
Abstract
Background:
Unemployment and mental ill health often contribute to each other and lead to social exclusion with negative consequences for individuals and society. Yet, unemployed people with mental health problems often do not seek care.
Aims:
The aim of this study was to assess predictors of help-seeking among unemployed people with mental health problems.
Methods:
At baseline, 301 unemployed participants with mental health problems reported potential predictors of help-seeking in terms of mental health literacy, perceived barriers to care, self-concept as having a mental illness and current mental health service use. At 6-month follow-up, 240 participants reported whether or not they had started new mental health treatment since baseline.
Results:
Adjusted for symptoms, sociodemographic and work-related variables, help-seeking was predicted by previous mental health service use and by fewer non-stigma-related barriers, not by stigma-related barriers.
Conclusion:
Implications for interventions to increase help-seeking among this vulnerable group are discussed.
Introduction
Unemployed people report unmet mental health care needs (Åhs, Burell, & Westerling, 2012; Bijl & Ravelli, 2000), but predictors of help-seeking in this vulnerable group are poorly understood. A better understanding is relevant from a public health perspective because unemployment and mental health problems often contribute to each other and lead to social exclusion with negative consequences for individuals and society (Olesen, Butterworth, Leach, Kelaher, & Pirkis, 2013). In general, different barriers to access mental health services exist, some of which are stigma-related such as shame or the fear to be seen as weak for having a mental illness (Clement et al., 2012). Non-stigma-related barriers can be instrumental (e.g., lack of transportation) or attitudinal (e.g., belief that professional treatment will not help; Clement et al., 2012). Recent longitudinal studies among people with mental health problems showed that help-seeking is a complex process influenced by stigma, mental health literacy, attitudes towards help-seeking, self-identification as having a mental illness and intentions to seek help (Bonabi et al., 2016; Schomerus et al., 2018).
Previous research on mental health service use among unemployed people has mostly been cross-sectional (Åhs et al., 2012) and sometimes focused on specific groups such as veterans (Levine et al., 2018). A small qualitative study among unemployed persons has shown that there is a complex interplay of barriers and facilitators of help-seeking such as mental health literacy, stigma and structures of health care (Staiger, Waldmann, Rüsch, & Krumm, 2017). A cross-sectional study on the same sample as in this study found a positive correlation between perceived discrimination and reduced job search self-efficacy as well as higher barriers to care (Staiger, Waldmann, Oexle, Wigand, & Rüsch, 2018). Especially, the double discrimination due to unemployment and mental health problems was harmful (Staiger et al., 2018). A recent longitudinal study among unemployed individuals with mental health problems found a positive association between welfare receipt and service use, but did not investigate barriers to help-seeking (Pymont, Schofield, & Butterworth, 2017).
In this longitudinal study among unemployed people with mental health problems, we expected that better mental health literacy, more self-identification as having a mental illness and less perceived stigma-related and non-stigma-related barriers at baseline would predict help-seeking over time. Furthermore, we wanted to investigate the influence of mental health service use at baseline.
Methods
Participants
Data were collected in the context of a larger study on unemployment and mental health problems (Rüsch et al., 2018; Rüsch et al., 2019). In employment agencies in Southern Germany, 301 currently unemployed participants were recruited based on the following inclusion criteria: participants either showed relevant psychological distress as indicated by a score ⩾ 13 on the K6 Psychological Distress Scale (range of possible sum scores 0–24; Kessler et al., 2003) or screened positive for alcohol or substance-use problems as indicated by a score of ⩾1 on items 2 to 4 of the CAGE-adapted to include drugs (CAGE-AID) (Hinkin et al., 2001); item 1 (‘cut down’) was omitted for the sake of specificity. Other inclusion criteria were an age of 18–64 years and a score of ⩾17 on the 12-item World Health Organization (WHO)-Disability Assessment Schedule 2.0 (range of possible sum scores 12–60; Üstün et al., 2010), indicating relevant illness-related disability. Sociodemographic variables of the baseline sample (N = 301) were as follows: age M = 43.7 years, SD = 11.2; female N = 151, 50.2%; length of current unemployment M = 35.6 months, SD = 42.7; and total education M = 13.7 years, SD = 3.3. At 6-month follow-up, data were available from 270 participants (age M = 44.0 years, SD = 11.1; female N = 137, 50.7%; length of current unemployment M = 36.4 months, SD = 43.4; and total education M = 13.8 years, SD = 3.3).
Measures
Barriers to care were assessed using the 30-item Barriers to Access to Care Evaluation scale (BACE), rating current barriers to professional care from 1/not at all to 4/a lot (Clement et al., 2012). The BACE contains a 12-item stigma-related (M = 2.0, SD = 0.7; Cronbach’s alpha 0.95) and an 18-item non-stigma-related subscale, the latter covering attitudinal and instrumental barriers (M = 1.9, SD = 0.5; Cronbach’s alpha 0.90; Clement et al., 2012). Examples of stigma-related items are ‘Feeling embarrassed or ashamed’ or ‘Concern that people might not take me seriously if they found out I was having professional care’. Examples of non-stigma-related items are ‘Being unsure where to go to get professional care’, ‘Problems with transport or travelling to appointments’ or ‘Thinking that professional care probably would not help’ (Clement et al., 2012). The non-stigma-related variables can be further subdivided into instrumental (8 items) and attitudinal barriers (10 items), and the first 2 items mentioned (unsure where to get care and lack of transportation) are examples of instrumental barriers, the other one of an attitudinal barrier to care.
The degree to which participants saw their present problem as a mental illness was measured by the 5-item Self-Identification as Having a Mental Illness Scale (SELFI; Schomerus et al., 2019; Stolzenburg et al., 2017) with items rated from 1/do not agree at all to 5/agree completely and mean scores from 1 to 5 (M = 3.7, SD = 0.9; Cronbach’s alpha 0.84). Examples of items are ‘My present problems could be the first signs of a mental disorder’ or ‘The thought of myself having a mental illness seems absurd to me’, with the latter item reverse coded.
Mental health literacy was assessed only using the 8 treatment-related items of the 22-item Depression Literacy scale (D-Lit; Griffiths, Christensen, Jorm, Evans, & Groves, 2004; M = 3.3, SD = 1.8). Examples of items are ‘Of all the alternative and lifestyle treatments for depression, vitamins are likely to be the most helpful’ and ‘People with depression should stop taking antidepressants as soon as they feel better’, possible answers are True/False/Do not know, with each correct answer counted and a range of possible sum scores from 0 to 8.
Depressive symptoms were measured using the Patient Health Questionnaire (PHQ-9; Kroenke, Spitzer, & Williams, 2001; range of possible sum scores 0–27; M = 14.7, SD = 5.2; Cronbach’s alpha 0.82), assessing the frequency of symptoms over the last 2 weeks (from ‘not at all’/0 to ‘nearly every day’/3). Examples of items are ‘Little interest or pleasure in doing things’ and ‘Feeling tired or having little energy’ (Kroenke et al., 2001). Most participants in this study fell into the categories moderate (score 10–14; n = 79), moderately severe (score 15–19; n = 91) or severe depression (score 20–27; n = 48).
At baseline, participants were asked whether they were currently treated for mental health problems by a psychiatrist or psychotherapist (n = 153), by a general practitioner (n = 103), or by taking psychiatric medication (n = 118). All in all, 194 used at least one of these services, while 76 indicated no current mental health service use. At follow-up, participants were asked whether they had begun any new psychiatric or psychotherapeutic treatment within the last 6 months (‘yes’, n = 94; ‘no’, n = 146; ‘have already been in treatment for a longer period of time’, n = 30). Only the 240 subjects answering yes/no were relevant for our research question and thus included into the analyses.
Ethical standards
The study was approved by the local ethics committee and was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All participants gave their written informed consent prior to their inclusion in the study.
Results
In a stepwise multiple logistic regression, baseline predictors of treatment initiation during follow-up were analysed. Model 1 included sociodemographic variables, symptoms and length of current unemployment; in Model 2, D-Lit, BACE and SELFI were added; and in Model 3, mental health service use at baseline (Table 1). Model 4 is a modified version of Model 3, in which the non-stigma-related BACE subscale is further subdivided into attitudinal and instrumental barriers (Table 2).
Stepwise logistic regression on help-seeking (initiation of psychiatric/psychotherapeutic treatment) within 6 months after baseline, n = 240.
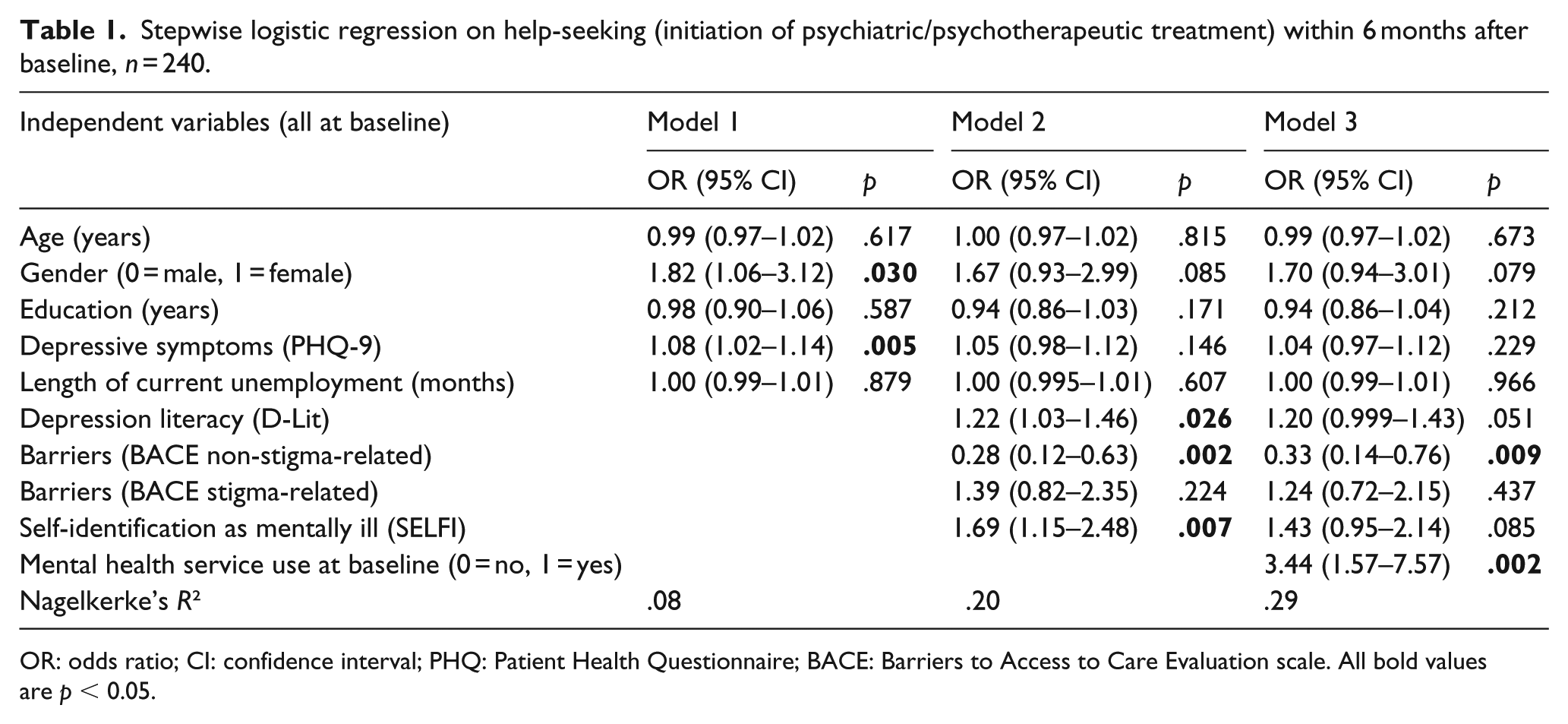
OR: odds ratio; CI: confidence interval; PHQ: Patient Health Questionnaire; BACE: Barriers to Access to Care Evaluation scale. All bold values are p < 0.05.
Stepwise logistic regression on help-seeking (initiation of psychiatric/psychotherapeutic treatment) within 6 months after baseline, Model 4, n = 240.
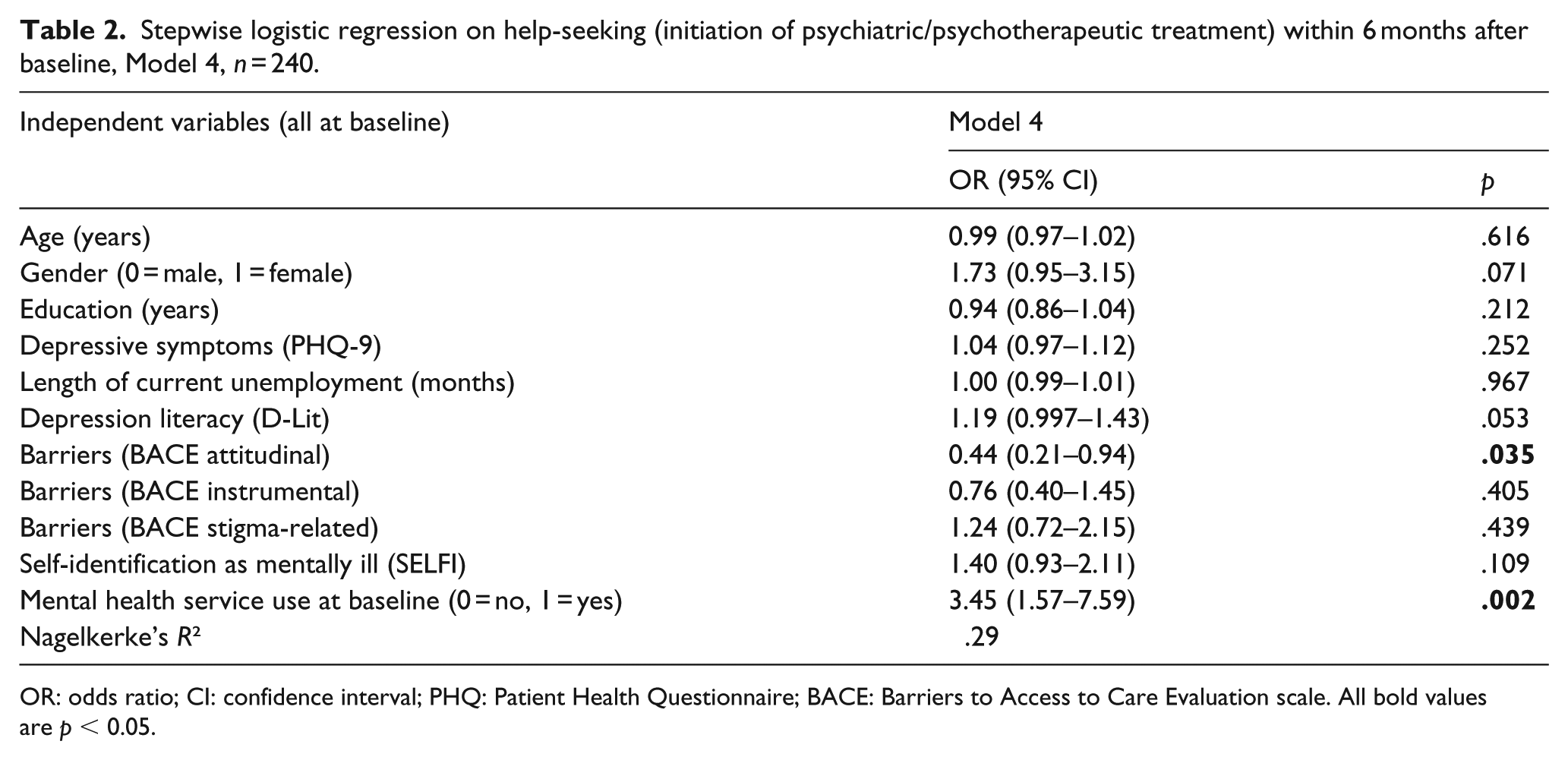
OR: odds ratio; CI: confidence interval; PHQ: Patient Health Questionnaire; BACE: Barriers to Access to Care Evaluation scale. All bold values are p < 0.05.
Bivariate Pearson correlations between all independent variables were analysed. All correlations were r < 0.4, except for intercorrelations of the BACE subscales: BACE instrumental with BACE attitudinal r = 0.48; BACE instrumental with BACE stigma-related r = 0.52; BACE attitudinal with BACE stigma-related r = 0.59; all p-values < .01.
In Model 1, female gender and more depressive symptoms significantly predicted seeking new help during the follow-up period. In Model 2, more mental health literacy, fewer non-stigma-related barriers and more self-identification as having a mental illness predicted help-seeking; stigma-related barriers did not predict help-seeking, gender and depressive symptoms lost significance. In Model 3, mental health service use at baseline and fewer non-stigma-related barriers predicted help-seeking, while more mental health literacy, more self-identification as having a mental illness and female gender did so on a trend level (all p-values < .085). In Model 4, mental health service use at baseline and attitudinal barriers, but not instrumental barriers predicted help-seeking; more mental health literacy and female gender did so on a trend level (all p-values < .085).
Discussion
To the best of our knowledge, this is the first longitudinal quantitative study to investigate barriers and facilitators of help-seeking in the vulnerable and hard-to-reach group of unemployed people with mental health problems, recruited in employment agencies and thus outside the mental health care system. While some of our findings are in line with previous research on help-seeking, other findings add novel aspects which might be related to the challenges faced by people with two stigmatised conditions such as unemployment and mental health problems.
Female gender has previously been shown to be associated with more positive attitudes towards help-seeking for mental illness (Kagstrom et al., 2019; Park, Jeon, Lee, Ko, & Kim, 2018), which is in line with our findings. It seems evident and has been shown before (Bonabi et al., 2016; Kagstrom et al., 2019; Schomerus et al., 2018) that better knowledge about mental health and the ability to identify oneself as having a mental illness facilitate help-seeking. In a previous cross-sectional study among the same participants as in this study, better mental health literacy was associated with stronger intentions to seek both professional and informal help (Waldmann, Staiger, Oexle, & Rüsch, 2019).
Before discussing implications of our findings, limitations of this study need to be considered. Our results cannot be generalised because participants were recruited in Southern Germany, a region with a very low unemployment rate of about 3% at the time of this study. Another limitation is that at follow-up participants were only asked if they had initiated any new treatment for mental health problems, but the existing treatments were not reassessed.
While stigma is a frequent obstacle to help-seeking (Clement et al., 2015), in this study stigma-related barriers did not influence help-seeking which needs explanation. One reason why stigma-related barriers did not play a significant role might be that our real-world sample of unemployed people with mental health problems mostly had already some form of primary or secondary mental health care at baseline. Thus, for most of our participants, treatment initiation during follow-up was not their first step into the mental health care system and label avoidance was likely less relevant. Another explanation could be the prominence model, according to which multiple forms of discrimination might not be worse than one prominent form, which could be explained by inurement, by coping mechanisms and by the identity centrality of the stigmatised condition (Thoma & Huebner, 2013). In our case, unemployment, which affects different areas of life and is itself associated with self-stigma (Blau, Petrucci, & McClendon, 2013), could be so central to participants’ identity that the additional stigma of mental illness was not perceived as a barrier to help-seeking.
As in other samples (Schomerus et al., 2018), depression severity did not predict help-seeking, pointing to a potential mismatch between objective need and treatment coverage. Those already in the mental health care system may find it easier to seek additional help, probably through better knowledge and referrals within the system. Seeking additional secondary mental health care seemed adequate given the depression severity among our participants and the known unmet mental health care needs of unemployed people (Åhs et al., 2012). However, our findings indicate that there is a large group of unemployed individuals with serious mental health problems who fall through the cracks, and the goal for services should be to identify and help those in order to stop the vicious circle of mental health problems and long-term unemployment. Attitudinal barriers seem to play a key role, possibly because some people with long-term unemployment have given up in a mindset of hopelessness and others do not trust mental health services. Interventions should thus target attitudinal barriers and address especially those outside the mental health care system. Mental health coaching in employment agencies to identify mental health needs and to provide information about mental illness and low-threshold access to mental health services could be particularly useful (Wabnitz et al., 2017).