual listed the warning signs, coping strategies and list of available support in the safety planning cards. Participants were encouraged to use the cards when in distress. After every visit, a short contact form was filled, which was based on the SUPRE MISS follow-up form. If there was an imminent risk for suicide, ADRA and Sneha volunteers were immediately informed who then provided the necessary care and referrals. A monthly review of the contact forms and discussions with the CVs were undertaken by designated Sneha volunteers for clarifying doubts, initiating referrals and providing support to the CVs. Those who needed professional intervention were referred to the psychiatric department of the Government Hospital, but logistical and infrastructural difficulties proved a major deterrent. Thus, after 4 months, the help of a private psychiatrist was sought who offered both his services and medication free of cost. Every month ADRA representatives escorted these patients for review.
In the control camp, posters containing contact numbers of Sneha and ADRA were displayed. Those in the high-risk group were informed of available mental health resources and urged to avail them. All outcome assessments were made at baseline and again at the end of 15 months following the intervention in both camps.
Statistical analysis
The quantitative data were entered using Epi Info Software and analysed using STATA 13.0. The rates of suicides, attempted suicides and composite outcome (suicide and attempted suicide) per 100,000 population per year were calculated. The analyses were done based on intention-to-treat (ITT) principle. The change from the baseline to follow-up rate was computed for the intervention and control groups. The difference between these changes in suicide rates was compared using proportion test. Two-sided test was considered for statistical significance. The change in CESD, PTSD and suicidal ideation scores was computed between baseline and follow-up measures and was checked for normality. These changes between two groups were compared using Student’s t-test.
Results
Sample description
Figure 1 shows the study profile. In total, 639 refugees residing in the intervention camp and 664 residing in the control camp participated in the study. The demographic characteristics of the refugees in the two camps in terms of age, gender, marital status and duration of residency were largely similar. The mean age of participants in the intervention and control camps was 41.58 years (15) and 39.1 years (±15.1), respectively. Their differences lay with respect to educational, occupational and religious characteristics. The intervention camp had more non-literate (11.3% vs 5.7%) and less-skilled persons (12.6% vs 24.6%). There were more Christians and Muslims in the control camp as compared to the intervention camp (38.4% vs 20.1%; Table1).
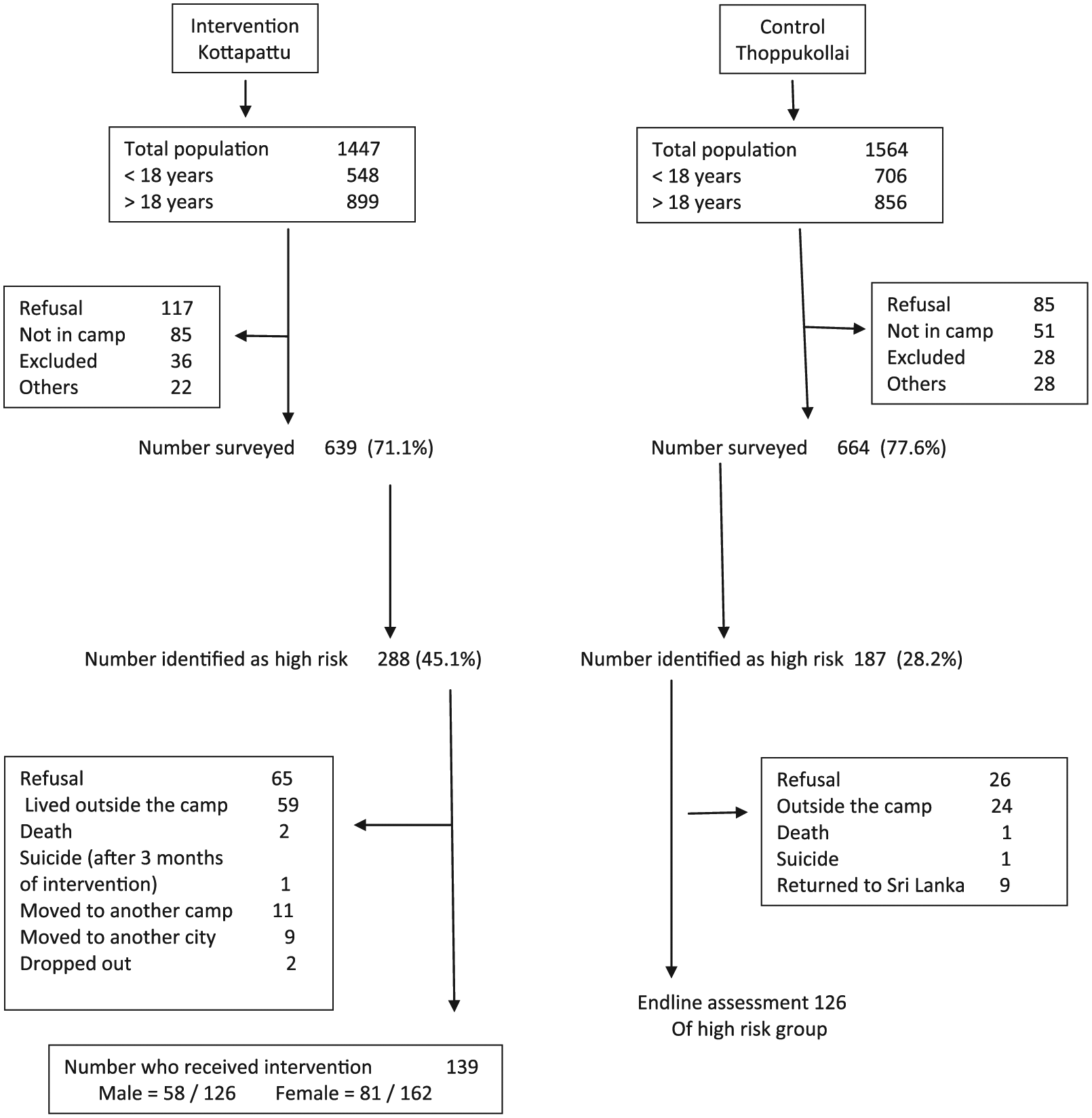
Study profile.
Baseline demographics.

Psychological variables – baseline
There were significant differences between the two sites with regard to symptoms of depression and post-traumatic stress. The mean CESD score was 11.03 (±15), with almost 25% having significant depressive symptoms in the intervention camp, whereas it was 7.32 (±12.7) and 17% in the control camp. The mean score for post-traumatic stress symptoms in the intervention camp was 28.15 (±11.80), with 35.6% presenting with clinically significant post-traumatic stress symptoms compared to 20% in the control camp. Suicidal ideation in the past 2 weeks was present in nine refugees in the intervention camp (mean: 15.33 (±5.2)) and seven in the control camp (mean: 16.43 (±6.2)). The mean AUDIT scores were 14.67 (±7.17) in the intervention and 10.31 (±2.52) in the control camp.
We assessed trauma by eliciting the experience of separation or death of a family member during the war and at the time of migration. War caused more trauma than migration. Trauma by separation or loss of a significant family member during war was significantly more among refugees in the intervention camp (36%) compared to those in the control camp (26%) (Table 2).
Prevalence of suicidal ideation, depression, post-traumatic stress, harmful alcohol use and trauma at baseline.

PTSD: post-traumatic stress disorder.
In total, 288 refugees (45%) in the intervention camp and 187 (28.2%) in the control camp were categorised as high-risk groups. Of the 288 refugees, only 139 completed the CASP intervention. Fourteen persons in the high-risk group in the intervention camp were identified as needing professional intervention. Of these, seven consented and were treated by the psychiatrist with medication, psychotherapy and regular follow-up. The remaining seven refused. There were 80 refugees with a prior history of suicide attempts in both the camps. Table 3 reveals that those with a previous history of suicide attempts exhibited clinically significant depressive and post-traumatic stress symptoms compared to those without such a history.
Demographic details of refugees with a history of suicide attempts.

IQR: interquartile range.
Suicides and suicide attempts – baseline and during intervention
In the 15 months prior to the intervention, there were four suicides and nine attempts in the intervention camp. Suicides were by immolation (two women), poisoning (one woman) and hanging (one man); suicide attempts were by hanging (three men), poisoning (two women) and self-immolation (four women). In the control camp, there was one suicide by hanging (man) and two attempts, a man and a woman, by hanging.
During the CASP intervention period, there was one suicide by a 24-year-old woman in the intervention camp through self-immolation during the sixth month of intervention. She had refused professional help when provided. There were also five suicide attempts, one by a 17-year-old boy who attempted suicide by poisoning. He had not been included in the baseline survey. Three women, identified as high risk, refused to participate in the intervention. Two attempted suicide by poisoning and one by hanging. The fifth person, a male, who had been abusing drugs refused professional intervention and attempted suicide by poisoning during the third month of intervention. All of them were referred for consultation following their suicide attempts. In the control camp, there was one suicide by a 54-year-old man by hanging and two suicide attempts by women through poisoning.
Table 4 presents the suicide behaviour data. With regard to suicides, the rates of change from baseline to follow-up in the intervention and control camps were 223/100,000 and 0/100,000 respectively. The difference in change between the two camps was 223 (95% confidence interval (CI): −29–474) and was not significant. With regard to attempted suicides, the difference in change was 296/100,000 (95% CI: 6.7–587) which was significant (p = .05). When suicides and attempted suicides were combined, the analysis showed a difference of 519/100,000 which too was significant (p = .01). In the intervention camp, there were 13 suicides and attempted suicides before intervention which reduced to 6 after the intervention. There was no change in the control camp.
Suicide, attempted suicide and combined outcome.
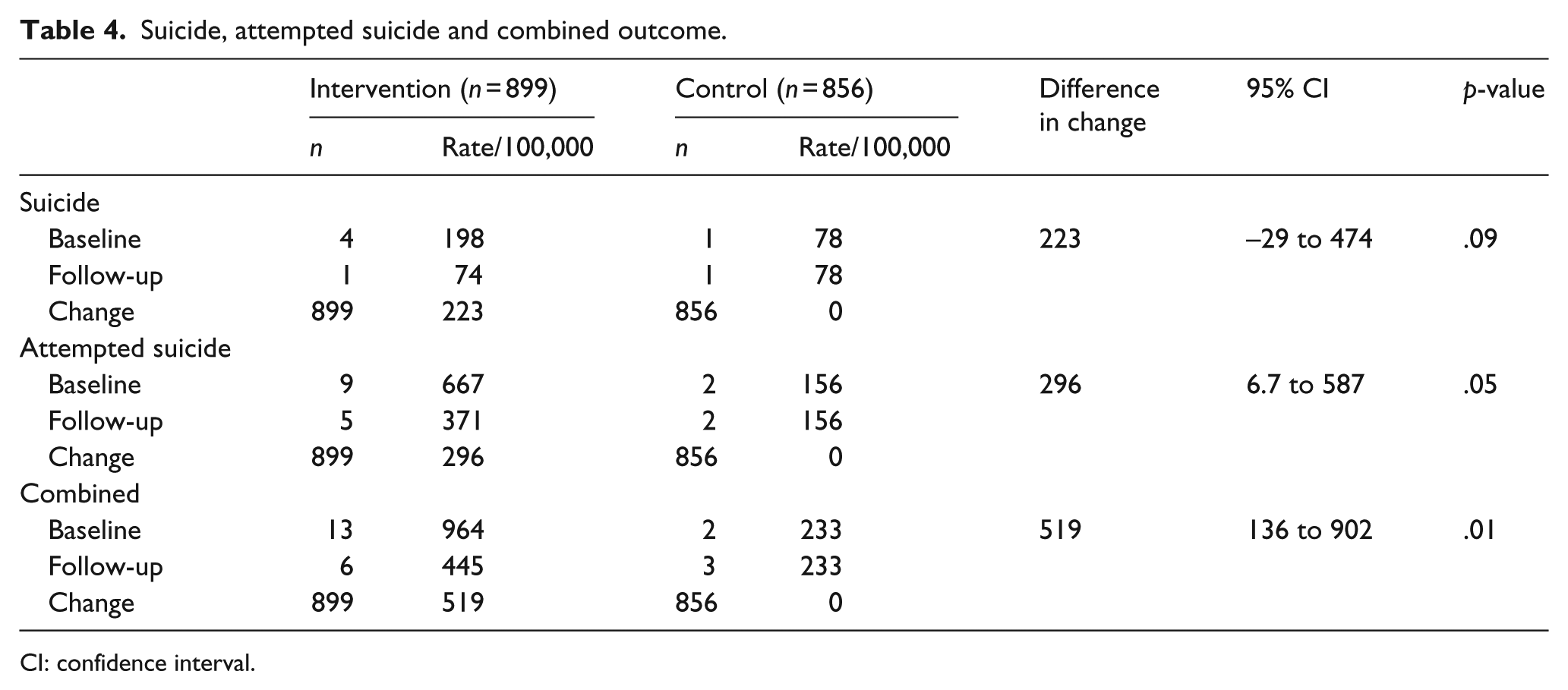
CI: confidence interval.
The change in the percentage of refugees with ‘suicidal ideation’ at baseline and ‘no suicidal ideation’ at follow-up was 55.6% in the intervention camp and 28.5% in the control camp. The difference was 26.9% (−19 to 73), which was not statistically significant. As there were three and five dropouts in the intervention and control camps, respectively, the ‘best’ and ‘worst’ case scenario analysis was carried out, which was also not statistically significant.
We analysed the mean depression and PTSD scores for the139 high-risk intervention refugees before intervention. For depression it was 21.54 (±17.3) and for PTSD it was 37.24 (±11.7). Post-intervention, the mean depression scores were 14.7 (±19.8) and PTSD scores were 30.6 (±12.0). However, when compared to the control camp, these differences in the means scores were not significant.
The FGDs too revealed that the CVs who served as an important point of contact with the community were well received, seen as individuals who were both supportive and encouraging and who gave useful advice. This motivated the intervention participants into engaging in behaviours that were positive and not destructive.
Discussion
To our knowledge, this is the first study to report an intervention aimed at reducing suicidal behaviour among refugees residing in camps in LAMIC. Our findings show that CASP consisting of regular contact and safety planning intervention delivered by trained CVs from the camps has the potential to reduce suicidal behaviour. Our intervention had two components and it precludes our ability to identify their respective contributions.
CASP is an intervention which can be easily delivered by trained CVs. The Inter-Agency Standing Committee, in fact, specifically recommends the utilisation of community self-help and social support. Recent studies have also shown the effectiveness of using lay counsellors in reducing depression and treatment gap for depression in India (Patel et al., 2017; Shidhaye et al., 2017). The CVs in our study by virtue of residing in these camps had the advantage of sharing the same language and culture of the refugees, thereby enhancing their acceptability. Stanley et al. (2016) found that SAFE VET, an intervention combining safety planning intervention and structured follow-up and monitoring, was acceptable and helpful in preventing further suicidal behaviour. A recent multi-centre study carried out in 1,376 emergency department, patients with recent suicide attempts or ideation found that an intervention consisting of expanded suicide risk assessment, self-administered safety planning and telephone calls resulted in a 5% absolute decrease in the proportion of patients subsequently attempting suicide (Miller et al., 2017). In our study too, participants viewed the safety planning card as a lifeline as it gave them ready access to a support system in times of crisis.
Bolton et al. (2007) used interpersonal therapy (IPT) and creative play among two groups of adolescents living in refugee camps in Uganda and found lowered scores for depression in both groups. Narrative Exposure Therapy and Trauma Therapy among Rwandan and Somalian refugees in Uganda were also found to be effective in reducing depression (Neuner, Schauer, Klaschik, Karunakara, & Elbert, 2004). However, these are intensive individual therapies requiring qualified personnel. Given resource constraints in LAMIC, CASP offers a practical and feasible solution to reducing suicidal behaviour. But its usefulness in reducing depression and trauma could not be proven in this study, suggesting the need for further research in this area.
Suicide attempts were found in 6.1% of surveyed refugees in our study. Ferrada-Noli, Asberg, Ormstad, Lundin and Sundbom (1998) reported that 40% of refugees in Sweden had attempted suicide, while another study reported that close to 40% of refugees made a suicide attempt following rejection of their asylum status (Sundvall, Tidemalm, Titelman, Runeson, & Bäärnhielm, 2015). Tousignant et al. (1999) reported 3.4% refugees in Canada had attempted suicide. Seven people identified as needing professional help for management of their depression and suicidal ideas who had participated in CASP were provided additional referrals, hence preventing potential suicides and attempts. Three persons who refused intervention and subsequently attempted suicide suggest that more proactive efforts are needed to enhance the reach of the programme.
Several challenges were encountered during the study. First, the prevalence of suicidal behaviour in the camps could reflect poorly on the government, and hence, there was considerable difficulty in obtaining permission from the various departments to conduct the study. Second, the refugees in the camp were reluctant to disclose their suicidal ideation as they felt that it could jeopardise their chances of relocation to developed countries such as United Kingdom and Canada. Third, it was difficult to maintain confidentiality in a closed camp. Regular visits by the CVs to their allotted high-risk persons sparked off speculations about the purpose of their visits, particularly for female CVs. Fourth, certain members of the camp were able to influence others in the community which had an impact on the study. For example, one applicant for the position of a CV was rejected. She, in turn, convinced 34 of her neighbours not participate in the baseline survey. Finally, as the CVs were residing in the camp, unscheduled contacts were made in the bus stand, shops and so on. Initiating a referral system to the mental health services was also a major challenge.
While we anticipated a two-unit reduction in the mean score, the basis on which sample size was calculated, we could not carry out the same as we did not have the endline scores on suicidal ideation. Another limitation of this study was that alcohol use disorder which is closely linked to suicide had not been addressed even though it was prevalent. We could not formulate an effective intervention for it which could be delivered by the CVs. There were demographic and psychological differences between the camps although they were chosen by lottery method. Another limitation was the high number of refusals for participation in the survey and in the intervention. This could be due to the stigma associated with suicide, lack of awareness about mental health and identification becoming a barrier for relocation. Furthermore, we did not use structured therapies. We developed an intervention of provision of contact and safety planning with supervision as they are evidence based and could be delivered by CVs. Similar to other suicide intervention studies, adequate power was not there to detect differences in deaths by suicide. The study was done in only one refugee camp which limits the generalisability of the findings. It will need to be replicated in a wider context involving larger populations. Many of the refugee camps in developing countries face similar resource constraints, and it is feasible to implement CASP in refugee camps in LAMIC.
Footnotes
Acknowledgements
We are very grateful to Ms Roja and Mr Elango, to volunteers from Sneha for training and supervision of the community volunteers and to all the volunteers from ADRA for their assistance in this project. Our special thanks to Dr G Gopalakrishnan for providing his services without remuneration and gratitude to Dr Jeyaseelan for his statistical support.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ADRA and Sneha jointly funded the project. However, data collection and evaluation were entrusted to an independent team of social scientists. Data management and analysis were entrusted to a biostatistician of an independent institute. The corresponding author had full access to all data in the study and had the final responsibility for the decision to submit for publication.