
Abstract
Background:
Several childhood stressors related to immigration have been documented, and it is important for clinicians to understand and address the various factors that may lead to or act as maintaining factors of mental disorders in children and adolescents.
Aims:
To describe the cultural profile of transcultural patients presenting to a Child and Adolescent Mental Health Service (CAMHS) in regional Victoria and identify the most common disorders and psychosocial stressors they presented with.
Method:
Descriptive analysis was applied to 101 case records of patients with a transcultural background who attended the CAMHS of Latrobe Regional Hospital in Gippsland Victoria from 2013 to 2017. The Adverse Childhood Experience questionnaire was retrospectively applied to capture psychosocial stressors such as ‘bullying’, ‘racism’ and ‘family conflict’, sexual abuse, physical violence, parents with mental illness and parental substance use.
Results:
Almost 60% of patients were male and over 46% Aboriginal. Those from a non-Aboriginal background belonged to 19 different cultural entities, the most common of which was a mixed Asian and European heritage. The most common diagnoses were disruptive mood dysregulation disorder (38.6%), attention-deficit hyperactivity disorder (32.7%) and developmental trauma disorder (26.7%). The most common psychosocial stressors were conflict and death in the family (44.6%), domestic violence (41.6%) and emotional abuse (34.7%). ‘Parent in jail’ and ‘domestic violence’ were associated with having an Aboriginal background (p < .005). ‘Cultural differences with parent’ was associated with a non-Aboriginal background (p < .005).
Conclusion:
This study provides a snapshot of challenges faced by children from different cultural backgrounds while adjusting in a rural area in Australia. A broad-based formulation and cultural awareness by clinicians can enable a better understanding of the complexities, guide management plans and inform public health policies for primary prevention and early intervention.
Keywords
Introduction
Children who endure traumatic experiences and have mental health problems are known to be at high risk of developing mental disorders in adulthood (Fryers & Brugha, 2013). Factors such as family adversity, parental incarceration, physical and sexual abuse and neglect as well as family conflict and separation are associated with negative mental health outcomes (Fryers & Brugha, 2013). Aboriginal children (the term Aboriginal is used to refer to Australian Aboriginal and Torres Strait Islander peoples), child refugees and children with a migrant background are considered to be at risk groups (Ceri et al., 2017; Fazel & Stein, 2002; Jorm, Bourchier, Cvetkovski, & Stewart, 2012) in whom social and cultural influences significantly contribute to their mental health outcomes (Kim, Sherman, & Taylor, 2008). However, ‘Culture is a moving target’ (Kirmayer, 2006) and new cultures and sub-cultures are continuously emerging as a result of globalization and people movement.
While the mental health impact of trans-generational trauma in the Aboriginal population is well known (Hunter, 2007; Zubaran, Foresti, & De Moore, 2013), difficulties faced by non-Aboriginal children of transcultural heritage is less clear. These children are being raised in a completely different social and cultural milieu when compared to their parents and grandparents. This is largely due to dramatic changes in migration patterns in the last few decades (Population Australia, 2019). The latest Census data has revealed that almost a quarter (24.6%) of Australia’s population was born overseas and 43.1% of people have at least one overseas-born parent (Population Australia, 2019). These percentages are among the highest in the developed world (Population Australia, 2019). Furthermore, the migration pattern into Australia is gradually shifting towards being predominantly Asian (Australian Bureau of Statistics, 2018).
These developments are significant because the rate of mental illness in first-generation children of migrants is known to be particularly high (Bhugra, 2004; Cantor-Graae & Selten, 2005 ; Pumariega, Rothe, & Pumariega, 2005) and there are several influences on the mental health of adolescents from a migrant background (Hilario, Oliffe, Wong, Browne, & Johnson, 2015). Several stressors related to immigration can have long-lasting negative consequences on the developing brain rendering children vulnerable to mental health problems (including psychosis). These include the stress of immigration itself, feelings of alienation in a new culture, lack of a social network, lack of an extended family, conflict with the family of origin, pressure to assimilate with the peer group, experience of racism, perception of rejection by the peer group and bullying (Bhugra, 2004; Priest, Paradies, Trenerry, & Truong, 2013). Hence, it is important for clinicians to understand and address the various factors that may lead to or act as maintaining factors of mental disorders in children and adolescents (Yearwood, Crawford, Kelly, & Moreno, 2007).
The purpose of this study is to describe the cultural profile of transcultural patients presenting to a Child and Adolescent Mental Health Service (CAMHS) in regional Victoria and to identify the most common disorders and psychosocial stressors they present with.
Methods
Setting
Gippsland occupies the Southeastern corner of the state of Victoria and stretches from the outer fringes of South-Eastern Melbourne to the New South Wales border in the East with the Great Dividing Range in the North (Victorian Government, 2015). It has regional centres and vast areas of remoteness. The Eastern part is more remote than the rest; the central part is the industrial hub and has a higher population density. The Western part has easier access to Melbourne and has been experiencing a steady population growth (Victorian Government, 2015).
The Gippsland region witnessed substantial non-Anglo, European immigration in the 1950s and 1960s mainly from Italy, Germany, Holland, Greece and Malta (Gippsland Immigration Park, 2019). Hence, Gippsland has a predominantly European culture (Population Australia, 2019). Most Europeans have Anglo-Saxon heritage mixed with other European heritage, speak mostly English at home and identify themselves either as Christians or as practicing no religion (Population Australia, 2019).
Data from the 2016 census showed that Gippsland had a total population of 143,033 of which about 1.9% were Aboriginal (Australian Bureau of Statistics, 2017). Aboriginal people in Gippsland are either ‘Gunai Kurnai’ (traditional owners of the land) or other tribes and ‘Stolen generations’ (Population Australia, 2019). The ‘Stolen generations’ refers to more than 50,000 children of mixed Aboriginal and White settler heritage who were taken away from their Aboriginal parents to be brought up in foster homes where many of them endured multiple forms of abuse. This was a government ruling and was implemented from the late 1800s to 1970. The practice is said to have resulted in intergenerational trauma, which is partly responsible for the high prevalence of chronic physical and mental conditions among Aboriginal people today (Human Rights and Equal Opportunities Commission, 1997).
The CAMHS of Latrobe Regional Hospital (LRH) Mental Health Services in the Gippsland region of Victoria is provided through more than 30 clinicians divided into five teams who cover the six shires of Gippsland, namely, East Gippsland, Wellington, Baw Baw, South Gippsland and Bass Coast (see Figure 1). The CAMHS team includes child and adolescent psychiatrists, social workers, psychologists, mental health nurses, occupational therapists and speech therapists. The service is inclusive of a region wide autism assessment service, early psychosis service, CAMHS in School Service and the regular CAMHS service. Interestingly, more than 50% of the clinicians from this service are overseas born, among whom more than 35% are from a non-English-speaking background.
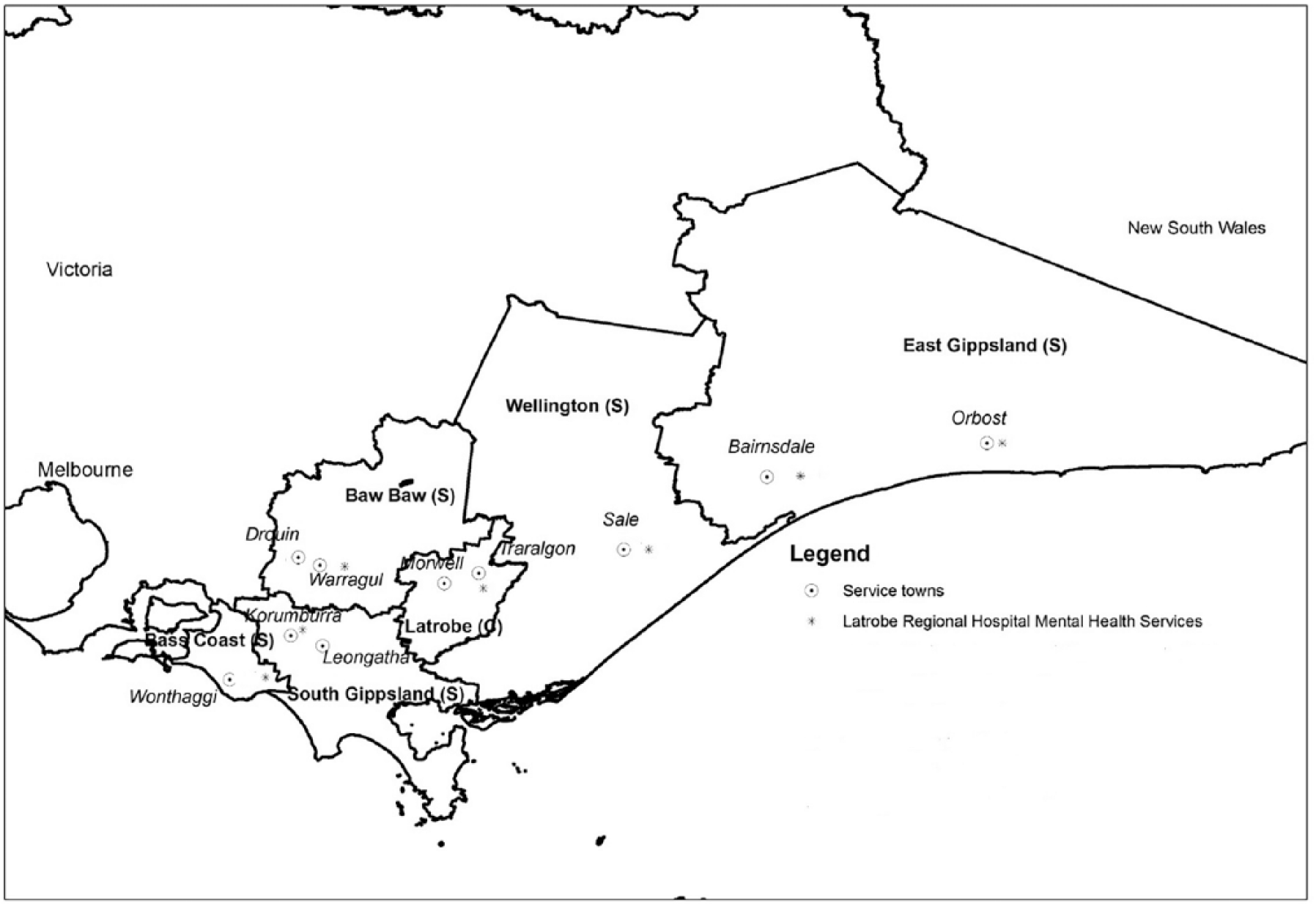
Map of Gippsland showing coverage of Latrobe regional hospital mental health services.
Patients are eligible to access the LRH CAMHS if they are under the age of 18 and have severe emotional and behavioural difficulties (Naughton, Maybery, & Goodyear, 2018). Each patient receives a comprehensive psychiatric assessment and a bio-psycho-social formulation (Mindful formulation; Havighurst & Downey, 2009). They are further assessed by HONOSCA (Naughton, Carroll, Basu, & Maybery, 2018) and the Strengths and Difficulties Questionnaire (Mathai, Anderson, & Bourne, 2002). Assessments are standardized and files are regularly audited by senior management to ensure consistency of assessments and quality of record keeping. These assessments are undertaken by CAMHS clinicians who along with their discipline specific training have successfully completed the Developmental Psychiatry Course provided by Mindful Victoria (Mindful Centre for Training and Research in Developmental Health, 2011). On an average, each clinician carries a case load of 16–24 patients (Naughton et al., 2018).
Data collection
A two-step approach was adopted for data collection. As an initial step, all clinicians were requested to list their previous patients who were from a transcultural background. A transcultural background was defined as one who was born overseas or whose parents were born overseas or from a non-English-speaking or Aboriginal background. Case records of all these patients were retrieved from the medical records department. Retrieved case records belonged to patients who were managed by CAMHS from 2013 to 2017. Following this, the first author browsed through all the current records with the clinicians to determine eligibility. Information on Aboriginality was readily available as it is routinely documented as part of socio-demographic data of all patients. A previous study has indicated that about 800 patients are referred to the CAMHS annually of which 300 receive comprehensive assessment and case management (Naughton, Carroll et al., 2018). A total of 101 case records satisfied the inclusion criteria (accounting for about 8.4% of clients assessed during the period 2013–2017).
Presenting complaints, diagnosis, comorbid diagnosis and management plan of patients were obtained from case records. The Adverse Childhood Experience questionnaire (Felitti et al., 1998) was retrospectively applied to capture psychosocial stressors such as ‘bullying’, ‘racism’ and ‘family conflict’, sexual abuse, physical violence, parents with mental illness and parental substance use (Felitti et al., 1998). Ethical approval for the study was obtained from the Human Research Ethics Committee of Latrobe Regional Hospital (Approval number 2016–06Q).
Data analysis
Data were analysed descriptively using frequencies, mean and standard deviation. Data were divided into two distinct groups – Aboriginal and non-Aboriginal. This distinction was made because although both groups were cultural minorities, they are very different: Aboriginal heritage is over 60,000 years old (Rasmussen et al., 2011) whereas the immigrant population is an ongoing addition to Australian multiculturalism. Significance of association between factors was measured using chi-square tests and significance was set at 5%. All calculations were performed using SPSS V20.
Results
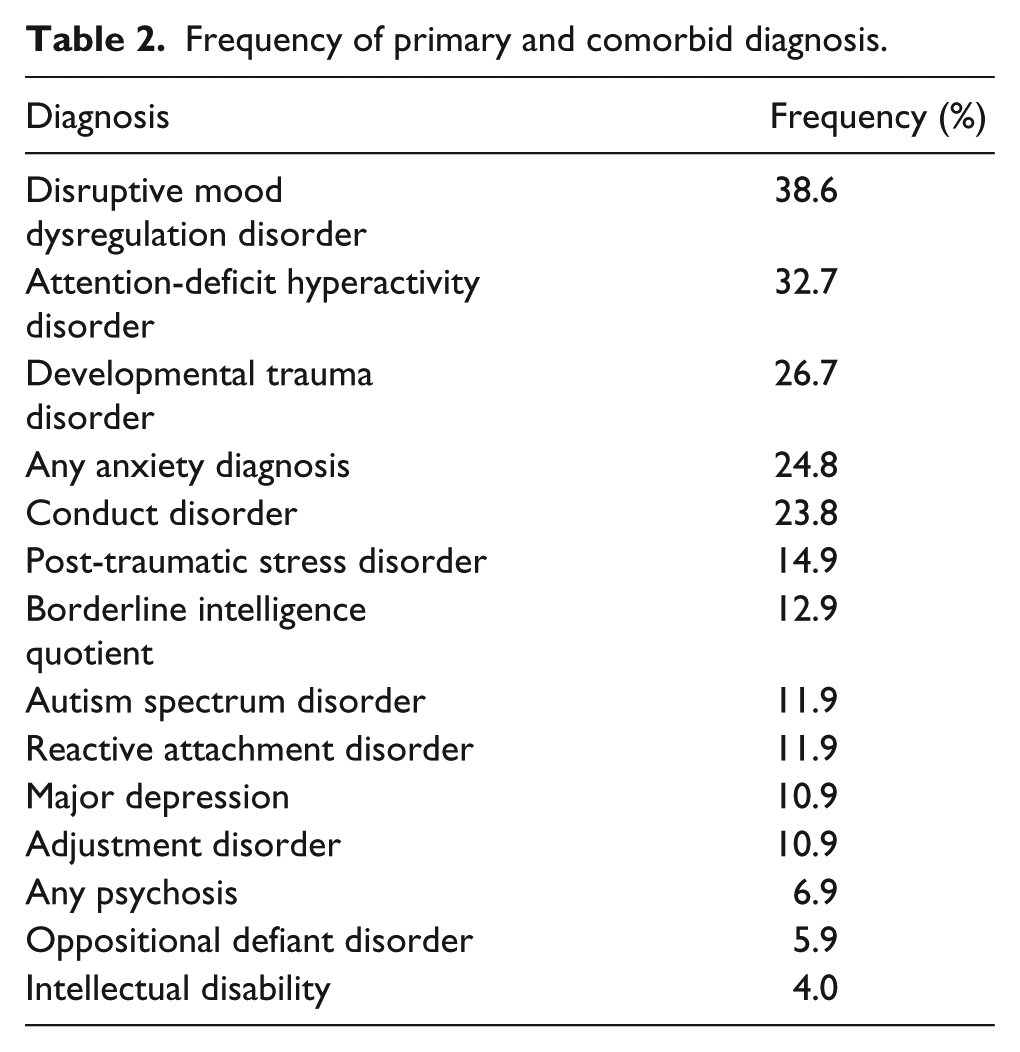
One hundred and one records were identified as being of patients from a transcultural background. Almost 60% of patients were male with less than half from an Aboriginal background. Those from a non-Aboriginal background belonged to 19 different cultural entities (see Table 1), the most common sub-group being of Asian and European heritage. The most common diagnoses were of children with disorders of emotion regulation and externalizing disorders. For most of the patients, more than one primary and comorbid diagnosis was entertained. The most common primary and comorbid diagnoses were disruptive mood dysregulation disorder (DMDD; 38.6%), attention-deficit hyperactivity disorder (ADHD; 32.7%) and developmental trauma disorder (26.7%). DMDD was diagnosed as a comorbid condition in patients with a primary diagnosis of conduct disorder (CD), oppositional defiant disorder (ODD) and developmental trauma disorder (see Table 2). All four children from an Indian background had an autism spectrum disorder (ASD). A significant association was observed between being male and having both CD (p < .005) and ASD (p < .005).
Demographic characteristics and cultural background of patients from a CALD background who attended CAMHS from 2013 to 2017 (N = 101).
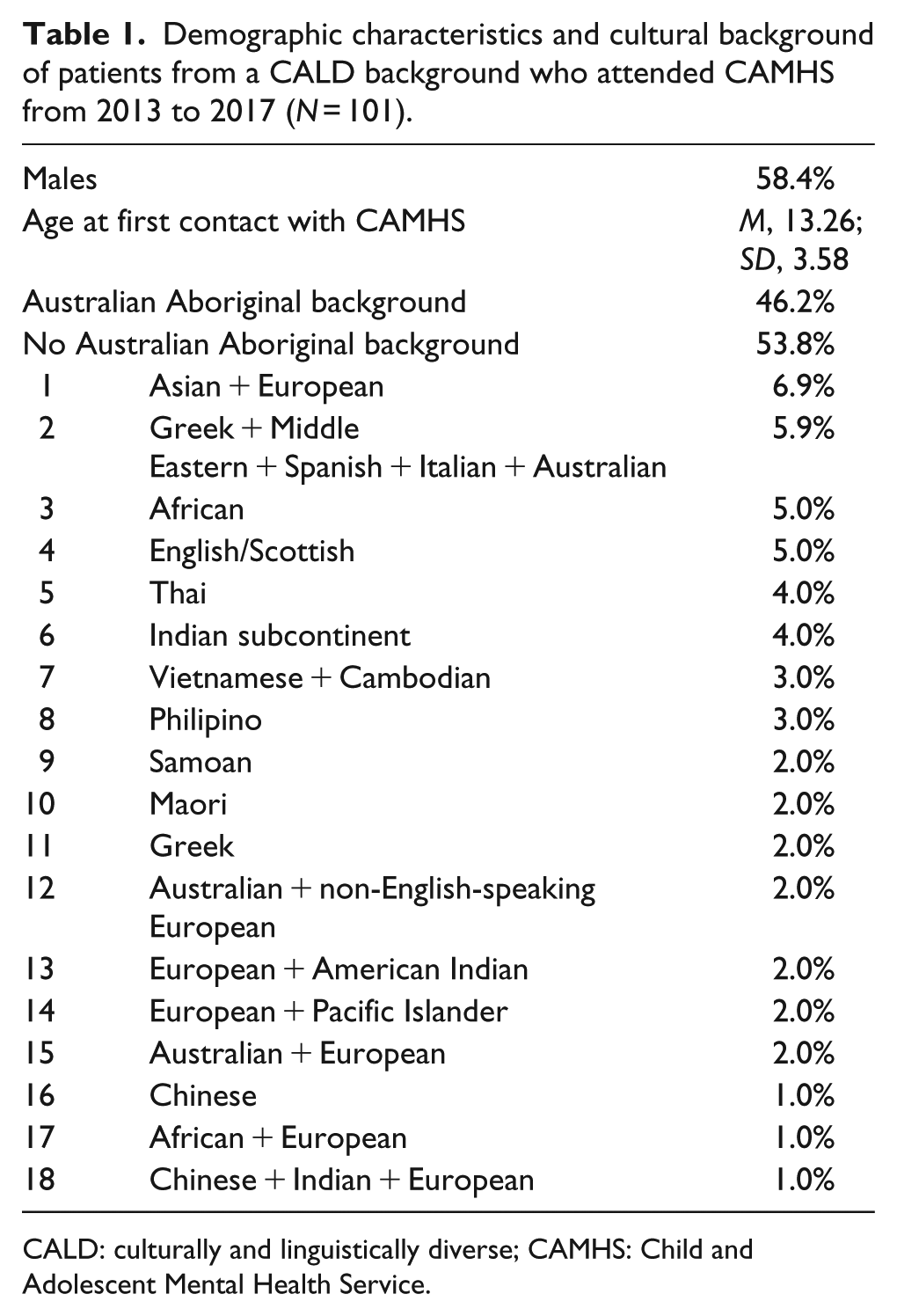
CALD: culturally and linguistically diverse; CAMHS: Child and Adolescent Mental Health Service.
Frequency of primary and comorbid diagnosis.
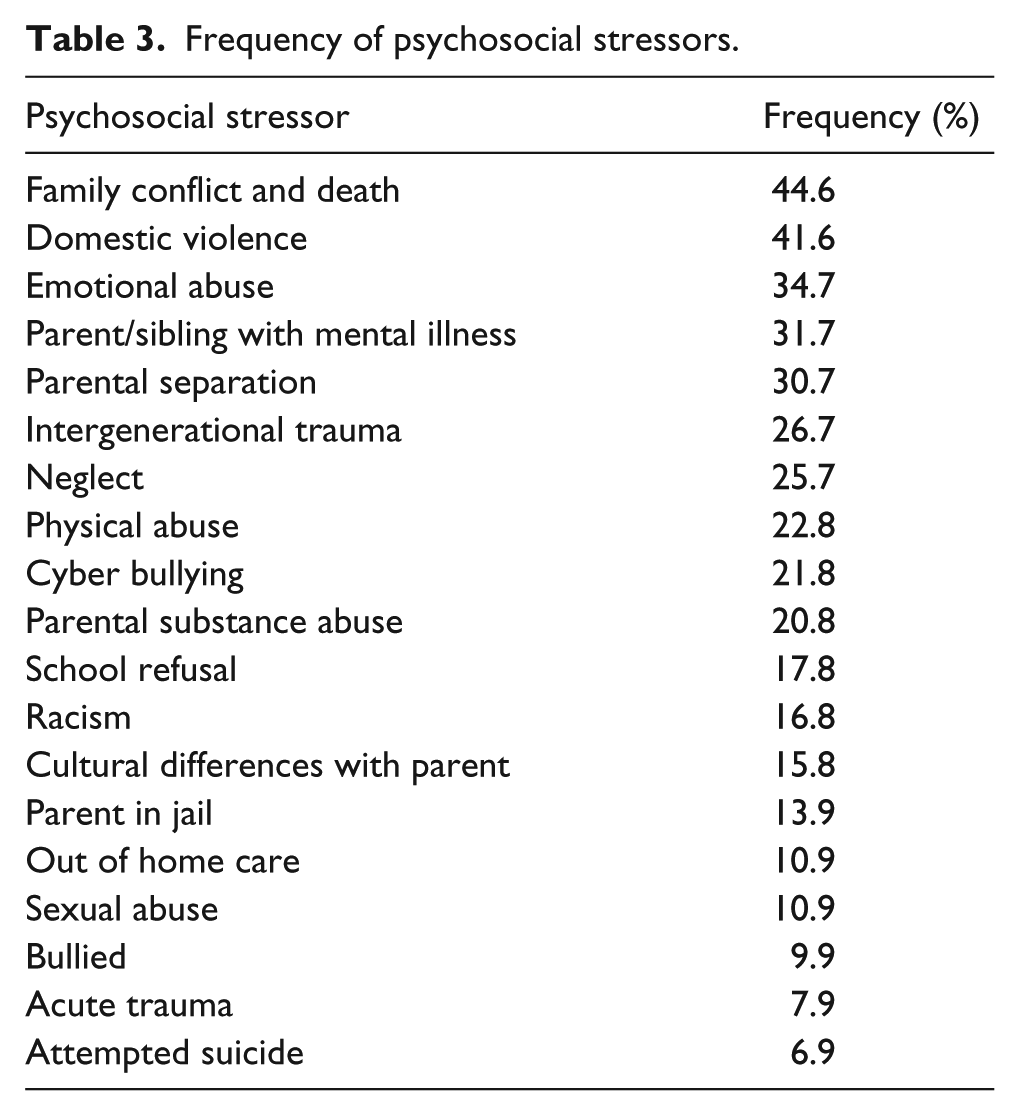
The most common psychosocial stressors were family conflict and death (44.6%), domestic violence (41.6%) and emotional abuse (34.7%; see Table 3). Females were more likely than boys to be sexually abused (p < .001). Associations between psychosocial stressors and cultural background are given in Table 4. ‘Parent in jail’ and ‘domestic violence’ were very significantly associated with having an Aboriginal background (p < .005). ‘Cultural differences with parent’ was significantly associated with a non-Aboriginal background (p < .005). Except for CD which was significantly associated with having an Aboriginal background (p < .005), no other diagnosis was significantly associated with an Aboriginal or non-Aboriginal background.
Frequency of psychosocial stressors.
Association between psychosocial stressors and cultural background.
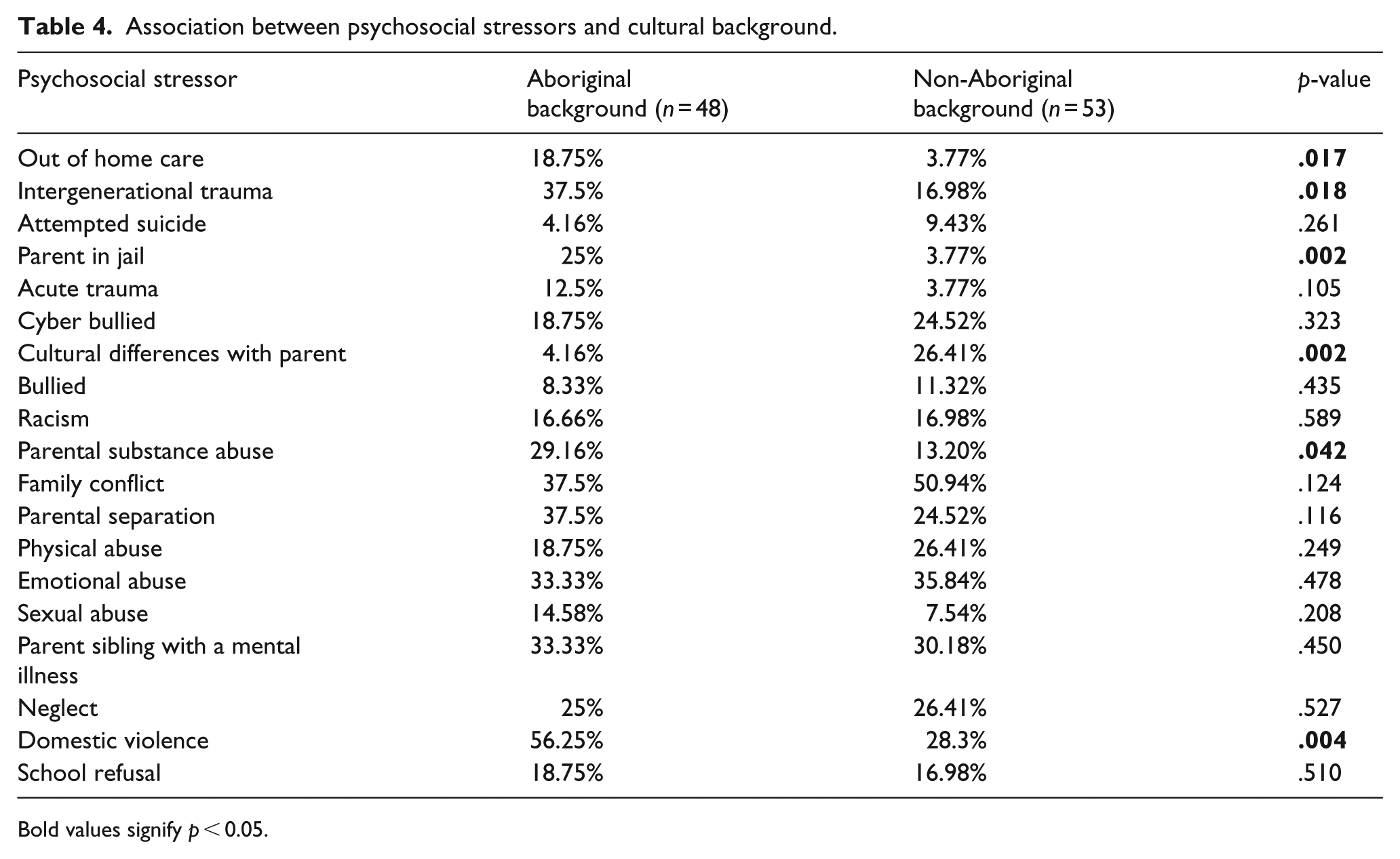
Bold values signify p < 0.05.
Discussion
This study shows the transcultural profile of children attending the CAMHS in Gippsland. Aboriginal children made up the overwhelming majority among those with a culturally diverse background. Nonetheless, the vast array of clients’ cultural make-up gives an indication of the complexities that exist in this field. For instance, a previous study suggested that when culturally diverse patients were matched with clinicians from a similar cultural background, outcomes tended to be better (Ziguras, Stankovska, & Minas, 1999). However, this approach becomes rather challenging in settings where there are close to 20 different types of cultural entities despite more than 50% of overseas born clinicians.
Diagnoses
The assessment, understanding, diagnosis and treatment of children presenting with severe anger and irritability is a hotly debated clinical issue in child psychopathology (Axelson, 2013; Leibenluft, 2011). DMDD, which is a recent addition to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5), was a comorbid diagnosis in the largest number of cases (37.6%). This is in contrast to the epidemiological studies on this disorder, which suggest that it is uncommon after early childhood (Copeland, Angold, Costello, & Egger, 2013). In this study, a diagnosis of DMDD was entertained for a number of patients who had significant difficulties with emotional regulation. These children had primary diagnoses of CD, ODD, ADHD and developmental trauma disorder and many of them had experienced adverse events in their childhood. The current criteria for externalizing disorders do not capture the emotional and mood component of their presentation (Burke et al., 2014), thereby making it necessary to add a comorbid diagnosis as exemplified in this study. It is possible that some of these patients were at a transition point where the impact of early childhood trauma manifested as significant dysregulation of mood (Etain, Henry, Bellivier, Mathieu, & Leboyer, 2008). Longitudinal studies of DMDD indicate that these conditions could develop into personality disorders in young adulthood (Copeland, Shanahan, Egger, Angold, & Costello, 2014).
Interestingly a primary diagnosis of developmental trauma disorder was entertained in 25% of the cases. This is not a recognized diagnosis according to DSM-5 or International Classification of Diseases, 10th Revision (ICD-10) (Schmid, Petermann, & Fegert, 2013) although there is a strong push for its inclusion (Van der Kolk, 2017). All the cases of selective mutism (SM) seen by this CAMHS service in the past 4 years belonged to the migrant group from a bilingual background (Elizur & Perednik, 2003; Australian Bureau of Statistics, 2018). The diagnosis of SM in migrant children is difficult to differentiate from the ‘silent period’ (Toppelberg et al., 2005). However, this finding replicates those from a number of previous studies, which indicate that SM may be 3–10 times more common in those with an immigrant background (Toppelberg & Collins, 2010). Furthermore, while most immigrant children with English-speaking backgrounds presented with internalizing disorders (Kovacs & Devlin, 1998) such as obsessive–compulsive disorder, anxiety spectrum disorder and depression, children with South Asian backgrounds presented mainly for the assessment of ASD. This may indicate different thresholds for health-seeking behaviour in the different communities.
Psychosocial stressors
This study has shown that high rates of male and female Aboriginal incarceration (Krieg, 2006) and domestic violence (J. Atkinson, 1990) are major social determinants of Aboriginal children’s mental health. Issues related to disconnection from culture and perceived loss of cultural identity were prominent in this group as most of their parents and grandparents were members of the ‘stolen generation’ (McKendrick, 1997). The complex interplay of factors such as traumatic upbringing, parental mental illness, substance abuse, a chaotic home-environment and a cultural heritage that has been gradually eroded by generations of neglect has an impact on the developing brain (Atkinson, 2008; Black et al., 2015; Zubaran et al., 2013).
The impact of trauma in Aboriginal children continues to be a complex clinical and political issue (J. Atkinson, 2002). In Gippsland, children from Aboriginal families have a higher chance of being removed from their family by the child protective services than other Australians (Human Rights and Equal Opportunity Commission, 1997; Victorian Multicultural Commission, 2012). There are generations of Aboriginal children who have lived in out-of-home situations for most of their lives thereby depriving them of necessary parenting skills and a support network to look after their infants and children (Atkinson, 2008; Zubaran et al., 2013). These individuals do not trust the system, who in the name of caring for them have created a cycle of living in out-of-home care with multiple placement breakups and attachment trauma (Brady, 1992; Henry, Houston, & Mooney, 2004). Early intervention strategies for this group need to be overhauled to break the ongoing cycle of trauma and mistrust of the system (Atkinson, 2008; Black et al., 2015; Henry et al., 2004).
The most common non-Aboriginal sub-group was of Asian and European heritage. This is perhaps due to the geographical proximity with Asia and the influx of Asian migration in recent years. Often mixed heritage occurs as a result of the union of an older Australian father and his relatively younger Asian partner. The children in this situation who have mixed European and Asian facial features are seen as unique and face issues about their identity, particularly during adolescence (Stephan & Stephan, 1989). There are a few studies from the United Kingdom and the United States that focus on similar issues faced by those of African–European mixed heritage (Choi, Harachi, Gillmore, & Catalano, 2006; Milan & Keiley, 2000; Rockquemore & Laszloffy, 2005).
The phenomenon of differential acculturation (Ying & Han, 2007) was evident in migrants, refugees and children of mixed heritage. Differential acculturation happens when the second generation assimilate to the dominant culture earlier than their parents thereby causing a cultural gap in the family (Ying & Han, 2007). Children in rural and remote areas are almost forced to integrate and assimilate with the local culture unlike their parents who have come to the local area for work and mix with people of their own background out of work. They strive to maintain their lost culture by joining cultural groups in the metropolitan area where they would go during weekends to socialize and celebrate their cultural heritage through food and language (DiNicola, 1998). Their children then constantly face two cultural entities while growing up (Toppelberg & Collins, 2010). While in the metropolitan areas there are many children from immigrant backgrounds, this is seldom the case in rural areas. The pressure to assimilate and integrate is hence more pronounced for the children than their parents. This leads to differential acculturation and is likely to cause family conflict (Toppelberg & Collins, 2010). To complicate matters further, children often shun their mother tongue and indirectly force their parents to speak in English which may not be the parent’s language of preference for emotional communication (Bhugra, 2004; Rothe, Tzuang, & Pumariega, 2010; Toppelberg & Collins, 2010). This study therefore concurs with previous reports (Rothe et al., 2010) by showing that there is a possibility that some of the linguistic nuances needed to manage adolescents facing complex issues may be difficult in bilingual groups of this type.
Limitations
This study has some limitations. Owing to the retrospective nature of the study and the use of file review as the methodology, the quality of the workup and formulation could differ between clinicians. Recruitment was based on the recall of clinicians, which may not be reliable. Moreover, it is possible that some clinicians may not have considered cultural background as essential and hence may not have entered those details in the case notes. There were also a few clinicians who left the service during the study period. Some of their patients would also have been missed in the study although it is likely that those patients would have been picked up by other clinicians who are currently still with the service.
Conclusion
Cultural diversity seen in this study provides a snapshot of Australian cultural diversity and the challenges faced by children from different cultural backgrounds while adjusting in a rural and remote area. A broad-based formulation and cultural awareness by the clinicians of these factors can provide a better insight into the current predicament of these children. This could not only guide better management plans for individuals but also inform public health policies for primary prevention and early intervention.
Footnotes
Acknowledgements
The authors would like to thank the team from the Child and Adolescent Mental Health services of Latrobe Regional Hospital.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.