
Abstract
Background:
Prevalence rates of mental health disorders in migrants are controversial. The socio-historical and economic background of the host country may play an important role in the mental health status of migrants. As studies are mostly conducted in developed countries, researching migration in developing countries may add important information to scientific literature.
Aims:
This study aims to investigate the prevalence and factors associated with posttraumatic stress disorder (PTSD), anxiety and depression symptoms in Haitian migrants in southern Brazil.
Methods:
The sample comprises 66 participants selected from four different sites in three cities of a Brazilian southern state. Participants fulfilled a sociodemographic questionnaire, as well as instruments investigate traumatic events; post-migration difficulties and symptoms of PTSD, anxiety and depression. Linear regression models were utilized to investigate factors associated with PTSD, anxiety and depression symptoms.
Results:
PTSD prevalence in the sample was 9.1%. Depression and anxiety symptoms were in the clinical range of 10.6%–13.6% of participants, respectively. A number of traumatic events, acculturation difficulties, discrimination and low social support were associated with the investigated mental health disorders.
Conclusion:
The results point to the importance of public policies in promoting better social and mental health support for migrants. Providing information to the Brazilian population about migration may improve receptiveness in the host society.
Introduction
The associations between migration and mental health have been the focus of many studies, especially in North American and European countries (Alegria, Atkins, Farmer, Slaton, & Stelk, 2010; Bhugra, 2004; Lindert, Ehrenstein, Von Priebe, Mielck, & Brähler, 2009; Pumariega, Rothe, & Pumariega, 2005). Rates of mental disorders in voluntary migrants vary, and several authors point to an epidemiological paradox, known as the immigrant paradox, defined by lower rates of mental health problems in immigrants than in nationals. This phenomenon occurs despite the greater exposure to risk factors related to migration (Breslau et al., 2007). However, evidence indicates that the occurrence of the immigrant paradox may be specific to certain populations and contexts (Lau et al., 2013; Sam, Vedder, Liebkind, Neto, & Virta, 2008). Posttraumatic stress disorder (PTSD) has been widely studied in refugee samples, but studies with voluntary migrants are still needed to better understand prevalence rates and associated factors in this population (Bogic, Njoku, & Priebe, 2015; Lindert et al., 2009).
Haitian migration to Brazil has increased in recent years, especially due to the Brazilian government offering of humanitarian visas to Haitian nationals since the 2010 Haiti earthquake that devastated the country and resulted in 222,000 deaths and let 2.3 million homeless (United Nations [UN], 2010). According to the UN (2010), decades of chronic political instability left a great number of Haitians vulnerable to the consequences of natural disasters. Haiti is the poorest country in the Americas and more than 6 million (59% of the population) live under the poverty line of US$ 2.42 per day. Haiti’s Human Development Index (HDI) is estimated to be .48, with the gross national income (GNI) being 1,668.7 (UN, 2015; World Bank, 2016). There are also reports of high levels of violence, corruption, human rights violations and unemployment (Cénat & Derivois, 2014; Cerdá et al., 2013; Kolbe & Hutson, 2006). Regarding the Brazilian context, the HDI is estimated to be .75 and the GNI 15,175. Despite the better economical context when compared to Haiti, Brazil also faces elevated violence levels, especially against low-income youth (UN, 2015; Waiselfisz, 2014).
This study is developed in Rio Grande do Sul, the southernmost Brazilian state (Handerson, 2015; International Organization for Migration, 2015; Seixas, 2014). The state has a high HDI (.746), and the number of migrants in the state has doubled since 2010, especially due to the increase in the state’s economy and job offers (Uebal, 2015). Presently, it is estimated that 40,000 Haitians live in Brazil, and that 1,575 live in the south. Although several Haitian migrants enter Brazil as asylum seekers, they are officially labeled voluntary migrants because refugee status is not granted to natural disasters victims (UN, 2016).
Economic migrants may also undergo traumatic events; however, few studies have investigated PTSD in this population (Lindert et al., 2009). PTSD prevalence in studies with migrants varies between 2.6% and 62% (Breslau et al., 2011; Carrer et al., 2011; de Bocanegra, Moskalenko, & Kramer, 2006; Kang, Razzouk, Mari, & De Shirakawa, 2009; Meeske et al., 2013; Norris, Van Landingham, & Vu, 2009; Rasmussen, Crager, Baser, Chu, & Gany, 2012; Tagay et al., 2008). Regarding anxiety and depression symptoms, a systematic review that included studies from 1994 to 2007 found a combined prevalence of 20% for depression and 21% for anxiety among labor migrants (Lindert et al., 2009). The process of migration comprises series of events in different levels of analysis (e.g. social and individual) that may influence the mental health status of migrants. Variables such as sex, age and biological vulnerability are related to the onset of mental health problems (Brewin, Andrews, & Valentine, 2000). However, focusing on individual factors is not sufficient to understand the complex patterns of protective and risk factors for mental health disorders in migrants. The acculturation process may play an important role in the mental health status of migrant populations (Bhugra, 2004; Meeske et al., 2013).
Acculturation occurs when individuals from different cultural backgrounds come in contact. This phenomenon may be studied in broader or more specific levels from ethnocultural groups to individuals, the latter being called psychological acculturation (Berry, 2006; Graves, 1967). The acculturation process encompasses not only the migrant’s adaptation but also the receptiveness of the host society. Conflicts between migrants and members of the host country (e.g. discrimination) may result in acculturative stress for the migrant, that is, difficulty in dealing with problems that result from intercultural contact (Berry, 2006). Several studies have found associations between acculturative stress and mental health problems (Aragona & Pucci, 2012; Chae, Park, & Kang, 2014; Chou, Asnaani, & Hofmann, 2012; Drogendijk, Van Der Velden, & Kleber, 2012; Gee, Spencer, Chen, Yip, & Takeuchi, 2007; Kartal & Kiropoulos, 2016). Post-migration living difficulties (PMLD) include issues related to the acculturation process, such as racial discrimination, unemployment and low proficiency in the new language. Studies investigating the relationship between PMLD and mental health found that higher levels of these difficulties were associated with higher levels of PTSD, anxiety and depression (Aragona & Pucci, 2012; Carrer et al., 2011; Schweitzer, Melville, Steel, & Lacherez, 2006).
The socio-historical background of the host country has important influences on migrants’ mental health. Countries with long-term high rates of immigration may provide more social support for immigrants (Kirmayer et al., 2011). Additionally, country laws regarding migration and economic development may also influence migrants’ acculturation and mental health (Lindert et al., 2009; Morawa & Erim, 2014). In this sense, the Brazilian economic and social contexts differ from those in which most studies in migration and mental health are conducted. For example, the estimated prevalence rate of traumatic events in the United States is 21.4%, while the expected rates in the Brazilian cities of São Paulo and Rio de Janeiro are 86% and 88.7%, respectively (Perkonigg, Kessler, Storz, & Wittchen, 2000; Ribeiro et al., 2013). Furthermore, the humanitarian visa provides all Haitians in Brazil with a legal status and the right to work, what may be a protective factor regarding exposure to traumatic events and post-migratory difficulties (Carrer et al., 2011; Pumariega et al., 2005).
Quantitative studies have investigated the mental health of immigrants in Brazil (Girardi, Borges & Bousfield, 2016; Kang et al. (2009) investigated the prevalence of mental health disorders in Korean migrants in São Paulo. The lifetime prevalence of PTSD, anxiety disorders and mood disorders were, respectively, 9.6%, 13% and 8.6%. The authors found that Korean migrants, in comparison with Korean Nationals living in South Korea, presented higher rates of PTSD (9.6 vs. 1.7), mood disorders (8.6 vs. 4.7) and anxiety disorders (13 vs. 9.1). However, compared with the Brazilian population, Korean migrants presented lower rates of mood disorders (8.6 vs. 18.4) and similar rates of anxiety disorders (13 vs. 12.5). The prevalence of PTSD in the Brazilian population was not reported in this study. However, another study conducted in São Paulo estimated the PTSD lifetime prevalence to be 10.2% (Ribeiro et al., 2013), higher than the 9.6% found in Korean immigrants (Kang et al., 2009). Other researchers have investigated the mental health of immigrants in Brazil through questionnaire validation studies (Wang, Andrade & Gorestein, 2005; Wang, Gorenstein, & Andrade, 2004) and case studies (Medeiros, Sampaio, Sampaio, & Lotufo-Neto, 2014).
Considering the need for more studies focusing on PTSD in voluntary migrants and on contexts other than those from mainstream research, this study aims to investigate PTSD, anxiety and depression symptoms’ prevalence and associated factors in Haitian migrants in southern Brazil. The prevalence of traumatic events and PMLD is also investigated, as well as the relationship between PMLD, traumatic events, individual factors, PTSD, anxiety and depression.
Method
Participants
Using a convenience sampling strategy, 66 participants were recruited from four sites. Inclusion criteria were (a) first-generation immigrants, (b) at least 18 years old and (c) able to speak French. Participants who lacked language proficiency to understand the questionnaires were excluded from the study.
Procedures
The interviews were conducted in a school offering Portuguese classes for immigrants, a workers’ union, a shelter for immigrants and an institution that helps immigrants with bureaucratic issues in the capital of the state. The Ethics Committee of the Pontifical Catholic University of Rio Grande do Sul approved this study (Report # 1.164.938). All participants provided written informed consent before being interviewed and did not receive any compensation for participation. Data collection lasted 7 months from September 2015 to April 2016. All material used during data collection, the written consent, instruments and the interviews were carried out in French by a Brazilian psychologist proficient in French in individual sessions of approximately 40 minutes. The participants were referred to health services when any mental or physical health problem was detected.
Instruments
Sociodemographic interview
A sociodemographic questionnaire was developed for this study. It consists of questions assessing age, sex, schooling, profession, employment, income, marital status and so on.
Hopkins Symptom Checklist – 27
The Hopkins Symptom Checklist (HSC) contains 27 self-report items answered through a four-point Likert scale (Mollica, Wyshak, de Marneffe, Khuon, & Lavelle, 1987). The instrument investigates anxiety and depression symptoms based on Diagnostic and Statistical Manual of Mental Disorders (DSM; 4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000) symptoms. The French version of the checklist was translated, adapted and validated by de Fouchier. (2013). The cut-off point described by de Fouchier. (2013) was 2.5, which may underestimate the symptoms in immigrants, given that the scale was validated with torture victims. Therefore, we have used the cut-off point of 1.75 in this study, as suggested in the original study (Mollica et al., 1987). The Cronbach’s alpha coefficient in our sample was .84.
List of migration experiences
The list of migration experiences (LiMEs) is a self-administered instrument that investigates traumatic events in immigrants (Aragona et al., 2014). It comprises 59 items enumerating types of traumatic events and stipulating if each event occurred before, during or after the migration process. The instrument also investigates post-migration difficulties experienced by immigrants (e.g. low access to health care). The validation study presented high internal consistency (α > .90) with a sample of 193 francophone participants who migrated to Italy.
PTSD checklist
The PCL-5 (PTSD checklist) is a self-report scale composed of 20 items answered through a four-point Likert scale (Weathers et al., 2013). The instrument assesses the severity of PTSD symptoms and provides a diagnostic measure of PTSD. Severity scores are calculated either through the total sum of items or through items representing individual symptoms of each cluster. The Cronbach’s alpha for this sample was calculated for the total scale (.83) and for clusters B (.70), C (.98), D (.50) and E (.62).
Data analysis
Data analysis was conducted on SPSS 20.0. Multivariate analyses of variance (MANOVAs) were conducted to investigate potential differences between anxiety, depression and PTSD symptoms and sociodemographic variables in the data collection sites. Pearson correlations, chi-square, and t-tests were performed to investigate possible associations and differences between demographic data; exposure to traumatic/stressing events and depression, anxiety and PTSD symptoms. Variables that showed significant association with anxiety, depression and PTSD were included in the linear regression models. A level of significance p < .05 was predetermined.
Results
The final sample is comprised of 66 first generation Haitians migrants. Sociodemographic data are presented in Table 1.
Sociodemographic data.
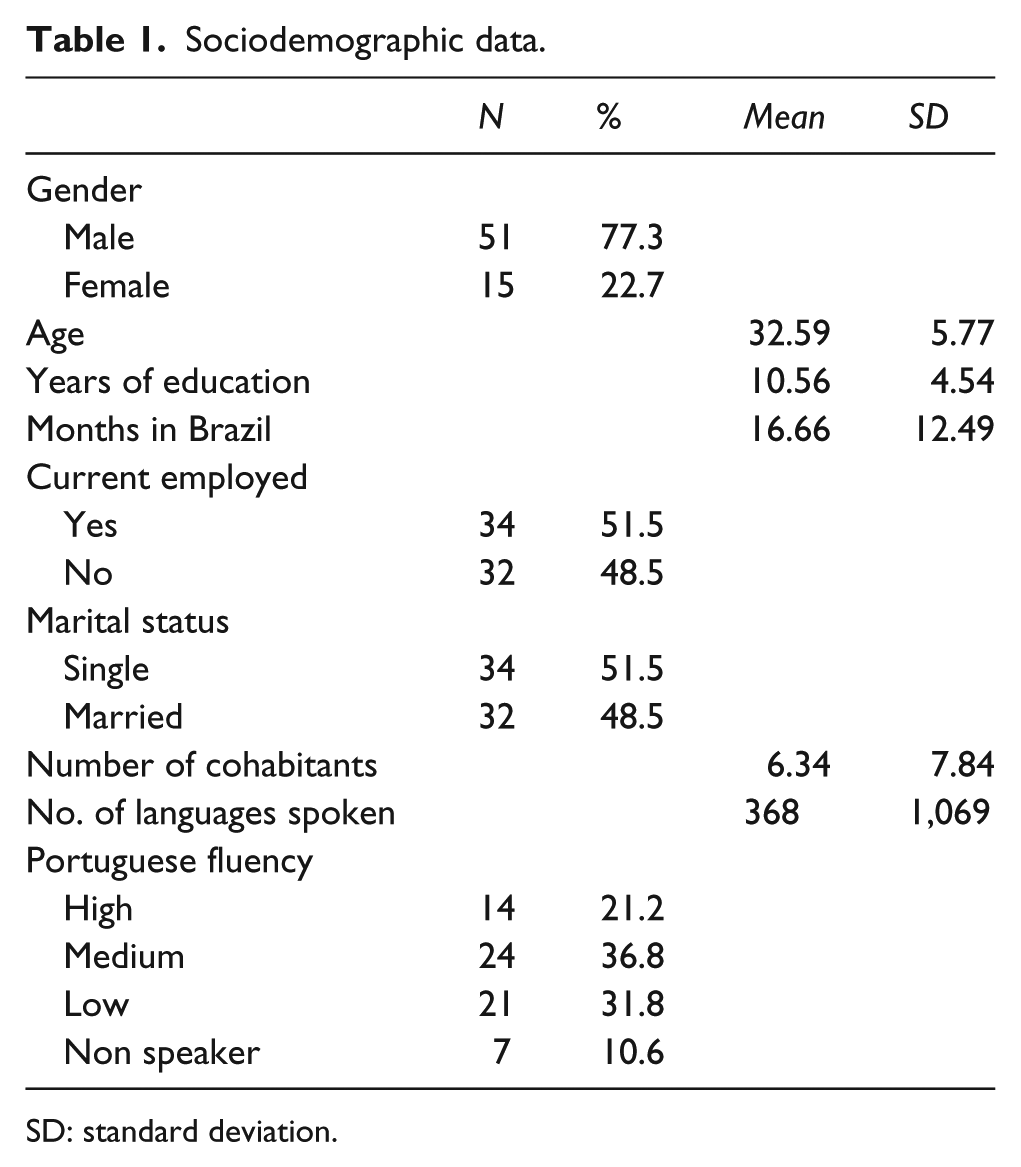
SD: standard deviation.
Almost all participants (93.9%) reported having a religion. Demographic and socioeconomic status classification was based on Brazilian public economic criteria (ABEP, 2008). One (1.5%) participant was in the middle class (B), and all others (98.5%) were in the low class (C, D or E).
Prevalence of traumatic events and PMLD
Participants were exposed to an average of 2.17 traumatic events, according to events described under the DSM-5 (5th ed.; DSM-5; APA, 2013) Criterion-A (APA, 2013) during their lifetime (min = 0; max = 6; standard deviation (SD) = 1.6). Natural catastrophes were the most prevalent event, affecting 40 participants (60.6%), followed by non-natural death of a family member (n = 29, 43.9%), vehicle accidents (n = 17, 22.7%), death of a family member by murder (n = 8, 12.1%) and imprisonment (n = 7, 10.6%). The average frequencies of traumatic events during and after migration were low, respectively, .18 (min = 0; max = 2; SD = .52) and .38 (min = 0; max = 3; SD = .76).
Events that are not addressed by Criterion-A were also investigated before and during migration. The most frequent stressful events reported by the participants before migration were lack of food and water (n = 19, 28.8%), poor living conditions (n = 10, 10.6%) and stressful work conditions (n = 9, 13.6%). During migration, lack of food and water (n = 13, 19.7%) and living in overcrowded temporary shelters (n = 9, 13.6%) were cited as stressful events.
The most frequent PMLD were concerns about family in the home country (n = 48, 72.7%), impossibility of returning home in an emergency (n = 40, 60.6%), loneliness and boredom (n = 39, 59.1%), living in an overcrowded home (n = 29, 43.9%), lack of adequate living conditions (n = 26, 39.4%), unemployment (n = 34, 51.5%), lack of food and water (n = 19, 28.8%) and discrimination (n = 18, 27.3%).
PTSD
Prevalence of PTSD in the sample was 9.1% (n = 6), following DSM-5 criteria. However, not all individuals with PTSD report elevated symptom severity when considering the cut-off point of 37 suggested for the PCL-5, ranging from 20 to 51 points (M = 30.33, SD = 11.37). Participants were asked to choose, according to their perception, the most stressful event they have experienced. The most stressful events reported by participants with PTSD were the recent Haitian earthquake (50%, N = 3) and situations of interpersonal violence/robbery (50%, N = 3). Participants with PTSD were younger than those without PTSD, but the difference was only marginally significant t(64) = 1.93, p = .057, Cohen’s d = .48.
Pearson’s correlations were performed between time spent in Brazil, years of study, number of traumatic and stressful events and PTSD symptoms. Correlations between sociodemographic variables and PTSD were not significant – time in Brazil (r = .074, p = .56) and years of study (r = −.057, p = .65). A correlation was found between the number of traumatic events before migration and PTSD symptoms (r = .459, p < .001), as well as between PMLD and PTSD symptoms (r = .372, p = .002). T-tests were conducted to compare PCL-5 scores with each PMLD. Individuals who experienced difficulties adapting to the new culture reported more PTSD symptoms (M = 17.22, SD = 7.77) than those who did not present adaptation difficulties (M = 9.94, SD = 10.42), t(64) = 2.00, p = .05, Cohen’s d = .05. Participants who were unable to return to their home country in an emergency present more PTSD symptoms than those who could (M = 13.17, SD = 10.58 vs. M = 7.50, SD = 9.17), t(64) = 2.24, p = .02, Cohen’s d = .56. Those immigrants who were victims of discrimination also presented more PTSD symptoms (M = 15.72, SD = 14.23) than those who did not experience discrimination (M = 9.14, SD = 7.95), t(64) = 2.37, p = .02, Cohen’s d = .60. A linear regression model (Model 1 in Table 2) included post-migration difficulties as independent variables, with PTSD symptoms severity as the dependent variable. All variables in the model were significant, and the model explained 21.5% of PTSD symptoms variance. When the number of traumatic events was added to the model as an independent variable (Model 2), the explained variance increased to 32.5%.
Linear regression analyses of PTSD symptoms for the total sample.

PTSD: posttraumatic stress disorder.
PTSD checklist (PCL-5) total score as the dependent variable.
Anxiety and depression symptoms
Mean scores were calculated for anxiety (M = 1.31, SD = .30) and depression (M = 1.38, SD = .32). The prevalence of high depression and high anxiety symptoms were 10.6% (N = 7) and 13.6% (N = 9), respectively.
Anxiety symptoms were correlated with PTSD symptoms (r = .53, p < .001), number of traumatic events before migration (r = .37, p = .002) and number of post-migration stressors (r = .38, p = .001). No significant correlations were found with age (r = .032, p = .80) or time spent in Brazil (r = .072, p = .57). Depression symptoms were also correlated with PTSD symptoms (r = .49, p < .001) and with the number of post-migration stressors (r = .47, p < .001), but were only marginally correlated with the number of traumatic events before migration (r = .23, p = .062). Moreover, no significant correlations were found with age (r = .074, p = .55) and time spent in Brazil (r = .062, p = 62).
Regarding specific PMLD, high symptoms of depression were present in participants who had (a) poor access to health services, marginally significant (M = 1.5, SD = .43 vs. M = 1.3, SD = .30), t(63) = 1.87, p = .065, Cohen’s d = .47; (b) ethnic discrimination (M = 1.51, SD = .37 vs. M = 1.3, SD = .29), t(63) = 1.9, p = .051, Cohen’s d = .47; (c) difficulties related to adjustment and coping with culture (M = 1.6, SD = .47 vs. M = 1.33, SD = .27), t(63) = 3.2, p = .002, Cohen’s d = .80; (d) loneliness and boredom (M = 1.4 SD = .36 vs. M = 1.2 SD = .19), t(63) = 3.3, p = .002, Cohen’s d = .83; and (e) worries about family in the home country (M = 1.4 SD = .33 vs. M = 1.17, SD = .18), t(63) = 3.42, p = .001, Cohen’s d = .86. PMLD reported by participants with higher anxiety symptom scores were (a) difficulties in adjustment and coping with culture (M = 1.5, SD = .27 vs. M = 1.2, SD = .29), t(63)2.6, p = .009, Cohen’s d = .65; (b) loneliness and boredom (M = 1.3, SD = .33 vs. M = 1.2, SD = .23), t(63) = 2.4, p = .019, Cohen’s d = .60; and (c) worries about family in the home country (M = 1.3, SD = .33 vs. M = 1.1, SD = .18), t(63) = 2.05, p = .044, Cohen’s d = .51.
Two linear regression models were tested for anxiety and depression symptoms as dependent variables and post-migration difficulties as independent variable (Table 3). The first model explained 37.5% of variance of depression symptoms and was significant (p < .001). The significant predictors were difficulties in adjustment and coping with culture, ethnic discrimination and worries about family in the home country. The second model explained 14.9% of anxiety symptoms variance and was significant (p = .001). The significant predictors were difficulties in adjustment and coping with culture and the number of traumatic events.
Linear regression analyses of anxiety and depression symptoms for the total sample.
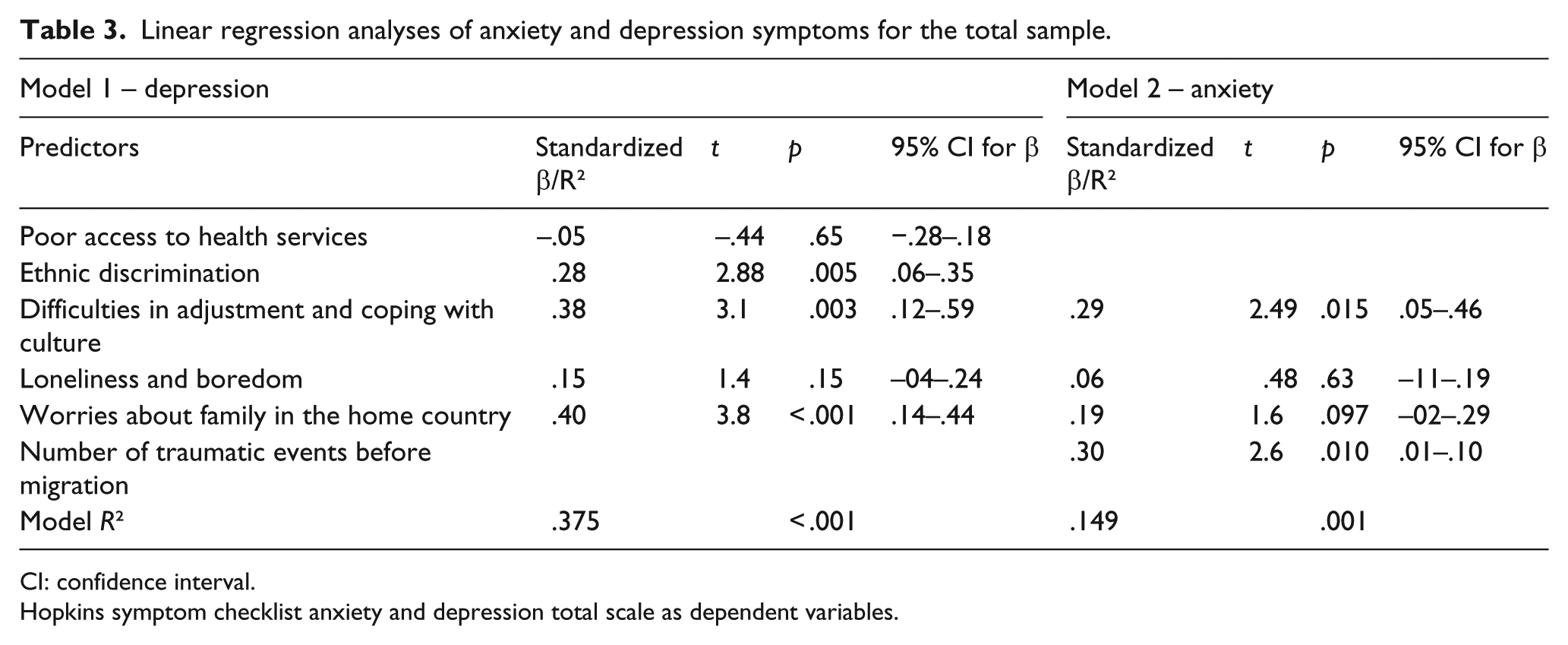
CI: confidence interval.
Hopkins symptom checklist anxiety and depression total scale as dependent variables.
Discussion
The main objective of this study was to investigate PTSD prevalence and associated factors in Haitian immigrants in southern Brazil. Full PTSD diagnosis according to DSM-5 criteria was found in 9% of the sample. In the overall sample, intrusion was the most prevalent cluster and negative alterations in cognitions and mood was the least prevalent. Factors associated with severity of PTSD symptoms were the impossibility of returning home in an emergency, being victim of ethnic discrimination, difficulties adapting to the new culture and higher number of traumatic events.
The 2010 earthquake in Haiti was the most prevalent traumatic event in this sample. Two studies conducted in Haiti 4 and 30 months after the earthquake estimated a PTSD prevalence of 24.5% according to the DSM-IV-TR criteria and 36.75% of severe PTSD symptoms according to the Impact of EventsScale – Revised (Cénat & Derivois, 2014; Cerdá et al., 2013). In Brazil, a 12-month prevalence of 5% and 3% was found in the general population of Rio de Janeiro and São Paulo (Ribeiro et al., 2013). The PTSD rates found in our study are, therefore, higher than those found in Brazil but lower than in Haiti. However, this comparison should be carefully analyzed, because our data collection took place 60 months following the earthquake and a part of the sample was not exposed to the event. This study design does not allow for a comprehensive investigation of the immigrant paradox, for we do not provide a proper comparison with nationals from Brazil and Haiti. However, our findings show that even with high rates of exposure to traumatic events, participants presented low PTSD symptom severity.
Prevalence of diagnostic criteria specific to each PTSD cluster differed in our sample, what may be explained through several perspectives. First, it should be noted that the most prevalent trauma type in our sample was experiencing a natural disaster, and it is known that the type of event may influence PTSD presentation (Smith, Summers, Dillon, & Cougle, 2016). Specifically, intentional interpersonal events (that involve deliberate infliction of harm) may be associated with worse outcomes than non-intentional ones. The course of PTSD differs in both types of events: PTSD symptoms increase over time in victims of intentional events and decrease in victims of non-intentional events (Santiago et al., 2013). A second explanation regards the sample’s cultural background. The DSM-orientated scales may be insufficiently sensitive to evaluate certain PTSD symptoms. Different prevalence rates and internal consistency between clusters were also found in the study of Norris et al. (2009), with Vietnamese immigrants exposed to the Hurricane Katrina. Participants reported less symptoms in Cluster C (avoidance/DSM- (4th ed.; DSM-IV); APA, 1994), and the Cronbach’s alpha was also low (.55).
Sociodemographic variables such as age, time as a migrant, sex and education are recurrently associated with PTSD in migrants (Breslau et al., 2011; Carrer et al., 2011; Meeske et al., 2013; Norris et al., 2009). In this study, sociodemographic variables were not associated with PTSD symptomatology or diagnosis. This may be due to the homogeneity of the sample concerning sociodemographic characteristics. Furthermore, the sample size and the convenience sampling strategy may have biased the sociodemographic data. The variable of time spent in the host country needs extra attention, for it has been presented in the literature as importantly – and positively – associated with mental health problems when the immigrant faces PMLD (Breslau et al., 2007; Breslau, Borges, Hagar, Tancredi, & Gilman, 2009; Rasmussen et al., 2012). This may have biased the results of this study, given that the longest time since migration in our sample was 4 years. Haitian migration in Brazil is a very recent phenomenon when compared to other countries (de Bocanegra et al., 2006; Norris et al., 2009).
Considering the lower number of traumatic events reported after migration in this study, it is possible to hypothesize that PTSD symptoms were already present before migration. However, PTSD model showed that the PMLD also explained part of PTSD severity, even with our sample being formed by recent migrants. Studies hypothesize that exposure to stressors such as acculturation problems, discrimination and lack of social support may explain the increase over time in the risk of mental health problems (Breslau et al., 2007; Rasmussen et al., 2012).
The results point to the relevance of the relationship between acculturation and mental health, as the variable ‘difficulties in adjustment and coping with culture’ was significant in the models of PTSD, anxiety and depression. Early acculturation problems related to adjustment and cultural discrepancies are expected to decrease over time (Berry, 2006; Ward, 1996). However, other associations found in this study may lead to a less optimistic course for mental health issues.
The impossibility of returning home in an emergency, worries about family in the home country and ethnic discrimination were related to PTSD, anxiety and depression. Only 24.2% of participants were living with their family in Brazil, and most of them provided financial support to those who stayed in the home country. In Brazil, however, they found several difficulties, including ethnic discrimination, which may increase the lack of social support. The experience of acculturation without a proper social support in Brazil may lead to mental health burdens, especially when previous traumatic experiences exist (Abebe, Lien, & Hjelde, 2012; Kirmayer et al., 2011). On the other hand, regarding the social erosion perspective of social support, it is possible that the process of acculturation in Brazil was influenced by mental health problems that were present before migration, which may also have impaired the ability to find new sources of social support (Shallcross, Arbisi, Polusny, Kramer, & Erbes, 2016).
To our knowledge, this is the first study addressing the prevalence and associated factors of mental health problems in Haitian migrants in Brazil, as well as one of the few to explore associations between migration and mental health in Brazil (Kang et al., 2009). The economical background of the host country also plays a role in the mental health status of migrants. Thus, studies of migration in developing countries add important information to the literature (Lindert et al., 2009). Strengths of this study include the control of traumatic and stressful events before, during and after migration, allowing to specify the impact of each stage of migration on mental health. Furthermore, methodological considerations were taken to reduce bias such as adapting the language of the interviews.
This study has, however, several limitations. There are fewer Haitian migrants in southern Brazil than in other countries (e.g. the United States or European countries), which may have influenced the sample size of the study. Furthermore, the sample may be unrepresentative of this population because it was selected by convenience. This study was conducted in a Brazilian region which is not the main destination of Haitian immigrants in Brazil (e.g. Acre and São Paulo). Thus, its data may be unrepresentative of the reality of Haitian migrants in Brazil as a whole. As discussed previously, the validity of DSM-based diagnoses in populations outside of Europe and North America is still controversial, and utilizing scales based on this diagnostic manual may have biased our results. The lack of data concerning PTSD prevalence in southern Brazil and in Haiti hindered the examination of the immigrant paradox. Studies with data collection in Haiti and Brazil may also add to the current knowledge about the effect of migration in this population.
Considering that Haitian migration to southern Brazil is recent, some actions in different levels should be taken to improve the acculturation process. First, health and social workers should be trained in intercultural abilities to offer proper assistance to the migrant population. Furthermore, public policies aiming to inform the Brazilian general population about migration may improve receptiveness, raising the probability of a better outcome of migration to the mental health of migrants.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq/Brazil) [grants number 312121/2015-6 and 421640/2016-2].