
Abstract
Objective:
Qualitative research has identified personal costs and benefits for peer supporters associated with their role; however, quantitative evidence is sparse. This study used quantitative methods to explore relationships in experiences of providing peer support with constructs of empowerment, hope, recovery, quality of life and internalised stigma. Differences were examined for those in statutory versus non-statutory services; who had themselves received peer support versus those who had not and who identified having had negative experiences in clinical teams versus those without such experiences.
Methods:
A cross-sectional online and postal survey was undertaken in tandem with a linked consensus study. In all, 147 peer supporters were recruited from a variety of organisations across the United Kingdom. Validated questionnaires were used to examine constructs. Instruments created for the study measured peer support experiences, and personal costs and benefits involved. Correlations were calculated and results informed further regression analysis. Chi-square tests and independent samples t-tests tested group differences.
Results:
Peer supporters indicated they experienced almost twice as many role-related personal benefits than personal costs. Benefits included improvements to mental health and well-being, reduced use of services, increased social functioning and development of skills. Total number of personal costs experienced was significantly negatively related to peer supporters’ empowerment and quality of life. There were no significant differences between the groups examined.
Conclusions and Implications for Practice:
An accumulation of personal costs may result in reduced quality of life; however, costs can be minimised by organisations. Limitations of the research are discussed and recommendations for future research are made including the need for longitudinal research.
Introduction
There has been a recent trend towards formalising peer support as provided by persons holding a distinct role in mental health services. Increasing numbers are employed in the United States, United Kingdom, Canada, New Zealand and other regions in such roles in a variety of settings including public/statutory services (Repper & Carter, 2011). The evidence for formalised peer support as an effective ‘intervention’ is growing (Chinman et al., 2014; Lloyd-Evans et al., 2014; Pitt et al., 2013), potentially having unique benefits over traditional care for service users who have ‘received’ it (Bradstreet, 2006; Davidson, Bellamy, Guy, & Miller, 2012; Gillard et al., 2015).
Mutuality and reciprocity are commonly viewed as essential to peer support (iNAPS, 2011; Repper et al., 2013a; SRN, 2012) suggesting that effects should be experienced by all peers in the relationship to some degree. Existing research on the impact of ‘doing’/’providing’ formal peer support on ‘peer supporters’ themselves has almost exclusively used qualitative methodologies. Positive impacts have been identified in various psychosocial domains. Improvements have specifically been noted in levels of empowerment (Faulkner & Kalathil, 2012; Ochocka et al., 2006), hope (Davidson, Chinman, Sells, & Rowe, 2006), recovery (Bailie & Tickle, 2015; Moran, Russinova, Gidugu, Yim, & Sprague, 2012; Salzer & Shear, 2002) and quality of life (Bracke, Christiaens, & Verhaeghe, 2008; Mowbray, Moxley, & Collins, 1998; Salzer & Shear, 2002). Peer support is also said to offer opportunities to actively challenge stigma (Faulkner & Basset, 2012) including through disclosure about mental health problems thereby undermining the secrecy and shame implicated in the internalisation of stigma (Corrigan et al., 2016).
Equally, qualitative research has described a range of role-related challenges people working as peer supporters can encounter. These include no/low wages, limited opportunities for career progression, mistreatment by non-peer colleagues and inadequate training, support and supervision (Vandewalle et al., 2016). It has been suggested that peers working in public services may experience more acute challenges for reasons including the dominance of biomedical models of mental distress in such environments (clashing with the values of peer support and recovery); highly hierarchical organisational structures (with peer supporters in relatively powerless positions) and little experience of how to best use peer support in such contexts, with a consequent lack of clarity about the role (Gillard, Edwards, Gibson, Owen, & Wright, 2013; Kemp & Henderson, 2012). Thus, peer supporters may experience adverse effects potentially having a detrimental impact on their well-being, and peer supporters working in public services may be at greater risk of this.
The qualitative studies which comprise the majority of the current evidence base have been undertaken with small samples. It is therefore unknown how prevalent role-related personal costs and benefits may be for the wider population of peer supporters. Quantitative research with larger samples is limited to two US studies. Moran, Russinova, and Stepas (2012) examined the relationship between peer supporters’ role characteristics and self-rated mental health recovery and found no significant association. Ahmed, Hunter, Mabe, Tucker, and Buckley (2015) found that employed peer specialists had higher self-reported hope and empowerment levels than unemployed peer specialists, though the difference may have been due to employment in general rather than employment as a peer supporter per se.
The study presented here used quantitative methods with a relatively large sample to address gaps in the evidence. It explored relationships between aspects of providing peer support and psychosocial constructs which qualitative research has indicated to be amenable to change. Specific hypotheses were as follows:
1. The satisfaction in the peer support role (namely, satisfaction with training, supervision, pay, and opportunities for career progression), perceived support in the role, team acceptance and value for peer support, and personal benefits experienced in the role would each be positively related to levels of empowerment, hope, mental health recovery and quality of life and negatively related to internalised stigma.
2. The personal costs experienced in the role would be negatively related to empowerment, hope, mental health recovery and quality of life and positively related to internalised stigma.
Furthermore, this study explored whether there might be differences in psychosocial well-being between peer supporters in different settings and with different experiences. Hypotheses were as follows:
3. The peer supporters working in public services and those with negative role-related experiences would report more internalised stigma and personal costs and less empowerment, hope, mental health recovery, quality of life and personal benefits compared to peers working in non-public services or without negative role-related experiences.
4. The peer supporters who had themselves received formal peer support would report more empowerment, hope, recovery, quality of life and personal benefits and less internalised stigma and personal costs than those who had not received formal peer support.
Method
Data for this study were collected at the same time as for a Delphi study which is linked within this volume. Readers are directed to that paper for sampling procedures.
Measures
Experience of providing peer support (EPPS)
The EPPS was devised by the authors for the purposes of this study and, in total, comprised 23 items about peer support experiences plus demographic questions (see online supplementary materials). Nine items were used as single-item variables. Satisfaction with the role, training, supervision and career progression was rated on a 10-point Likert-type scale, whereby 1 = very dissatisfied and 10 = very satisfied. Perceived support in the role, perceived acceptance by mental health team and perceived team value for peer support were rated on similar Likert-type scales whereby 1 = not well supported/accepted/valued and 10 = very well supported/accepted/valued. Item means were used in the analyses. A categorical item measured whether participants had negative role-related experiences within their team; participants responded yes, no or don’t know/would rather not say.
Personal costs and personal benefits of providing peer support
A list of statements concerning personal costs and personal benefits associated with providing formal mental health peer support were generated for this study through a process of literature review and expert consultation (see the linked Delphi study). There were 16 personal costs statements and 25 personal benefits statements. Participants were asked to respond yes or no to indicate whether each statement had been part of their experience as a peer supporter. A total count of yes responses were calculated for each participant. Mean totals were used in the analyses as a measure of personal costs and personal benefits experienced. A cost:benefit ratio was calculated by dividing mean totals into the possible total (i.e. costs = 16, benefits = 25) to compare proportions of participants endorsing costs versus benefits.
Mental Health Confidence Scale (MHCS)
Total score on the MHCS was used as a measure of empowerment. The MHCS has 16 items rated on a 6-point confidence scale whereby 1 = very nonconfident and 6 = very confident; higher scores indicate increased empowerment (Carpinello, Knight, Markowitz, & Pease, 2000). It has good psychometric properties (Castelein, van der Gaag, Bruggeman, van Busschbach, & Wiersma, 2008). Scores on the optimism subscale (the first six items of the MHCS) were used as a measure of hope. This was to reduce participant burden by keeping the number of measures to a minimum. In this study, Cronbach’s alpha for the total scale was α = .92 and for the hope/optimism subscale it was α = .89 indicating high reliability.
Process of recovery questionnaire (QPR)
The QPR was used to measure mental health recovery. It has 15 items which are rated on a 5-point agreement scale whereby 0 = strongly disagree and 4 = strongly agree; higher scores indicate more improved recovery (Law, Neil, Dunn, & Morrison, 2014; Neil et al., 2009). The QPR has good psychometric properties (Law et al., 2014; Williams et al., 2015). In this study, Cronbach’s alpha for the QPR was α = .93 indicating high reliability.
Manchester Short Assessment of Quality of Life (MANSA)
The MANSA was used to measure quality of life. A total of 12 items are rated on a 7-point satisfaction scale whereby 1 = couldn’t be worse and 7 = couldn’t be better; higher scores indicate better quality of life (Priebe, Huxley, Knight, & Evans, 1999). Good psychometric properties for the scale have been reported (Björkman & Svensson, 2005; Priebe et al., 1999). In this study, Cronbach’s alpha was α = .86 indicating high reliability.
Internalised Stigma of Mental Illness scale – brief version (ISMI-10)
The ISMI-10 was used to measure internalised stigma. It has 10 items rated on a four-point agreement scale whereby 1 = strongly disagree and 4 = strongly agree and includes two reverse-scored items (Boyd, Otilingam, & DeForge, 2014). Higher scores indicate more internalised stigma; thereby having an inverse valence to the other measures in the study. The ISMI-10 has good psychometric properties (Boyd et al., 2014; Hammer & Toland, 2016). Cronbach’s alpha was α = .81, indicating high reliability. With the permission of the author, the term ‘mental health problem’ was used in place of ‘mental illness’; this was following feedback from a service user group that many reject the concept of ‘illness’ when applied to mental distress and may find the term stigmatising.
Analyses
Analyses were conducted using SPSS Statistics software version 23 (IBM, 2015). Between-group differences for categorical variables were calculated using Chi-square tests and for continuous variables using independent samples t-tests. Data for EPPS variables were not normally distributed, and thus, two-tailed Spearman’s correlations were performed to examine relationships between these and costs/benefits and psychosocial constructs. Missing values were excluded analysis-by-analysis. The participant number (n) for each test changed reflecting the varying proportions of data provided by participants on different measures/items. In light of numerous tests planned, an alpha level of p ⩽ .01 was adopted to reduce the chance of false-positive results.
Results
Sample characteristics
A total of 147 peer supporters participated in the study; 76 of these provided a full dataset including all psychosocial measures. There were no statistically significant differences between those who provided a full dataset and those who did not. Table 1 provides a description of the total sample, categorical items included in the analyses and group differences (see supplementary materials for descriptive statistics of continuous variables). The majority of the sample was female. Approximately half (n = 76, 51.7%) provided peer support in public mental health services (i.e. the UK National Health Service (NHS)). Approximately half of the sample (n = 80, 54.4%) worked in a multidisciplinary mental health team (the majority in the NHS). Of those working in a multidisciplinary team, 32 (40%) had a negative experience within the team which they perceived to have been related to their role. Less than one-third of the total sample (n = 45, 30.6%) had themselves received formal peer support.
Characteristics of the total sample and of those who provided a complete and incomplete dataset.
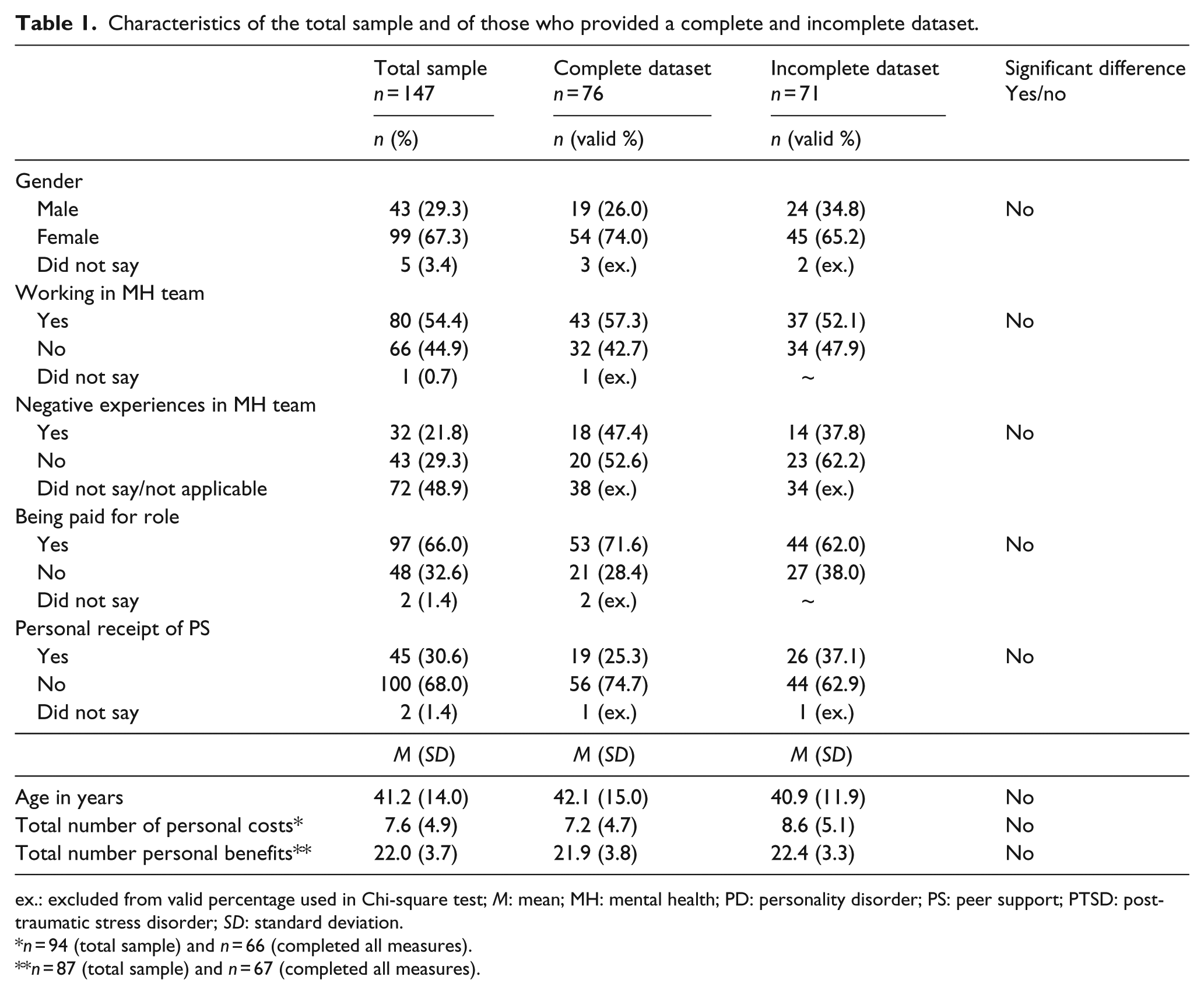
ex.: excluded from valid percentage used in Chi-square test; M: mean; MH: mental health; PD: personality disorder; PS: peer support; PTSD: post-traumatic stress disorder; SD: standard deviation.
n = 94 (total sample) and n = 66 (completed all measures).
n = 87 (total sample) and n = 67 (completed all measures).
Personal costs and benefits experienced
Mean number of personal costs endorsed was 7.6 (standard deviation (SD) = 4.9) and mean number of personal benefits endorsed was 22 (SD = 3.7). The costs:benefits ratio was .48:.88 meaning that, on average, participants endorsed almost twice as many benefits as costs. Tables 2 and 3 show the personal costs and benefits statements endorsed, ranked from highest to lowest (data are also provided for the NHS subsample).
Personal costs.
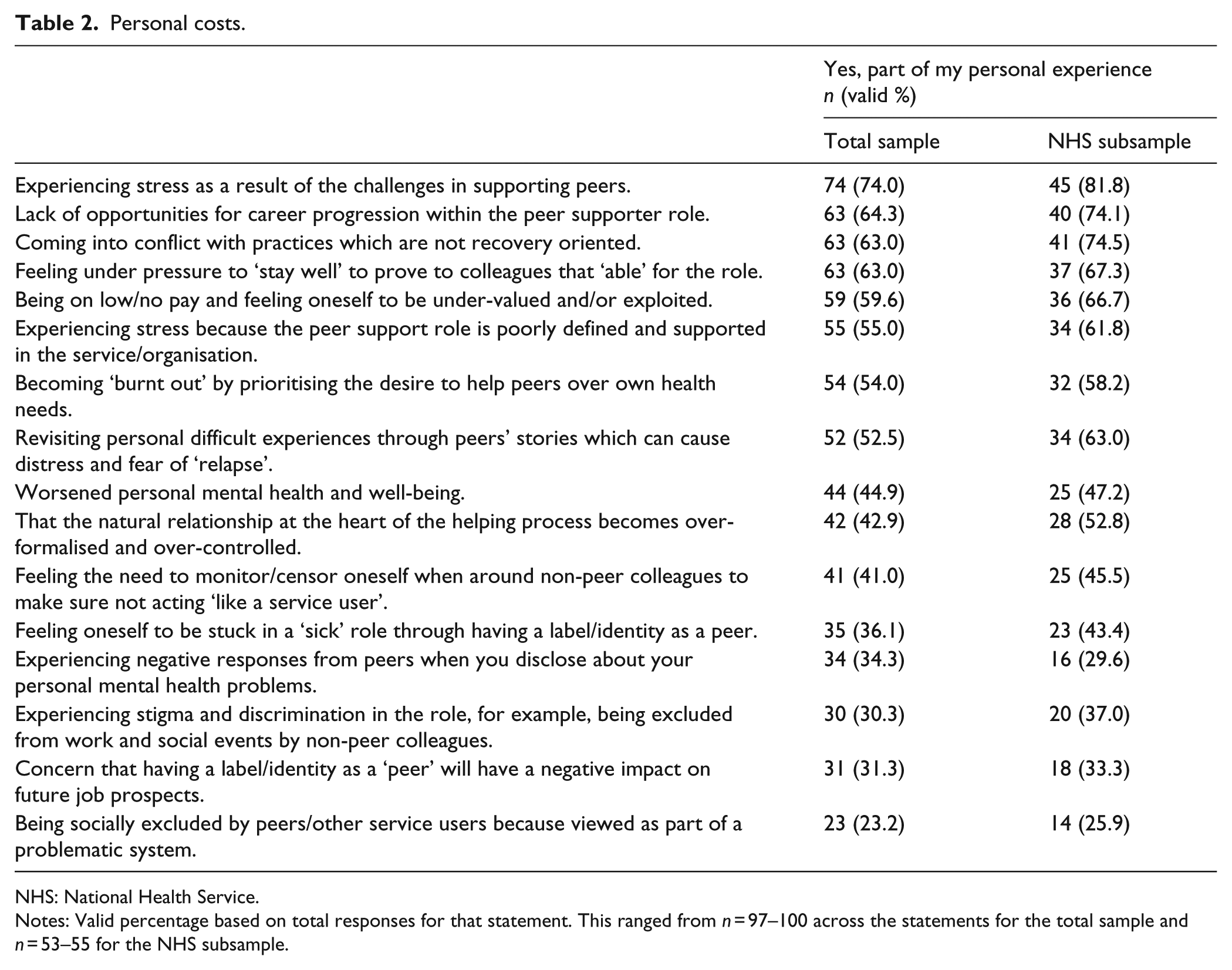
NHS: National Health Service.
Notes: Valid percentage based on total responses for that statement. This ranged from n = 97–100 across the statements for the total sample and n = 53–55 for the NHS subsample.
Personal benefits.
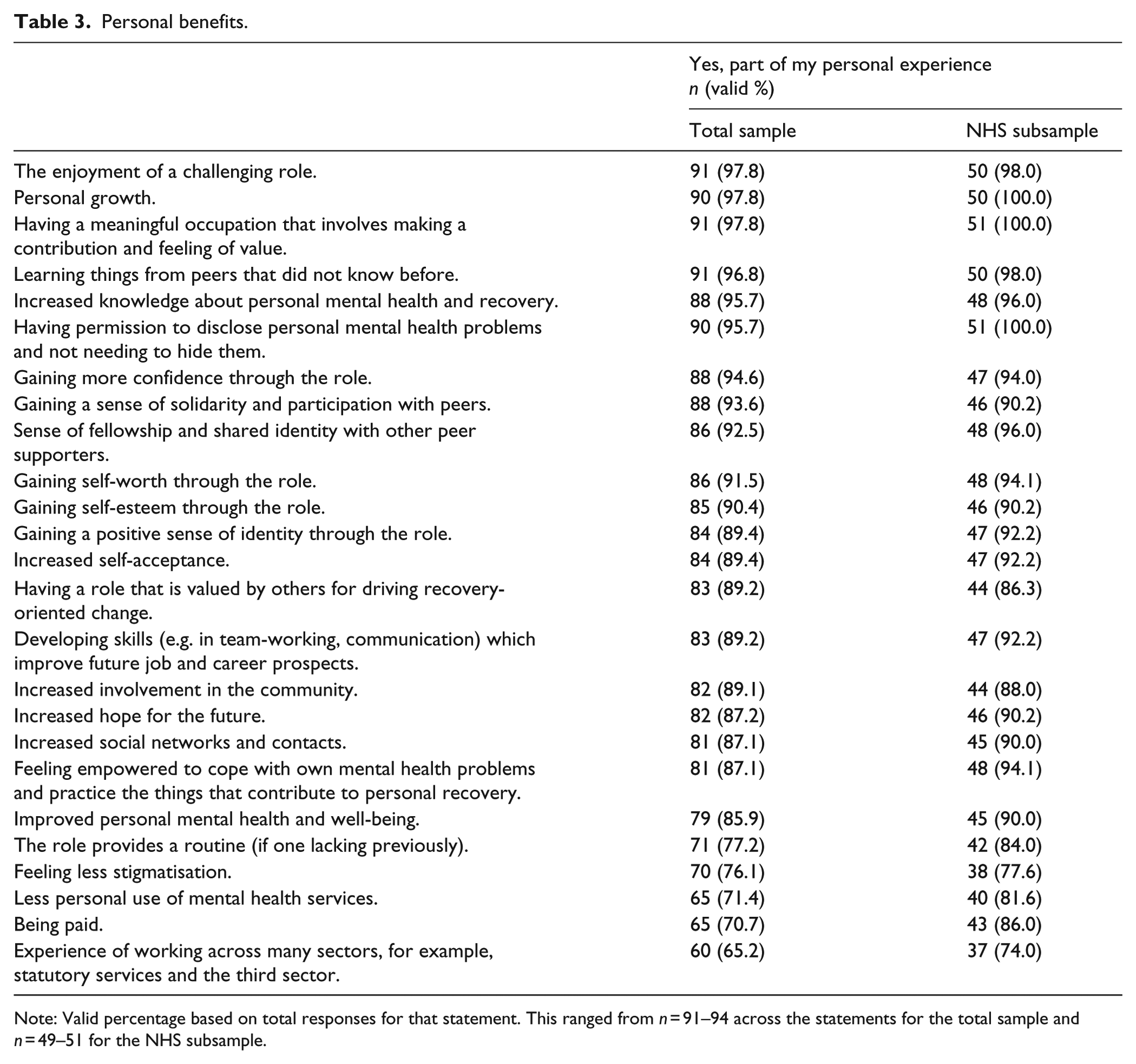
Note: Valid percentage based on total responses for that statement. This ranged from n = 91–94 across the statements for the total sample and n = 49–51 for the NHS subsample.
Relationships between experiences of providing peer support and psychosocial constructs
Correlations between scores on EPPS items, total number of personal costs and benefits experienced, and total scale/subscale scores on the psychosocial constructs are presented as a matrix in Table 4. EPPS items were highly inter-correlated, the majority at a statistically significant level. Similarly, the psychosocial constructs were all significantly inter-correlated. However, EPPS items did not significantly correlate with the psychosocial constructs, with the exception of quality of life which was significantly positively correlated with perceived support in the role (rs = .32), perceived acceptance by mental health team (rs = .41) and perceived team value for peer support (r = .46). Quality of life also positively correlated with satisfaction with training (rs = .24), satisfaction with professional supervision (rs = .25), satisfaction with pay (rs = .25) and satisfaction with career progression (rs = .27) at a level approaching statistical significance.
Correlations between experiences of providing peer support, personal costs and benefits experienced, and psychosocial constructs.
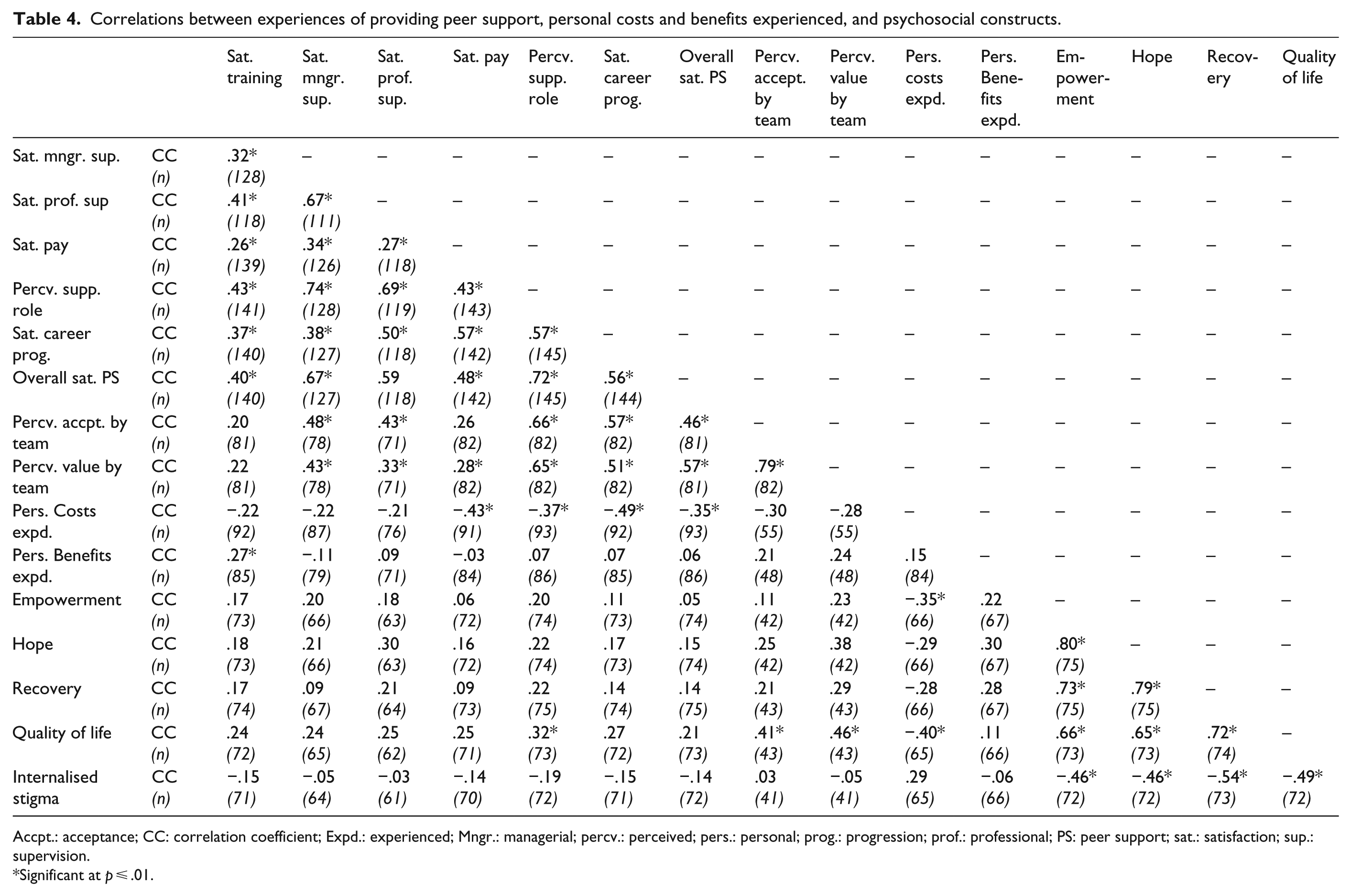
Accpt.: acceptance; CC: correlation coefficient; Expd.: experienced; Mngr.: managerial; percv.: perceived; pers.: personal; prog.: progression; prof.: professional; PS: peer support; sat.: satisfaction; sup.: supervision.
Significant at p ⩽ .01.
Total number of personal costs experienced was significantly negatively correlated with quality of life (rs = −.40) and empowerment (rs = −.35), as well as with satisfaction with pay (rs = −.43), satisfaction with career progression (rs = −.49), perceived support in the role (rs = −.37), and overall role satisfaction (rs = −.35). Total personal costs were also negatively correlated with hope (rs = −.29) and recovery (rs = −.28) and positively correlated with internalised stigma (rs = .29) at a level approaching significance. A positive correlation between total personal benefits and hope (rs = .30), recovery (rs = .28) and satisfaction with training (rs = .27) also approached significance.
Quality of life–sensitivity and regression analyses
Further exploratory analyses were conducted to investigate the potential relationship between experiences of providing peer support and quality of life as suggested by the results of correlational analyses. The MANSA quality-of-life measure contained an item concerning job satisfaction and satisfaction with finances so it was deemed possible that significant correlations between total MANSA score and EPPS items may have been artefactual (i.e. due to the same underlying constructs being measured by both). To rule this out, a ‘sensitivity’ analysis was conducted whereby a total MANSA score was calculated excluding the two aforementioned items, and Spearman’s correlations were re-run. Quality of life remained significantly correlated with perceived support in the role (rs = .30, p = .009), perceived acceptance by team (rs = .40, p = .007), perceived team value for peer support (rs = .46, p = .002) and personal costs (rs = −.46, p < .001). In order to explore which of these variables might uniquely predict quality of life, a regression analysis was then performed with quality of life as the dependent variable and perceived acceptance by team, perceived team value for peer support and personal costs as the predictor variables. Missing data were deleted listwise to generate a sensible model (Field, 2014); this left a sample of 37 participants with a full dataset to contribute to the model; all provided peer support in a multidisciplinary mental health team. Given the exploratory nature of the analysis, all variables were entered simultaneously (i.e. forced entry). Bootstrapping was used to generate confidence intervals and significance values because the data were non-normal. Results are presented in Table 5. The resultant model explained 40% of the variance in quality of life for this sample; R2 was .40 and significant (F(4,32) = 5.37, p = .002). The only significant predictor of quality of life in the model was total number of personal costs endorsed (β = −.48, partial r = –.49, p = .02).
Regression analysis with quality of life as the dependent variable (with confidence intervals (CI), standard errors and significance values based on 1,000 bootstrap samples).
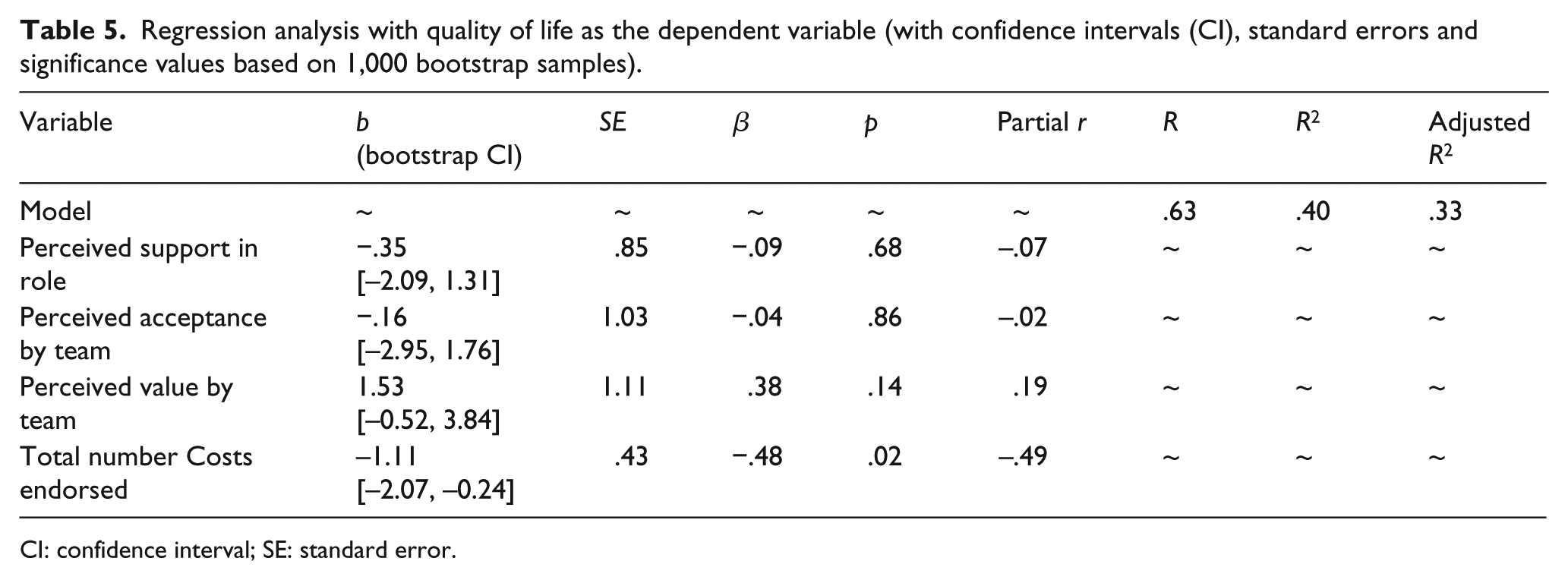
CI: confidence interval; SE: standard error.
Between-group differences
There were no statistically significant differences between the groups examined; however, there were a number of findings in the hypothesised direction at levels approaching significance (see Table 6). On average, NHS peer supporters reported more personal costs and more personal benefits than their non-NHS counterparts. Participants who had themselves received formal peer support had, on average, higher quality of life and higher recovery scores than those who had not received formal peer support. Those who had negative experiences within their team had, on average, lower quality-of-life scores than those who did not report negative experiences, and they endorsed a higher number of personal costs.
Between-group differences in psychosocial constructs, total costs and total benefits experienced.
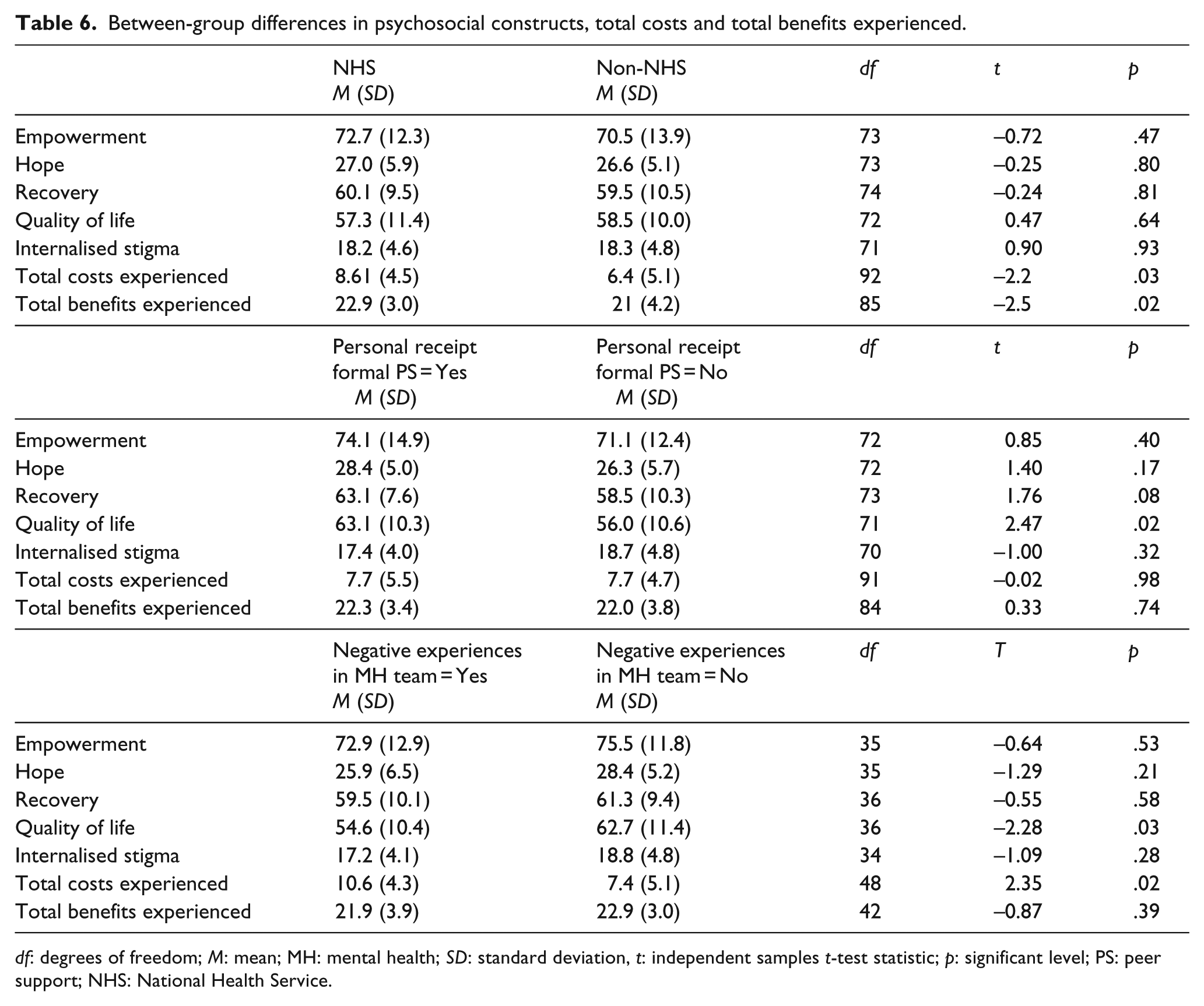
df: degrees of freedom; M: mean; MH: mental health; SD: standard deviation, t: independent samples t-test statistic; p: significant level; PS: peer support; NHS: National Health Service.
Discussion
This study used quantitative methods to explore relationships between experiences of providing peer support and levels of empowerment, hope, recovery, quality of life and internalised stigma in peer supporters. Previous qualitative research has indicated that providing peer support may influence these constructs. The study also looked at differences between peer supporters working in public versus non-public services and between those with and without negative experiences in the role. It is one of the first studies to use validated instruments to measure psychosocial well-being in peer supporters.
Results provide some limited and tentative support for the study’s first and second hypotheses. Relationships between experiences of providing peer support and the constructs examined were all in the predicted direction, though most were not statistically significant. Role satisfaction, perceived support and perceived team acceptance and value for peer support were not related to empowerment, hope, recovery or internalised stigma at levels more than would be expected by chance. However, perceived support in the role and perceived team acceptance and value for peer support were significantly positively related to quality of life of peer supporters. Also, the total number of personal costs endorsed had a significant negative relationship with quality of life and empowerment scores. Relationships between personal costs and the other psychosocial constructs approached statistical significance. Regression analysis suggested that personal costs had a unique negative effect on quality-of-life scores for those who worked in multidisciplinary mental health teams, such that increasing numbers of personal costs contributed to reduced quality of life in this group. The total number of personal benefits endorsed was positively correlated with hope and empowerment, but this relationship was not strong enough to be statistically significant given the strict criteria used. On average, participants reported having experienced nearly twice as many role-related personal benefits as personal costs.
These results have some important implications. They suggest that an accumulation of personal costs experienced in peer support roles may be disempowering and reduce the quality of life of peer supporters. When interpreting this finding, it is important to return to the content of the personal costs statements; most of the most highly endorsed statements were related to organisational difficulties in how the peer support role is set-up (e.g. low pay, lack of opportunities for career progression and non-recovery-oriented service cultures). Thus, organisations can limit any potential adverse effects of taking on the role by improving working conditions for peer supporters; indeed, it is their responsibility to do so. The intentional use of personal experiences of distress is an additional duty inherent to the peer supporter role which is not expected of non-peer staff. It is therefore appropriate that additional tailored support is provided (Davidson et al., 2012). In this study, high endorsement of stress in the role, for example, peer supporters’ feeling under pressure to ‘stay well’ to prove they are ‘able for the job’ suggests that managers should not only ensure support is readily available but be pro-active in encouraging peer supporters to utilise this and discuss barriers to take-up.
Results indicate that the behaviour and attitudes of non-peer colleagues matter for peers working in multidisciplinary mental health teams. Perceptions of being accepted, valued and supported in the team were related to better quality of life. This finding is in-line with previous qualitative studies which have highlighted the importance of team readiness for peer support (e.g. Hamilton, Chinman, Cohen, Oberman, & Young, 2015; Moll, Holmes, Geronimo, & Sherman, 2009) including having shared expectations and agreement on the parameters of the role (e.g. Asad & Chreim, 2015; Gillard et al., 2015; Kemp & Henderson, 2012). Organisations planning to implement peer support must consider how to prepare teams and undertake ongoing promotion of the role within the team context.
It warrants highlighting that participants endorsed almost twice as many role-related personal benefits than costs. The most highly endorsed personal benefit was ‘the enjoyment of a challenging role’, suggesting that even though challenges in supporting peers could be stressful, the role was also valued as personally rewarding. Other benefits endorsed included improvements in well-being (e.g. self-worth, self-esteem, self-confidence and hope); improved social functioning; the development of skills and peer reciprocal benefits (e.g. learning from peers, feelings of solidarity and fellowship). Over 70% of the sample reported decreased personal use of mental health services as personal benefit of the role. These findings will of interest to mental health service providers since they suggest that the introduction of peer support initiatives may reduce costs of care. Equally, just under half of the sample reported ‘worsened personal mental health and well-being’. These somewhat contradictory findings are nevertheless consistent with qualitative research which has highlighted that providing peer support can both enhance and inhibit personal recovery (Bailie & Tickle, 2015). It is probable that role-related factors influence peer supporters’ well-being and recovery in complex ways and that these change over time. A longitudinal case-series study has examined the impact of providing group supervisory support for peer specialists and found improvements over time with ongoing supervision on recovery and self-efficacy (Weikel, Tomer, Davis, & Sieke, 2017).
The hypothesised differences between groups of peer supporters were not supported. NHS peer supporters did not have worse scores on psychosocial measures that their non-NHS counterparts. On average, they endorsed more personal costs than non-NHS peer supporters; however, they also endorsed a higher number of personal benefits. There were no significant differences between peer supporters with negative team experiences and those without. Similarly, peer supporters who themselves had received formal peer support did not do better than those who did not have peer support. It is important to state that had significant differences been found between groups these would have required further investigation, controlling for other potentially influencing factors. However, results may suggest that peer supporters working in public services fare no better or worse than those working in non-public services.
Limitations
This study has a number of limitations. Perhaps most important is the use of measures without established psychometric properties. The EPPS was generated for this study and has not been previously validated; single items were used as variables, which reduces reliability and increases the likelihood of error. Due to the absence of a pre-existing way to measure the personal costs and benefits of providing peer support, this was measured by summing the number of costs and benefits statements endorsed by participants. It is acknowledged that this is a crude method which presumes a simple cumulative effect for the impact of personal costs and benefits which has not been verified. Other limitations include potential sampling bias (discussed in the linked paper) and a small sample size for the regression analysis which limits power. It is also probable that there were external variables not included as predictors in the regression, thus results should be interpreted with caution.
Conclusions and recommendations for practice and future research
Peer supporters in this study endorsed a wide range of personal costs and benefits associated with providing formal peer support that were derived from existing evidence and literature. Results indicate that the role exposes peer supporters to almost twice as many personally beneficial experiences than personally costly experiences. An accumulation of personal costs may contribute to reduced quality of life, especially for peer supporters in multidisciplinary mental health teams; however, many of these costs can be minimised by organisations. Ways that organisations can minimise the potential for adverse effects and facilitate the successful introduction of peer support are described in the linked paper within this volume and elsewhere in the literature (Davidson et al., 2012; Gillard, Edwards, Gibson, Holley, & Owen, 2014; Repper et al., 2013b). For example, organisations who wish to implement peer support successfully must already be working in a recovery-oriented way. Attention should be paid to clarifying the remit and responsibilities of the role and to preparing and educating non-peer staff in advance. Appropriate ongoing supervision and workplace support is a priority; organisations should ensure this is provided and reasonable adjustments are made.
This study supports previous research indicating that providing peer support may contribute to both improvement and decline in peer supporters’ well-being. More longitudinal research is needed to understand this further. Well-designed randomised controlled trials may make more robust conclusions about the effects of peer support; given mutual and reciprocal effects, outcomes for all peers in the supporting relationship should be measured. On the basis of this study, it is recommended that quality of life should be measured as an outcome in future research and it is also an appropriate outcome measure for peer support in services. Adverse effects for peer supporters should be monitored in research and clinical practice with a view to ensuring necessary supports are in place so that these may be minimised in the future.
Supplemental Material
Supplementary.Materials1 – Supplemental material for Providing mental health peer support 2: Relationships with empowerment, hope, recovery, quality of life and internalised stigma
Supplemental material, Supplementary.Materials1 for Providing mental health peer support 2: Relationships with empowerment, hope, recovery, quality of life and internalised stigma by Eilish M Burke, Melissa Pyle, Karen Machin and Anthony P Morrison in International Journal of Social Psychiatry
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.