
Abstract
Background:
The caregivers of patients with first episode psychosis (FEP) experience significant distress. It is important to understand their needs to plan adequate interventions for them.
Aim:
The aim of this study was to explore the needs of caregivers of young patients with FEP in India, using a qualitative approach.
Methods:
The study was conducted in two phases. In phase I, a script for conducting focus group discussions (FGDs) with caregivers was developed, based on literature search and expert opinion generated from FGD with mental health professionals. In phase II, five FGDs were conducted with 30 caregivers of young patients with FEP having minimal of 6 participants in each FGD. Data was analyzed using principles of grounded theory.
Results:
Seven broad themes and subthemes of the needs of caregivers emerged from the FGDs. The final themes, which highlighted the needs of caregivers of young patients with FEP, were (in order of ranking) as follows: information regarding treatment, information regarding illness, services provided by the government, optimum quality of care from treatment facility, management of psychosocial issues related to patient’s illness, availability and accessibility of treatment, and identification and recognition of mental health and physical problems in family members.
Conclusion:
Qualitative method was useful to identify the needs of the caregivers of young patients with FEP in multiple domains.
Introduction
Psychotic disorders are one of the leading causes of disability globally. In most of the cases, onset is in younger age groups between 15 and 17 years that makes it essential to intervene early for preventing long-term disability (Kessler et al., 2007; McGorry et al., 2011; Thomsen, 1996). The patients with first episode psychosis (FEP) who receive early intervention have better chances of recovery (40%) in comparison to persons with chronic illness (Goldstein, 1996). The caregivers bear the major burden of getting treatment for these patients. They experience significant distress, anxiety and financial hardships, and have multiple needs due to their caregiving role (Chadda, 2014). The needs of the caregivers having young relative suffering from psychosis for the first time are different from those who are providing care to patients who have a long duration of illness as the expectations and requirements differ with circumstances of life (Carr, 2001). Addressing their needs will not only help in understanding their expectations (social, emotional, economical, etc.) and developing adequate intervention care plans but also will improve the level of functioning of the patient leading to better disorder outcome (Solomon & Draine, 1995; Suro & Mamani, 2013).
Due to lack of adequate resources and dissimilar cultural settings, caregivers of young patients with FEP in India, unlike in high income countries, also take on the responsibility of fulfilling age-specific tasks of completing education and choosing vocation in the absence of well-established community care in the form of support from educational agencies, social workers, vocation, housing and social security benefits (Chadda & Deb, 2013).
Needs of the caregivers of patients with psychotic disorders have been studied mostly by using quantitative scales, on the caregivers of chronic patients, and are cross-sectional in nature. The scales used in these studies are from high-income countries and may not be appropriate for low- and middle-income countries as caregivers’ needs differ across various settings due to differences in the sociocultural context and budget allotted to health sector (Jagannathan et al., 2011). Such a difference in caregivers’ needs can be better understood in qualitative studies. A qualitative approach is useful in tapping a broader range of needs that are specific to the context in which it is used. Studying the needs of caregivers involves probing of sensitive, emotional and personal themes, which is more suited to a qualitative approach (Hiday et al., 2002). Qualitative studies are especially helpful when one intends to generate impressions and develop assessment scales. In a qualitative study on caregiver needs of Indian inpatients with chronic schizophrenia, four main themes were reported: management of behavioral problems, rehabilitation, health needs of caregivers, and problems in social interaction and interpersonal relationships (Jagannathan et al., 2011).
There has been no study assessing the caregivers’ needs of young patients with FEP from India. Therefore, the present study was aimed at assessing caregivers’ needs of young patients with FEP using a qualitative approach.
Methodology
The study was conducted in a tertiary care public funded general hospital psychiatric unit of a medical college in North India. Caregivers of patients aged 15 to 25 years of either gender, diagnosed as schizophrenia, persistent delusional disorder, schizoaffective disorder, other and unspecified nonorganic psychotic disorder (FEP) on International Classification of Diseases–10th Edition, Diagnostic Criteria for Research (ICD-DCR; World Health Organization, 1993), with illness duration of 3 months to 2 years and who were in contact with treatment services for at least 3 months, were included in the study. Caregivers of the patients with any other psychiatric disorder except nicotine and caffeine use, having any chronic medical disease, pregnancy or in the postpartum period were excluded from the study. To be included in the study, caregiver needed to meet criteria of age ⩾18 years, living with the patient for at least 1 year, not having any psychiatric or chronic medical illness and not caring for any other relative with psychiatric or chronic medical disorder. Caregivers could be from either gender. Psychiatric disorder in caregivers was excluded by the Mini-International Neuropsychiatric Interview screen (Sheehan et al., 1998). Chronic medical illness in caregivers was assessed by history and physical examination. The caregivers and the patients were assessed on separate semi-structured questionnaires to assess sociodemographic and clinical characteristics. Written informed consent was obtained from patients and caregivers for participation in the study. Ethics approval was taken from the Institute Ethics Committee.
Procedure
The study was conducted in two phases. In Phase I, the script for conducting focus group discussions (FGDs) with caregivers was developed based on literature search and expert opinion generated from FGDs with mental health professionals (MHPs). A literature search was conducted on the needs and concerns of caregivers caring for their young relative with FEP. The following databases were used – MEDLINE/PubMed, MedIND, Internet, Psychological Abstracts, Indian Journal of Psychiatry, Indian and International mental health journals and back-references to the obtained articles. After a review of the literature, a script consisting of 11 questions was developed about the felt needs of the caregivers. The questions were open-ended in face-to-face ‘conversational’ style and flexible in nature.
Expert opinion was generated by conducting an FGD with MHPs comprising of psychiatrist, clinical psychologist, anthropologist, psychiatric nursing staff, occupational therapist and psychiatric social worker. A written informed consent was taken from the participants before participation. One of the authors (G.K.) moderated it in the presence of two authors (R.V., M.S.). During the FGD, questions from the script were used, and some direction was given when the focus was lost, and probes were used when necessary. At the end of the script set, a general question was posed to every participant to raise any other remaining issue related to caregiving of young patients with FEP that had not been addressed during the discussion. The whole session was audio recorded and lasted for about 2½ hours. The recording was commenced on the entry of the first member of the group and was stopped only after the last person had left so that points, that came up before the formal discussion had commenced and after it was over, were also included. From FGD with MHPs, eight themes were generated, namely, (a) psychoeducation about illness, (b) psychoeducation about treatment, (c) stigma, (d) management of behavioral problems in the patients, (e) need for rehabilitation and employment, (f) information regarding marriage and marital relationship, (g) issues during follow-up sessions and (h) expectations from the government. A revised final script with 11 questions was generated for use in Phase II that incorporated suggestions from the FGD with MHPs (Table 1).
FGD script for caregivers.
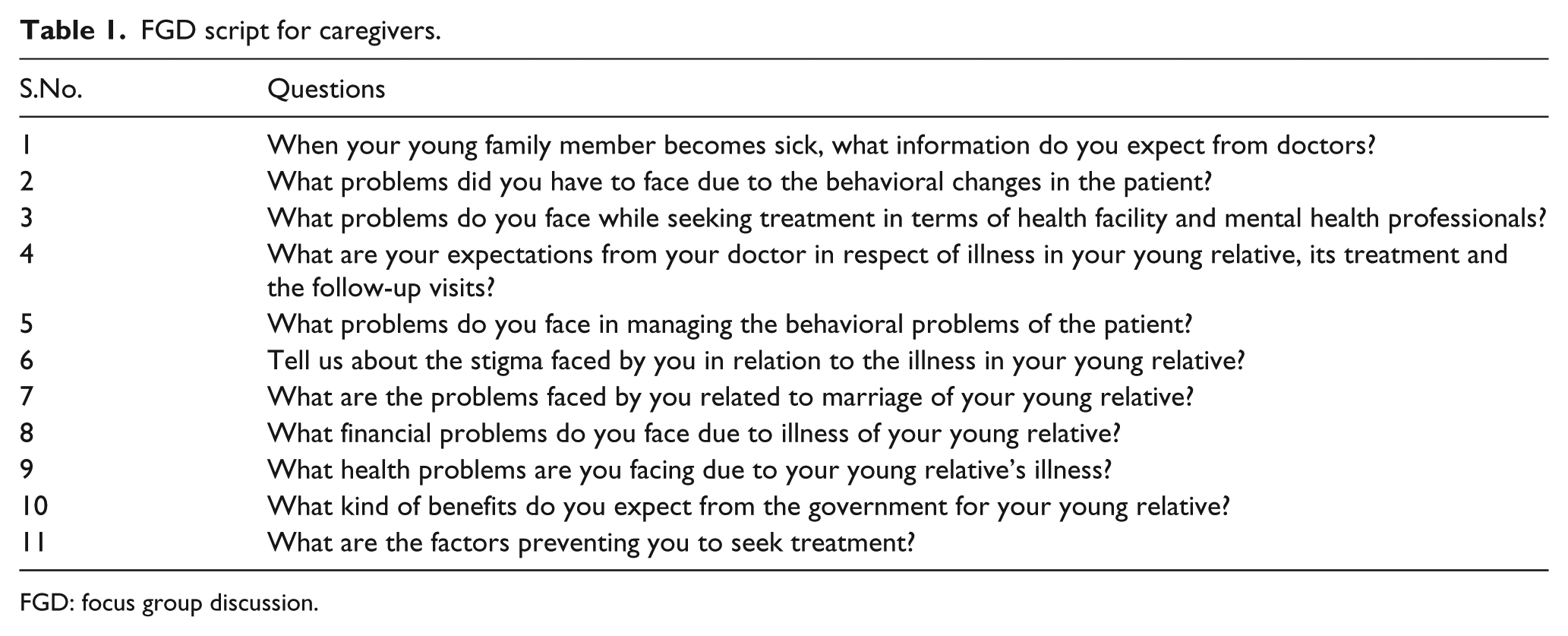
FGD: focus group discussion.
In Phase II, five FGDs were conducted with caregivers of patients with FEP. For any FGD, a minimal number of six to eight participants were included (Morse, 2000). A total of 397 patients were assessed, and only 45 fulfilled the inclusion and exclusion criteria for the study. Subsequently, caregivers of these 45 patients were evaluated for inclusion in the study. Thirty-seven caregivers fulfilled the inclusion and exclusion criteria for the study. Seven caregivers were not able to attend the FGDs, though willing to participate at screening time, due to logistic issues (n = 3), unreachable phone numbers (n = 2) and those arriving late after initiation of FGD (n = 2). Finally, FGDs were conducted with 30 caregivers, with 6 caregivers in each FGD.
Data analysis
The frequencies of sociodemographic and clinical characteristics of the patients and caregivers were tabulated. The data obtained from five FGDs were analyzed using principles of Grounded Theory (Braun & Clarke, 2006). The FGDs were conducted in Hindi. Data were audio recorded and individually transcribed verbatim into written data in Hindi (as spoken by the session participants) by the investigator. The Hindi data were translated into English, one by the investigator and the other by a language translator, both finally approaching a unified final translated English version in consensus for separate FGD sessions.
The English data were then analyzed to identify codes and subsequent themes and subthemes by iteration. The investigators also evaluated and incorporated Hindi data at multiple times for coding wherever found reasonable for appropriate conveyance of the conversational theme. Three authors (G.K., M.S. and A.M.) separately identified the codes, and a consensus was reached before finalizing the codes, themes and subthemes. For the transcript of each question asked during one FGD, open coding was done. Based on the open codes, conceptual codes were assigned by the authors. After conceptual coding, a list of needs was made based on the conceptual codes obtained for each question. This was done for all the questions for all the five FGDs. The needs of the caregivers were then divided into themes and subthemes, and ranked according to their frequency of occurrence in the transcript. Following the technique of iteration, the group went over these themes and rankings several times before finalizing them. In each FGD, the most important theme (based on the frequency of occurrence in the FGD) was given the highest score (equal to the number of times it occurred). If a theme was not represented in a particular FGD, it was given a score of 0 in that FGD. The scores for each theme across the five FGDs were totaled. The final ranking of the themes corresponded to these totals; the theme with the highest total score was ranked as the most important need. The needs under each theme across the five FGDs were listed. A final list of themes and needs under each theme was tabulated for analysis.
Results
Mean age of patients was 19.90 (±2.57) years, ranged between 16 and 20 years. Males comprised 56.7% of the sample with most of the patients being unmarried (90%). Twenty-seven (90%) patients were students, two were unskilled workers and one was unemployed. About two-thirds of the patients (66.7%) were educated up to 10th standard followed by those educated up to 12th (30%), and only one of them was graduate. All the patients who were students had dropped out of the studies after they were affected by illness. Regarding religion, most of the patients were Hindus (93.3%). Mean duration of illness was 12.78 (±6.05) months and the mean duration of treatment was 7.6 (±4.19) months. All the patients were receiving atypical antipsychotic medications, and family history of psychiatric illness was positive in 23.3% of patients. Twenty patients had schizophrenia (66.7%), nine had psychosis not otherwise specified (NOS) (30%) and only one had schizoaffective disorder (3.3%).
Mean age of caregivers was 37.7 (±8.13) years. About two-thirds of the participants were males (63.3%). Most of the caregivers were married (83.3%). The unmarried caregivers were siblings of patients. Regarding occupation, the largest group of caregivers was of unskilled workers (26.7%) followed by homemakers (16.7%), unemployed (16.7%), businessmen (13.3%), farmers (10.3%) and students (6.7%). About one-third of the caregivers were educated up to 5th standard (36.7%), one-fourth of them had studied up to 10th standard and 12th standard (26.7% each) and 10% were graduates. About half of the caregivers (53.3%) were earning INR 10,000 to 15,000 per month. Fifty percent of the caregivers were fathers, and the rest comprised 30% mothers, 13.3% brothers and 6.7% sisters as caregivers.
Themes and subthemes of the needs of the caregivers generated for the FGD are depicted in Table 2. After the data analysis, seven broad themes emerged (Table 3). In order of frequency of occurrence, these were as follows:
Information regarding treatment (26.2%)
Information regarding illness (19.8%)
Services provided by the government (16.4%)
Optimum quality of care from treatment facility (16.1%)
Management of psychosocial issues related to patient’s illness (12.8%)
Availability and accessibility of treatment (5.1%)
Identification and recognition of mental health and physical problems in family members (3.3%).
Themes and subthemes in FGDs.
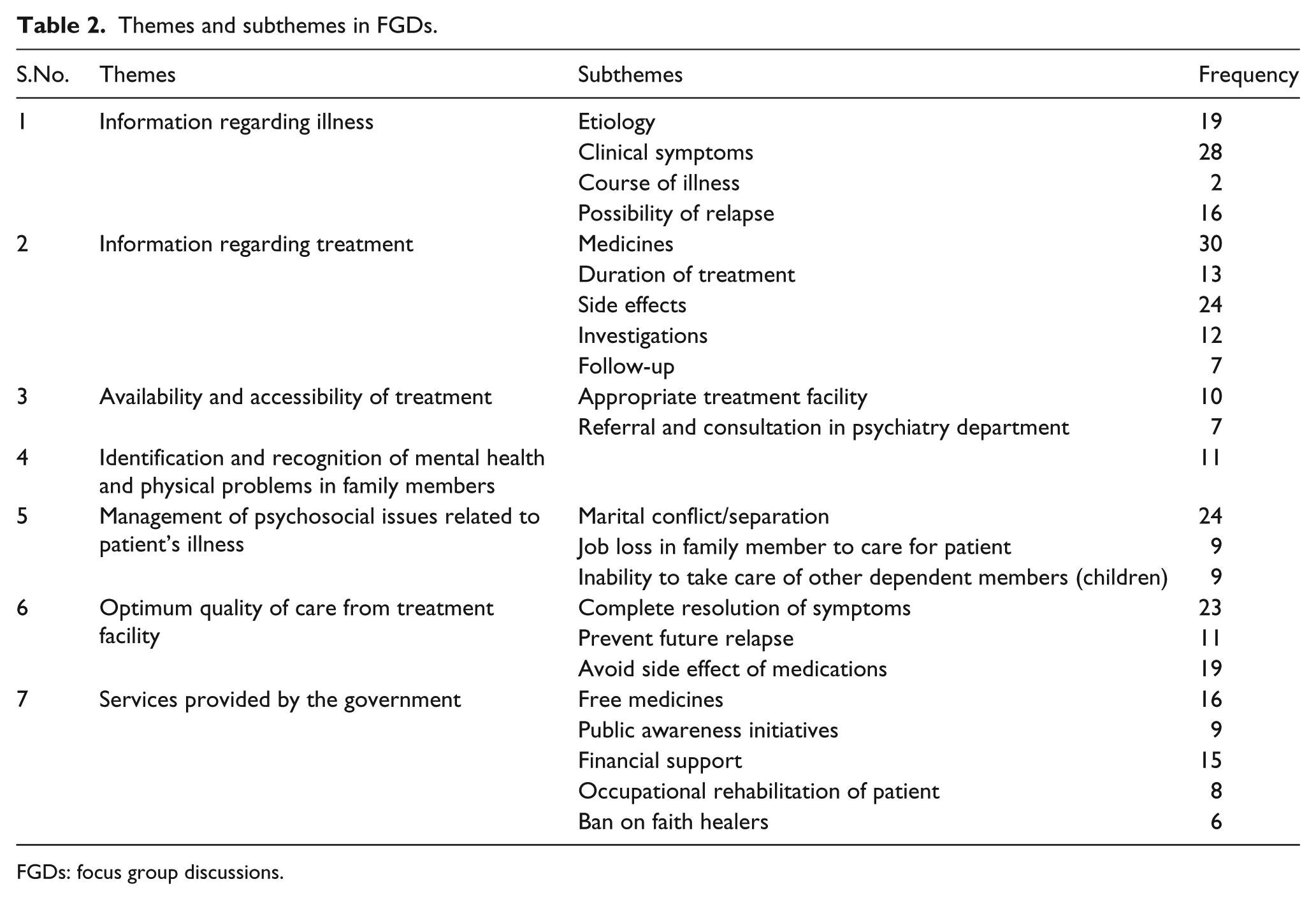
FGDs: focus group discussions.
Ranking, rating and percentage of themes across five FGDs.
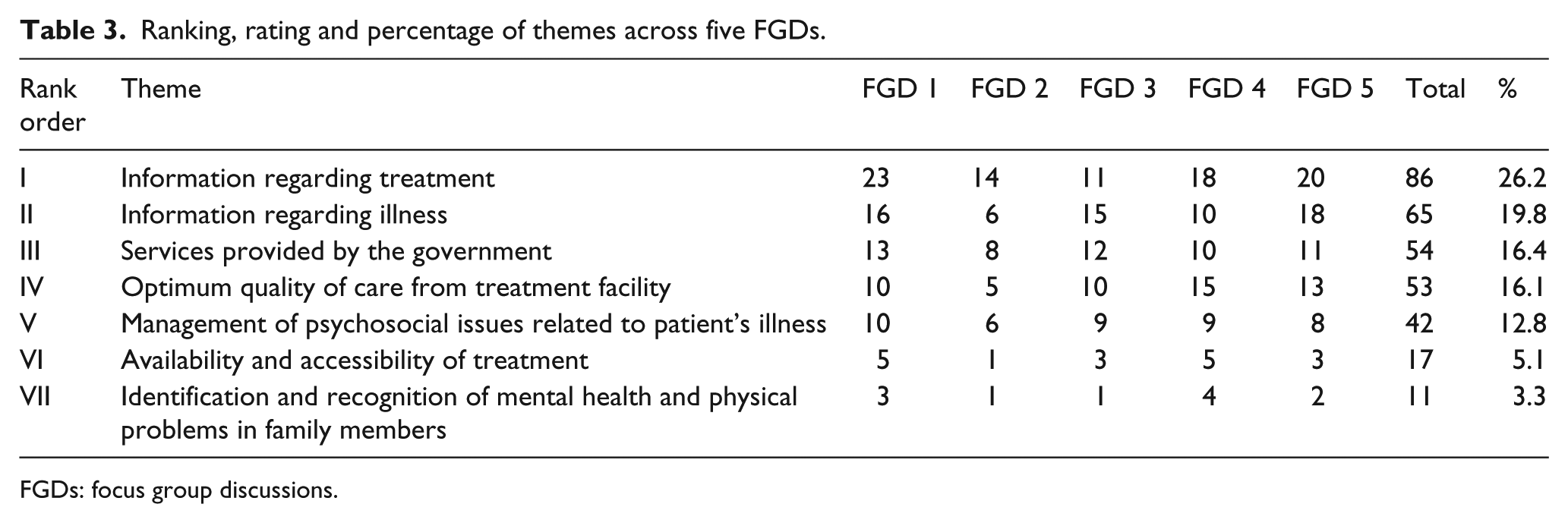
FGDs: focus group discussions.
The following quotes of the caregivers depict the needs expressed in the seven domains that emerged following analyses.
1. Information regarding treatment
Doctor told me to continue medication for a period of 2 years. We would like to know why we have to give him medication for 2 years and what is the reason for that.
2. Information regarding illness
When the problem started, initially we didn’t get his illness. We didn’t have any clue about this illness; we felt strange and weird. After a couple of weeks somebody told us that it is a psychiatric problem, so we came here for treatment. We would like to know why this illness appeared all of a sudden. My child was absolutely all right before few months! Why it happened?
3. Services provided by the government
We expect free medication from the government and some preference in job interviews or applications if possible.
4. Optimum quality of care from the treatment facility
We expect 100% treatment from the doctor and that he considers about his future and treat him properly so that he must be free from the disease in future as well.
5. Management of psychosocial issues related to patient’s illness
When our child gets violent all of a sudden then the entire family is confused, tensed and we don’t know what to do? Where to go? The entire family environment is changed due to this behavior of my child. Sir, we can’t afford treatment from private sectors, we have spent money while commuting and we have to buy some of the medication from outside, and I lost my daily wages whenever I come for his follow-up. We always think about our child’s illness! We constantly feel tense about it! We try to divert our mind but still we could not stop this worry. Our two children would stay in the single room with us. Due to our son’s behavior, his sister is also suffering from a disturbance in studies, and they always fight.
6. Availability and accessibility of treatment
We consulted the doctor late; it took a few months to find the right doctor who could tell us about his illness.
7. Identification and recognition of mental health and physical problems in family members
We are worried about our younger son. Will he also get this illness? Our elder son was well a few years ago. How will we know if our younger son gets the same illness?
Discussion
This study was conducted to assess the needs of caregivers of young patients with FEP in an outpatient setting at a tertiary care public funded general hospital psychiatric unit using a qualitative approach.
Eighty percent of the caregivers were parents, and 20% were siblings. Interestingly, about two-thirds of the caregivers were males. This is in contrast with previous studies where mothers have been reported to be caregivers in the majority of the case (Magliano et al., 2000; Meijer et al., 2004; Wancata et al., 2008). The siblings have been rarely reported to be caregivers in FEP (Amaresha et al., 2014). More number of male caregivers in this study could be explained by the fact that the mothers preferred to remain at home looking after other family members and carrying out household chores.
The needs of the caregivers of young patients with FEP are extensive and span over multiple domains. The need for information regarding treatment was most common. The caregivers needed information about the medicines used for treatment, the duration for which they were to be used, possibilities of side effects and the need for follow-up as the primary need of the caregivers. This reflects the need for appropriate psychoeducation programs targeting the families/caregivers of young patients suffering from FEP. Addressing the need for information about treatment through family psychoeducation programs might also be crucial in order to maintain treatment adherence and follow-ups, thereby improving outcomes.
The second most important need was the need for information regarding various aspects of FEP, specifically its etiology, signs and symptoms, further course of the illness and possibility of relapse after the symptoms had subsided. Because of the prevalent myths and misconceptions regarding mental illnesses and by the nature of symptoms in psychosis, it is often difficult for caregivers to get a grasp of the situation leading to psychological stress and burden (Magaña, Ramírez García, Hernández, & Cortez, 2007). Psychoeducational interventions for caregivers improve relatives’ attitudes toward schizophrenia, which in turn impacts the caregiver’s quality of life (Paranthaman et al., 2010). Although the exact role of providing psychoeducation in caregivers of FEP needs to be elucidated, its emergence as a prominent need from the caregiver’s perspective warrants further research in this direction.
Another important domain of needs elaborated by the caregivers in the FGDs was the need for services in multiple sectors by governmental organizations. The most prominent among them included financial support, provision of free medicines and public awareness initiatives regarding the illness. A significant number of the caregivers reported being misguided by faith healer and local physicians leading to delay in seeking treatment at appropriate treatment facilities. Broadcast and print media are considered to be the public’s primary source of information regarding mental health/illness. Numerous studies have documented an association between negative media portrayals of people with mental illness and the public’s negative attitudes, and have concluded that stigmatizing presentations have a direct negative impact on individuals living with mental illness as well as on social policies (Ohaeri & Fido, 2001).
An interesting finding from the analysis of the FGDs highlighted the caregiver’s need for optimum quality of care from the treating team. The subjective perception of optimum quality included treatment, which would ensure that the symptoms ‘never come back’ and that the patient becomes ‘fully functional’ and can contribute to the family in multiple ways. The caregivers reported that according to them, such quality of care would be possible if the ‘doctor gave his 100% to the patient’ and also with appropriate medicines. This has been an interesting finding that has not been reflected in previous studies and needs to be explored further. The demonstration of this need strongly from the caregivers may be a reflection of their lack of information regarding the nature of psychosis, the progression and the resolution of symptoms. This reiterates the need for appropriate information and psychoeducation regarding illness to avoid disillusionment and disappointment in the future, often leading to caregiver stress and burnout. Alleviation of this need might be possible by taking care of the information needs with which this need is intricately linked.
Various psychosocial needs highlighted by the caregivers included management of marital and familial conflict due to the patient’s illness, loss of a job to care for the patient and inability to care for other dependent family members such as other children to care for the patient. Caregivers have to spend more time when their family member is symptomatic, as they need to care for their hygiene, calm down during the emotional outburst and take the brunt of abuse and assaults from their mentally ill family members. This also leads to psychological stress. Families are forced to acknowledge the stark reality of having a member with schizophrenia and to mourn the loss of unfulfilled expectations. Moreover, because of the chronic stress associated with the task of caring, the family may experience a series of marital conflicts between parents or differences about the other siblings. Thus, it is common for families to have emotional responses such as anxiety, fear, guilt, stigma, frustration, anger and sadness. A study in India, carried out to understand the needs of families of those with mentally ill members and the impact of family-level interventions at the community level on those families, revealed that the psychosocial problems of families were related to their high level of expectations (of the person with mental illness) and of their emotional (over) involvement (Suman et al., 1980).
The caregivers of young patients with FEP also highlighted the need for appropriate treatment facilities geared toward the treatment of the patient. Often this need is equated with the information needs of the caregiver. Lack of information about the illness would often lead to the caregivers approaching faith healers and local physicians instead of a psychiatry facility. In general hospital settings, the need for referral to psychiatry department was highlighted, as the patient would often initially approach a different department. Often a department of psychiatry is not available in the vicinity of the patient’s residence, especially in rural and peripheral areas (Naik et al., 1996). The need for readily accessible treatment is also invariably linked to the need for governmental services in the form of establishment of accessible treatment at the primary care level for patients with FEP. This would facilitate early diagnosis and management, and alleviation of the patient’s symptoms as well as the burden of caregiving for the family members. Another important need highlighted by the caregivers is the need for healthy coping measures in the caregivers to deal with the patient’s illness. The caregivers develop different kinds of coping strategies to deal with the burden of caregiving. Caregiver’s positive evaluation of their coping strategies is associated with reduced distress levels and positive attitude toward the patient, which is independent of symptoms and levels of burden (Grover, et al., 2015).
A previous qualitative study from India exploring the needs of caregivers of inpatients with schizophrenia revealed the primary need to be managing illness behavior of the patient followed by managing social–vocational problems of the patient (Jagannathan et al., 2011). The information needs did not feature as prominently as in caregivers of FEP in our study, although education about schizophrenia was one of the needs expressed by the caregivers. An explanation of this difference may be that caregivers of patients with schizophrenia eventually are psychoeducated at various points of their interaction with the treating team, regarding the characteristics of the illness, its signs and symptoms as well as treatment options. Moreover, the previous study was conducted with inpatients who were admitted, and thus could have been more focused on management issues in it compared to the current study where the sample comprised of outpatients. Similarly, expressed concern regarding managing negative symptoms in the patient emerged as one of the important needs in the previous study (Jagannathan et al., 2011). This was not seen in the current study. This again may be attributed to the inherent difference in the symptom profile between FEP and schizophrenia. In the previous study, the issue of stigma was also highlighted in the context of ‘educating society to minimize stigma’. In our study, stigma did not figure prominently among the caregivers. Although the caregivers did express the need for government services to educate people, public awareness campaigns and so on, the need to alleviate stigma was not expressed explicitly in any of the FGDs.
A previous study which assessed the needs of caregivers of patients with chronic schizophrenia (mean duration of illness: 13 years) using quantitative assessment tools reported amelioration of psychotic symptoms (76%), information about the illness and treatment (68%) and relief of psychological distress (62%) as the three most prominent needs as perceived by the caregivers (Grover et al., 2015). The most commonly reported total needs by the caregivers of patients with schizophrenia included psychoeducation (76%), free treatment (60%), medical reimbursement (58%) and certification (56%). Of these needs only, the psychoeducation needs were met for the majority of the patients (Grover et al., 2015). A comparison with our study findings reveals that in caregivers of chronic schizophrenia, the management- and rehabilitation-related needs take precedence over information needs. Over the course of treatment, often psychoeducation-related needs are met. The patients with FEP approach a treatment facility for the first time, often after numerous visits to faith healers or general physicians. This is significant from intervention point of view as studies have demonstrated that caregiver psychoeducation specifically for FEP directly improves knowledge of the illness overall and, in particular, knowledge of medication, and also improves relapse prevention (McWilliams et al., 2010). Caregiver needs assessment in other chronic physical illnesses have reported different facets of themes like emotional impact (fear of future or sense of hopelessness), dealing with emergencies, role definition, ignorance of self-health care, promotion of physical activities, exclusion or engagement with social services (Wingham et al., 2017; Wingham et al., 2015). Cultural and linguistic diversity also accounts for a varied presentation of caregiver needs in diverse illnesses (Schaffler et al., 2019).
Our study had a few limitations. As there was a male preponderance of caregivers in the study sample, the results might have not accurately depicted the needs of mother and siblings of patients. The findings of this study may not be generalizable to the caregivers of young patients with FEP in other parts of India as the access to education and age-specific role or duties of an individual may have regional variations due to diverse cultural practices across India. Although the sampling method to recruit the caregivers was aimed at getting a representative sample, it is possible that frequent attendees were overrepresented. The method of FGDs has certain inherent limitations such as the group members’ responses are not independent of one another, which restricts the generalizability of the results. Some of the members were hesitant to talk in a group situation – especially when sharing sensitive issues. Caregivers might have expressed other needs if they had been interviewed individually. Key informant interviews could thus have added considerable strength to the results of the study.
Conclusion
The present study explored the needs of caregivers of young patients with FEP in India, using a qualitative approach. The study found that the needs of the caregivers of young patients with FEP are extensive and in multiple domains quite different in many aspects from those suffering from a chronic illness.
While the need for information regarding treatment was most common, illness-related information was reported second to it. Unlike caregivers of chronic schizophrenia, illness-related information needs took precedence over the management and rehabilitation-related needs. Stigma did not feature centrally in the themes, but the component of need for services in multiple sectors by governmental organizations identified the need for public awareness initiatives regarding the illness that indirectly addressed the issue of stigma. Expectations toward optimum quality of care from the treating team also emerged as an important facet of theme in the FGDs. Need for identification and recognition of mental health and physical problems in family members was also identified.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.