
Abstract
Background:
There is not enough information regarding the participation in the working life of the patients with schizophrenia in Turkey.
Aims:
The aim of this study was to examine the occupational experiences of patients with schizophrenia before and after the illness and to investigate the factors that predict work participation.
Methods:
The data on occupational life of the patients with schizophrenia, which were treated as outpatients in six different centers, were examined. The rates of participation in working life before and after the disease were evaluated. Patients with and without occupational life history after the disease were compared in terms of demographic characteristics. Factors predicting participation in work life after the disease were analyzed by logistic regression analysis.
Results:
Out of the 587 patients evaluated in the study, 73% were males, 73% were single, the mean age was 42, mean level of education was 9 years and the average duration of illness was 18 years. The duration of the employment before the disease was higher than that after the disease regarding expected working time. The rate of employment was 11% currently, 14% in the last year, 62% after the disease and 83% for the lifetime. While the factors that predicted to be in working life after the illness were male gender (odds ratio (OR) = 2.9), diagnosis of schizoaffective disorder (OR = 2.6), high level of education (OR = 1.2) and employment history before the onset of the illness (OR = 1.0), only the shorter duration of illness (OR = 1.1) predicted the current working status when the gender variable was excluded.
Conclusion:
Rate of employment of patients with schizophrenia living in Turkey was low as in other countries. Good premorbid functioning seems to determine participation in occupational life after the illness.
Introduction
Schizophrenia is the disease with the highest rate of functional loss among serious mental illnesses (Wewiorski & Fabian, 2004). In patients with schizophrenia, dysfunctions of self-care, independent living, social relationships and working life are so prominent that they are among the diagnostic criteria (American Psychiatric Association [APA], 1994). Despite all treatment interventions, functional impairment in schizophrenia is almost sustained lifelong at certain levels (Mueser, Deavers, Penn, & Cassisi, 2013). Functional impairment in schizophrenia manifests its exact result by not being able to get a job or quitting the job. The participation in work life of the patients is generally very low, reported as 10%–30% by the studies conducted in different countries (Evensen et al., 2015; Gaite et al., 2002; Lu et al., 2018; Marwaha & Johnson, 2004; Marwaha et al., 2007; Mueser, Salyers, & Mueser, 2001; Salkever et al., 2007; Yang et al., 2013). The participation in working life of the patients with schizophrenia may vary from country to country and even from region to region in the same country depending on the region they live in and the support provided to them (Drake et al., 1998; Marwaha et al., 2007; Yang et al., 2013). The employment rate of the first episode patients is relatively high yet decreases in the proceeding years. While employment rates in the healthy population do not change much over the years, it is observed that this rate decreases in patients with schizophrenia (Marwaha & Johnson, 2004). These data suggest that schizophrenia patients constitute a significant cost for both families and the health system (Carmona, Juan, Tania, & Emilio, 2017; Knapp, Mangalore, & Simon, 2004).
In studies investigating the employment rate of the patients with schizophrenia, it is noted that there is no standard method for determining the employment (Marwaha & Johnson, 2004). Some studies evaluate the working life after the illness (AI), some report the current employment rate and others give employment rates in the last 1 month or the last 1 year (Kinoshita et al., 2013; Vauth et al., 2005). The qualifications of the works can be changed according to the studies. Some of them only include competitive works, while others considered both competitive and supported employment together (Carmona et al., 2017; Evensen et al., 2015). The duration of work also varies. While some studies consider working for at least 1 day as participating in working life, others can set a limit of at least 1 week or 1 month (Campbell, Bond, Drake, McHugo, & Xie, 2010; Carmona et al., 2017; Catty et al., 2008; Martini et al., 2018). Moreover, full-time or part-time employment appears to be another criterion (Luciano & Meara, 2014; Rosenheck et al., 2006). Regardless of the criteria adopted by the studies, the employment rates of the patients with schizophrenia were found to be very low compared with the average population. In the studies examining the working life in schizophrenia, there is no information about the employment rate of the patients before the onset of the illness. Knowing this experience can be meaningful in understanding the effect of the illness.
Many studies have reported that work performance is associated with negative symptoms and cognitive impairment for this group of patients and that because of these symptoms they have never been involved in working life or that they could work only for short periods of time (Erickson, Jaafari, & Lysaker, 2011; Lexen, Hofgren, Stenmark, & Bejerholm, 2016; McGurk, Mueser, Harvey, LaPuglia, & Marder, 2003; Mueser et al., 2001; Patel, Jayatilleke, Jackson, Stewart, & Mcguire, 2014; Tsang, Leung, Chung, Bell, & Cheung, 2010) The high level of education, young age, the less number of attacks, a previous successful working life, adequate functioning and attending rehabilitation services are considered as the predictors of participating in working life of the patients with schizophrenia (Bond & Drake, 2008; Carmona et al., 2017; MacEwan & Athawes, 1997; Marwaha et al., 2007; Mueser et al., 2001; Rosenheck et al., 2006; Tsang et al., 2010).
Occupational rehabilitation studies (vocational training, sheltered workplaces, supported employment and individual placement, temporary employment, job clubs, etc.) are carried out to eliminate the disadvantages of unemployment in patients with schizophrenia. With these opportunities, patients can get into a job in significant ratios and stay in working life in parallel with the qualifications of the support given to them. Supported employment consistent with the patient’s individual capacity is among the main components of the long-term social therapy (Becker, Whitley, Bailey, & Drake, 2007; Kopelowicz & Liberman, 2003; Liberman, 2008/2011).
The employment rate of patients with schizophrenia in Turkey was reported to be between 10% and 33% in cross-sectional studies (Belli et al., 2007; Kaytaz, Abut, & Yıldız, 2017; Şaylan, Alptekin, Akdemir, Tetik, & Korb, 2004; Yıldız, Yazıcı, & Böke, 2010). In a study examining the patients’ working life, working duration of the patients before the illness (BI) was longer than the duration AI (Kaytaz et al., 2017). It is seen that the illness strictly detaches individuals from working life.
We aimed to answer the following questions with this study:
What are the employment rates before and after the onset of the illness of patients diagnosed with schizophrenia and schizoaffective disorder in Turkey?
What are the predictors of participating in working life for the patients who have worked AI?
Methods
Participants
The study was carried out with patients treated in psychiatric units in six different cities (Kocaeli, N = 163; İstanbul, N = 101; Bursa, N = 100; Kayseri N = 101; Sivas, N = 101 and Niğde N = 100) between 1 January and 20 May 2018. Patients who were diagnosed with schizophrenia or schizoaffective disorder according to Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013), followed up with this diagnosis for at least 2 years, were between 18 and 70 years of age, and gave consent to participate were accepted to the study by random sampling method. Patients with mental retardation, dementia, autism spectrum disorder, epilepsy, Parkinson’s disease and other diseases that cause disability, and those who have problems in Turkish language preventing communication were excluded from the study.
Ethical approval of the study was obtained from Kocaeli University Non-Invasive Clinical Research Ethical Committee (KÜ GOKAEK 2018/135). Informed consent was taken from all of the participants. The sociodemographic and clinical data form was filled by the interviewers during a 20 minute interview with the patients. Forms gathered from different centers were checked concerning the reliability of the data. Forms with inconsistent, suspicious or unanswered questions or with two choices marked for one question, and of patients who did not meet the inclusion criteria were excluded from the evaluation.
Socio-demographic characteristics and clinical information form
Socio-demographic characteristics and clinical information form (SDCCIF) includes the patient’s sociodemographic information, information about family (income, level of support to the patient), illness-related information (diagnosis, onset of illness, number and duration of hospitalization) and information about the working life (working experience, total duration of working BI and AI, number and qualifications of the jobs, the total expected working time after 18 years of age, the patient’s current and for the last 1 year working status and the patient’s health insurance).
The patient’s work experience was evaluated in two groups as BI and AI. ‘Total working time before and after the illness’ was calculated as total time worked as insured or uninsured. Having experience at a workplace for a person was bound by the condition that they work for at least 1 day in that institution. Because of our assumption that the working duration of the patients might be short, the time was recorded in days. The expected age for starting work was set as 18 since it was indicated in Turkish Labor Law No. 4857 (Turkish Labor Law (İş Kanunu), 2003).
The status of the working of the patients was evaluated as ‘temporary or regular job’. Among the patients who worked in more than one work, their essential main work is determined and its characteristics were recorded. Temporary jobs were accepted as works that were not continued regularly, which were not connected to any institution, for example, marketing, peddling, an agricultural laborer, sheepherding, shoemaking and construction. In addition, workers who were employed in permanent labor positions for an indefinite period with employment contracts were also included in the category of temporary workers. Regular jobs were accepted as working in blue collar and white-collar jobs continuously for at least six months regardless of whether they are insured in a certain institution, for example, craftsmen, technicians, drivers, engineers, furniture masters and welders. The employment status was used to express the current working situation and classified as ‘not working’, ‘working’, ‘normally retired’ and ‘retired due to disability’.
Furthermore, the statement ‘employment status in the last one year’ was used to find out the position of the patient’s jobs who have worked in the last year and grouped as ‘temporary jobs’, ‘assisted works’, ‘disabled position’ and ‘normal position’. Disabled position refers to the full-time working on the positions of public or private sector reserved only for disabled persons. The statement of ‘assisted work’ was defined as working along with the families or relatives of the individual, with the help of the co-workers and the employer, and usually part-time work, without any insurance or fee. ‘Temporary/day works’ was defined as mentioned above.
Statistical analyses
Descriptive analyses and bivariate tests were carried out using the Statistical Package for the Social Sciences version 22. Using chi-square tests for categorical outcomes and t-tests for continuous outcomes, we analyzed the association of employment with various sociodemographic variables. These correlates were the level of education, age, gender, marital status, age at illness onset, duration of illness, type of illness, number of hospitalizations, the total number of hospitalization days, work history and work days BI. Logistic regression was then used to identify explanatory variables independently associated with employment using the ‘enter’ method, in which independent variables associated with employment on univariate analyses at the p ⩽ .15 level of significance.
Results
A total of 666 patients participated in the study. A total of 79 patients’ forms were excluded from the study because of missing or unreliable information. The demographic and clinical features of 587 patients were analyzed using descriptive statistics. Patients’ sociodemographic information are given in Table 1.
Sociodemographic characteristics of the patients (schizophrenia = 527, schizoaffective disorder = 60).

Per capita income in the household: the total monthly income of the patient and the people with whom they live together divided by the number of people in the home.
Includes never married and divorced or separated.
Family support: determined by the clinician’s opinion.
Professional status: a white collar for civil servants and a blue collar for workers.
Table 2 shows the characteristics of the patients’ employment status BI and AI.
Data about the occupational life of the patients (N = 587).

BI: before the illness; AI: after the illness.
Expected working time after 18 years of age (by the law), computed as subtracting 18 from the patient’s current age.
The level of education, gender, diagnosis and duration of the illness was significantly different in patients with working history when compared with the patients without working experience AI. Comparison results are given in Table 3.
Comparison of the demographic characteristics according to the working experience after the illness.
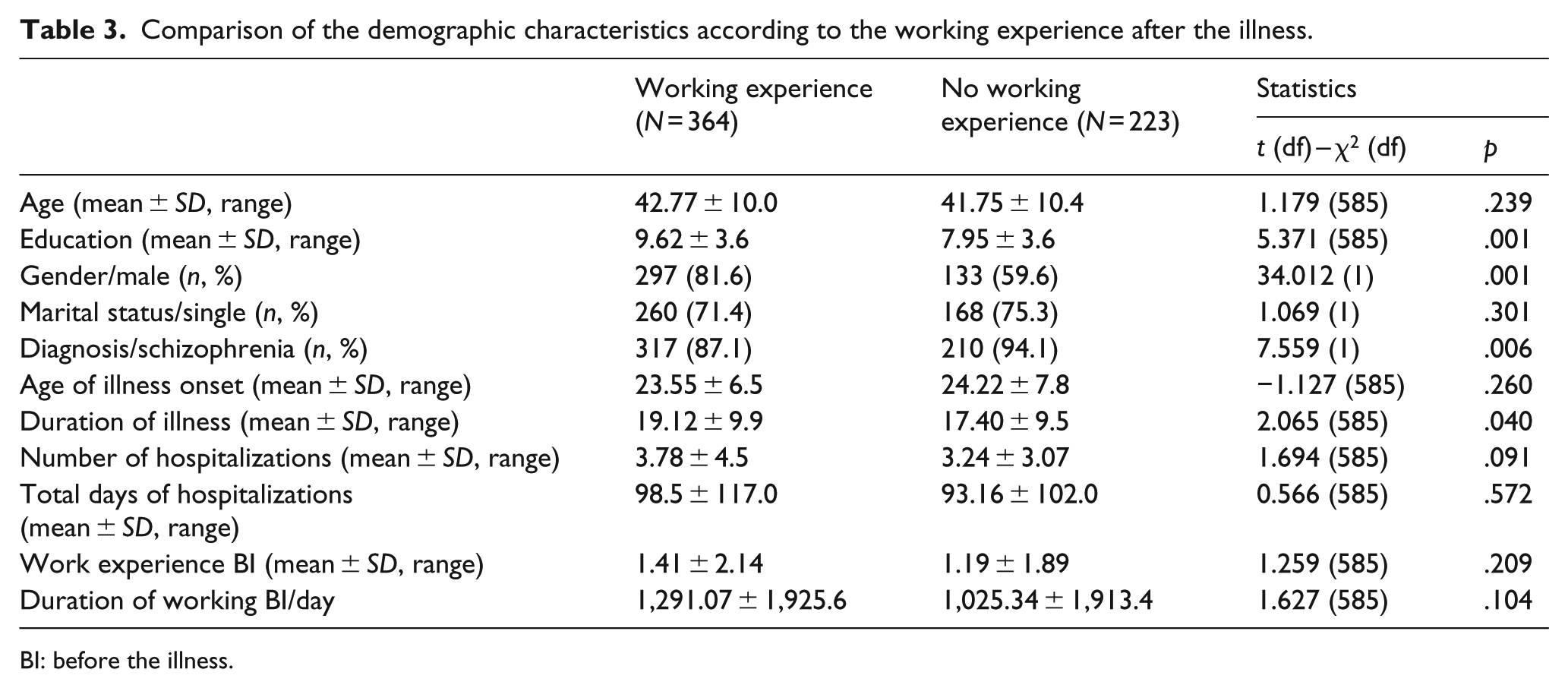
BI: before the illness.
To investigate the factors predicting to participate in working life AI, the variables that were significant at the level of p < .15 were taken into the regression analysis. Logistic regression analysis (Hosmer and Lemeshow Test, χ2 = 10.978, df = 8, p = .203) results are given in Table 4. Statistically significant predictors were found as a high level of education, male gender, having schizoaffective disorder diagnosis and longer duration of the illness. As the fact that majority of the patients were men and that women were less involved in working life due to their role as housewives could be explained with socio-cultural characteristics, the analysis was repeated by subtracting the gender variable. In that case, ‘working duration before the illness’ was added to the education year, diagnosis and the duration of the illness variables.
Logistic regression analysis on the predictors of participating in working life after the illness (N = 364).
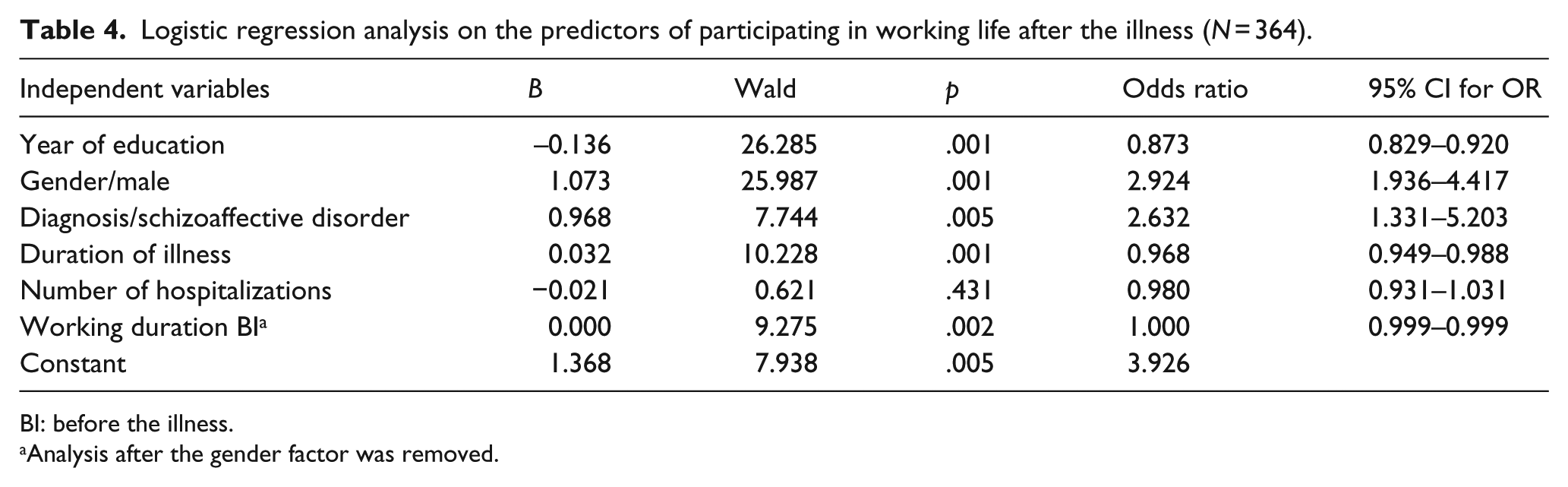
BI: before the illness.
Analysis after the gender factor was removed.
Patients who were working at the time of the interview (N = 66) and those who did not (N = 500) were compared regarding demographic characteristics. In this comparison, we set 18–65 years as working age range and excluded the patients who completed the working life in an average time period and retired. Young age, male gender, higher education levels, shorter duration of hospitalization, lower number of hospitalizations and lower duration of hospitalization were significantly different among working patients. Comparison results are given in Table 5.
Comparison of the demographic characteristics of currently working and non-working patients (age range 18–65).
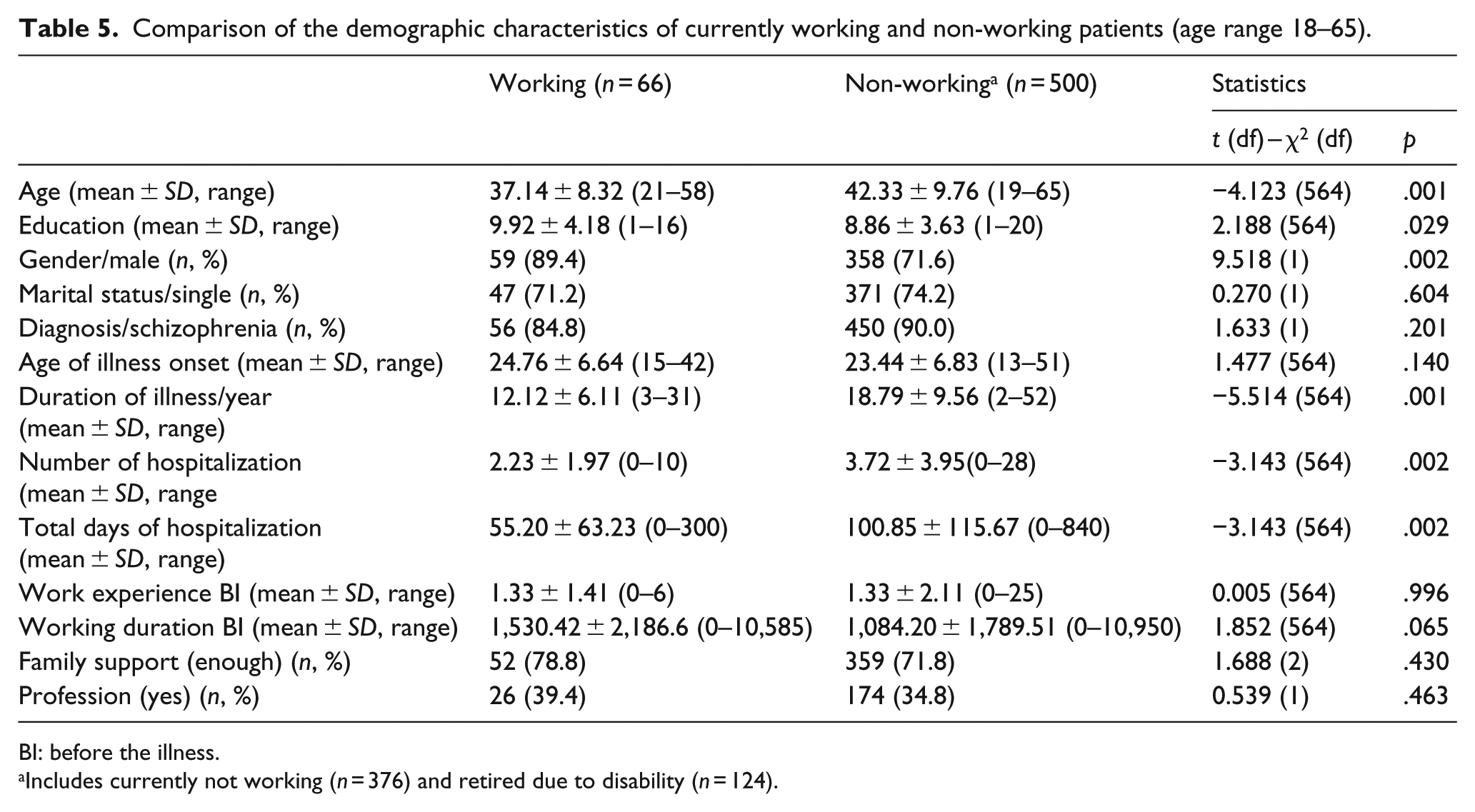
BI: before the illness.
Includes currently not working (n = 376) and retired due to disability (n = 124).
To investigate the factors that predicted to be currently working life, the variables that were significant at the level of p < .15 were taken into the regression analysis. Since the correlation coefficient between the number and duration of the hospitalization was found as rs = 0.90, only the number of hospitalizations was included in the analysis. The results of the logistic regression analysis (Hosmer and Lemeshow Test, χ2 = 7.764, df =8, p = .457) are given in Table 6. Male gender, shorter duration of illness and a smaller number of hospitalizations were found as significant predictors. After the gender variable was subtracted from the analysis, the only remaining predictor was found to be a shorter duration of illness (OR = 1.07).
Logistic regression analysis on the predictors for those currently working.
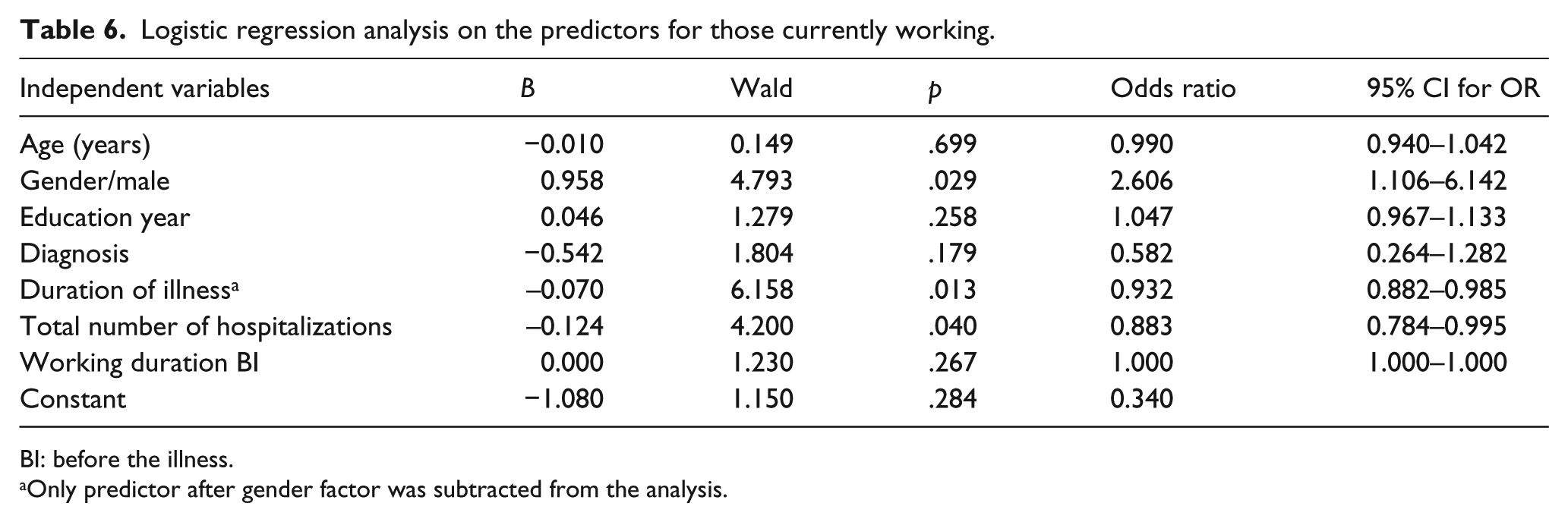
BI: before the illness.
Only predictor after gender factor was subtracted from the analysis.
Discussion
This study is the first multicenter study that examines the working life of patients with schizophrenia in Turkey. We found that only 3% of the patients completed their expected working period and 21% had retired due to disability. The proportion of patients with working life in the last year was 14%, and this rate was 11% during the interview. It is understood that some of the patients who get into a job have left their jobs in a short time. Employment rates of patients both in current and last year are like the results of the national and international studies (Belli et al., 2007; Evensen et al., 2015; Marwaha et al., 2007).
While the rates of working experience BI and AI were the same (62%), the duration of working life decreases significantly AI. Patients’ duration of working BI and AI was very close. It is understood that patients who had worked 55% of the expected working time BI (6 years), worked only 19% of the expected working time AI (18 years). At this point, it is seen that the disease has a significant negative impact on working life of the patients.
Factors that predict patients to be in working life AI were examined in two ways. In the first one, the factors that predicted to have a working life at least once AI were examined. In the second, the factors that predict to be currently working were investigated. The level of education (high), gender (male), diagnosis (schizoaffective disorder) and duration of the illness (long) were found to be the predictors of working AI (Table 4). The data about the male gender as a predictor of working life can be explained by socio-cultural factors. In Turkey, the working life conditions are in favor of men than women. In the general population, 73% of males had at least one work experience in adulthood, while this rate was 35% in females (Turkish Statistical Institute, 2018). Since the same ratio could be applied for the patients as well, the longer duration of work BI became one of the predictors after the gender variable was subtracted from the analysis. Considering the high level of education as it was another predictive factor, it can be said that premorbid functioning was better in these patients. Good premorbid functioning BI is known as a positive indicator for prognosis (Cook & Roussel, 1987; Marwaha & Johnson, 2004; Mueser et al., 2001; Perkins, Miller-Andersen, & Lieberman, 2006). Having higher education may also have raised the chances of finding a job because of a diploma with education (Mueser et al., 2001). It has been reported in many studies that the level of education and working experience BI are predictors of the working life in schizophrenia (Catty et al., 2008; Lauber, Rossler, & Muller, 2007; MacEwan & Athawes, 1997; Marwaha et al., 2007; Mueser et al., 2001; Russinova, Wewiorski, Lyass, Rogers, & Massaro, 2002; Tsang et al., 2010).
In this study, psychopathology levels of the patients were not evaluated. Although there are studies showing that negative symptoms and cognitive impairments negatively affect the working life in schizophrenia (Lexen et al., 2016; Ventura, Hellemann, Thames, Koellner, & Nuechterlein, 2009), working life may be more affected by social, cultural, and economic conditions; labor acts, disability compensations; supported employment opportunities, rather than by varying levels of psychopathology (Bond & Drake, 2008). In a multicenter study in Europe, it was shown that the psychopathology levels of the patients were not correlated with the employment rates (Marwaha et al., 2007). However, it is known that recent employment rates are directly related to the symptoms (Rosenheck et al., 2006). In our study examining the employment status of the patients, it was seen that the patients with and without working experience AI were not different from each other regarding the number and duration of hospitalizations considered as the variables that could reflect the psychopathology level of the patients. The duration of the illness was also longer in patients with working experience. It can be said that the number of hospitalizations and total days of hospitalization are not significant variables in terms of the working life AI. It is understood that with the longer duration of the illness, patients had a chance to settle in the job. The age and level of education of the patients with working life AI were higher, the age of onset was slightly lower, and the rate of the male was higher.
Considering the current working status, significant differences were found between the working and nonworking patients. The working patients were mostly males and younger ones. The level of education and working duration BI were higher; duration of illness, number of hospitalizations and duration of hospitalization were lower in currently working patients. As the duration of illness, the frequency of hospitalization, and total duration of hospitalizations reflect the level of psychopathology, and it may also indicate the withdrawal from the normal life and increased disability. It is expected from the patients to have less working experience if they had longer duration of or more frequent hospitalizations (Catty et al., 2008; Honkonen, Stengård, Virtanen, & Salokangas, 2007; Nordt, Lauber, Rossler, & Muller, 2007; Rogers, MacDonald-Wilson, Danley, Martin, & Anthony, 1997). Being a male was a predictor for both working lives AI (OR = 2.9) and current working life (OR = 2.6). Because of the lower rate of females in our study sample, lower expectations concerning working of the females by the society, and having other social roles as housewives, the gender variable was subtracted from the equation, and the analysis was repeated. After the gender variable was extracted, shorter duration of illness (OR = 1.1) was found as the predictor of currently working. While having the diagnosis of schizoaffective disorder was a predictor (OR = 2.6) for participating in working life, it was not a predictor for currently working. The higher level of education was found as a predictor of participation in working life (OR = 1.2), yet it could not predict the current working status. While the longer duration of illness was a predictor of participating the working life AI (OR = 1.0), the shorter duration was a predictor for currently working (OR = 1.1). In Turkey, the unemployment rate (for the age range between 18 and 65) is 10% as reported in March 2018 data (Turkish Statistical Institute, 2018). In our sample, the unemployment rate was 86% when we consider currently working and retired patients as in worker status. It can be concluded that the unemployment rate is 8–9 times more among the patients compared with the normal population. In our study, 65% of the patients were not working, 21% worked but unable to continue and retired due to the illness.
The results of the study indicated that the rate of employment of the patients was meager, and the duration of working was also quite low compared with the working days BI. It was found that the patients spent most of their time (81%) throughout the illness as nonworker, and hospitalized for 3.6 times (96 days) on average. It indicates that a severe workforce loss is seen after the disease. In the management of this illness with prominent disabilities, treatment and rehabilitation services should include coordinated and comprehensive employment services. To reduce the burden of the illness to the individual, family and health care system, supported employment services should be the main component of treatment and rehabilitation. It has been shown that supported employment has an important contribution to the patients in participation to working life and maintaining the job (Burns et al., 2007; Campbell et al., 2010; Cook et al., 2008).
Limitations
The fact that the data in the study were based on the declaration of the patients is one of the important limitations of the study. While questioning the working experience of the patients, no further investigation was conducted whether they were full-time or part-time. Also, we did not evaluate the working life experiences as competitive and non-competitive since protected workplaces, job clubs and supported employment models are not common in Turkey. We also did not evaluate the patients’ residences as rural or urban. It is known that employment rates are high in rural areas compared with urban residents (Yang et al., 2013).
Another limitation was that patients were not questioned for alcohol and substance dependence. Dependence often has a negative impact on working life. In our study, not having alcohol dependence at the time of the interview was an inclusion criterion for our sample. However, it is not possible to exclude the negative impact of the history of dependency on working life with these data. It has also been suggested that alcohol and substance use is not predictive of working life (Bond & Drake, 2008; Tsang et al., 2010). Alcohol and substance dependence rate found as 5%–8% in studies in Turkey (Akvardar et al., 2004; Uzun, Cansever, & Basoglu, 2003). Therefore, the fact that a history of addiction was not questioned in the interview was not thought to have an important effect on the results.
It is recommended that job qualifications can be examined in more detail, and the information obtained from the patients may be verified by relatives or caregivers of the patients or government agencies, which will help to acquire more accurate outcomes. Since the duration of working BI is a predictor of the future working life, the examination of the qualifications of the jobs can also reveal new information.