
Abstract
Background:
Involuntary admissions can be detrimental for patients. Due to legal, ethical and clinical considerations, they are also challenging for referring physicians. Nevertheless, not much is known about the subjective perceptions of those who have to decide whether to conduct an involuntary admission or not.
Aims:
This study aimed at answering the question whether psychiatrists’ perceptions of confidence during psychiatric emergency situations and consecutive involuntary admissions differ from those of physicians without a psychiatric training.
Method:
We assessed the professional background and subjective perceptions during psychiatric emergency situations in physicians who executed involuntary admissions to the University Hospital of Psychiatry Zurich. We used one-way analysis of variance (ANOVA) with Bonferroni-adjusted post hoc tests and chi-square tests to compare the responses of 43 psychiatrists with those of 64 other physicians.
Results:
Psychiatrists felt less time constraints compared with non-psychiatric residents. The latter also had more doubts on the necessity of the involuntary admission issued. Psychiatrists considered themselves significantly more experienced in handling psychiatric emergency situations and in handling the criteria for involuntary admissions than other physicians. Psychiatrists and other physicians did not differ in their satisfaction concerning course and results of psychiatric emergency situations which was overall high. About half of all participants felt pressure from third parties.
Conclusion:
Psychiatric emergency situations are challenging situations not only for patients but also for the involved physicians. Physicians with a specialized training might be more confident in the handling of psychiatric emergency situations and exertion of involuntary admissions. Non-psychiatric physicians might benefit from specialized training programs.
Keywords
Introduction
Involuntary admission (IA) violates the patients’ rights of freedom and self-determination, and therefore has been discussed controversially since the very beginning of modern psychiatry (Katsakou & Priebe, 2006). The majority of patients have negative attitudes toward IA, but some tend to retrospectively change their opinion and believe they needed hospitalization (Gardner et al., 1999; Priebe et al., 2009, 2010). Furthermore, between one and two thirds of involuntarily admitted patients only perceived low levels of coercion or were not certain in which aspects they were restricted (Bindman et al., 2005; Ivar Iversen, Hoyer, Sexton, & Gronli, 2002; Monahan et al., 1995). However, it was shown that although some patients concluded they had needed hospitalization, they disagreed with the IA (Gardner et al., 1999). Besides these findings, some patients who experienced coercive treatment tend to avoid contact with the health care system in a later crisis (Smith, 1995; Swartz, Swanson, & Hannon, 2003) and see psychiatric clinics as ‘adversaries’ (Mielau et al., 2018).
Due to its restriction of the patients, IA is regulated by national and in some countries by regional laws (Dressing & Salize, 2004; Jaeger et al., 2014; Zhang, Mellsop, Brink, & Wang, 2015). Besides that, mental health service structures and treatment culture (Emons et al., 2014), societal attitudes and personal values have an important impact on the execution of coercion (Lauber & Roessler, 2007; Steinert et al., 2010). This might play a role in the internationally but also regionally varying numbers of IA and other coercive measures. However, it is difficult to relate these varying rates directly to differences in legislation, in treatment culture or other factors (Dressing & Salize, 2004; Faulkner, McFarland, & Bloom, 1989; Fiorillo et al., 2011; Riecher-Roessler & Roessler, 1993; Rotvold & Wynn, 2015b; Salize & Dressing, 2004; Steinert et al., 2010).
In Switzerland, a federal republic with 26 cantons (states), IA is regulated on a national and cantonal level by the Swiss civil code which was revised in 2013 (Federal Assembly of the Swiss Confederation, n.d.). One of the aims of this revision was to comply with the international objectives to reduce coercive measures in psychiatry and encourage the patients’ autonomy (Swanson et al., 2008). In the canton of Zurich (with 1.4 million people the most populated canton of Switzerland), the overall rate of IAs is constantly high, ranging from 21% to 33% (Lay, Nordt, & Roessler, 2011; Salize & Dressing, 2004; Schuler, Tuch, & Peter, 2018) of all admissions to psychiatric hospitals. In this canton, every physician who is entitled to practice medicine is legally authorized to mandate IAs, regardless of specialization or experience. Accordingly, IAs are mandated by a large number of physicians with different medical specializations and varying experience in psychiatric emergency situations (PESs) (Jaeger et al., 2014). It was shown that the length of involuntary hospitalization was significantly higher in patients referred by physicians assumed to have more routine in PESs (i.e. psychiatrists and emergency medicine physicians) compared with those referred by physicians assumed to have less routine (i.e. general practitioners (GP) and hospital physicians). This indicates that some IAs of the latter might have been unnecessary and therefore could have been avoided (Hotzy, Kieber-Ospelt, Schneeberger, Jaeger, & Olbrich, 2018; Fuglseth et al., 2016). Nevertheless, not much is known about the subjective feelings of the referring physicians during IA.
It was found that referring GP described pressure from different sides (the patient’s family, police and so on) (Rotvold & Wynn, 2015a) and insecurities (Jepsen, Lomborg, & Engberg, 2010). This was discussed to be the result of a lack of routine in the handling of such situations (e.g. in Norway, a GP mandates about one or two patients involuntarily per year; Jepsen et al., 2010; Rotvold & Wynn, 2015a). Low education level and lower age were shown to be associated with arbitrary attitudes toward the process of admission (Shao, Xie, & Wu, 2012).
More insights into the subjective perceptions of referring physicians from different professional backgrounds and with different working experience could help to better understand the process leading to IA. The canton of Zurich with its broad range of mandating physicians is conducive to such a type of study as it enables comparison of the perspectives of physicians with different specialization and working backgrounds.
This study aimed at answering the question whether referring physicians with a psychiatric specialization compared with other physicians differ in their self-experienced competence in PES and their confidence in dealing with criteria for IA. We hypothesized that psychiatrists feel more confident in handling PESs and the criteria for IA compared with other physicians, particularly to those with little working experience.
Material and methods
Sample and subgroups
We collected data from physicians who referred patients for IA to the University Hospital of Psychiatry Zurich. With its affiliated departments for in- and outpatient treatment, it constitutes the largest clinic for psychiatry in Switzerland, providing mental health services for a catchment area of nearly 500,000 inhabitants from a mostly urban region.
During a 12-month period (October 2016–September 2017), 560 physicians accounted for a total of 1,242 IAs to the University Hospital of Psychiatry Zurich. Due to missing or unclear contact information, job changes, admissions from other cantons of Switzerland or because the physicians refused to be contacted, we were able to invite 364 physicians to participate in an online questionnaire. The online questionnaire was completed by 107 (30%) participants.
We built three groups to compare the perceptions and feelings of competence in PES and IA between the referring psychiatrists and other physicians: psychiatrists, non-psychiatric senior physicians with a degree in any other medical specialty and several years of working experience and non-psychiatric residents who had not yet completed their training/specialization. For the referring psychiatrists, there was only one person with less than 6 years of working experience (i.e. 4 years). Thus, we could assume a generally high working experience in psychiatrists and refrained from a division of this group.
Procedures
We contacted the eligible physicians by telephone. If they were interested to participate in the study, we sent them an email with information material about the study and a link to an online questionnaire. The completion of the questionnaire took about 10–15 minutes.
Measures
For this study, we developed a structured online questionnaire. The questionnaire was reviewed and discussed by physicians with experience in the handling of PES and execution of IA. One part of the questionnaire consisted of questions about the physicians’ professional background and their experience with PES. More precisely, participants’ gender, age, years of working experience, education level (specialization – completed or not) and working place (e.g. inpatient or outpatient setting) were assessed. In addition, participants reported the number of IAs issued during the last 12 months. We then assessed the participants’ perceptions during their last PES that resulted in an IA. This included questions about the participants’ situational experience of competence (e.g. ‘How confident did you feel handling the patient?’) as well as an assessment of the general experience and certainty related to PES and IA (e.g. ‘How confident are you in dealing with the criteria for IA?’). We asked the participants to rate these questions with a 4-point Likert-type scale (not at all = 1 to strongly = 4).
During the study, we also assessed details on the PES and legal considerations of the referring physicians as well as their compliance with the law. Those are described in detail elsewhere (Hotzy et al., 2019; Marty et al., 2018).
Statistical analysis
We conducted a one-way analysis of variance (ANOVA) with Bonferroni-adjusted post hoc tests for continuous data and chi-square tests for categorical data to examine the effect of physicians’ specialization and working experience on the subjective perceptions during PES and IA. Spearman correlation coefficients were calculated to assess relationships between the variables. For statistical analyses, we used SPSS 23.0 (IBM Corp. Released 2011; IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.) for Windows. The level of significance was set at p < .05.
Results
Sample characteristics
The mean age of the participants was 46 years, they had a mean professional working experience of 18 years (min = 1, max = 45, SD = 11 years), and 61% were male. A total of 92 (86%) participants stated that they had conducted more than one IA during the last 12 months. Of those, 16 (15%) had referred more than 10 patients involuntarily during this period. The sample is described in more details in another publication elsewhere (Marty et al., 2018).
Subjective perceptions of the referring physicians during their last IA
Nearly one third of the participants felt an intermediate or strong need to cut things short or leave them away because of time constraints (for details see Tables 1 and 2). We found a significant positive correlation between perceived time constraints and the extent of perceived pressure from third parties (rs = .36, two-tailed p < .001). About half (n = 50) of the participants felt to some extent pressure from a third party to order an IA. Of those, most named the patient’s private environment (next of kin (NOK) and/or friends) as a source of pressure, followed by colleagues/supervisor and the police (for details see Table 3).
Situational and general perceptions of PES and IA.
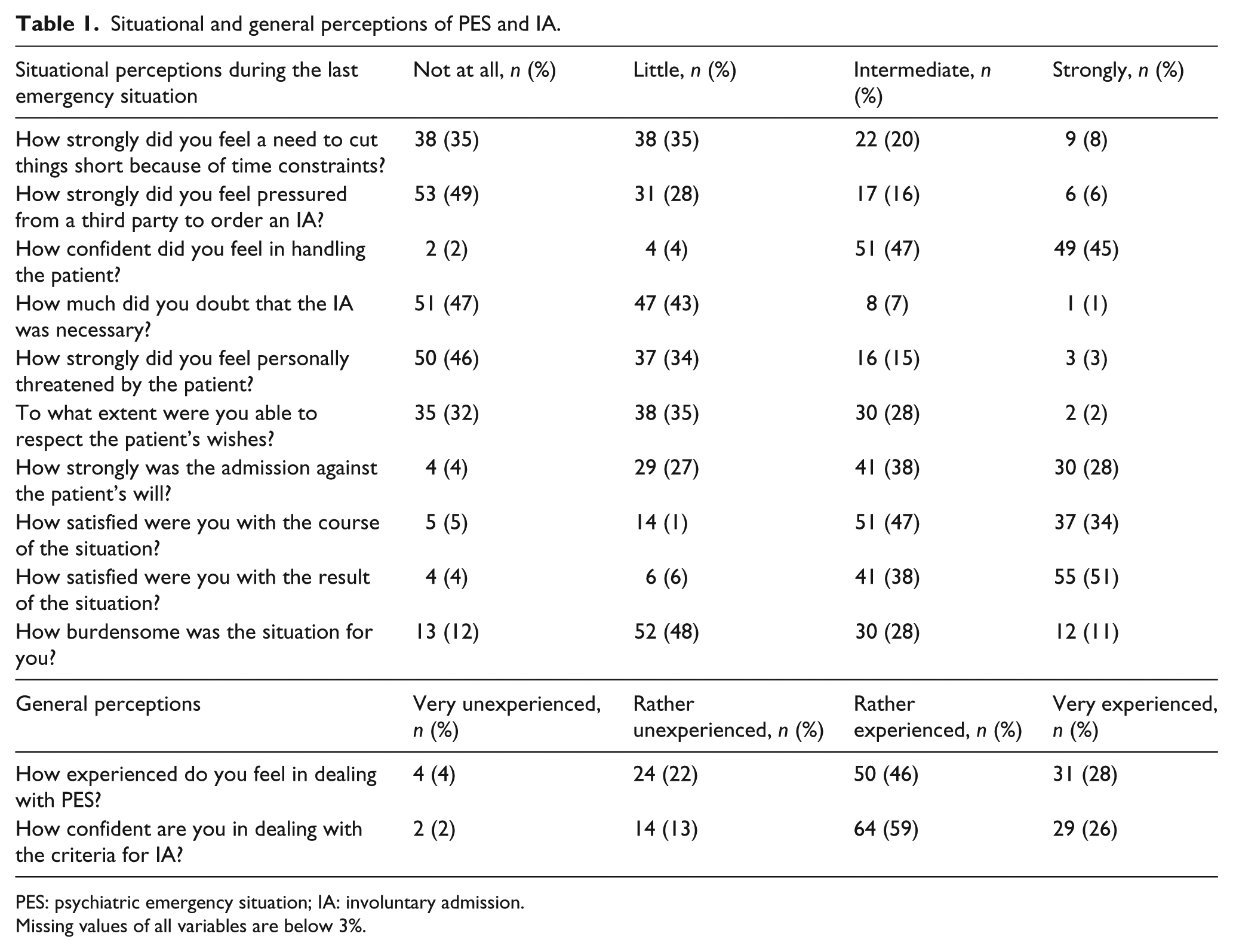
PES: psychiatric emergency situation; IA: involuntary admission.
Missing values of all variables are below 3%.
Relationship of perceptions during the last psychiatric emergency situation determined by Spearmen rank correlation coefficients.
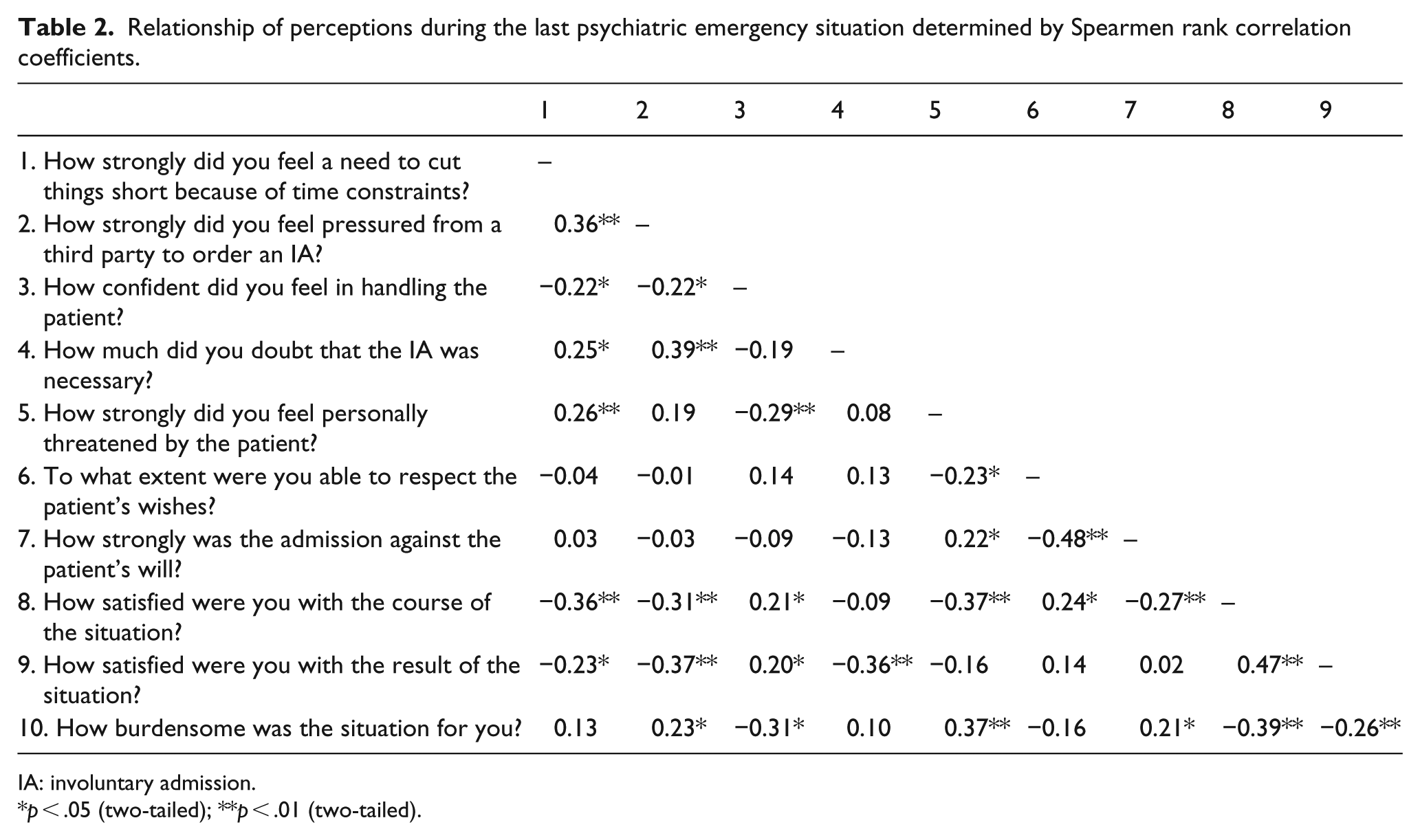
IA: involuntary admission.
p < .05 (two-tailed); **p < .01 (two-tailed).
Referring physicians’ perceptions of pressure from third parties during the psychiatric emergency situation.

In total, 54 respondents naming 79 parties.
The majority had no or little doubts on the necessity of the IA. Nevertheless, doubts on the necessity correlated significantly with higher perceived pressure from third parties (rs = .39, two-tailed p < .001).
About half of the participants felt threatened by the patient to some extent. When we compared the participants who stated that no police was involved to those with police involvement (induced by the physicians themselves (n = 32) or others (n = 37)) during the PES, we found that the latter felt threatened to a significantly higher extent (χ2(3) = 15.55, p < .001, n = 106). Furthermore, we found a significant negative correlation between subjective feelings of threat and confidence in handling of the patient (rs = −.29, two-tailed p = .001), whereas subjective feelings of threat were positively correlated with burdensomeness of the situation (rs = .37, two-tailed p < .001).
Although some participants described aversive perceptions (threat, time constraints, burden), nearly all felt confident in the handling of the patient and about two thirds also described that they could respect the patient’s wishes at least a little. In contrast, about one third stated that the admission was strongly against the patient’s will.
Nearly 40% of the participants reported that the PES was burdensome for them, with most of them feeling only intermediate burden.
The majority of the referring physicians were satisfied with the course and the result of the PES. The satisfaction with the course of the PES was negatively correlated with time constraints (rs = –.36, two-tailed p < .001), pressure from third parties (rs = –.31, two-tailed p < .001), perceptions of personal threat (rs = –.37, two-tailed p < .001) and burdensomeness (rs = –.39, two-tailed p < .001) and if the admission was highly against the patients will (rs = –.27, two-tailed p < .001). The satisfaction with the result again was negatively correlated with doubts on the necessity (rs = –.36, two-tailed p < .001) and pressure from third parties (rs = –.37, two-tailed p < .001).
Subjective perceptions of psychiatrists compared with other physicians
Psychiatrists and other physicians did not differ in gender and the amount of IAs conducted during the past 12 months, whereas, as expected, age and years of working experience did differ. Non-psychiatric residents had significantly less working experience and were significantly younger compared with non-psychiatric seniors and psychiatrists.
In the participants’ perceptions during the last IA, the extent of perceived time constraints differed significantly between psychiatrists and non-psychiatric residents. Furthermore, the residents felt less confident in the handling of the patient and did doubt the necessity of the IA to a significantly higher extent compared with psychiatrists. The non-psychiatric seniors’ ratings constantly ranged between psychiatrists and non-psychiatric residents but did not differ significantly from both the groups.
When we asked for the general rating of the personal experience in dealing with the PES, we found significant differences between all groups. Residents felt significantly less experienced than psychiatrists and seniors. The latter felt significantly less experienced than psychiatrists.
When asking for a general rating of the confidence in dealing with the criteria for IA, psychiatrists were significantly more confident than the other physicians. Although non-psychiatric seniors were more confident than non-psychiatric residents, the effect was not statistically significant. For details see Table 4.
Differences in situational and general perceptions of PES and IA related to referring physicians’ specialization and experience.
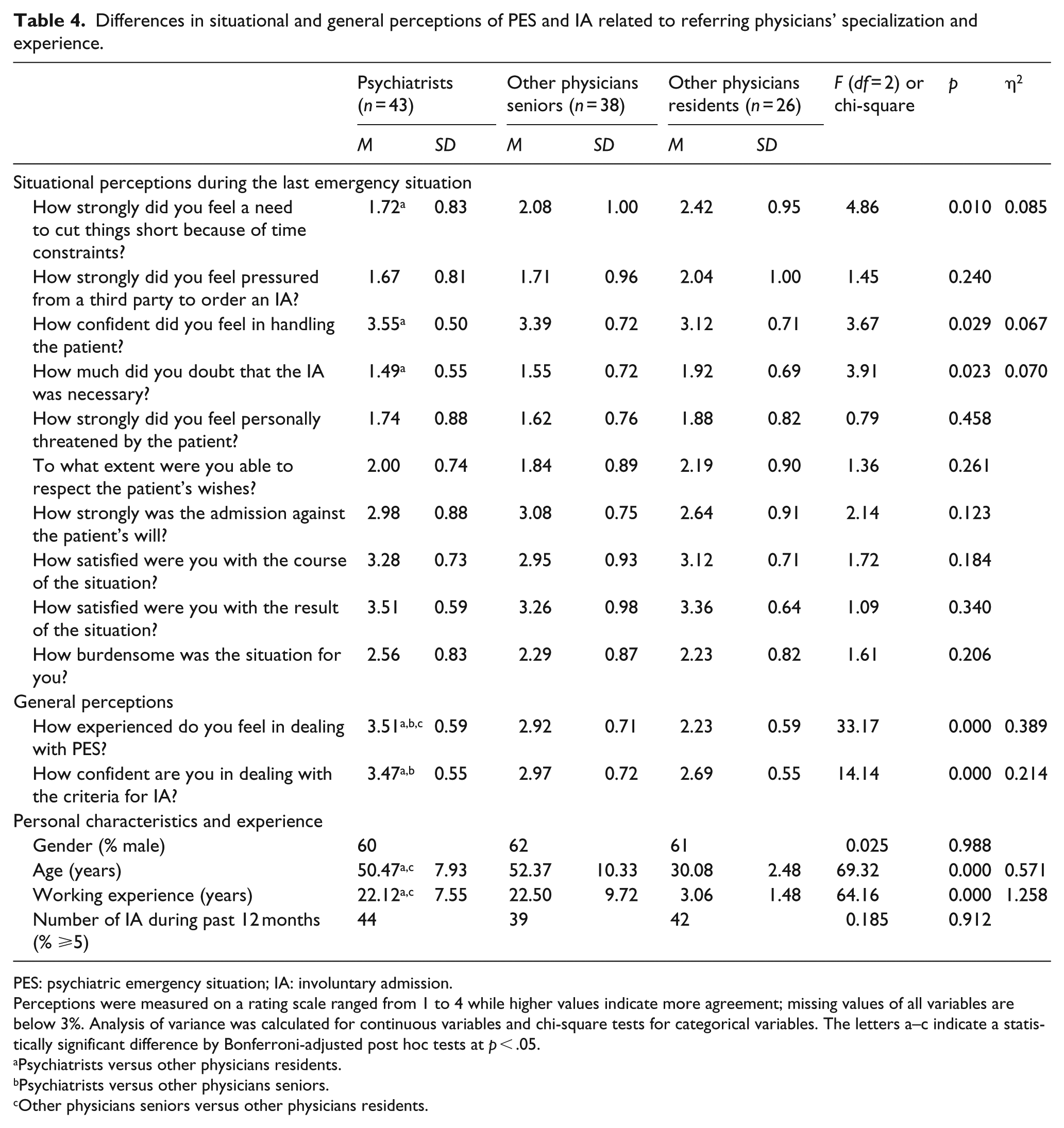
PES: psychiatric emergency situation; IA: involuntary admission.
Perceptions were measured on a rating scale ranged from 1 to 4 while higher values indicate more agreement; missing values of all variables are below 3%. Analysis of variance was calculated for continuous variables and chi-square tests for categorical variables. The letters a–c indicate a statistically significant difference by Bonferroni-adjusted post hoc tests at p < .05.
Psychiatrists versus other physicians residents.
Psychiatrists versus other physicians seniors.
Other physicians seniors versus other physicians residents.
Interestingly, the amount of IAs ordered per physician within the last 12 months did not significantly correlate with the confidence in dealing with the criteria for IA (rs = .09, two-tailed p = .334) nor with the personal experience in dealing with PES (rs = .14, two-tailed p = .142).
Discussion
In this study, we could show that physicians who refer patients for involuntary hospitalization have to deal with a variety of challenges like pressure from third parties and sometimes even threats from the patient. Furthermore, we found significant differences in the confidence in dealing with PES and the criteria for IA between psychiatrists and other physicians, with more profound effects if the latter were residents. Compared with psychiatrists, the residents also differed significantly in the perception of procedural aspects, such as time constraints.
In line with previous studies (Carstensen et al., 2017; Harris, Beurmann, Fagien, & Shattell, 2016; Rotvold & Wynn, 2015a), our study confirmed that PESs are very diverse in terms of the different parties involved and the time needed to come to a decision based on medical and juridical aspects. Furthermore, we were able to show that referring psychiatrists and other physicians describe different grades of confidence and knowledge in the handling of PES and the criteria for IA.
Psychiatrists are trained to detect, assign and intervene in PES. Consequently, they may feel more experienced and confident in dealing with such situations. In contrast, most other physicians lack such a structured training and might rarely be involved in PES. A Norwegian study showed that GP felt uncertain with the criteria for IA. This was considered to result partly from the low number of IAs conducted by these physicians, that is, one or two IAs per year (Rotvold & Wynn, 2015a, 2015b). However, in our study, the amount of IAs per year did not differ significantly between the groups of referring physicians and most of the participants conducted two or more IAs per year. Thus, the different perceptions of confidence between psychiatrist and other physicians may have other reasons than the quantitative number of IAs conducted per year.
PESs are time-consuming, even for experienced physicians (Jepsen et al., 2010). Most of the non-psychiatric residents (in this study those with the least confidence and experience) were working in institutions. Procedural aspects in such institutions were shown to hinder comprehensive and thorough consultations which are needed in PESs (Hong, 2016). This might explain the higher perception of time constraints in somatic physicians and especially in the group of residents. Physicians in charge might remain with open questions if they assessed all important aspects and ruled out less invasive alternatives, as it is stipulated by law.
We found that non-psychiatric residents more often stated doubts regarding the necessity of their IA and felt higher time constraints than psychiatrists. It was discussed that in the curricula of emergency medicine residents, the diagnostic and treatment principles of psychiatric patients seem to be underrepresented (Bode & Jackson, 2017) although the amount of psychiatric patients in non-psychiatric settings (e.g. emergency departments) is high (Downey, Zun, & Burke, 2012; Fulbrook & Lawrence, 2015; Lally et al., 2015). We suggest that psychiatric patients would benefit from the availability of specialized psychiatric teams. With their profound training and knowledge in the handling of PESs, they can give their professional advice for further treatment options (Wise & Berlin, 1987). The exchange and discussion with these experienced physicians might have a beneficial training effect on the residents and consequently reduce the rate of IAs. Future studies should evaluate whether an assessment by a specialized psychiatric team can reduce the number of IAs.
Besides the time constraints, about half of the participants felt pressured from third parties. NOK, the police and colleagues were most frequently named. This is comparable to findings from a Norwegian study where about half of the referring physicians reported pressure from third parties (Rotvold & Wynn, 2015a). In Switzerland, the needs of third parties, that is, from the patients’ environment, are considered by the legislation. It stipulates that one should take into consideration whether the affected person induces burden to his or her environment (Federal Assembly of the Swiss Confederation, n.d.). This paragraph in combination with pressure from the NOK may facilitate the physician’s decision for IA and may partly contribute to the high prevalence of IA in Switzerland compared with other countries (Riecher-Roessler & Roessler, 1993; Salize & Dressing, 2004). In this context, it is important to differentiate two major sources of pressure: On one hand, pressure – taken into account by the law – comes from the patients’ NOK due to the burden caused by the patient’s disorder. On the other hand, there is pressure to conduct an IA initiated by the police or caretakers. Especially such kind of pressure should not be a relevant factor in the decision-making process for an IA.
In some cases, it can be helpful for patients and third parties, that is, the NOK, to disrupt a conflictual situation, which may be perpetuated by symptoms of a psychiatric disorder. In a vicious cycle, the conflict may perpetuate the symptoms. Nonetheless, such a disruption should go along with the least possible coercion. Therefore, knowledge about (outpatient) alternatives to IA for psychiatric crisis intervention is important. On an organizational level, it is necessary to provide a broad range of alternatives to IA and secure their accessibility. It was shown that availability of outpatient services 24/7 was associated with reduced rates of IA (Gandre et al., 2017). Nevertheless, PESs are based on various grounds and there is not one best alternative to IA. This is a challenge for the health care system and the physicians in charge of a PESs who have to be aware of the treatment options in their area.
About half of the participants felt threatened by the patients. It is important that physicians can rely on the presence of police when necessary (Douzenis et al., 2012). This finding also underlines the importance to strengthen skills in de-escalation during PESs and the accurate assessment of the clinical symptoms of a patient. Such an assessment allows a profound estimation of potential prevention strategies in dangerous situations due to illness (clearly distinguish, for example, threats which fall within the jurisdiction of police). Nearly half of the participants experienced the PESs as burdensome. Nevertheless, most participants could accept the course and result of the PESs. One reason for this might be a relief to have terminated this burdensome situation. If the physicians in charge lack specific knowledge, patients with psychiatric symptoms may cause negative feelings, resulting in the impulse to finish the consultation as soon as possible (Hong, 2016; Zun, 2016). In this context, it is interesting that two thirds of the participants felt that they were able to respect the patients’ wishes in some aspects. It was shown that even if IA is used, the referring physician can sometimes comply with ambivalent feelings (Katsakou et al., 2012), and even with parts of the patients’ autonomy (e.g. way of transport to the hospital, choice of hospital, in-/or exclusion of third parties). Such interventions might be one explanation for the lower levels of perceived coercion during IA in some patients (Bindman et al., 2005; Ivar Iversen et al., 2002; Lidz et al., 1995). Future research should aim to assess not only whether interventions like crisis cards provide transparent information to patients about the reasons for hospitalization and its presumable duration, inform the patients about their rights and encourage NOK (Fiorillo et al., 2011), but also whether better training for the referring physicians or the regular implementation of specialized psychiatrists for the handling of PES can help to reduce the perceived coercion in psychiatric patients during both the admission and the course of hospitalization.
Strengths and limitations
Analyses were confined to responses from Swiss participants. Their experiences and attitudes may differ from referring agents from other countries with different mental health care systems and resources.
We were not able to invite all physicians who referred patients for IA during the study period (missing or unclear contact information, job changes, admissions from other cantons of Switzerland, refusal to be invited for participation). The participation in this study was voluntary and only one third of those physicians who were invited to participate in the study completed the online questionnaire. Thus, the results might be biased and not representative for the whole sample of referring physicians. However, we can assume that none of the groups of referring physicians were extremely over- or underrepresented as comparable distributions of the groups of referring physicians in Zurich were described in a former study (Kieber-Ospelt et al., 2016).
Conclusion
PESs are not only problematic, stressful and burdensome for patients. They also go ahead with perceptions of doubts, pressure and threats in the involved physicians who have not only the authority but also the obligation to decide whether coercion will be used or not. It is obvious that PESs are time-consuming and challenging. Furthermore, we found that factors other than the quantitative number of IA are correlated with confidence and experience in the handling of PES and IA.
Future studies should assess the benefit of specialized psychiatric teams with training in the handling of PES. Like consultation-liaison psychiatrists, they could provide profound assessment and recommendation for physicians with another specialization or complete the assessment and initiate further steps.
This might have an impact on the rates of IA and the patients’ perception of autonomy. In addition, other physicians might have more time to concentrate on patients who meet their expertise and benefit from educational effects from the expertise of the psychiatrists.
Footnotes
Acknowledgements
The authors thank our colleagues who were involved in the development of the structured questionnaire.
Author contributions
S.Ma., F.H. and M.J. conceptualized the study and collected the data. F.H., S.Mo. and S.Ma. performed the analysis and interpretation of data. F.H., SMa, S.Mo., A.T., P.H. and M.J. drafted the article or revised it critically for important intellectual content. F.H., S.Ma., S.Mo., A.T., P.H. and M.J. approved the final version to be published.
Compliance with ethical standards
In this study, no patient data were analyzed, and the data collection was anonymous. Therefore, the Cantonal Committee for Ethics decided that it was not subject to the Swiss Human Research Act (Humanforschungsgesetz) and exempted the study from further ethics approval. The study has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The authors informed the participants about the study in a cover letter. They assured the participants of the confidentiality and anonymity of the data and the voluntariness of participation. Participation and completion of the questionnaires were constituted as confirmation of their consent.
Data availability statement
The data sets used and/or analyzed during this study are available from the corresponding author on request.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.