
Abstract
Background:
Floods are the most common type of natural disaster, which have a negative impact on mental health. Following floods, survivors are vulnerable to develop PTSD (post-traumatic stress disorder), depression, anxiety and other mental health problems.
Aim:
The aim is to study the psychiatric morbidity in the persons affected by floods during December 2015.
Materials and methods:
This study was carried out in Chennai and Cuddalore. In total, 223 persons who were directly exposed to floods were assessed. PTSD Checklist–Civilian Version, Beck’s Depression Inventory, Beck’s Anxiety Inventory and World Health Organization–Five Well-Being Scale (WHO-5) were used in the study. Chi-square test was used to compare the means.
Results:
Overall, psychiatric morbidity was found to be 45.29%; 60 (26.9%) persons had symptoms of PTSD. Anxiety was found in 48 (27.4%) and depression was found in 101 (45.29%) persons; and 11 (4.9%) persons have reported an increase in substance abuse.
Conclusion:
Following disaster like floods, there is a need for better preparedness in terms of basic necessities and medical and psychological assistance, particularly emphasizing the needs of older persons in order to prevent the development of psychiatric problems.
Introduction
Study site
Chennai is the capital of Indian state of Tamil Nadu. Two major rivers flow through Chennai: the Cooum river through the centre and the Adyar river to the south. A third river, the Kortalaiyar, travels through the northern fringes of the city before draining into the Bay of Bengal. Cuddalore is a town, which is the headquarters of the Cuddalore district in Tamil Nadu, situated at a distance of 200 km from Chennai. The Pennayar river runs to the north of the town, while Gadilam river runs across it (Wikipedia.org).
Chennai and Cuddalore have a tropical wet and dry climate. They get the seasonal heavy rainfall from the north-east monsoon. Cuddalore receives heavy rainfall in Tamil Nadu and frequently prone for fluvial floods (Ragunathan, 2005).
Chennai city has a long history of facing the vagaries of nature in the form of cyclones and high intensity rainfall. Chennai has experienced catastrophic flooding in 1943, 1976, 1985, 1998, 2002 and 2005 due to heavy rain associated with cyclonic activity (Comptroller and Auditor General of India (CAG), 2018).
In December 2015, heavy rains and subsequent overflow of the Adyar and Cooum rivers have caused severe flooding and extensive evacuation in Chennai and surrounding areas causing extensive damage to property (Nurullah & Prabhakar, 2015). Alongside heavy rains, indiscriminate discharge of water from the Chembarambakkam reservoir, in excess of inflows burdened the Adyar river, led to floods in the city and suburbs, amounting to a man-made disaster (CAG, 2018). Other areas affected by the heavy rains were Kanchipuram, Cuddalore and Tiruvallur districts, with over 10 million people being affected (Joint Needs Assessment Report of Tamilnadu Floods, 2015).
In India, following disasters like floods, there is unacceptably high morbidity and mortality among the affected population (Carroll, Morbey, Balogh, & Araoza, 2009). The impact of floods on those who experience them can be significant. In addition to economic loss, detrimental short-, medium- and long-term effects on well-being, relationships and physical and mental health are common (Fernandez et al., 2015). Mental health consequences include post-traumatic stress disorder (PTSD); anxiety; depression; suicide; poor psychological well-being and psychosocial distress; increase in tobacco, alcohol and other substance abuse; and an increase in medication usage (Fernandez et al., 2015).
Prevalence of PTSD/PTSD-related symptomatology is found to be increased in flooded areas, which could be responsible for the development of other mental health problems such as depression, anxiety and substance abuse disorders (McMillen, North, Mosley, & Smith, 2002).
Need for the study
In view of extensive damage caused by floods, this study aims to explore the psychiatric morbidity in flood-affected population.
Aim and objectives of the study
The aim is to study the psychiatric morbidity of the affected population in Chennai and Cuddalore during the December 2015 floods.
Method
It is a cross-sectional study. The study was conducted during the month of February 2016 at two places, Chennai and Cuddalore. A total of 223 persons who were affected by floods were interviewed by a team of psychiatrists and psychologist after taking written informed consent. All the rating scales used were translated into Tamil. This was re-translated into English by a person with postgraduate degrees in English who is well versed with Tamil.
The study was approved by Institutional Ethics Committee.
Inclusion criteria
Age: persons above 18 years.
Persons who were directly affected by floods.
Exclusion criteria
Those who did not give consent.
Statistical analysis
Statistical analysis is done using IBM SPSS 24. Means and standard deviation and chi-square test were used for analysis.
Tools used
Semi-structured intake proforma, including details of socio-demographic data and data pertaining to floods.
PTSD Checklist–Civilian Version (PCL-C): The PCL-C is a standardized self-report rating scale for PTSD, comprising 17 items that correspond to key symptoms of PTSD.
Beck’s Anxiety Inventory (BAI): The BAI is a 21-item self-report inventory to assess symptoms of anxiety.
Beck’s Depression Inventory (BDI): The BDI, created by Aaron T. Beck, is a 21-item self-report inventory to assess the severity of depression.
World Health Organization–Five Well-Being Scale (WHO-5): WHO-5 is a scale to measure the subjective quality of life based on positive mood, vitality and general interest. It consists of five items rated on a 6-point Likert-type scale.
Results
Socio-demographic variables
Out of the 223 persons, 50 of them were from Cuddalore and remaining 173 were residents of Chennai; 107 (48%) were males and 116 (52%) were females.
The socio-demographic variables of the sample are shown in Table 1.
Socio-demographic data.

n = number of persons.
General information regarding floods (as per the semi-structured proforma)
Only 36 (16.1%) persons were aware of the forthcoming floods, whereas the remaining 187 (83.9%) had no prior information regarding floods. The source of information about the impending floods was from television and social networking sites like Facebook and WhatsApp.
Most of the persons reported that they did not get immediate help; 136 (61%) persons received help/were rescued only after a period of 2 days to 1 week. Most of the persons received help from friends (45.7%), followed by non-governmental organizations (NGOs) and strangers, relatives and government agencies. Only 2.2% persons reported that they did not receive any help.
When enquired about the emotional reaction following floods, shock was the most common reaction (n = 113, 50.07%) followed by fear (n = 63, 28.3%), disbelief (n = 41, 18.4%) and feeling numb (n = 6, 2.7%).
About 154 (69.1%) people were affected for less than a week, 61 (27.4%) reported to be affected for up to a month and 8 (3.6%) reported to be affected for more than a month.
A total of 176 (78.6%) people had no access to food, 84 (37.7%) had no access to safe drinking water, 189 (84.8%) informed that they did not have electricity and 128 (57.4%) had no access to medicines.
A total of 178 (79.8%) reported that they were not able to take their important belongings with them and 15 (6.7%) reported their belongings were stolen.
Level of water was reported to be less than 5 feet by 114 (51.1%), 76 (34.1%) people reported 5 to 10 feet and 33 reported >10 feet (14.8%); 138 (61.9%) subjects had to evacuate their places of residence because of floods.
When looked into the various ways in which people tried to overcome stress, 121 (54.3%) people were asking others’ help in time of distress, and 48 (21.5%) were trying to help others; 36 (16.1%) people had to shift their place of residence after floods, 52 (23.3%) reported material loss in the form of damage to house and movable properties and 21 (9.4%) had personal loss like death of a family member and injury. Most of them had financial loss.
On enquiry into the perception of the people on how much their life was affected by the floods, 122 (54.7%) of them felt that they were a bit affected, whereas 77 (34.5%) reported that they were severely affected.
Psychiatric morbidity
Three (1.3%) people had a previous history of mental illness before floods. Overall, psychiatric morbidity was found to be 45.29% (n = 101; Table 2).
Age groups and psychiatric disorders.
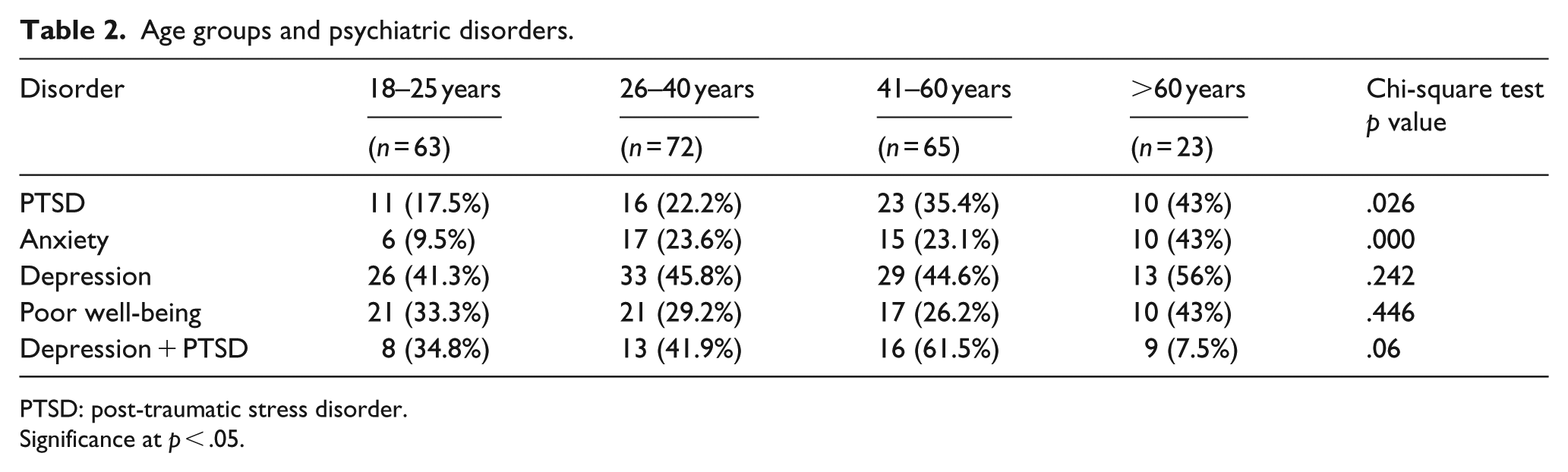
PTSD: post-traumatic stress disorder.
Significance at p < .05.
PTSD
A total of 60 (26.9%) persons had symptoms of PTSD. PTSD was seen to be high in elderly individuals (>60 years) followed by younger individuals (p = .02) (Table 2). PTSD was found to be more in Christians (p = .014), those exposed to higher level of water during floods (>5 feet, p = .005), those who had to evacuate their place of residence (p = .006) and in those who had to shift their place of residence after floods (p = .000). Those who perceived that they were very much affected had symptoms of PTSD when compared to others (p = .00). Persons with PTSD had an increase in substance abuse after floods (p = .034).
Anxiety
Anxiety amounting to a diagnosable disorder was found to be in 48 (27.4%) persons. Elderly people had more levels of anxiety when compared to younger individuals (p = .000). Those who were affected maximum by floods (Tambaram area being the worst affected with floodwater more than 10 feet) had reported more severe levels of anxiety (p = .000). Severe anxiety was found to be more in Christians, followed by Hindus (p = .000). Persons who are widowed/divorced had comparatively more anxiety than married people (p = .27). Shock and fear were the predominant emotions experienced during the floods in people who also had severe levels of anxiety (p = .026). Anxiety was found to be more in those persons who had no access to food, water and basic medical facilities (p = .01). Those who had to evacuate and shift their place of residence had significant levels of anxiety (p = .02). Those who perceived that they were very much affected had symptoms of anxiety when compared to others (p = .00). Anxiety was also found to be higher in those who experienced loss in the form of material (p = .001) or personal (death/injury to a family member) (p = .001).
Depression
Depression was found to be in 101 (45.29%) persons: 24 (10.8%) had mild depression, 28 (12.6%) had moderate depression and 49 (22%) had severe depression. No variations across various age groups and gender differences in depression were seen. Those persons belonging to lower socio-economic status had significant levels (p = .042) of depression. Those who were affected maximum by floods (Tambaram area being the worst affected with floodwater more than 10 feet) had reported more severe levels of depression (p = .014). Depression was found to be more in Christians, followed by Hindus (p = .001). Depression was found to be more in those persons who had no access to food and basic medical facilities (p = .014). Those persons who did not receive help and those in which help was delayed (>7 days) had significant levels of depression (p = .007). Those who had to shift their place of residence had significant levels of depression (p = .007). Those who perceived that they were very much affected had symptoms of depression when compared to others (p = .00). Depression was also found to be higher in those who experienced loss in the form of material (p = .002). Depression was found in those persons who had a history of substance abuse (p = .07) and those who are having family problems (p = .025).
Depression and PTSD
In total, 46 (20.62%) persons had depression and PTSD. It was found to be significantly higher in Christians (18 (78.3%), p = .005), elderly (>60 years, 9 (75%)), those who had no prior information about floods (p = .02) and those in whom shock and fear were the predominant emotions (p = .05).
Well-being
Psychological well-being is assessed by WHO Well-Being Scale. Poor well-being was reported by 89 (39.9%) persons. Those who perceived that they were severely affected (p = .03) and those having substance abuse like alcohol (p = .04) reported poor well-being.
Substance abuse
In total, 27 (12.1%) people have reported to be using some kind of substance like alcohol, tobacco and so on. Out of them, 11 (4.9%) people have reported an increase in substance use. Increase in substance abuse was found in those having symptoms of PTSD (p = .03), anxiety (p = .01) and depression (p = .00); 18 (8.1%) people reported that there is an increase in problems in the family after the floods. Those having PTSD (p = .04) and anxiety (p = .05) reported significant increase in family problems after floods.
Discussion
The present study assessed 223 persons who were affected by the floods in Tamil Nadu during December 2015 for psychiatric problems like PTSD, depression, anxiety, psychological well-being and substance abuse, 1 month after the floods.
Overall, psychiatric morbidity was found to be 45.29% in the present study. Psychiatric morbidity following floods varies broadly between studies from 13% to 87% (Mcmillen et al., 2002).
In India, psychiatric morbidity found in natural disasters (N. Kar, 2010) was estimated to be 80.4% (Orissa super cyclone; G. C. Kar, 2000), 59% (Latur earthquake; Sharan, Chaudhary, Kavathekar, & Saxena, 1996) and 27.2% tsunami in coastal Tamil Nadu (Nambi, Desai, & Shah, 2007).
Factors related to floods
Mental health problems were reported to be more in those who had higher levels of exposure to the floods (Norris Kaniasty et al., 2002), higher flood level in the house (Shirley, Nilkamal, & Meesha, 2001), those who were evacuated (importance of house and place as identity and importance of reintegrating people as soon as possible back into their community; Mason, Andrews, & Upton, 2010), inability to collect possessions and perceived severity of loss and threat (Assanarigkornchai, Tangboonngam, & Edwards, 2004). Those who have experienced financial loss, material loss and personal loss (in terms of bodily injury/death) also reported higher levels of psychiatric morbidity (Bei et al., 2013).
Compared with sustained rainfall in a river catchment leading to flood, victims of flash floods have an increased risk of developing PTSD (Liu et al., 2006). In the present study, depression (p = .01) and anxiety (p = .01) were found to be more in people exposed to flash floods (Chennai) than those exposed to fluvial floods (Cuddalore).
In terms of social support, more support was associated with less severity of symptoms. Social support was a protective factor for mental disorders (Norris, Murphy, Baker, & Perilla, 2004). Those who have positive or proactive behaviours like helping others during floods experienced less severe problems (Bei et al., 2013). During 2015 Chennai floods, adolescents and young adults proactively participated and helped themselves, and those in need and those who received support reported lesser severity of psychiatric symptoms.
In general, children, females and elderly people were at risk of developing mental health problems following floods (Norris, Kaniasty, Conrad, Inman, & Murphy, 2002). A systematic review on the impact of natural disasters on elderly concluded that there is contradictory evidence regarding whether older individuals have a worse or more favourable psychological outcome than younger individuals (Cherniack, 2008). In the present study, elderly persons reported more levels of PTSD (p = .01) and anxiety (p = .00) when compared to other age groups.
Lower socio-economic status is a risk factor owing to loss that they cannot cope with. Low socio-economic circumstances are linked to poor mental health, and impact of floods on mental health is higher in areas of material deprivation (Jones, Gupta, Murphy, & Norris, 2011).
Depression (p = .042) was found to be more in persons belonging to lower socio-economic strata in the present study, while no difference in other disorders was observed.
There could be cultural differences related to the expression of emotions. Among the religious groups, Christians reported to have high levels of PTSD (p = .014), anxiety (p = .00) and depression (p = .001) followed by Hindus. Religious beliefs, cultural aspects and so on might have influenced the above findings (Norris et al., 2002).
Where adequate warning was given, it was a very good factor determining the effect of floods on mental health (Parker, Tapsell, & McCarthy, 2007; Tunstall, Tapsell, Green, Floyd, & George, 2006). Acute stress–related response, if not addressed properly, can evolve to more severe disorders such as PTSD and depression. It is important to monitor these two conditions due to high suicide risk that is associated.
Psychiatric morbidity
Poor mental health status before floods and existing physical health problems were associated with post-event mental health. More severe exposure, female gender, middle age, ethnic minority status, secondary stressors, prior psychiatric problems and weak or deteriorating psychosocial resources most consistently increased the likelihood of adverse outcomes (Norris et al., 2002).
PTSD was found to be more in affected areas (Shirley et al., 2009), which was also seen in the present study. It has been suggested that PTSD or symptoms associated with PTSD could be responsible for the development of other mental health problems such as depression, anxiety or substance disorders. PTSD was found to be more in high exposed areas, lower educational levels and average socio-economic status. Elderly people had more PTSD when compared to younger generation as in the present study. Women are of higher risk of PTSD and depression was significantly associated with PTSD (Galea, Nandi, & Vlahov, 2005). No such difference in gender was seen in this study.
Prevalence of PTSD was 26.9% in accordance with other studies. PTSD prevalence, ranged from 5% to 60% (Cao, McFarlane, & Klimidis, 2003; Kaiser, Sattler, Bellack, & Dersin, 1996), was found in first 1 to 2 years after the disaster. Psychological factors such as neuroticism (McFarlane, 1989), guilt, difficulty concentrating, coping strategies (Benight, Swift, Sanger, Smith, & Zeppelin, 1999), obsessive traits and psychiatric comorbidity were found to be associated with PTSD across studies.
Television viewing has been associated with PTSD after natural disaster (McFarlane, 1988), and the prevalence of PTSD was shown to decrease by one-half in the first 2 years.
Overall, people from the flood-affected areas experienced an increase in depression symptomatology (North, Kawasaki, Spitznagel, & Hong, 2004). The prevalence of depression in the present study was 45.29%. This association was not found in old people. Level of exposure was not associated with depression after the flood.
Contradictory evidence regarding suicide following a flood event
Some studies found increased rates of suicide (Krug et al., 1998), while others found no difference (De Leo, San Too, Kolves, Milner, & Ide, 2013). The present study did not find any increase in suicidal ideation following floods.
Another study reported that greater amounts of time spent volunteering in flood recovery efforts were associated with feelings of belonging and a decrease in suicidal ideation (Gordon, Bresin, Dombeck, Routledge, & Wonderlich, 2011). However, those persons who volunteered to help others during the December 2015 floods reported more sense of belonging and less psychiatric problems.
Groups exposed to flooding events showed higher levels of anxiety when compared to non-exposed groups (Maltais et al., 2000). In the present study, similar findings were seen, wherein the persons exposed to the maximum water levels had more severe levels of anxiety when compared to others (p = .001). Shock and fear were the predominant emotions experienced during the floods in people who also had severe levels of anxiety (p = .026).
Overall, psychological-health- and mental-health-related quality of life was significantly worse in affected areas when compared to non-affected areas. Increase in tobacco, alcohol and other substance use was found post floods.
Difference in psychiatric morbidity in Cuddalore and Chennai
Anxiety (p = .001) and depression (p = .001) were found to be more in those exposed to flash floods (Chennai) when compared to those from fluvial floods (Cuddalore). This could be because of sudden floods, lack of adequate early warning system and unpreparedness of the individuals for the forthcoming catastrophy. People reported poor well-being in Cuddalore when compared to those from Chennai. This may be due to the less available resources and slightly disadvantaged socio-economic status of the residents when compared to their urban counterparts in Chennai.
Acute responses and long-term support are needed to reduce the mental health impacts (Rao, 2004) and it is important to have a well-trained workforce dealing with mental-health-related issues (Diaz, Lakshminarayana, & Sujatha, 2004).
Hence, disaster response should involve the following:
Attempt to prevent the floods where possible (as in case wherein there was a breach in the embankment of an adjoining river; Gaitonde & Gopichandran, 2016).
Better preparedness in terms of basic necessities and medical and psychological assistance, particularly emphasizing the needs of children, women and older people.
Implications
This study suggests that following a disaster like floods, there is an immense effect on the mental and psychological well-being of the affected population. Hence, vulnerable population should be adequately screened, and support should be provided on immediate and long-term basis in order to prevent the morbidity arising from the mental health issues.
Limitations
Some limitations of the study include a sample size and lack of long-term follow-up, as the latter would have thrown insight into the course of the psychiatric illness under study.
Footnotes
Acknowledgements
We want to thank all the participating subjects for taking time to share their experiences with us. We would also like to thank Dr G. Umesh, Assistant Professor, Department of Psychiatry, Sri Muthukumaran Medical College Hospital and Research Institute, Chennai, for his help during the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.