
Abstract
Background:
Network- and cohesion-based social capital may play an important role in improving mental health. However, there is limited understanding about these relationships among adults in Taiwan.
Aim:
The aim of this study was to examine the association between individual-level network and cohesion-based social capital and depressive symptoms among a population-based sample of Taiwanese adults.
Methods:
Data were obtained from the 1997 Taiwan Social Change Survey (n = 2,598). The 20-item Center for Epidemiological Studies Depression Scale was used to measure depressive symptom scores; ⩾16 represented high depressive symptoms. Network-based social capital was measured using a position generator. Two dimensions of cohesion-based social capital were assessed: cognitive (perceived neighborhood trust and reciprocity) and structural (local community participation and organizational participation). Multivariable log-binomial regression models, weighted to account for the complex sampling design and adjusted for confounders, estimated prevalence ratios and 95% confidence intervals (CIs) to examine the association between each social capital measure and depressive symptoms.
Results:
In this study, 29.6% of respondents were classified as having high depressive symptom scores. Higher scores of composite cognitive social capital (adjusted Prevalence Ratios (aPR) = 0.92, 95% CI = [0.90, 0.95]) and structural social capital (aPR = 0.80, 95% CI = [0.65, 0.99]) were associated with a lower likelihood of high depressive symptom scores after controlling for confounders. However, there was no association between network social capital and depressive symptoms.
Conclusion:
The findings suggest that the relationship between social capital and depressive symptoms in Taiwan differs according to the specific dimension of social capital assessed. Differentiating between network- and cohesion-based social capital merits greater attention to inform our understanding of building social capital to promote and improve mental health outcomes.
Introduction
Social capital, broadly defined as resources available to individuals as a result of social relationships, is a multidisciplinary concept, derived from sociology, political science and economic theories. In public health, there are two main conceptual approaches to measuring social capital: network- and cohesion-based approaches (Berkman & Kawachi, 2014; Moore & Kawachi, 2017). Network social capital refers to the resources that are generated and accessed within social networks (Bourdieu & Wacquant, 1992). It is commonly used social network instruments such as the name, position or resource generators, to appraise sources of networks (Lin, 2001; Song, 2011, 2013; Song & Lin, 2009). The cohesion-based approach signifies membership in social organizations and perceptions of the quality of social relationships such as trust, reciprocity and support that facilitate coordinated actions (Putnam, Leonardi, & Nanetti, 1993). Cohesion-based social capital can be further characterized into two dimensions: cognitive (i.e. perceptions of trust, reciprocity and shared values) and structural (i.e. opportunity structures or activities to develop social ties and build social networks). Numerous studies have documented that social capital measured using either network- or cohesion-based approaches are key social determinants of health (Derose & Varda, 2009; De Silva, McKenzie, Harpham, & Huttly, 2005; Hu et al., 2014; Kawachi, Kennedy, Lochner, & Prothrow-Stith, 1997; D. Kim, Subramanian, & Kawachi, 2008).
Empirical studies linking social capital and depression generally demonstrate a protective association (Almedom, 2005; De Silva et al., 2005; D. Kim et al., 2008), although evidence of negative or null associations have also been documented (De Silva et al., 2005; Ehsan & De Silva, 2015). The variability between studies may be partly attributable to differences in operationalizing social capital. Diverse tools are used to measure social capital in different countries, preventing comparability across studies, and authors conceptualize social capital as both individual and ecological constructs (Cao, Li, Zhou, & Zhou, 2015). Furthermore, results from recent systematic reviews exploring the relationship between social capital and mental health suggest that variations in the associations may be due to differences in the conceptualization – network- versus cohesion-based social capital (De Silva et al., 2005; Ehsan & De Silva, 2015). For example, Bassett and Moore (2013) demonstrated that high levels of cohesion-based social capital reduced the likelihood of depressive symptoms. However, network-based social capital measures – for example, the position generator – were unrelated to depressive symptoms (Bassett & Moore, 2013).
The inconsistent associations between type of social capital and depression may reflect different mechanisms by which network- or cohesion-based approaches of social capital operate. Network social capital is postulated to influence depressive symptoms by accessing socially valuable resources (i.e. informational resources) that may help to reduce the chances of depression (Bassett & Moore, 2013; Lin, 2001; Song & Lin, 2009). The mechanisms linking cohesion-based social capital to depressive symptoms may operate through the cognitive domain by producing positive psychological states, such as a sense of being ‘accepted’ (Fujiwara & Kawachi, 2008), feelings of security and high self-esteem or self-efficacy (Harpham, Grant, & Thomas, 2002; Myer, Stein, Grimsrud, Seedat, & Williams, 2008). Alternatively, the structural dimension may influence depressive symptoms via access to social support resources or information through social participation and civic engagement (Kawachi & Berkman, 2001).
There is a dearth of information in the literature about social capital and depression among Taiwanese adults. First, the relationship between social capital and depression may be influenced by the political, historical and cultural context of the environment where individuals live (Blakely et al., 2006; Islam, Merlo, Kawachi, Lindström, & Gerdtham, 2006; Iwase, Suzuki, Fujiwara, & Takao, 2012). The extensive knowledge of the relationship between social capital and depression is largely derived from work conducted in Western countries (Cao et al., 2015). Although there are a growing number of studies conducted in China (Cao et al., 2015; Li, Zhou, Ma, Jiang, & Li, 2017; Wu et al., 2010) and Japan (Murayama et al., 2013), there remain relatively few studies conducted in Taiwan. The extent to which associations between social capital and health outcomes can be generalizable to East Asian countries remains unclear. For example, prior studies have shown variations in levels of social capital by world region, where East Asian countries, such as Taiwan, have lower levels in comparison to North America and Western Europe (Lee, Jeong, & Chae, 2011). Second, most social capital research tends to explore the influence of a single dimension on one health outcome (Bassett & Moore, 2013), thus limiting our understanding of the full extent of the relationship between social capital and depression. Distinguishing the health impact of network- versus cohesion-based social capital approaches can add value to explaining observed variations in depressive symptoms.
This study builds upon prior research and seeks to fill these gaps in our knowledge of the relationship between social capital and depressive symptoms by using several comprehensive measures of social capital. Data from the Taiwan Social Change Survey (TSCS), a nationally representative population-based sample, provide a unique opportunity to shed light on this association between social capital and depressive symptoms within Taiwan. More specifically, we compare the relative association between depressive symptoms and social capital as measured using network- and cohesion-based approaches. It is hypothesized that measures of both network- and cohesion-based social capital would be negatively associated with high depressive symptom scores. We also examine the association of composite and individual components of social capital measures and its association with depressive symptoms.
Methods
Data
The TSCS is a multi-cycle, long-term, nationally representative cross-sectional survey. The survey collects data on social issues relating to family, culture, religion, politics, social networks and social class, in addition to self-reported health and behavioral characteristics among residents in Taiwan. The TSCS is conducted by the Institute of Sociology, Academia Sinica, and sponsored by the Ministry of Science and Technology, Republic of China. The detailed survey procedures of the TSCS have been published elsewhere (Chu, 1998; Lin, Fu, & Hsung, 2001). Briefly, TSCS used a stratified random sampling method to select adults 20 to 74 years old for participation in the survey. Data were collected by face-to-face interviews using a structured questionnaire. All participants were given full instruction of the study and informed consent was obtained from each participant. The ethics committee of the National Science Council of Taiwan approved the survey.
The data in the study were conducted from June to November 1997. The 1997 TSCS dataset is unique because it is the only cycle to date that contains measures of both network-based (name and position generator) and cohesion-based (cognitive and structural) social capital and allows for one to distinguish and make comparisons among the different forms of social capital. Research conducted on the health impact of conceptually distinct forms of social capital and depression symptomatology in Taiwan has been limited. In more recent administrations of the TSCS, only cohesion-based measures (i.e. cognitive and structural) of social capital were included (H.-L. Cheng & Chiang, 2002; Chuang & Chuang, 2008) and the selected measures lacked comparability relative to other global studies examining social capital (Bassett & Moore, 2013; Haines, Beggs, & Hurlbert, 2011). A total of 2,835 participants completed the questionnaire with a response rate of 94% (Chu, 1998). Respondents were excluded if they were missing information on the outcome (n = 85) or the exposure (n = 161), yielding a final analytic sample of 2,598 adults.
Measurements
Outcome variable
Depressive symptoms were measured using the 20-item Center for Epidemiological Studies Depression Scale (CES-D; Radloff, 1977) . The Chinese version of CES-D was translated directly from the 20-item CES-D by two psychiatrists (Chien & Cheng, 1985) and has been widely used in Taiwan (Boey, 1999; S. T. Cheng & Chan, 2005; Cornman, Goldman, Glei, Weinstein, & Chang, 2003; C. Fu, Lee, & Chen, 2003; Yang, Soong, Kuo, Chang, & Chen, 2004). Prior studies have shown that the Chinese version of the CES-D is reliable (Cronbach’s α of .86) and validly measures depressive symptoms with high sensitivity (92%) and specificity (91.0%) (Chien & Cheng, 1985). Participants were asked the frequency of experiencing each symptom in the past week. Item responses were on a 4-point scale to indicate the frequency of the symptoms (0 = less than 1 day, 1 = 1–2 days, 2 = 3–4 days and 3 = 5–7 days). After summing the score for each item, CES-D scores ⩾16 were categorized as high depressive symptom scores and <16 as low (Radloff, 1977).
Exposure variable
We utilized network- and cohesion-based approaches to conceptualize social capital. The TSCS position generator assessed network social capital using a list of 15 ordered occupational positions (Lin & Dumin, 1986; Lin et al., 2001). Each participant was asked, ‘Of your relatives, friends and acquaintances, are there any who have the jobs listed in the following table?’ The choices for the 15 positions ranged from housemaids/cleaning workers to physicians. Network social capital was measured along three components: (1) extensity – the total number of occupations identified by each participant, (2) upper reachability – the highest prestige occupation that each participant could access and (3) range – the difference between the highest and the lowest prestige occupation (Lin et al., 2001; Song & Lin, 2009). The three variables were standardized (i.e. M = 0 and standard deviation (SD) = 1) for comparability. As a result of the high correlation between these components (Pearson correlation coefficient range: .64–.84), a composite network social capital score was constructed by the weighted sum of the three network social capital components. The weights were the standardized scoring coefficients from the first component of a principal components analysis because 84% of the variability could be accounted by the first component. High internal reliability justified the use of the composite score (Cronbach’s α = .90).
Cohesion-based social capital was conceptualized using the cognitive and structural dimensions. Two components of cognitive social capital were measured: trust in neighbors and perception of neighborhood reciprocity. Trust in neighbors was measured with one question: ‘For the aspect of trust, how would you describe people who live around you?’ Perceived neighborhood reciprocity was measured using two items: (1) care and (2) familiarity. To assess care, respondents were asked, ‘For the aspect of care, how would you describe the people who live around you?’ To assess familiarity, respondents were asked, ‘For the aspect of familiarity, how would you describe the people who live around you?’ Respondents were asked to rank the responses from the three questions using a 7-point scale. A composite cognitive social capital score was calculated by taking the sum of the three variables and used as a continuous variable in the main analyses. The three items of the composite score were highly correlated with each other (Pearson correlation coefficient range: .65–.72) and demonstrated high internal reliability (Cronbach’s α = .86).
Structural social capital was operationalized using two measures: organizational participation and local community participation. Organizational participation was assessed by the following question: ‘Have you attended an organization or club activity in the past 1 year?’ Respondents indicated whether they participated in one or more of the following types of organizations: religious, political, social movement, social service, alumni, occupational and ‘other, if any’. Local community participation was based on the question: ‘Have you attended a local community event in the past 1 year?’ Respondents indicated whether they participated in one or more of the following types of events: li’s/village’s meeting (a li is a geographical division with around 2,000 individuals created by the Taiwan Census Bureau), activity held by li/village, activity held by school, temple fair, church activity and activity held by other club/organization. Each variable of structural social capital was categorized into two levels: (1) no participation and (2) participation in one or more. The composite score for structural social capital was measured as a categorical variable with two levels: (1) no participation and (2) participation in at least one organization or local community event.
Confounders/covariates
We included several potential confounders that have been used in prior studies examining social capital and depression (Harpham et al., 2002; Song & Lin, 2009). Demographic factors included age (continuous), sex (men and women), marital status (currently married, single and formerly married) and religion (religious belief and no religious belief). Three commonly used socioeconomic variables were included: employment (not currently employed, currently employed and retired), education (junior high school or below, senior high school and junior college or above) and income status (no income, less than NT$19,999, NT$20,000–NT$39,999 and over NT$40,000).
Data analyses
Descriptive statistics for continuous variables were reported by weighted means and standard errors, and categorical variables were reported by weighted percentages and standard errors. The distribution of demographic factors, socioeconomic status and social capital measures were stratified according to high or low depressive symptom scores; comparisons were assessed using the chi-square test for categorical variables and t-test for continuous variables. A series of multivariable log-binomial regression models were used to separately estimate prevalence ratios (PRs) and 95% confidence intervals (CIs) of the association between social capital measures and depressive symptoms. For each social capital variable, two models were constructed: Model 1 (crude): social capital score; Model 2 (fully adjusted): Model 1 + demographic factors (age, sex, marital status and religion) and socioeconomic status (educational attainment, income and employment). The same series of multivariable log-binomial regression models were used and repeated for the composite score and individual components of network, cognitive and structural social capital. All statistical analyses applied sampling weights to adjust for the complex sampling frame and were conducted using Statistical Analysis System (SAS), version 9.3, with significance level at α = .05.
Results
In this study, nearly 30% of all participants were classified with high depressive symptom scores. Characteristics for the study population are presented in Table 1. Participants with high depressive symptom scores were less likely to be men, married, employed and have an income higher than NT$20,000 when compared to those with low depressive symptom scores. Network and cognitive social capital scores were lower among participants with high depressive symptom scores compared to those with low scores. For structural social capital, people with high depressive symptom scores had higher percentage of participating in either local community, organization or both when compared to those with lower depressive symptom scores.
Distribution of demographic factors, socioeconomic status and social capital by depressive symptoms, 1997 TSCS.
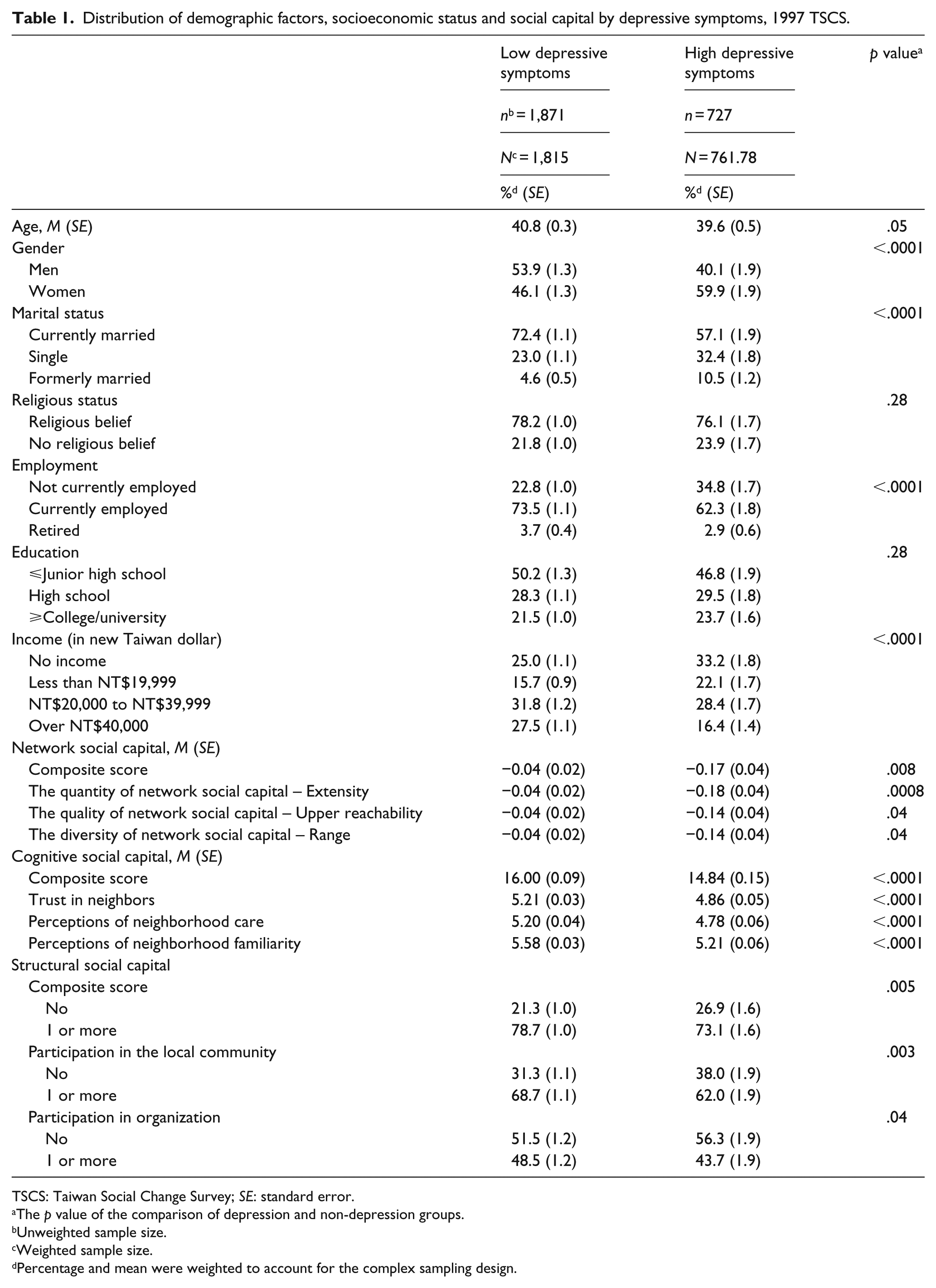
TSCS: Taiwan Social Change Survey; SE: standard error.
The p value of the comparison of depression and non-depression groups.
Unweighted sample size.
Weighted sample size.
Percentage and mean were weighted to account for the complex sampling design.
The results of the association between composite and component scores for the association between network social capital and depressive symptoms are shown in Table 2. Neither the composite score nor the individual components of network social capital were associated with having high depressive symptom scores after controlling for confounders.
Crude and adjusted PRs and 95% CIs for the association between network social capital and depressive symptoms; 1997 TSCS.
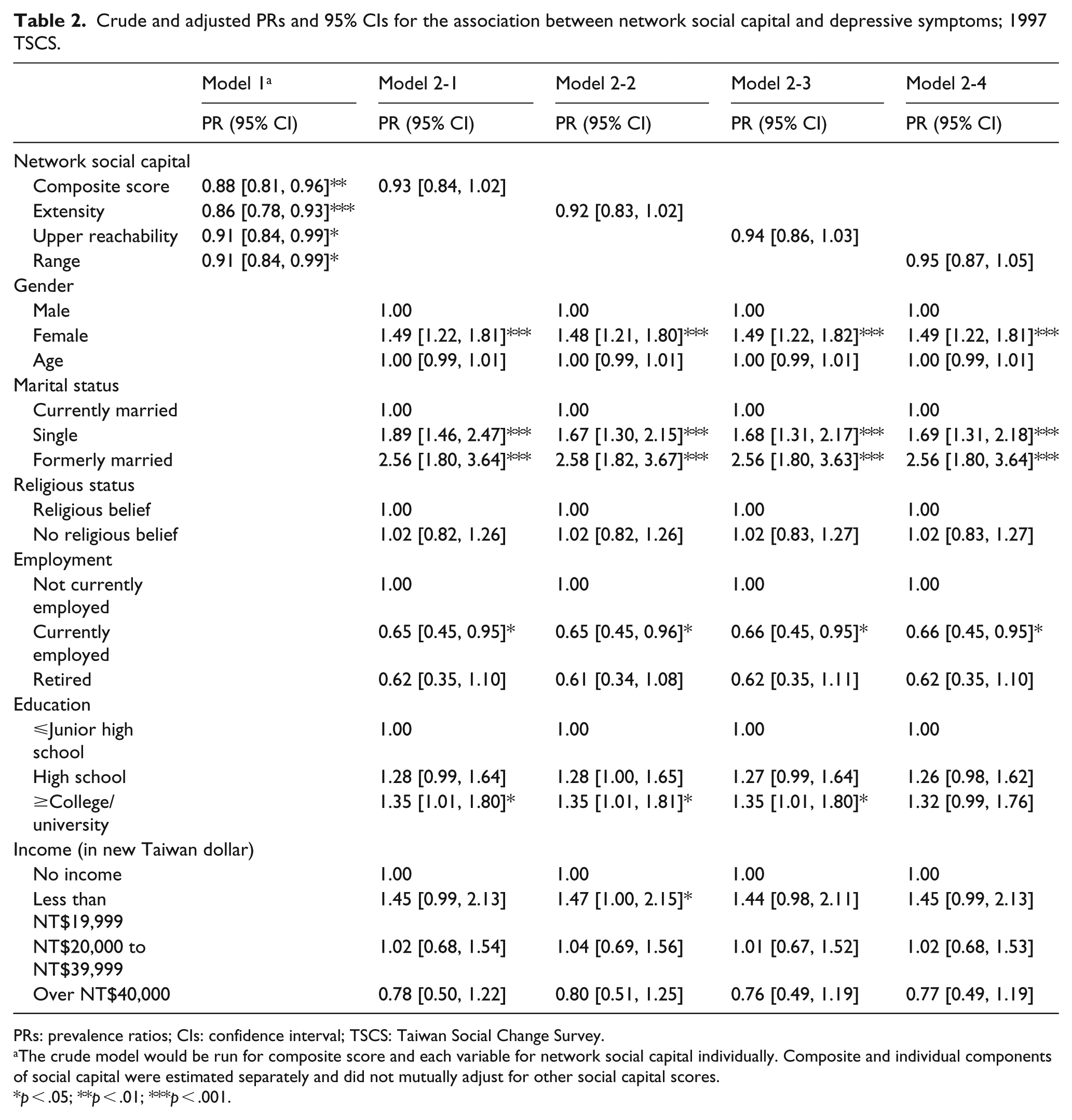
PRs: prevalence ratios; CIs: confidence interval; TSCS: Taiwan Social Change Survey.
The crude model would be run for composite score and each variable for network social capital individually. Composite and individual components of social capital were estimated separately and did not mutually adjust for other social capital scores.
p < .05; **p < .01; ***p < .001.
Table 3 presents crude and adjusted PRs and 95% CIs for the association between cognitive social capital and depressive symptoms. People with higher composite cognitive social capital scores were associated with lower likelihood of high depressive symptom scores after controlling for potential confounders (PR = 0.92, 95% CI = [0.90, 0.95]). Specifically, people who reported higher trust in neighbors (PR = 0.82, 95% CI = [0.77, 0.88]), higher perceptions of neighborhood care (PR = 0.84, 95% CI = [0.79, 0.89]) and higher perceptions of neighborhood familiarity (PR = 0.84, 95% CI = [0.79, 0.90]) were associated with lower likelihood of high depressive symptom scores after controlling for potential confounders.
Crude and adjusted PRs and 95% CIs for the association between cognitive social capital and depressive symptoms; 1997 TSCS.
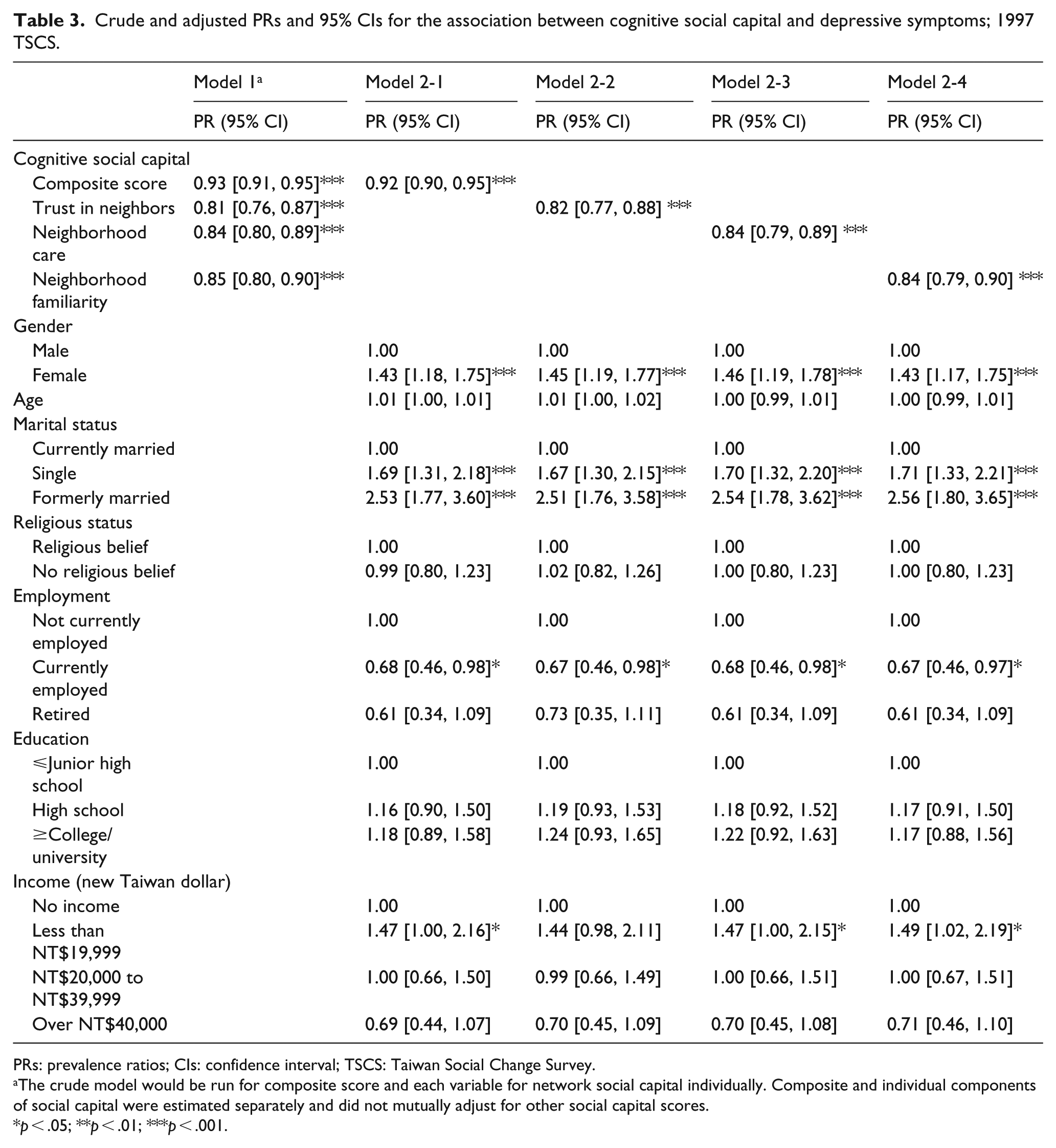
PRs: prevalence ratios; CIs: confidence interval; TSCS: Taiwan Social Change Survey.
The crude model would be run for composite score and each variable for network social capital individually. Composite and individual components of social capital were estimated separately and did not mutually adjust for other social capital scores.
p < .05; **p < .01; ***p < .001.
PRs estimating the association between structural social capital and depressive symptoms are shown (Table 4). In the fully adjusted model, the composite structural social capital score was associated with lower likelihood of high depressive symptom scores (PR = 0.80, 95% CI = [0.65, 0.99]). Individuals who reported participating in one or more local community events had a lower likelihood of high depressive symptom scores in comparison to those who reported no participation (PR = 0.78, 95% CI = [0.64, 0.94]).
Crude and adjusted PRs and 95% CIs for the association between structural social capital and depressive symptoms; 1997 TSCS.
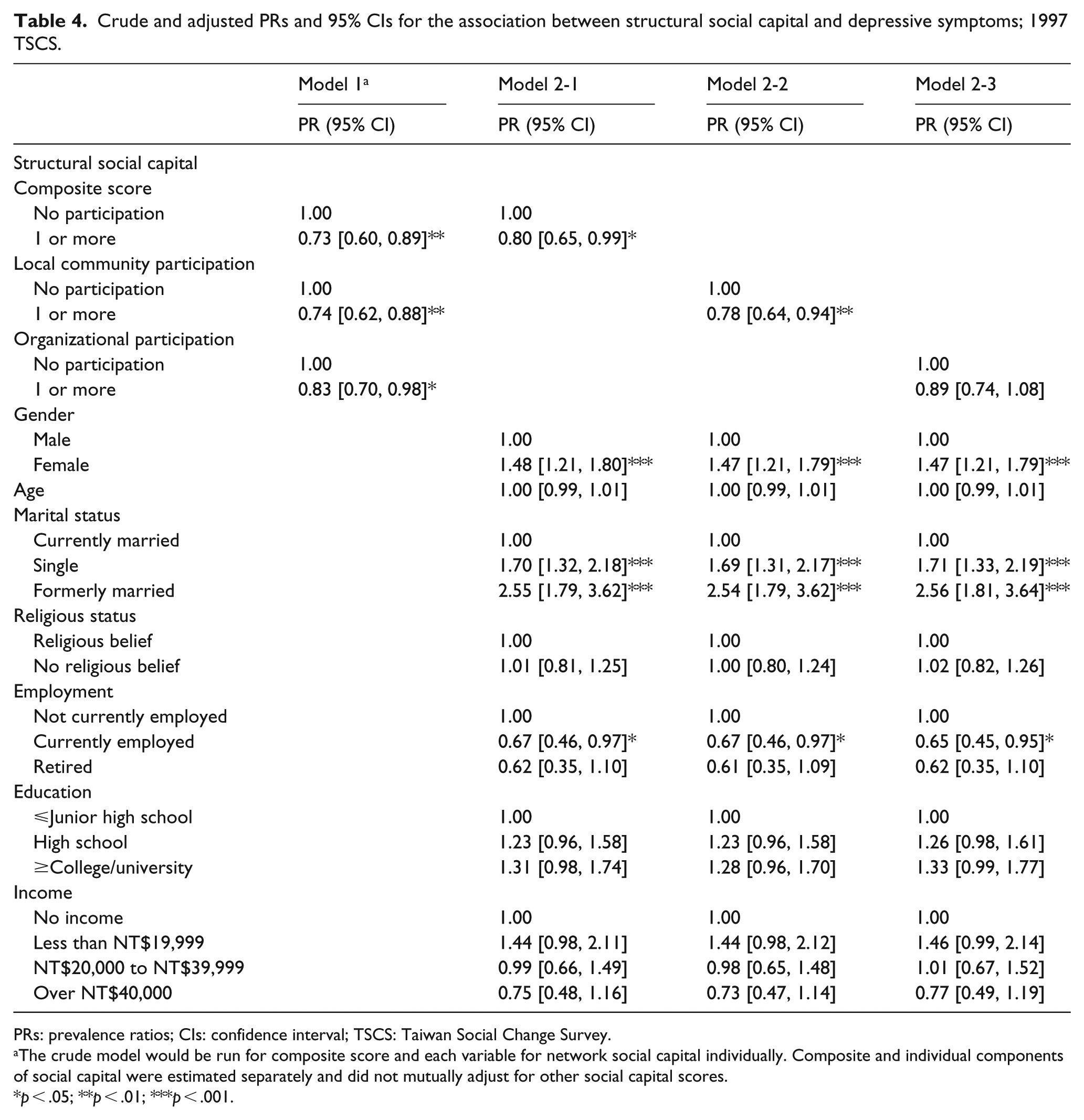
PRs: prevalence ratios; CIs: confidence interval; TSCS: Taiwan Social Change Survey.
The crude model would be run for composite score and each variable for network social capital individually. Composite and individual components of social capital were estimated separately and did not mutually adjust for other social capital scores.
p < .05; **p < .01; ***p < .001.
Discussion
The current study examined the association between network- and cohesion-based social capital and depressive symptoms among a population-based sample of Taiwanese adults. The primary finding of this study highlights variations in the association between network- and cognitive-based social capital and depressive symptoms. The likelihood of high depressive symptom scores was lower among people with higher composite scores of cohesion-based measures of social capital. However, network-based social capital was not associated with depressive symptoms in this sample.
Both composite and individual-level components of cognitive social capital were associated with lower reports of high depressive symptom scores in the study. Our findings are similar to previous research exhibiting an inverse association between depressive symptoms and cognitive social capital (represented as either perceived neighborhood trust, interpersonal trust, perceived neighborhood cohesion or social reciprocity) in other countries, including the United States, Europe, Japan and China (Bassett & Moore, 2013; Forsman, Nyqvist, Schierenbeck, Gustafson, & Wahlbeck, 2012; Fujiwara & Kawachi, 2008; S. S. Kim, Chung, Perry, Kawachi, & Subramanian, 2012; Norstrand, Glicksman, Lubben, & Kleban, 2012). Prior studies have shown a strong consistent relationship between cognitive social capital and mental health in general, and depression, more specifically (De Silva et al., 2005; Ehsan & De Silva, 2015). Reporting high levels of cognitive social capital may be related to lower depressive symptoms because it may produce positive psychological states, such as a sense of being accepted and feelings of security, which help to cope with and buffer against stress (Fujiwara & Kawachi, 2008; Kawachi & Berkman, 2001; Phongsavan, Chey, Bauman, Brooks, & Silove, 2006).
According to our results, the composite and only one component of structural social capital score was associated with depressive symptoms. Evidence linking structural social capital and depressive symptoms is mixed. Some studies show that structural social capital, as measured by community and neighborhood participation, was not associated with depression in the general population (Bassett & Moore, 2013; Fujiwara & Kawachi, 2008; Lewin, Mitchell, Rasmussen, Sanders-Phillips, & Joseph, 2011; Norstrand et al., 2012), whereas various forms of social participation (i.e. religious and political) were associated with depression among older adults (Ellison & George, 1994; Sugihara, Sugisawa, Shibata, & Harada, 2008). It is possible that the inconclusive findings may be dependent upon the type of participation measured. For example, although we observed an association between composite structural social capital and depressive symptoms, this was largely driven by participation in local community activities, whereas organizational participation was unrelated to depressive symptoms. While we did not have detailed information regarding the group context (i.e. bonding, bridging and/or linking ties) of structural social capital, it is possible that differences in the nature of ties characterizing participation in local community organizations versus organizational participation may explain the divergent findings. In Taiwan, local organizations with strong neighborhood and community orientation tend to be kinship-based and provide a social context with strong bonding ties (Chang, 2009). Alternatively, organizational participation, organizations with less of a local orientation, typically includes non-family members and is characterized by bridging and linking ties that may be less influential in mobilizing resources to impact depressive symptomatology. Although social participation represents a potential key mental health resource enabling an individual to reduce depressive symptoms, additional research is needed to determine whether distinguishing between different forms of social participation can further our understanding of the mechanisms linking structural social capital and depressive symptoms.
Network social capital measures were not associated with depressive symptoms in this study. This is contrary to the results of prior research conducted in Taiwan, which used the same dataset and found that network social capital was associated with depression (Song & Lin, 2009). Discrepancies in the results may be attributable to methodological differences. In our study, both composite and individual components of network social capital were associated with depressive symptoms in the unadjusted model; however, after adjustment for relevant confounders, neither estimate retained statistical significance. In our analyses, we controlled for more confounders (e.g. religion and employment status) in comparison to Song and Lin (2009). Differences in study sample selection may also account for the conflicting conclusions. For example, the Song and Lin (2009) study excluded more people (n = 517) in their analyses because they lacked complete information on the name generator.
Several other studies found that network social capital, as measured by the position generator, was unrelated to depression (Bassett & Moore, 2013; Vyncke et al., 2014; Webber, Huxley, & Harris, 2011). It has been suggested that this lack of association may be due to the type of network ties that the position generator captures (Bassett & Moore, 2013). The social ties identified by a position generator may reflect weaker ties (Lin, 2001, 2008; Moore, Daniel, Gauvin, & Dubé, 2009; Moore, Daniel, Paquet, Dubé, & Gauvin, 2009) that represent the extent of access to structural positions in a hierarchy, but not strong ties (Lin, 2008). It is possible that weak ties may not provide adequate support or resources to help people manage, cope or alleviate moderate to severe depressive symptoms (Bassett & Moore, 2013).
Strengths and limitations
This study has several strengths. First, the TSCS is nationally representative and the results are largely generalizable to the overall Taiwanese adult population. This study measured social capital comprehensively using network- and cohesion-based approaches to compare the relative strength of association between the different measures. The use of these measures is a fundamental strength of this study because it adds theoretical value and deepens our understanding of social capital and depressive symptoms.
Findings from this analysis must be considered in light of several limitations. First, confirmation of a causal relationship between social capital and depressive symptoms is not possible given the cross-sectional study design. Furthermore, it is possible that reverse causality, the idea that some of our participants may have been depressed and therefore reported lower ratings of social capital, may potentially explain some of the associations observed. However, our findings are consistent with evidence from longitudinal studies assessing social capital and depression in the United States (Fujiwara & Kawachi, 2008) and South Korea (S. S. Kim et al., 2012), and we do not think that this may have a major impact on our overall study findings. Second, measurement error in the assessment of social capital may have influenced our results. Detailed information about the timing of cognitive social capital could not be captured because participants were not asked when they experienced neighborhood trust or reciprocity. Furthermore, for structural social capital, we were not able to specify the nature of ties in the activities and organizations that study respondents participated in because the questionnaire did not include this level of detail. Third, we only measured social capital at the individual level. There is increasing evidence showing that neighborhood-level social capital may be independently associated with depression (Tomita & Burns, 2013) and future studies should explore this further among Taiwanese adults.
Fourth, there are other factors such as personality and underlying genetic traits, and life experiences that may influence depressive symptomatology. Unfortunately, these variables were not available to examine in the dataset. Finally, we used data from the 1997 TSCS because of the unique opportunity to compare network- and cohesion-based measures of social capital within the same time period with measures that were comparable to other studies. Although the data are older, some temporal patterns, such as the stability of the prevalence of major depression between the late 1980s until the present (Liao et al., 2012), lead us to believe that our analyses are still informative regarding factors that impact depression. Furthermore, research suggests that recent trends in common mental disorders have increased over time simultaneously with social inequalities (e.g. national rates of unemployment) in Taiwan (S.-T. Fu, Lee, Gunnell, Lee, & Cheng, 2013). It is possible that social psychiatric population–based preventive measures, such as social capital interventions, may be an important additional component to support the clinical management of mental health and further reduce the burden of mental health problems (Flores et al., 2018).
Conclusion
While our study largely mirrored the results from studies conducted in Western countries and China, these findings add to the limited body of research on social capital and depressive symptoms in Taiwan. Our results suggest that the association between social capital and depression in Taiwan differs according to the specific dimension of social capital assessed. Differentiating between network- and cohesion-based social capital merits greater attention to serve as the evidence base to develop intervention programs that strengthen social capital and mitigate poor mental health.