
Abstract
Background and aims:
Married immigrant women in South Korea undergo a wide array of psychosocial challenges in the process of adapting to a new culture and marriage with a Korean husband. For an integrative understanding of women’s mental health status and to determine the key risk and protective factors, we systematically reviewed empirical articles about the mental health of married immigrant women.
Methods:
We searched and reviewed articles from nine online databases: PubMed, Scopus, PsycINFO, Embase, DBpia, KISS, KMbase, KoreaMed and RISS, which were published up until January 2017. We identified 38 quantitative studies that examined psychiatric symptoms and pertinent factors for this population.
Results:
The relative risks of psychiatric symptoms among married immigrant women varied across diverse samples. We summarized the associated factors existing prior to and after marriage migration that may moderate their mental health consequences. We identified five key risk factors: acculturative stress, country of origin, family stress, domestic violence and extended family structure, and two protective factors: social support and marriage satisfaction, which were consistently supported by the included studies.
Conclusion:
With the paucity of prospective studies, longitudinal research is needed that addresses the long-term processes of married immigrant women’s psychological adaptation and the underlying risk and protective factors at diverse settlement phases. Furthermore, we suggest that future research should focus on how women’s personal attributes interact with macro-level, socio-cultural contexts, including familial relationship and the community social-support system. Future evidence-based policy and interventions should comprehensively address married immigrant women’s socio-cultural, economic and mental health needs.
Keywords
Introduction
International marriage is a growing trend in East and Southeast Asia, largely affecting the country’s demography, and South Korea is one of the countries that experience the dramatic changes, along with Taiwan, Singapore and Japan (Jones & Shen, 2008). The population of multicultural families has been rising steadily in South Korea, with a surge of marriage migration of foreign brides (Ministry of Gender Equality and Family, 2016). This increase was especially spurred by a Korean version of transnational brokered marriage, which is often referred to as the ‘mail-order bride industry’ with a negative connotation (D’Aoust, 2009). It has become a worldwide phenomenon: matchmaking men from more developed countries, such as the United States, Canada and Europe, and women from relatively poor countries in Southeastern Asia, Eastern Europe and South America (Asia Pacific Mission for Migrants, 2007; Yakushko & Rajan, 2017). In Korea, it was originally initiated by local governments and associations, with ‘Rural Bachelors Matching Drives (Kim, Yang, & Torneo, 2012)’, aimed at matching unmarried, rural Korean men with ethnic Korean women in China (Joseonjok). Since then, the private marriage brokerage industry has thrived to profit by matching Korean men and foreign brides from other developing countries. This meets the needs of both Korean men, who are marginalized from the domestic marriage market, and foreign women, who wish to pursue better economic conditions (H. Kim, 2011). A high proportion of married immigrant women (MIW) in Korea are from China and developing countries in Southeast Asia such as Vietnam and the Philippines (Statistics Korea, 2015).
Similar to the MIW in other countries who are exposed to multiple social risks, including domestic violence and social isolation (Belleau, 2003; Noda, 1998; Raj & Silverman, 2002; Shu, Chuang, Lin, & Liu, 2008; Yang & Wang, 2003), in contrast to their initial expectations of better life conditions, MIW in Korea often face a wide range of psycho-social challenges, including adapting to a new culture and married life. Acculturation process can be a mental health risk (Hunt, Schneider, & Comer, 2004). Eighty-five percent of MIW reported subjective difficulties in adapting to life in Korea, including language difficulties and a sense of isolation (Ministry of Gender Equality and Family, 2016). Particularly, in Korea, where cultural and ethnic homogeneity is emphasized (Han, 2007), MIW are exposed to extensive social discrimination and exclusion (Ministry of Gender Equality and Family, 2016).
Adjustment to marriage is another major challenge. MIW are susceptible to marital distress due to conflicts with their spouse and family-in-law, domestic violence experience and spouses’ alcohol problems (An, Park, & Choi, 2010; Choi & Byoun, 2014; Choi, Kim-Goh, & Yoon, 2013) and often experience gender inequality in their marriage because of spouses’ conservative patriarchal view of women’s roles and behaviours (I. Lim, 1997). In addition, higher proportions of MIW experience socio-economic difficulties in comparison to native Korean women, including low family income (Jo, Yeon, Han, Ryu, & Lee, 2012). These social disadvantages may place them at an elevated risk for mental health problems.
To date, studies have explored the associated variables of MIW’s mental health outcomes; however, to our knowledge, there has not been a review study that synthesizes the existing findings into an integrative understanding of key risk and protective factors of MIW’s psychiatric symptoms. Therefore, this review study integrated the existing literature about the epidemiology of psychiatric problems among MIW in South Korea and their risk and protective factors. Specifically, we summarized the findings by adopting a modified form of the acculturation framework of Berry (1992, 1997; see Figure 1), which presents the associations of mental health problems with challenges arising from marriage migration (i.e. acculturation and adaptation to married life) and the moderating factors that exist prior to and arise after marriage migration. Then, we identified the key risk and protective factors that were consistently supported.

Methods
Article selection
We included quantitative studies examining mental health of MIW in South Korea with a minimum sample size of 25 participants. Articles that did not examine psychiatric outcomes were excluded (e.g. studies on physical health, general adaptation or life satisfaction).
English or Korean language articles were systematically searched through nine online databases (international journals: Embase, PubMed, Scopus and Web of Science; Korean journals: DBpia, Research Information Sharing Service (RISS), Korean Studies Information Service System (KISS), KoreaMed and KMbase) for articles published up until January 2017. The following key search terms were used: MIW (married OR marriage OR wives) AND (immigrant OR migrant OR foreign) AND mental health (psychiatr* OR psycholog* OR mental OR psychosocial OR wellbeing OR adjustment OR adaptation OR protective factor OR risk factor OR vulnerability factor OR resilience OR emotion OR behaviour OR behaviour) AND Korea (Korea OR Korean). Initially, 981 articles were identified. After excluding duplicates and irrelevant articles by reviewing titles and abstracts, 38 articles were included in this review study (see Table 1 and Figure 2).
Included studies.

CES-D: Center for Epidemiological Studies-Depression Scale; EPDS: Edinburgh Postnatal Depression Scale; GHQ-20: General Health Questionnaire; SCL-90-R: Symptom Checklist-90-Revision; BDI: Beck Depression Inventory; BAI: Beck Anxiety Inventory; SSI: Scale for Suicide Ideation; SDS: Short-form Depression Scale; GDSSF-K: Geriatric Depression Scale Short Form-Korea; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders, 4th Edition; STAI: State-Trait Anxiety Inventory; K10: Kessler Psychological Distress Scale.
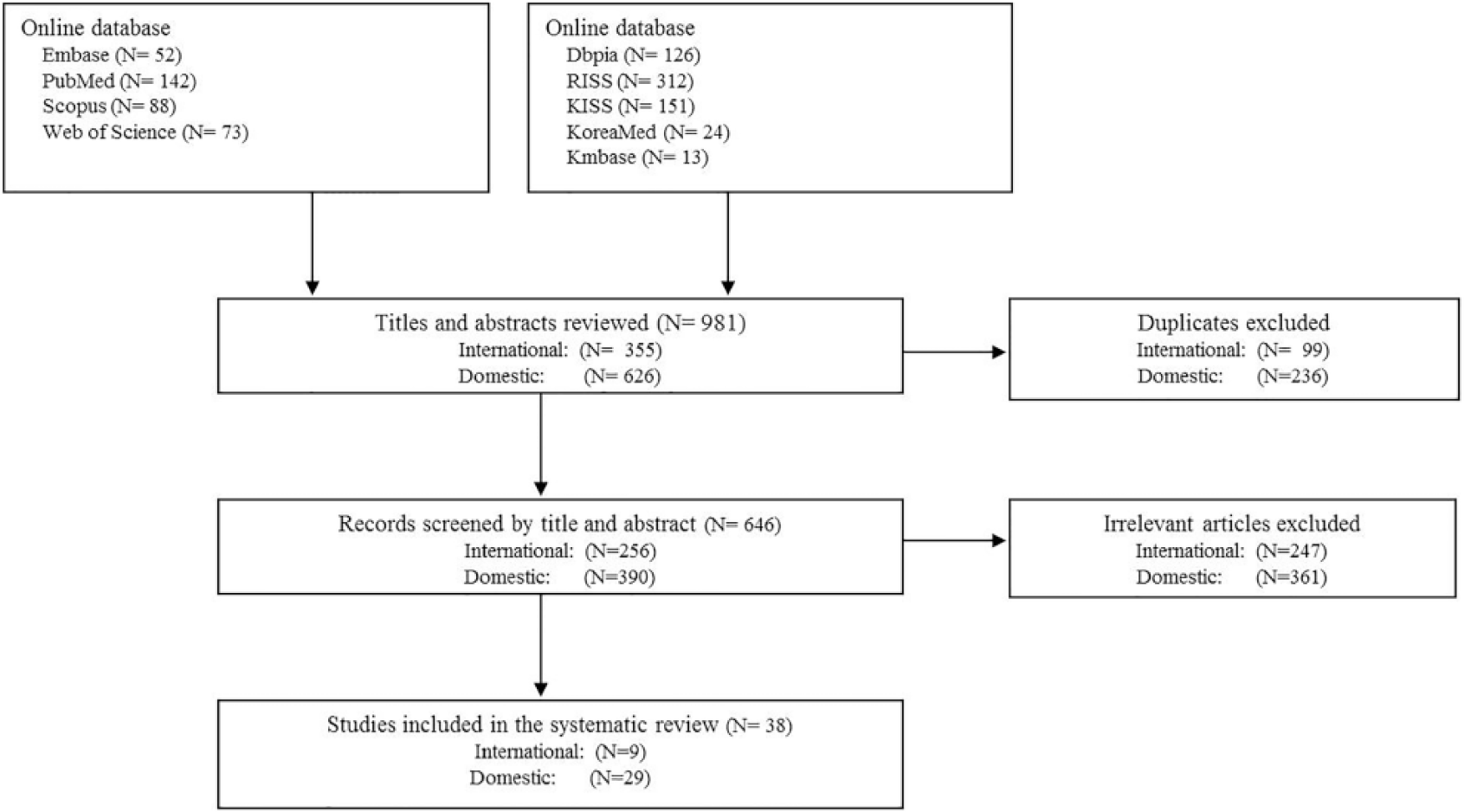
Search strategy and article selection process.
Results
The epidemiology of psychiatric symptoms
We found 10 studies that either compared the psychiatric symptoms between MIW and other female groups or reported the prevalence of their psychiatric symptoms with diagnostic criteria. The relative mental health risk in MIW was inconsistent in the existing evidence.
Among five case-control studies, four studies compared MIW with native Korean women and yielded mixed results. Specifically, in contrast to the findings of a higher level of postpartum depression (Choi, Kim, Ryu, Chang, & Park, 2012) and anxiety symptoms (Lee, Park, Hwang, Im, & Ahn, 2014) among MIW than native Korean women, other findings noted a relatively low prevalence of depression and anxiety (Jo, Yeon, Han, Ryu, & Lee, 2012) and a lower level of overall psychiatric symptoms (Park, Yong, & Hong, 2015) of MIW. In addition, no significant difference was noted in the prevalence of depression and anxiety between Vietnamese MIW in Korea and native Vietnamese women (Hong et al., 2013).
Five cross-sectional studies reported the prevalence of MIW’s psychiatric problems, notably depression. Using the Center for Epidemiological Studies-Depression Scale (CES-D), these studies reported the prevalence of depression with distinct cut-off scores: with 16 cut-off scores, 39.9% (Kim, Yang, Chee, Kwon, & An, 2015; Kim, Yang, Kwon, & Kim, 2011); with 21 cut-off scores, 9.2%– 26.9% (H. Kim & Kim, 2013; O. Yang & Kim, 2007); with 22 cut-off scores, 15.9% (Lee & Kim, 2011) of MIW were classified as depressed. In some findings (Kim et al., 2015, 2011), the prevalence in MIW (39.9%) was relatively high than the previously reported prevalence in the native Korean population (14.0%; Oh et al., 2013). However, due to the noteworthy variations in the prevalence reported across studies, the relative mental health risk of this population cannot be determined.
Interestingly, the heightened risk for more severe psychiatric symptoms was suggested in this population. For instance, the prevalence of mild depression with lower cut-off scores was similar to that of native Korean women, but the prevalence of severe depression with higher cut-off scores was particularly high (25 cut-off scores, 18.2%; 31 cut-off scores, 8.7%) in a report (O. Yang & Kim, 2007). Similarly, in another study (J. Lee & Kim, 2011), the prevalence of MIW’s mental disorders was lower than that of native Korean women with lower cut-off scores (t ≥ 63); however, with higher cut-off scores (t ≥ 70), the prevalence was higher in MIW. Mild psychiatric symptoms might not be particularly more prevalent in MIW; however, they may tend to be exacerbated with MIW’s lack of social resources (O. Yang & Kim, 2007).
The aforementioned variations in the findings of the relative risk for MIW’s psychiatric symptoms may reflect individual variations in psychological outcomes depending upon both situational and personal factors (Berry, 1997). Therefore, to target high-risk groups and to establish interventions that enhance protective factors for their mental health, the risk and protective factors that moderate the mental health consequences of their marriage migration should be understood.
Risk and protective factors
Challenges arising from marriage migration
Acculturation
The stress that MIW experience in the process of acculturation – acculturative stress (Berry, Kim, Minde, & Mok, 1987) – includes the stress from perceived social discrimination and exclusion, homesickness, fear and cultural shock due to change, and guilt about acculturation (Sandhu & Asrabadi, 1994). This acculturative stress is highly relevant to their overall mental health outcomes, including depression and anxiety symptoms (Choi & Park, 2016; Hyun & Kim, 2012; Im, 2010; Im, Lee, & Lee, 2014; Ji et al., 2012; Jo et al., 2012; Kim, Kim, Moon, Park, & Cho, 2013; Kim & Kim, 2013; Kim, 2011; Kim, 2007; Kweon & Park, 2007; Lee & Chu, 2012; Lim, Oh, & Han, 2009; Park et al., 2015; Yang & Kim, 2007). In one study (Lee & Chu, 2012), the predictive power of fear of change and cultural shock was particularly more robust than other sub-factors of acculturative stress in predicting anxiety symptoms. Perceived social discrimination – both the frequency of discrimination experience and the associated stress – also adversely influenced MIW’s psychological adaptation (Cho & Hyun, 2012; Ryu, 2016). Given that approximately 40% of MIW experience social discrimination, with more than three quarters being unable to cope with it (Ministry of Gender Equality and Family, 2016), MIW’s experience of social discrimination can aggravate their mental health problems. In a further study of Vietnamese MIW (Youn & Lee, 2010), marginalization – an acculturative strategy where immigrants fail in both retaining their home culture and accepting the host culture (Berry, 1997) – predicted somatization and depression symptoms. Further studies are needed to elucidate the causal pathways underlying its mental health effects and effective acculturative strategies.
The association between Korean language ability and mental health problems showed additional variations. Poor language ability was linked with psychological distress in several studies (Cho & Hyun, 2012; G. Chung & Lim, 2016; Kang, Kang, Park, & Son, 2016; Kim, Lim, & Jeong, 2013; Kim, 2007), but not in the other studies (Hyun & Kim, 2012; Im, 2010; Jo et al., 2012; Kim & Kim, 2013; Kim & Lee, 2010; Lee & Kim, 2010; Lee & Kim, 2011; Ryu, 2016; Yang & Kim, 2007). The inconsistent results may be due to the low specificity of the one-dimensional assessment of the Korean language used in these studies. When assessing language ability in four distinct domains – reading, listening, speaking and writing ability – only speaking ability predicted lower depression (J. Kim et al., 2011). The role of language proficiency may vary upon domain. In another study (S. Kim & Lee, 2010), language ability independently predicted socio-cultural adaptation, but not psychological adaptation. Taken together, MIW’s poor language ability may not be a consistent independent risk factor for psychiatric symptoms; however, language difficulty, notably poor speaking ability, may act as an obstacle to adapting to Korean culture.
Adaptation to married life
Successful adjustment to marriage and new family is another significant factor that impacts MIW’s mental health functioning. A satisfactory marriage with a Korean husband was linked to a decreased risk of mental health problems, including anxiety and depressive symptoms, in several studies (Choi et al., 2013; Chung & Han, 2009; Im et al., 2014; Kang et al., 2016; Kim, Kim, Moon, Park, & Cho, 2013; Lim et al., 2009; You & Kim, 2012). In contrast, marital conflicts predicted an increased risk of depression and somatization symptoms of Vietnamese immigrant women (You & Kim, 2012). In another study (Chung & Han, 2009), the consideration of divorce was the best predictive indicator for MIW’s depressive symptoms.
More specifically, MIW’s mental health outcomes were relevant to the perception of cultural gaps, emotional intimacy, and communication with their husbands (K. Chung & Han, 2009; K. Park & Jeong, 2011). Given the significant role of emotional communication with husbands in attenuating MIW’s depressive symptoms (Ji et al., 2012), intervention to enhance marital communication may be effective for both MIW’s marital and psychological adaptation.
Husbands’ problematic behaviours are also closely associated with MIW’s psychiatric symptoms. Husbands’ alcohol problems and domestic violence were strongly associated with MIW’s depressive symptoms (Choi et al., 2013; Im, 2010; Kim, 2011; Yang & Kim, 2007). Husbands’ oppressive behaviour, including controlling MIW’s finances or routines, was also predictive of their depressive symptoms (K. Chung & Han, 2009). Considering the higher prevalence of problematic alcohol consumption (H. Choi et al., 2013) and domestic violence in the husbands of MIW, including physical, sexual and verbal abuse (Choi & Byoun, 2014), clinical and policy attention is warranted.
In addition to marital distress, family-related stresses arising from parenting or conflicts with parents-in-law were reported. These family stresses were consistently related to MIW’s psychological distress, including the severity of diverse psychiatric symptoms and suicidal ideation (Im, 2010; Kang et al., 2016; Kang, 2013; Kweon & Park, 2007; S. Park et al., 2015; O. Yang & Kim, 2007).
Moderating factors prior to marriage migration
Country of origin
The prevalence or the levels of psychiatric symptoms in MIW varied by their country of origin in several studies (Choi & Park, 2016; Chung & Han, 2009; Kim et al., 2015, 2011; Kim, Lim, & Jeong, 2013; Lee, 2010; Lim et al., 2009), albeit not all (Kim et al., 2013; Park et al., 2015). Specifically, MIW from the Philippines and China reported higher levels of depression and anxiety symptoms, and, conversely, MIW from Japan reported a lower level of depressive symptoms than others (K. Chung & Han, 2009; J. Kim et al., 2015; Kim et al., 2011, 2013; Lee, 2010; Lim et al., 2009). Different mental health outcomes according to the country of origin may be due to the differential treatment of MIW in Korea according to their home country, such that those from developing countries may experience stronger social discrimination and stigma. Lower recognition level of home country in Korean society was associated with higher levels of MIW’s depressive symptoms in one study (H. Kim & Kim, 2013). The association between origin countries and depressive symptoms was attenuated or disappeared after controlling for such social variables as social-support and marital relationships (K. Chung & Han, 2009). This suggests that MIW’s differential psychiatric outcomes across countries of origins may be due to the different social status and support they acquire after migration, depending upon their home countries.
Educational background
The effect of educational background before immigration on MIW’s psychiatric symptoms is unclear – either having no effect (Choi et al., 2012; Chung & Han, 2009; Hyun & Kim, 2012; Jo et al., 2012; Kang et al., 2016; Kim et al., 2013; Kim & Kim, 2013; Kim, 2011; Kim et al., 2013; Lee & Kim, 2010; Lee & Kim, 2011; Lee, 2010; Park & Jeong, 2011; Park et al., 2015; Yang & Kim, 2007) or a protective effect (Choi & Park, 2016; Hong et al., 2013; Im, 2010; Im et al., 2014). With the mixed results, definitive conclusions cannot be drawn yet about the role of previous education in MIW’s psychological adaptation.
Moderating factors after marriage migration
Length of stay or marriage
The association between mental health outcomes and length of marriage or stay in Korea is unclear from existing findings. MIW in the initial phase of immigration or marriage reported higher levels of mental health problems in two studies (Im et al., 2014; O. Yang & Kim, 2007); however, contrastingly, in other studies (Hong et al., 2013; J. Kim et al., 2011; S. Park et al., 2015), those who stayed longer in Korea or marriage had higher levels of psychiatric symptoms. In other studies (O. Kim, 2007; S. Kim et al., 2013), MIW in middle-aged marriages had a higher level of depressive symptoms than those in younger or older marriages. In the remainder of the studies ( H.Choi et al., 2013; K. Chung & Han, 2009; Hyun & Kim, 2012; Im, 2010; Jo et al., 2012; Kang et al., 2016; Kang, 2013; Kim et al., 2013; Kim & Kim, 2013; Kim, 2011; Kim et al., 2013; Lee & Kim, 2011; Lim et al., 2009), no significant association with psychiatric symptoms was noted, particularly after controlling for such variables as acculturation, family stress and social support (O. Kim, 2007).
A further study noted that the length of stay in Korea was variably linked with each type of MIW’s stresses (Kweon & Park, 2007), in that those who stayed in Korea less than 3 years had a higher level of acculturation stress; however, those who stayed for 3–8 years had more family stress. The results may indicate that the length of stay in Korea or marriage does not directly predict psychiatric symptoms; however, MIW may encounter distinctive stressors across the distinct phases of acculturation that are potentially linked to mental health problems. Longitudinal studies addressing the trajectory of MIW’s psychological adaptation will contribute to the development of intervention strategies that help them to cope better with crucial difficulties at each settlement phase.
Family structure
A larger proportion of MIW have extended family than do native Korean women (S. Choi et al., 2012). The findings have shown variable effects of living with family-in-law or having children – either no effect or negative effect. No association was noted between psychiatric symptoms and having a child or the number of children in other studies (Choi et al., 2013; Jo et al., 2012; Kim et al., 2013; Kim et al., 2013; Lee & Kim, 2011; Lee, 2010; Yang & Kim, 2007), except for one study noting higher levels of somatization symptoms among MIW who had children (Im, 2010). In contrast, living with family-in-law appears to be a risk factor that increases family-related stress, thus increasing MIW’s mental health risks. Living with parents-in-law was associated with internalizing symptoms, including depression and anxiety (Jo et al., 2012; G. Kim et al., 2013; S. Kim et al., 2013). However, after controlling for other social variables such as family supports, no association was noted between extended family structure and depression (J. Kim et al., 2011; M. Lee, 2010). The results may imply that such protective factors as support from family members may compensate for the potential stresses that come from an extended family structure. Further studies that examine the qualitative relationships with other family members than husbands will provide a richer understanding of the role of new family members in MIW’s mental health.
Social support
Both the quantity and quality of support from diverse social relationships play a key role in attenuating MIW’s psychological distress (Hyun & Kim, 2012; Im, 2010; Im et al., 2014; Kang et al., 2016; Kim, 2011; Kim, 2011; Kim, 2007; Kim & Lee, 2010; Kweon & Park, 2007; Lee & Kim, 2010; Ryu, 2016; Yang & Kim, 2007). In a study of MIW in rural areas (O. Kim, 2007), having each support from one’s spouse, origin country friends, parents-in-law and social organizations independently predicted decreased depressive symptoms. Other findings noted a more key role of support from one’s spouse and family in comparison to other relationships with friends or neighbours, suggesting diverse levels of impact depending upon the relationship type (J. Kim et al., 2011; C. Lee & Kim, 2010). In a large study examining MIW’s social networks (M. Lee, 2010), not co-ethnic ties in Korea, but ties with Koreans had a significant association with their depressive symptoms, underscoring the significance of connection with Koreans, including their Korean family. Professional support from social workers and health professions, such as counselling and home services, was also associated with MIW’s decreased depressive and anxiety symptoms (Cho & Hyun, 2012; Jang & Lee, 2010). On the contrary, such negative aspect of relationships as perceived social conflict was linked to diverse psychiatric symptoms of Vietnamese MIW (J. Lee & Kim, 2011).
Social-economic status
Financial strain adversely influences MIW’s mental health outcomes. Self-reported low economic status and economic difficulty were consistently correlated with internalizing disorders such as depressive symptoms (G. Chung & Lim, 2016; Hyun & Kim, 2012; Im et al., 2014). However, the association with actual family income had variable effects. Family income had a negative association with psychiatric symptoms in several studies (Choi et al., 2013; Choi & Park, 2016; Kang et al., 2016; Kim, 2011; Lee, 2010; Park et al., 2015; Youn & Lee, 2010), and particularly those with income lower than 1–2 million Korean won (equivalent to 889–1778 USD) had more symptoms (Chung & Han, 2009; Im, 2010; Kim & Kim, 2013; Kim, 2007). However, a significant association was not noted between psychiatric symptoms and family income in other studies (Choi et al., 2012; Jo et al., 2012; G. Kim et al., 2013; S. Kim et al., 2013; S. Lim et al., 2009), and one noted that economic change after marriage, not family income, was linked to their depressive symptoms (Jo et al., 2012). The results indicate that perceived relative economic status may have more of a significant role in MIW’s psychological health than actual income does.
Interestingly, in the remainder of the studies (C. Lee & Kim, 2010; S. Lim et al., 2009; K. Park & Jeong, 2011), a positive association was found between family income and depression after controlling for social variables. For instance, in one study (K. Park & Jeong, 2011), higher family income was a protective factor for marital intimacy and communication; however, after controlling for such variables, family income became linked to an increased risk of depressive symptoms. As one of the sources of marital dissatisfaction, financial distress has a negative impact on marriage and family relationship (Conger, Conger, & Martin, 2010), thus adversely affecting MIW’s mental health. However, high family income may not guarantee MIW’s positive psychological adaptation, particularly when there is a poor relationship with the husband and the husband alone controls the finance.
Employment
According to a national survey, 58.5% of MIW were employed, which is similar to the employment rate of native Koreans (Ministry of Gender Equality and Family, 2016). Existing evidence is mixed on the relationship between employment status and psychological health. Although no significant association was noted in several findings between being employed and psychiatric symptoms (Choi et al., 2012; Choi & Park, 2016; Kang et al., 2016; Kim et al., 2013; Lee, 2010; Lim et al., 2009; Yang & Kim, 2007), in other studies (Hong et al., 2013; S. Kim et al., 2013), MIW having a job had higher levels of anxiety and somatization symptoms. On the contrary, in the remainder of the studies (C. Lee & Kim, 2010; K. Park & Jeong, 2011), being employed was linked with decreased depressive symptoms even after controlling for socio-demographic variables such as income. A further study examined the psychological mechanisms underlying the role of employment and found that being employed decreased depressive symptoms by enhancing their adaptation to new society (Bae & Seo, 2011).
The variable effect of employment may arise from diverse job qualities. MIW who had a satisfying job presented decreased depressive symptoms than those who held an unsatisfying job, independently of other variables, including family income (K. Chung & Han, 2009). Insecure and low-wage jobs that involve simple labour account for the highest proportion of MIW’s job (Ministry of Gender Equality and Family, 2016). Given the mental health impacts of job quality, such as job insecurity and effort–reward imbalance (Butterworth et al., 2011; Kim & von dem Knesebeck, 2015), MIW’s low-quality job may pose an additional risk to their well-being. Furthermore, MIW reported experiencing the severest level of social discrimination at their workplace (Ministry of Gender Equality and Family, 2016), which can be liked to adverse mental health outcomes (Kessler, Mickelson, & Williams, 1999). In contrast, having a satisfying job with a supportive work environment may facilitate MIW’s social adaptation, thus decreasing their psychological distress.
Discussion
This study reviewed previous findings concerning the mental health of MIW in South Korea by focusing on pertinent risk and protective factors. The relative prevalence or levels of MIW’s psychiatric symptoms, in comparison with native Korean women or women in MIW’s home country, showed much variation between diverse samples. The variable results are similar to the variations among varied studies of Taiwan – another hosting country for Southeast Asian women who migrated through marriage. While MIW from Southeast Asian countries (e.g. Vietnam and Indonesia) reported an elevated level of mental health problems in several studies (W. J. Chou, 2010; Y. M. Yang & Wang, 2011; Y. M. Yang, Wang, & Anderson, 2010), in other studies, MIW had a lower prevalence of depression and a higher quality of life than Taiwanese native women, suggesting a healthy immigrant effect ( F. H.Chou et al., 2010; Huang & Yang, 2016). Although immigration is a potential mental health risk, it does not inevitably result in adverse outcomes (Berry, 1997). The mental health consequences of marriage migration may be moderated by a wide range of individual and social factors before and after marriage migration. The key risk and protective factors for MIW’s mental health are summarized in Table 2. To identify key, consistent factors, we used an approach employed in other review studies (Cannon, Jones, & Murray, 2002; Fazel, Reed, Panter-Brick, & Stein, 2012). In this approach, only the factors that were associated with MIW’s mental health outcomes in the same direction in at least three studies were included. However, if any result noted the opposite association between the factor and the same mental health outcome, we excluded the factor from Table 2.
Summary of risk and protective factors.
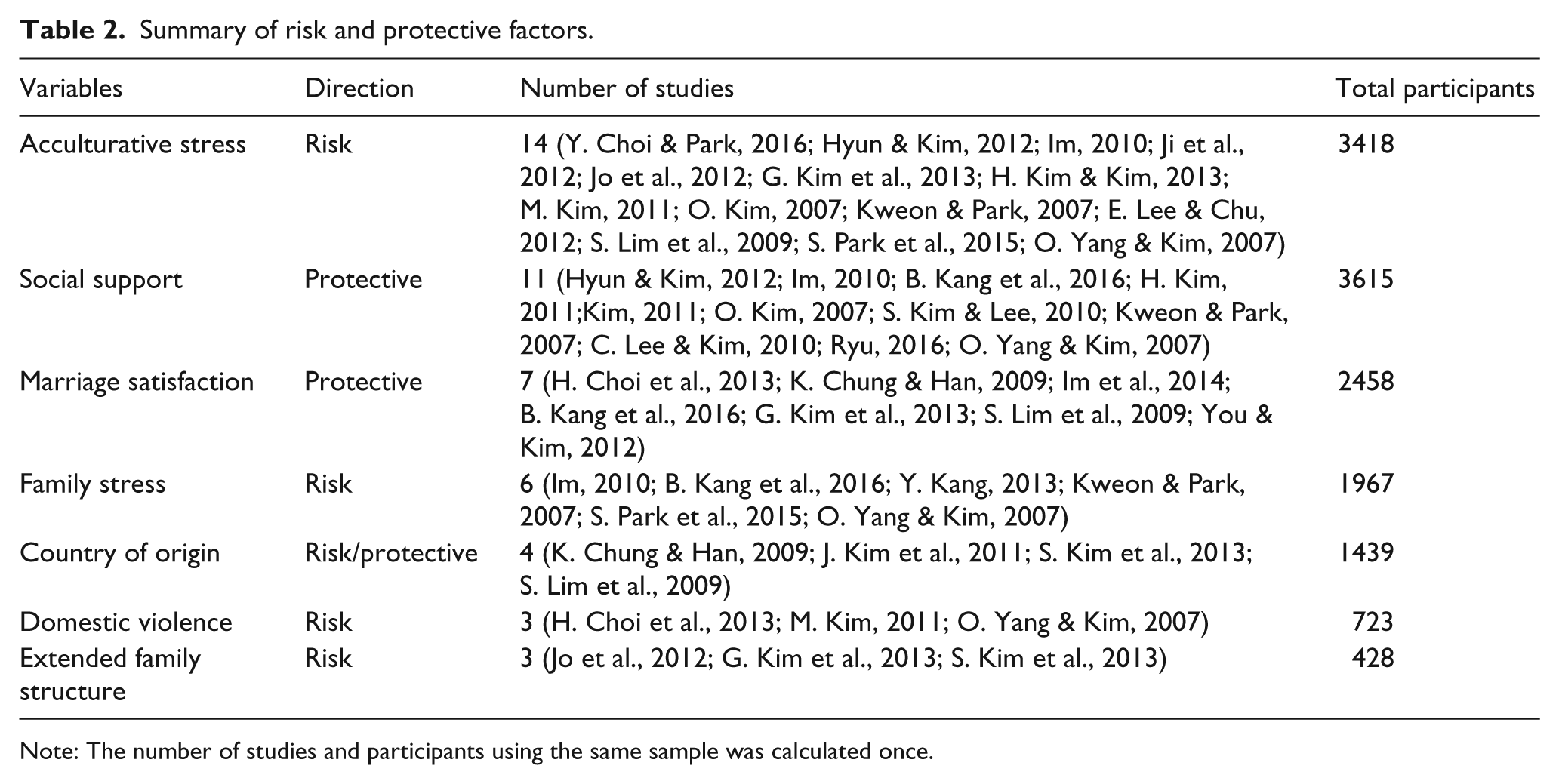
Note: The number of studies and participants using the same sample was calculated once.
As expected, the stress arising from acculturation process was the most consistent risk factor for MIW’s general psychiatric symptoms. Successful acculturation involves both maintaining one’s cultural identity acquired in their country of origin and participating in the culture of the new host society (Berry, 1997). Considering the heightened mental health risk for MIW who are marginalized from both home and host culture (Youn & Lee, 2010), interventions addressing the development of a successful acculturation strategy – integrating both cultures – will benefit this population. Of note, special consideration should be provided to the social attitude towards cultural diversity in Korea, which plays a pivotal role in immigrants’ successful cultural integration (Berry, 1991).
Among the factors that exist prior to marriage migration, country of origin showed consistent associations with mental health outcomes, in that MIW from countries who are less recognized by Koreans were more susceptible to mental health problems. The results are similar to the findings from Taiwan that Southeast Asian MIW had a higher likelihood of depressive symptoms than did Chinese MIW (W. J. Chou, 2010; Shu, Lung, & Chen, 2011). Considering that MIW from less developed countries have a higher proportion of brokered marriage (W. J. Chou, 2010), their elevated mental health risks may be partly attributable to the negative consequence of brokered marriage, where men often hold a superior position to women in marriage. Further attention is required concerning heterogeneous MIW population across countries of origin and its influence on post-migration adaptation, including differential power position of MIW in family and host society.
After marriage migration, multiple layers of social ties in Korea can mitigate or exacerbate MIW’s mental health difficulties. In the core layer of one’s personal networks, having a positive relationship with one’s Korean husband, indicated by marital satisfaction, has a significant impact on MIW’s psychological adaptation. On the contrary, family distress that can arise from domestic violence or co-living with parents-in-law threatens MIW’s mental health. Family system interventions are highly encouraged regarding fostering a positive marital and family relationship. Moreover, family educational programmes should be provided to promote egalitarian spousal relationships and prevent domestic violence.
Overall, as noted for immigrant women in other countries (Shu et al., 2011; Small, Lumley, & Yelland, 2003), social support in Korea was the most consistent protective factor that alleviated MIW’s psychological difficulty, and ties with Koreans, including their new family members, were particularly effective. In contrast, a recent survey presented that more than 30% of MIW in Korea reported having no one to ask for help when in need, demonstrating social isolation problems (Ministry of Gender Equality and Family, 2016). In addition, more than half of MIW’s social participation occurred only within co-ethnic ties, with a weak connection with Koreans. Given the positive role of cross-group relationships with majorities in minority’s well-being (Mendoza-Denton & Page-Gould, 2008), community efforts to increase opportunities for MIW to interact with Koreans will benefit their psychosocial adaptation.
Conclusion
Towards an integrative understanding of MIW’s mental health risks, we elucidated the key determinants of psychological consequences after their marriage migration to Korea. Although previous findings identified a broad range of factors that are associated with mental health outcomes, due to the cross-sectional nature of all studies, causal mechanisms underlying such mental health effects require further investigation. Future longitudinal studies that examine MIW’s mental health changes over time will extend current knowledge about the long-term processes of their psychological adaptation and key risk and protective factors at each settlement phase. Furthermore, given the striking individual variation of mental health status among this population, individual differences in the process of coping with marriage migration should be addressed. Successful psychological adaptation involves multiple layers of causes (Berry, 1997). Considering the paucity of studies examining personality attributes of MIW, prospective research should consider more how the micro-level of MIW’s personal attributes interplays with the macro-level of socio-cultural contexts, including familial relationship and community social-support systems, for deeper insights into multi-level processes underlying MIW’s adaptation. Future evidence-based interventions and policy formulation should comprehensively address MIW’s socio-cultural, economic and mental health needs.
Footnotes
Acknowledgements
SP made substantial contribution to conception and design of the study and drafting of the article. YL contributed to acquisition and analysis of data and drafting of the article and figures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (NRF – 2016R1D1A1B03931297).