
Abstract
Background:
A better understanding is needed about how people make decisions about help seeking.
Materials:
Focus group and individual interviews with patients, carers, healthcare staff, religious authorities, traditional healers and community members.
Discussion:
Four stages of help seeking were identified: (1) noticing symptoms and initial labelling, (2) collective decision-making, (3) spiritual diagnoses and treatment and (4) psychiatric diagnosis and treatment.
Conclusion:
Spiritual diagnoses have the advantage of being less stigmatising, giving meaning to symptoms, and were seen to offer hope of cure rather than just symptom control. Patients and carers need help to integrate different explanatory models into a meaningful whole.
Keywords
Introduction
The reactions to psychological symptoms can have a significant effect on the outcome, for example, critical or hostile reactions from family members (Butzlaff & Hooley, 1998), stigmatising reactions from society or receiving medical treatment late, all leading to less favourable outcomes in psychosis (Barnes et al., 2008; Farooq, Large, Nielssen, & Waheed, 2009; Perkins, Gu, Boteva, & Lieberman, 2005). Understanding reactions to fpsychological symptoms is important if we wish to improve outcomes, but most research on pathways to care is based in higher income countries and Western societies (Anderson, Fuhrer, & Malla, 2010). Goldberg and Huxley’s model describes how patients go through various ‘filters’ in order to reach care, including community help, primary care and secondary mental health services (Goldberg & Huxley, 1992). In cultures where people have strong religious beliefs, supernatural explanatory models are common and traditional or religious healing is a large part of the response (Fung & Wong, 2007; Murdock, Wilson, & Frederick, 1978; Patel, 1995). Although there are several quantitative studies looking at pathways to care, there are few qualitative studies from these societies looking at how treatment decisions are made (Boydell, Stasiulis, Volpe, & Gladstone, 2010).
Sabah is one of the East Malaysian states on the island of Borneo. The population is mainly Muslim or Christian, but many people have prominent animist/pagan beliefs as well. The health services in Sabah are under-resourced, with the psychiatric services under particular strain (Yoon, 2010). Most psychiatric disorders are not treated or treated very late, with one study in health clinics in the capital Kota Kinabalu showing that over 90% of people with mental illness in primary care clinics are not diagnosed or treated (Abdullah, Minas, Meadows, & Kumaraswamy, 2011). The psychiatric system mainly treats psychotic illness. Depression and anxiety are rarely treated, mainly because symptoms of these disorders are normalised (Shoesmith & Pang, 2016). In Malaysia, religious authorities and bomoh (traditional healers) are a large component of the response to mental disorder (Crabtree, 2005; Phang, Marhani, & Salina, 2010; Razali & Najib, 2000). Bomoh are traditionally believed to have supernatural powers and are found all over Indonesia, Malaysia and Brunei (Kumaraswamy, 2007; Osman, 1972). The duration of untreated psychosis in Malaysia is more than 2 years (Salina Abdul Aziz, 2005) and part of the reason was believed to be that people seek traditional or spiritual help before they seek medical help (Razali & Najib, 2000). However, recent studies have shown that the duration of untreated psychosis is not significantly different for patients who seek traditional treatment first, and that traditional healers are frequently advising patients to seek treatment in the hospital (Phang, Midin, & Abdul, 2010).
Psychological symptoms are responded to by several different systems (e.g. the family, the village, the traditional healthcare system, the psychiatric system), and we need to better understand how these systems interact with each other in order to improve collaboration and access to evidence-based healthcare. We also need a better understanding of how patients, families and communities make the decision about which system to use for help seeking.
Methods
This study was part of an action research study, directed towards finding ways of improving collaboration across the different systems. Semi-structured individual and group interviews were conducted in Bahasa Malaysia and English in 2013, with interviews lasting between 30 minutes and 2 hours. Participants were selected using a mixture of purposive and theoretical sampling. Interviews were recorded and transcribed. Preliminary analysis was conducted during the period that the interviews were taking place, and emerging themes explored in subsequent interviews. The interviews were analysed in their original language using NVivo software with a grounded theory approach (Glaser & Strauss, 1967; Urquhart, 2012). Highly detailed codes reflecting all possible meanings were generated first, before higher order codes were created. Reflexivity was built into the process by having two people with different cultural and professional backgrounds coding together (author 1: psychiatrist and author 2: linguist), having regular discussions with other researchers, using memos and a reflective diary. A third researcher (author 3: anthropologist) read the relevant sections of the manuscripts and assessed the appropriateness of the codes. Findings were presented and discussed by a committee consisting of staff, patients and carers, which provided a form of member checking. The study was approved by the Ministry of Health ethics committee and all participants gave written informed consent.
Results
A total of 130 people were interviewed in 27 individual interviews and 26 focus groups of two or more people. This included 62 mental healthcare staff, 20 patients, 11 family members, 8 village heads, 5 school and college counsellors, 5 primary healthcare staff, 5 district hospital staff, 4 members of non-governmental organizations (NGOs) and 7 religious authorities and 3 bomoh (traditional healers). First episodes of mental illness were described by all groups of respondents, with staff and community members describing episodes in several people. Nearly all descriptions from patients, carers and staff were of psychotic illness.
The typical pathway to psychiatric services involves four steps (see Table 1), although these four steps were not followed in all cases. Steps were sometimes missed or not followed in a linear order.
Stages in pathway to psychiatric treatment.
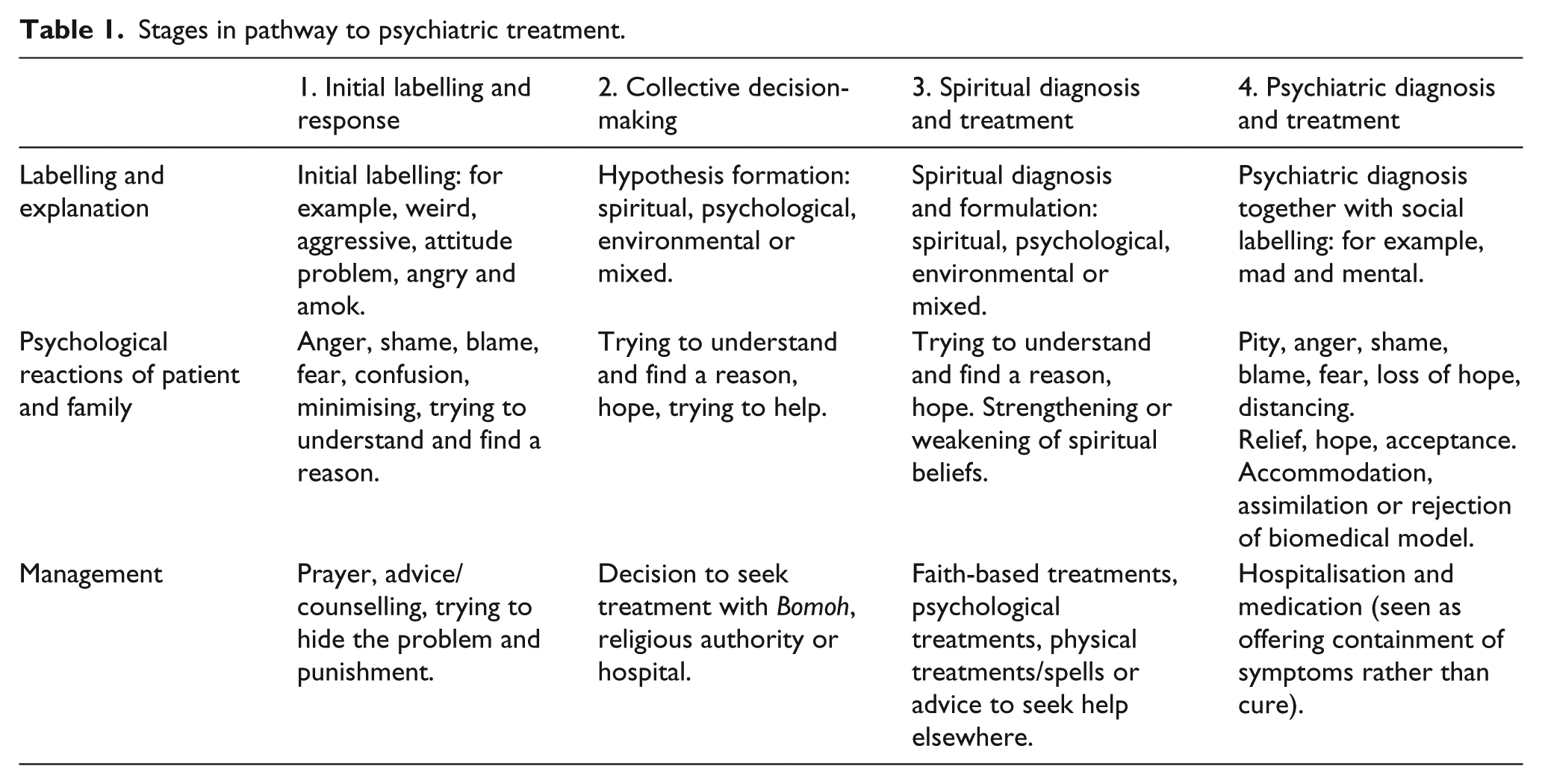
Initial labelling and response
The symptoms of mental disorder described by participants were nearly all external phenomena, such as changes in behaviour. The most common changes were anger, violence against others and hearing voices. These symptoms were noticed by people around the patient, rather than the patients themselves in nearly all accounts. The families were the first to respond to the change. The first response included labelling the problem as abnormal, for example, ‘attitude problem’, ‘lazy’, ‘aggressive’ and ‘weird’. Patients and families described a number of emotional reactions when the patient started to behave abnormally, which were predominantly anger, shame and fear. Initial management strategies included prayer, advice, trying to find a reason, trying to hide the problem, attempts to control the person and punishment: Maybe because she was being beaten by the family she felt stressed by them. She was beaten when she fought back. She was different to other girls, she didn’t want to do housework, didn’t wash her clothes and that was what made my mother angry. (Carer 1, Brother of patient)
Community participants also gave accounts of people with symptoms of common mental disorders such as anxiety and depression, but they did not label these as ‘mental disorder’: I do not have any mental disorder student because in school we just focus about their motivation, problem of learning, discipline, social problems and drug taking or smoking. (School counsellor 4)
These symptoms were managed by patients, families, schools and communities using the initial management strategies described above. They did not proceed to the next stage of help seeking if the symptoms were contained.
Collective decision-making regarding what is causing the problem and what should be done
Respondents described family discussions, during which hypotheses were formed about what was causing the problem and a decision taken about what to do. The family and others around the patient attempt to find a reason for the problem. This discussion may include extended family or people such as village leaders: Before this we didn’t discuss..but after this her own family members noticed and felt it was weird … her changes.. her way of talking.. then we discussed with her family. (Carer 7)
Explanations for symptoms at this stage were mainly psychological (e.g. too much thinking), spiritual or environmental in nature. Sometimes all elements are in the explanation (e.g. relationship problems lead to mental weakness, which allowed spiritual attack): Regarding mental illness, there are two types of mental illness. The first type is stress. The second is where a curse is put on someone and we can see they are truly sick. (Village head 2)
The family has to make a decision about where to seek help. In most cases the family decided to rule out spiritual causes first. Family members and patients sometimes described feeling pressured by other family members to try treatments from the bomoh first, even if they did not believe in them. Scepticism towards bomoh was seen in most hospital staff, and many patients and carers. Some believed in spiritual causes, but saw mystical healing from bomoh as a form of heresy or felt afraid of it: Maybe she got possessed or something else, such as a curse. But I wasn’t brave enough to get mixed up with these things. Because this type of illness, when they get it, sometimes he gets … how to explain … sometimes it gets worse. (Carer 8, Husband of patient)
In contrast, uncertainty of religious authorities was not expressed and respondents (including hospital staff) appeared confident in their explanations and were satisfied with their treatments.
In most cases, the hospital is seen as the last resort, after other options have been tried. Reasons for this was the community perception of the hospital, which was described by one school counsellor as ‘like a jail for crazy people’. The hospital was seen as a repository where the patients were held without any hope of treatment. Some patients described how they were surprised when they came to the hospital that offered treatment: Patient 2: I thought [the hospital] is a place for mad people. I didn’t know that you could get treatment here. No-one told me. Pastor 2: I mean psychiatry in this country has not been well developed. And the mental hospital is viewed as a one way ticket, like you go in there and you get locked up forever.
This was sometimes based on experience of people they know who went to the hospital and did not get cured: It is proven that a lot of cases that we refer to the doctors are not fully cured, so in the end it will be advised to meet with us. (Bomoh 3)
Spiritual diagnosis and treatment
Most patients and carers reported going to Bomoh or religious authorities for spiritual diagnosis and treatment.
Spiritual diagnosis
Bomoh and religious authorities described a diagnostic process, parallel to the diagnostic process used in medicine. They take a history and formulate an aetiology, which is based on the likely precipitants for the illness. These precipitants include issues in relationships, emotional issues and spiritual issues. Bomoh and religious authorities differed in the degree to which they believed that behavioural and psychological symptoms can be attributed to spiritual problems. Some believed that nearly all behavioural and psychological symptoms are spiritual in nature. Some had integrated different explanations, for example, using biomedical language, but attributing spiritual causes: So they hear voices that others can’t hear, in the language of the hospital it is schizophrenia. But there are two categories: the first one is the Jin (a kind of spirit) inhabiting the body through a medium using a curse, the second is the Jin inhabiting the body without us realising it. (Ustaz, Islamic religious teacher)
Some respondents distinguished between spiritual problems and mental disorders and some distinguished psychological problems as a separate category. Ways that they distinguished a mental disorder from a spiritual diagnosis included the voice or appearance changing, the person becoming stronger, fainting or unusual movements, such as the person acting like an animal. If the problem is spiritual, the patient will react when prayers or holy texts are read: For example, when I ask the person to say the prayer, if the person with no problem, he says the prayer, then it is not a possession. Because normally the spirit will not allow the person to say the prayer. (Pastor 1)
Spiritual diagnoses included saka (spiritual inheritance), curses and heresy. Saka was mainly described by Islamic respondents and is where someone befriends or makes a deal with a spirit, who has possessed them. When the person dies, the spirit is passed onto their descendants. The background history is important for spiritual diagnosis, in that someone with a spiritual problem may have a history of not practising the religion appropriately, practising black magic, failing to keep an agreement with a Jin, having conflict with someone who may be responsible for a curse or having an ancestor who also had a saka.
Spiritual treatment
Treatments from religious authorities normally included reading a Holy Text or prayer, which may be specific to the diagnosis. The patient was sometimes advised to change his or her lifestyle to avoid future attack. Faith in God is seen as important to recovery. Treatment sometimes involved psychological elements, such as counselling: Patient 18: … they pray according to the illness. Like for me, I have a mental illness, they have a special prayer for it. Patient 4: Because I trust her [the Catholic sister] to keep secrets, to not talk outside. If it was my mother she would get angry with me. But talking to the sister, she listens more and I can talk about whatever is troubling me.
Treatments from bomoh also normally included reading holy texts and prayers. Bomoh that provide services with elements in line with holy texts were more likely to be seen as legitimate by Muslim respondents. Treatment from bomoh also included spells and physical elements, such as sprinkling water, pulling or pushing or slapping parts of the body and removing objects (e.g. needles, eggs) from the body. They sometimes asked the client to drink things (e.g. special water, a lime and onion mixture).
If the treatment was not effective, some bomoh and religious authorities advised the patient to seek treatment from another religious or spiritual healer with more specialised knowledge in spiritual disturbance or from psychiatric services: After meeting [the bomoh] then they told me to get the treatment here in [the hospital]. (Patient 1)
Others treated the illness for many years: Yes for cure it can take many years, and until now there are people who have not been cured yet. The reason is that Saka is slow to be cured. Saka is hereditary, dangerous and hard to become normal again. (Imam)
Psychiatric diagnosis and treatment
Sending the patient to the hospital usually happened during a crisis. Families generally sent patients to the hospital directly, sometimes with police assistance, but usually bypassing primary care. One of the main factors that appeared to influence sending to the hospital was contact with someone who worked in the health services: It was like I couldn’t stand it because I couldn’t control her. My daughter was in the house for three days, three nights. Every door was locked. I can’t let her go out. I can’t sleep any more. She couldn’t sleep. She slept for a while and when she awoke, she started throwing things. After that … she was possessed … so I called the Church. They came to persuade her and there is one hospital worker, related to the church, who said it is better to go to the hospital. (Carer 8, Mother of patient)
After attending psychiatric treatment, decisions still needed to be made about whether to take biomedical treatment when in the community. Decisions about whether to follow medical advice was sometimes collective, going back to steps two or three.
For me, before I make any decision, whatever the doctor’s advice is, I will meet with my closest family and ask for opinion or permission.. if they say OK I will follow. Because in the village I will meet with the village head.. family, then village head. (Carer 9, Husband of patient)
Patients and carers rarely gave biological explanations and retained spiritual explanations after psychiatric diagnosis. Some patients and carers gave several different explanations for the illness, either assimilating the explanations or accommodating them without any integration or assimilation: When she is stressed or depressed, her spirit is weak, and that is when the bad spirits can enter. (Assimilation of explanations; Carer 8, Mother of patient)
Some patients fully rejected biomedical explanations, but still attended hospital appointments. Patients and carers were more likely to use social labels, such as ‘mad’ than biomedical labels, such as schizophrenia. Some patients described themselves as ‘mad’, Others used these terms to describe other patients in the hospital, from whom they differentiated themselves. The way that they differentiated themselves from the other ‘mad’ people in the hospital was by showing that their illness was explainable, not permanent or severe. The label of madness was normally applied when the decision is made to bring them to the hospital. ‘Mental’ was used as a synonym for madness, and also had connotations of permanence, being unexplainable and severe.
Discussion
The pathways to care in this study were different from pathways to care in studies from Western societies. Primary care was absent for most people interviewed, with decisions being made collectively, and spiritual diagnosis and treatment are a significant part of the response to mental illness. The subjects interviewed in this study had a range of beliefs about illness. The decision about which system of care to use is determined by beliefs about the cause of illness, beliefs about the acceptability and perceived efficacy of treatment options and potential stigmatising effect that any label might have. It was not only the patient’s beliefs but also the beliefs of their family and community that led to treatment-seeking decisions. The spiritual explanations are generally preferred over the biomedical explanations, and seeking help from psychiatric services is the last resort. Kleinman (1980) described five processes which are performed by health systems, including lay and traditional healthcare systems as follows: (1) social construction of the illness experience, (2) establishment of general criteria to guide help seeking, (3) managing specific illness episodes through labelling and explaining, (4) healing activities and (5) management of outcomes, including management of chronic illness, or treatment failure. The first three functions were all performed more by the spiritual system of care than by the biomedical system. For some respondents, the fourth function, healing, is performed only by the alternative and religious healers. The psychiatric system is only performing the fifth function, that is, managing the symptoms after the real healing activity has failed.
It is clear from the interviews that the label of mental disorder is more stigmatising than the spiritual explanations. Attribution theory (Weiner, 1980, 2014) helps to give some explanation for this. Attribution theory describes how searching for cause and meaning behind events is a fundamental part of human behaviour and influences motivation for action. Attribution theory gives three dimensions which affect the way illnesses are stigmatised (Corrigan, 2000): locus, control and causal stability. Locus is whether the problem is in the person himself or herself, or something external to the person. Spiritual explanations have a more external locus, in that the problem is not the within the person himself or herself, but the spirit. Control is about whether the person can control the illness or is to blame. The perception of control for both mental disorders and spiritual disorders varies between respondents and different diagnoses. For example, the patient is not normally seen as being responsible for saka or curses, but is to blame if the cause is heresy. Causal stability is about whether the problem will persist or improve. Spiritual causes were mainly seen as something that could be recovered from. In contrast, mental illness was seen as a ‘one-way street’ that cannot be recovered from. Initial labels (e.g. lazy) were also more stigmatising than spiritual labels, in that they normally had an internal locus and control and described enduring personality traits.
Some subjects simultaneously held a mixture of biomedical, psychological and spiritual illness beliefs. Patients and carers sometimes had spiritual beliefs about causation, but were still receiving biomedical treatment. Spiritual and religious healers were also assimilating spiritual with biomedical beliefs, and many said they referred to health services. Good (1977) described how patients and families used a network of semantic systems to label and explain symptoms. These systems are often conflicting and contradictory, but when faced with symptoms most people pragmatically use whatever explanatory system gives rise to relevant treatment options. Osman described similar conflicts in Malay culture, between pre-Islamic, Islamic and modern scientific belief systems (Osman, 1972). This study also shows these conflicts when the decision is made to seek help from the bomoh, the religious authorities or the hospital.
If mainstream evidence-based medical practitioners wish to collaborate with religious and alternative healers, we need to understand who they are treating. From the descriptions given by religious and alternative healers, many of the people who they heal have symptoms that are not typical of psychotic illness or other mental disorders. If we were to use a psychiatric label for this group, it would most likely be dissociative disorder. Religious authorities are also likely to be treating people with common mental disorders (such as anxiety and depression), through faith based and psychological treatments. The people who are diagnosed as saka may have some overlap with schizophrenia. Hearing voices is one of the main symptoms, and it is clear from the descriptions that it is considered to be chronic, requiring many years to heal. Working with religious authorities and alternative healers may allow this group to be treated earlier.
Further study is needed to better understand the outcomes of people who were given spiritual diagnosis rather than psychiatric diagnosis. Significant improvements in symptoms in patients treated by spiritual healers have been observed in other settings (Sorketti, Zainal, & Habil, 2013). The spiritual explanatory models have some clear advantages in that the stigma is less and so they are accepted by the people around them. The spiritual treatments are perceived as offering cure, rather than just offering symptom control. They give meaning to symptoms, which is now accepted as one of the most important aspects of recovery from illness (Andresen, Caputi, & Oades, 2006; Romano, McCay, Goering, Boydell, & Zipursky, 2010). When the symptoms are understandable and not seen as permanent, patients are able to differentiate themselves from the label of madness. However, the biomedical models mean that medication and other evidence-based treatments are given.
Limitations
The study did not use systematic sampling, so no conclusions can be drawn on the proportion of patients choosing each pathway to care.
Conclusion
Healthcare providers need to be aware of the deficits of the illness models that that they are using and understand how other healthcare systems can fill those holes. Biomedical models fail to perform some of the essential functions needed by a healthcare system, particularly failing to provide meaningful and acceptable labels and explanations. Patients need help to integrate their different systems of understanding to construct labels and explanations that are meaningful and acceptable to them. Integrating biomedical elements into their existing explanatory models in a meaningful way will increase the chance of them taking medication and other evidence-based treatments. Meaning-making needs to be a central component of healthcare provision, and working with practitioners from other systems of care will allow us to do this better.
Footnotes
Acknowledgements
We would like to thank the Director General of Health, Malaysia, for permission to publish this article. We would like to thank all of the participants of this study.
Author’s note
Author Dawn Forman is also affiliated to College of Health and Social Care, University of Derby.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by a grant from the National Institute of Health NMRR-13-30814792.