
Abstract
Background:
Apart from its evident impact on physical health, physical activity also has a role to play in mental health. Individuals engaged in physical inactivity have been found to have higher morbidity and health care expenditure. In order to combat these issues and preserve mental health, interventions of exercise are typically advocated. This review aimed to assess the benefits of physical activity on common and severe mental disorders in the Indian context.
Materials and methods:
A Boolean search was carried out using both relevant keywords and MeSH terms. Articles were sourced from online databases including PubMed, ScienceDirect, Cochrane Database, PsycINFO and Google Scholar. All studies included in the review were peer-reviewed articles exclusively from India with Indian subjects reporting the relationship between physical activity and at least one mental health outcome including depression, anxiety, psychosis, stress, self-esteem and cognitive functioning.
Results:
Nineteen articles were found eligible for the narrative review. Out of these, 7 were cross-sectional studies and 12 were intervention studies.
Conclusion:
Existing literature from India has shown promising results towards the impact of physical activity in mental health disorders. However, more research is needed in the assessment of physical activity and physical activity interventions suitable to the Indian context. This review found that exercise and yoga are effective in reducing mean scores for both severe and common mental disorders. Yoga had a more significant impact on patients with schizophrenia than exercise or no intervention. To confirm that exercise is an effective add-on treatment, further research is required.
Introduction
Extensive literature highlights the benefits of physical activity for normal healthy living and prevention and management of health problems (Warburton, Nicol, & Bredin, 2006). Robust evidence exists implicating the association between medical conditions like cardiovascular diseases and individual lifestyle behaviours, particularly those that involve exercise or a lack there of (Warburton & Bredin, 2017). The effect of physical activity in preventing numerous chronic conditions and premature mortality has been systematically reviewed and analyzed (Warburton & Bredin, 2017). The influence that physical activity has over health is distinct enough that international guidelines recommend a quota of 150 minutes per week of moderate to intense physical activity for clinical and normal populations (Warburton & Bredin, 2017). Adherence to these recommendations can result in 20%–30% risk reduction for many chronic diseases (Warburton & Bredin, 2017). The dose-response nature of the relationship has resulted in an emphasis on physical activity for improving the course of all health problems and maintaining good physical health. Furthermore, systematic reviews on studies conducted globally have found that a minor volume of physical activity is sufficient for health benefits (Warburton & Bredin, 2017).
Apart from its evident impact on physical health, physical activity also has a role to play in mental health. Systematic reviews have found that mental illnesses have resulted in better outcomes when coupled with physical activity of some form (Warburton & Bredin, 2017). Pooled studies conducted globally have found that physical exercise is a promising intervention for depression, moderately more effective compared with a control (Mura & Carta, 2013; Rimer et al., 2012). General findings show that exercise improves mood state and self-esteem, and lowers stress dispositions, a factor known for aggravating mental and physical disorders alike (Callaghan, 2004; Raglin, 1990). Although causal links have not been established, methodologically robust studies have found that there is an associated improvement among both mentally ill and normal samples. However, significant improvements were found in pooled studies using long-term exercise programmes and individuals with anxiety or depression (Raglin, 1990). Individuals with schizophrenia are generally more sedentary in nature, increasing the risk of worsening their symptoms or additional health problems. Increasing the amount of physical activity can be effective in amelioration of some psychotic symptoms as well as prevention and treatment of comorbidities (Curcic et al., 2017).
Individuals engaged in physical inactivity have been found to have higher morbidity and health care expenditure. In order to combat these issues and preserve mental health, interventions of exercise are typically advocated. These insights have been extrapolated from global studies and research predominantly from the West. Whether the same holds true for Indian patients requires further investigation. Similar results as those published in global research and pooled reviews have been found in Indian studies. Review of such literature can combine evidence from different regions and settings within India to address a common national health problem. Furthermore, review of India specific studies could highlight the prevalence of such mental illnesses and the effectiveness of physical activity as an add-on treatment.
This review looked at articles from Indian literature which studied the effect of physical activity on mental health and its potential implications in the management of illness and course of treatment. There is literature available on interventions of varying physical activity from India. Among these, studies using exercise and yoga as add-on treatment for mental illnesses are common. Investigations into using yoga as an intervention for mental health have shown that although the amount of activity involved in yoga is not considered intense, the remaining components of the programme like relaxation or breathing techniques may simultaneously impact a practitioner’s mental state. In addition, studies have found that the amount of activity required to impart a beneficial effect on health problems may in fact be lower than recommended thresholds prescribe (Warburton & Bredin, 2017). Thus, including yoga in this review would be justified on account of the low to moderate level of activity it involves and its cultural relevance as a standard form of physical activity among Indians. In India, most research on physical activity surrounds the study of common mental disorders like depression and anxiety and their significant improvement when intervened by exercise or yoga programmes. Therefore, this review collected articles primarily using interventions of yoga and exercise for both severe and common mental disorders. Data on the prevalence of mental disorders and physical activity have also been included in the review. Conclusive evidence in support of physical activity could form a premise for altering course of treatment for neurosis and psychosis in Indian clinical populations.
Methods
Search strategy
A Boolean search was carried out using both relevant keywords and MeSH terms such as ‘Physical activity and mental health and India’, ‘Physical health and mental health and India’, ‘Physical activity and mental illness and India’, ‘Physical activity and mental health and India’, ‘Exercise and mental health and India’, ‘Yoga and mental health and India’, ‘Yoga and depression and India’, ‘Yoga and anxiety and India’, ‘Yoga and schizophrenia and India’, ‘Physical activity and depression and India’, ‘Physical activity and anxiety and India’, ‘Physical activity and schizophrenia and India’, ‘Exercise and depression and India’, ‘Exercise and anxiety and India’, ‘Exercise and schizophrenia and India’, ‘Yoga and severe mental illness and India’, ‘Yoga and common mental illness and India’, ‘Yoga and SMD and India’, ‘Yoga and CMD and India’, ‘Yoga and severe mental disorder and India’, ‘Yoga and common mental disorder and India’, ‘Physical activity and severe mental illness and India’, ‘Physical activity and common mental illness and India’, ‘Exercise and severe mental illness and India’, ‘Exercise and common mental illness and India’, ‘Physical activity and SMD and India’, ‘Physical activity and CMD and India’, ‘Exercise and SMD and India’, ‘Exercise and CMD and India’, ‘Physical activity and OCD and India’, ‘Physical activity and obsessive compulsive disorder and India’, ‘Physical activity and bipolar disorder and India’, ‘Yoga and OCD and India’, ‘Yoga and bipolar disorder and India’, ‘Physical activity and social functioning and India’, ‘Physical activity and cognitive functioning and India’, ‘Physical activity and stress and India’, ‘Physical activity and self-esteem and India’, ‘Physical activity and psychosis and India’ ‘Physical activity and neurosis and India’. Articles were sourced from online databases including PubMed, ScienceDirect, Cochrane Database, PsycINFO and Google Scholar. The mentioned databases were searched for articles published up to January 2019.
Study selection
Articles were first screened by abstract and the following criteria applied. Further screening of full-text articles was based on eligibility. Cross references of the articles were also screened. Study selection criteria included (a) peer-reviewed articles exclusively from India with Indian subjects; (b) studies that reported the relationship between physical activity and at least one mental health outcome including depression, anxiety, stress, self-esteem and cognitive functioning; (c) published in English and (d) studies with a cross-sectional or intervention methodology. Other reviews, case reports, animal studies, or studies using invalidated or inappropriate measurement tools were excluded from the current review.
Data extraction
The studies were screened according to the abovementioned inclusion and exclusion criteria, and the data were then extracted and later organized into various themes such as methodological aspects, epidemiology, and interventions.
Results
Out of 41 studies, 19 were found eligible for inclusion in the review. Exclusion of 22 articles was due to their use of non-Indian participants and study sites outside India. Furthermore, some excluded articles had studied variables other than common or severe mental illnesses such as neurological conditions like dementia and autism spectrum disorder, or physical illnesses like cardiovascular disease. The distribution of studies is shown in Figure 1. Ten articles studied the association of yoga and mental health, while nine studied exercise and mental health. Of all articles studying mental health outcomes, eight studied the effect of physical activity on depression and anxiety, and four on psychosis. Seven studies found cross-sectional data on a wide range of participants with mental illness and exercise. The major findings of the reviewed studies are organized in Tables 1 to 4.

Flow diagram of included studies for review.
Prevalence of mental illness and physical activity from seven cross-sectional studies.

WHO: World Health Organization; WHODAS: World Health Organization Disability Assessment Schedule; QOL: quality of life.
Clinical profile and findings from two exercise intervention studies for CMD.

Clinical profile and findings from six yoga intervention studies for CMD.

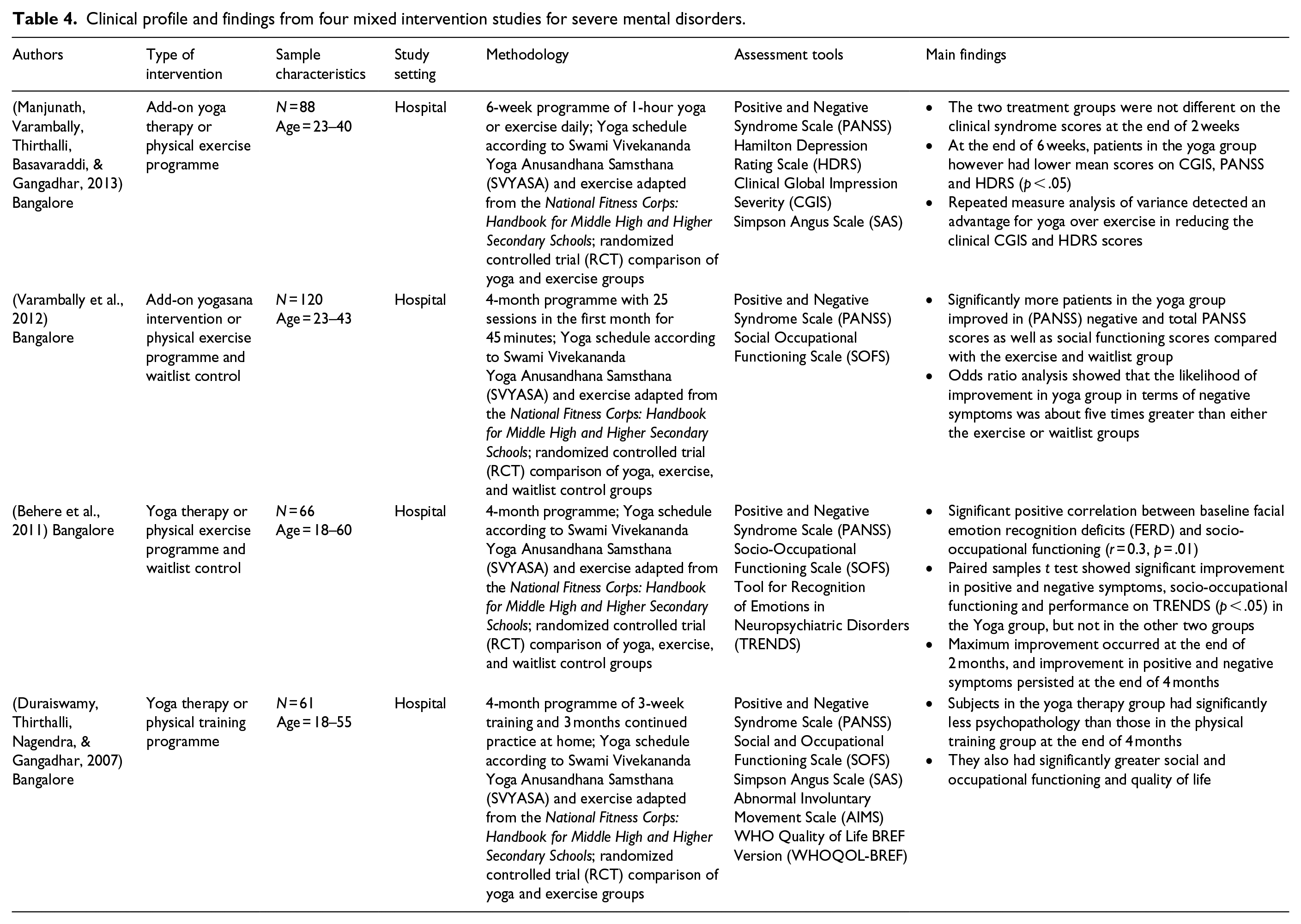
Clinical profile and findings from four mixed intervention studies for severe mental disorders.
Discussion
Methodological aspects
Type of study
The articles included in this review followed either a cross-sectional or intervention study design. A majority of studies were conducted in clinical settings (Behere et al., 2011; Duraiswamy, Thirthalli, Nagendra, & Gangadhar, 2007; Ganesh & Mishra, 2016; Krishnamurthy & Telles, 2007; Manjunath, Varambally, Thirthalli, Basavaraddi, & Gangadhar, 2013; Ramanathan, Bhavanani, & Trakroo, 2017; Roy, Govindan, & Muralidharan, 2018; Telles, Singh, Yadav, & Balkrishna, 2012; Varambally et al., 2012), while other study settings included educational institutions, community, geriatric centres, a park, and a corporate organization (Deb et al., 2016; Ghosh & Datta, 2012; Ghrouz et al., 2019; Godse, Shejwal, & Godse, 2015; Hallam, Bilsborough, & de Courten, 2018; Mukherjee et al., 2017; Nayak, Mohapatra, & Panda, 2019; Ray et al., 2001; Singh et al., 2018; Telles et al., 2018). The recruitment of clinical patients in many of these studies could prevent results from being generalizable to a broader population of mentally ill individuals. Seven intervention studies utilized a randomized controlled trial (RCT) design with a control group or other intervention group for comparison (Behere et al., 2011; Duraiswamy et al., 2007; Godse et al., 2015; Manjunath et al., 2013; Ramanathan et al., 2017; Ray et al., 2001; Varambally et al., 2012). Use of RCTs for comparison among groups was a more effective way to assess outcomes and odds ratios than allowing participants to choose a group. Studies that used waitlist control groups allowed for a more robust method of comparing outcomes via clinical scores.
There were no longitudinal studies found comparing physical activity for mental disorders. Studies reporting short-term results show differences between groups attributed to the intervention but do not have the capacity to assess the lasting effect of a programme after its completion. Convenience sampling was the most common sampling strategy, as most participants were patients from the hospitals where studies took place or students recruited from institutions.
Instruments used to measure physical activity and mental health/illness
Studies used Diagnostic and Statistical Manual of Mental Disorders (DSM) and International Classification of Diseases (ICD) to diagnose mental illnesses. Self-rated, teacher-rated and clinician-rated questionnaires were used for assessment. Among all tools used, the Positive and Negative Syndrome Scale (PANSS) was mostly commonly administered (Behere et al., 2011; Duraiswamy et al., 2007; Manjunath et al., 2013; Varambally et al., 2012). Majority of studies used more than one tool for assessment, where studies on schizophrenia used PANSS along with Simpson Angus Scale (SAS) or Social and Occupational Functioning Scale (SOFS); studies on depression or anxiety frequently used Hamilton Depression Rating Scale (HDRS) or State Trait Anxiety Inventory (STAI) with Warwick-Edinburgh Mental Well-Being Scale (WEMWBS) (Behere et al., 2011; Duraiswamy et al., 2007; Manjunath et al., 2013; Roy et al., 2018; Telles et al., 2018; Varambally et al., 2012). All tools used in the studies were validated and appropriate for use among Indian patients. No study created their own questionnaires or tools, thereby assuring more reliable and clinically valid results.
There was no standard measurement of physical activity via assessment tools which could have resulted in variations in reporting prevalence. A few studies used validated measure like the Physical Activity Scale for Individuals With Physical Disabilities (PASIPD), the World Health Organization (WHO) Disability Assessment Schedule 2.0 (WHODAS 2.0), and the International Physical Activity Questionnaire–Short Form (IPAQ) (Ganesh & Mishra, 2016; Ghosh & Datta, 2012; Ghrouz et al., 2019; Mukherjee et al., 2017). The remaining studies measured prevalence by designing their own questionnaires asking participants whether they were active or not (Deb et al., 2016; Ghosh & Datta, 2012; Nayak et al., 2019; Singh et al., 2018). Medical data were not collected except in one study which recorded body mass index (BMI) of the participants and determined cut-off values for obesity according to WHO guidelines (Misra et al., 2009; Singh et al., 2018). Using unstandardized tools and questionnaires could have neglected reporting on the nature of the physical activity as well as its intensity and duration. Studies that asked closed yes or no questions may have received subjective and inaccurate responses when no criteria for physical activity were implied.
Epidemiology
The association between mental illness and physical activity has been studied in the seven cross-sectional studies included in this review. Among them mental retardation, depression, anxiety, sleep quality, cognitive disorders and quality of life were studied along with the level of physical activity or inactivity reported by participants (Deb et al., 2016; Ganesh & Mishra, 2016; Ghosh & Datta, 2012; Ghrouz et al., 2019; Mukherjee et al., 2017; Nayak et al., 2019; Singh et al., 2018). No investigation into prevalence of physical activity and severe mental disorders was made by any study. This limits epidemiological investigations on prevalence of mental disorders and physical activity in India.
The prevalence of common mental disorders in the study samples was high as was their assessed level of inactivity. Prevalence of depression and anxiety were commonly assessed, ranging between 30%–57.3% and 18%–46.7%, respectively (Deb et al., 2016; Ghrouz et al., 2019; Nayak et al., 2019). The prevalence of physical activity among the studies varied, from 40% to 59% of participants having low physical activity. The reviewed studies report higher prevalence than studies from low- and middle-income countries where prevalence of depression and low physical activity were 6.6% and 16.8%, respectively (Stubbs et al., 2016). Most reviewed studies reported an association between low or no physical activity and the presence of mental illness. Other variables like sleep quality and psychological well-being were also found with prevalence of mental illness and physical activity (Ganesh & Mishra, 2016; Ghrouz et al., 2019). These results correspond with that of studies conducted worldwide where prevalence of low physical activity was significantly higher among those with depression compared with those without (26.0% vs. 15.8%, p < .0001) and significantly higher among those with anxiety compared with those without (22.9% vs. 16.6% (p < .001) (Stubbs et al., 2017; Stubbs et al., 2016). These findings imply that interventions of physical activity may have some impact on improving mental health.
Intervention studies
Intervention programmes for depression and anxiety
Yoga was also used as an intervention for assessing changes in neurosis in six studies (Godse et al., 2015; Krishnamurthy & Telles, 2007; Ramanathan et al., 2017; Ray et al., 2001; Telles et al., 2018, 2012). Clinical variables like depression, anxiety, somatization of stress, quality of life, sleep quality and self-esteem were studied. All yoga programmes followed similar schedules including asanas, breathing techniques and relaxation albeit from various types and teachings of yoga like Hatha yoga, Patanjali yoga, Bhakti yoga as well as Suryanamaskar, yoga theory and a protocol developed by Centre for Yoga Therapy, Education, and Research (CYTER) (Godse et al., 2015; Ramanathan et al., 2017; Telles et al., 2012). The duration of these programmes ranged from 1 week to 10 months, while programmes had participants practice yoga for as short as 20 minutes to as long as 5 hours. There was no uniformity in the structure, length or type of yoga among any of the programmes. Comparison of these studies’ respective programmes is based on reported outcomes of statistical significance among participants. Although the intensity of various types of yoga programmes differs, they all incorporated elements of relaxation, breathing techniques and meditation in their practice. Inclusion of such techniques could have influenced outcomes of these programmes. Similar incidences have been reported in studies which attribute meditation and relaxation to reducing stress as well as symptoms of anxiety and depression (Ospina et al., 2007; Ramanathan et al., 2017; Shannahoff-Khalsa, 2004; Srivastava, Talukdar, & Lahan, 2011). Yoga breathing or pranayamas was found by one meta-analysis to be one of the most effective techniques for reducing symptoms of anxiety and post-traumatic stress disorder (Cabral, Meyer, & Ames, 2011).
Yoga brought about a statistically significant improvement in scores, thus indicating decreased levels of anxiety and depression, two clinical variables common to all six studies. A reduction in feelings of sleepiness and stress dispositions was found in one study that practised Suryanamaskar, while other studies found significantly reduced somatization of stress and improved self-rated quality of sleep, significant improvement in self-esteem scores and improved total sense of mental well-being. Similar reductions in clinical scores and improvement have been found in other studies which also highlight that yoga can be an inexpensive and effective add-on intervention (Cabral et al., 2011). All studies promoted yoga for neurosis and hypothesized that its benefits in reducing clinical scores could be due to its effect on reducing stress, which is known to exacerbate health problems. Yoga has a calming effect on stress responses in the body, potentially reducing levels of anxiety and depression (Ramanathan et al., 2017). Numerous studies have reported yoga’s beneficial effect of stress reduction among healthy adults (Chong, Tsunaka, Tsang, Chan, & Cheung, 2011). All studies reported that participants experienced increased physical relaxation, mental peace, strength and awareness as well as lower stress dispositions. Studies’ control groups experienced no change on any clinical scale and thus no measured improvement was found (Godse et al., 2015; Krishnamurthy & Telles, 2007; Ramanathan et al., 2017; Ray et al., 2001; Telles et al., 2018, 2012). Improvement in the yoga groups of these studies promotes its use as a treatment for neurotic disorders like anxiety and depression. Further assessments need to be made on other neuroses in order to bring to light the extent of yoga’s benefit for mental disorders.
Two studies used exercise as an intervention for mental health disorders. Roy et al. (2018) utilized a RCT to designate patients to either intervention or control group and conversely Hallam et al. (2018) did not use a comparison group. The lack of randomization and control group could have produced subjective results among the employee participants recruited for the study (Hallam et al., 2018). Furthermore, the narrow representation of participants in these studies makes results appear less generalizable as study participants were from either a hospital or corporate office.
There was no common exercise programme followed by the studies as each utilized participants with varying abilities and settings. Interventions ranged in duration from 10 days to 100 days and involved either an exercise programme with walking or jogging for a minimum of 10,000 steps per day as proposed by Hallam et al. (2018) or an add-on video assisted aerobic exercise programme with warm-ups, low intensity aerobic exercises and cool-down for 20 minutes a day designed by Roy et al. (2018). Short-term programmes may have insufficient amount of time to report clinical changes; however, both studies found significant improvements.
Major findings from the two reviewed studies state that exercise as an intervention can significantly reduce stress, depression and anxiety (Hallam et al., 2018; Roy et al., 2018). Roy et al. (2018) found no significant reduction in somatic symptoms as well as no improvement in the control group. The significant changes reported by these studies stand out where other studies and reviews globally reported that exercise programmes brought about only moderate or little change in measured outcomes (Pearsall, Smith, Pelosi, & Geddes, 2014). These findings could imply that exercise programmes of this calibre have more of an impact on Indian participants than those in other countries. Overall, these studies are consistent with literature found globally on the use of exercise for reducing symptom scores in patients with depression and anxiety (Callaghan, 2004; Rimer et al., 2012). Only a small number of studies conducted in India reported an association between exercise and mental disorders like anxiety and depression. These report the beneficial use of exercise for improvement of clinical scores. However, in order to derive a conclusion more research is required from India.
Intervention programmes for psychosis
Four studies have assessed the effect of physical activity on symptoms of psychosis, using a sample of patients with schizophrenia. Researchers had assessed patients’ clinical state prior to the study to determine their ability to take part and give consent. All studies’ participants were either inpatients or outpatients and were monitored throughout or by caregivers at home recording progress in a log book.
All studies compared yoga and exercise; however, only two studies used waitlist control groups receiving no add-on treatment for comparison along with yoga and exercise groups (Behere et al., 2011; Varambally et al., 2012). All studies were RCTs and single blinded to evaluators; no studies were double-blinded. The utilization of RCT for intervention and waitlist control groups allowed for a systematic comparison of the effectiveness of each group and their improvement on clinical scales. Stabilization of medication for all patients recruited in these studies facilitated a more ethical and reliable assessment. Three out of four study samples were on antipsychotic medication for several months without any changes in medication dosage for a period of at least 4 weeks prior to the intervention and during the study period in order to assess results attributed to the programme and not due to effects of medication (Behere et al., 2011; Duraiswamy et al., 2007; Varambally et al., 2012).
All yoga programmes followed similar schedules adapted from the integrated yoga treatment developed by Swami Vivekananda Yoga Anusandhana Samsthana (SVYASA) (R. Nagarathna & H. R. Nagendra, 2004). The use of a single SVYASA programme for yoga among all studies on patients with schizophrenia allowed a more systematic method of assessing and reviewing reported outcomes. Yoga sessions lasted around an hour and were held five times a week. All studies’ programmes consisted of (a) Sithilikarana Vyayama, (b) asanas, (c) breathing practice and (d) relaxation techniques. Practice of Vyayama, asanas and breathing techniques were in equal measure (R. Nagarathna & H. R. Nagendra, 2004). Meditation was not included in any studies’ yoga regime. Similarly, a structured programme was followed for exercise groups. All exercise programmes were adapted from the National Fitness Corps: Handbook for Middle High and Higher Secondary Schools (Ministry of Education, Government of India, 1965). The regime included brisk walking, jogging and exercises in standing and sitting postures as well as relaxation. All sessions were around an hour and held five times a week. The yoga and exercise programmes utilized by all studies ranged in duration from 6 weeks to 4 months. All studies followed the same structured and well-established programmes, a feature which adds legitimacy and aids in comparison of results.
Minor differences were found in the method of monitoring patients participating in these programmes. The continuation of practice at home and logging participation and duration of yoga or exercise had drawbacks, where many patients either did not stick to the schedule of the programme or caregivers had not consistently logged their progress (Duraiswamy et al., 2007; Varambally et al., 2012). The studies found that allowing patients or caregivers to log progress was not a reliable method of confirming adherence to the programme (Behere et al., 2011; Duraiswamy et al., 2007; Manjunath et al., 2013; Varambally et al., 2012). Absence of a third party monitoring progress may have impacted the credibility of the results, especially those reporting significant improvements as a result of physical activity. This led to the exclusion of some participants who had not followed the programme as instructed. These dropouts ranged from 16 to 28 and were common in all studies.
Major findings of these studies show that yoga has significant benefits in reducing mean clinical scores in patients with schizophrenia. Studies that planned interventions longer than 2 weeks showed significantly lower mean scores in patients on the Clinical Global Impression Severity (CGIS), PANSS general psychopathology subscore, and HDRS than studies conducted for a period of 2 weeks or less. Manjunath et al. (2013) compared results at 2 weeks and at 6 weeks and found improvement only in the latter assessment. Benefits of both programmes have been recorded by all studies; however, significantly more patients in the yoga group had improved PANSS and socio-occupational functioning scores compared with the exercise or waitlist group (Behere et al., 2011; Duraiswamy et al., 2007; Varambally et al., 2012). In addition, yoga improved facial emotion recognition deficit, improved quality of life, and lowered scores on HDRS and CGIS (Behere et al., 2011; Duraiswamy et al., 2007; Manjunath et al., 2013). All studies highlight the advantage of yoga over exercise in reducing clinical mean scores and improving social-occupational functioning in patients with schizophrenia. The likelihood of improvement in the yoga group according to odds ratio analysis for negative symptoms was five times greater than either the exercise or waitlist groups in one study (Varambally et al., 2012). Furthermore, Behere et al. (2011) found no significant differences in mean scores in the exercise or waitlist group on any scales. These results are consistent with global studies reporting little or no effect of exercise on severe mental disorders (Pearsall et al., 2014; Vancampfort et al., 2012). Such results have been hypothesized to be due to insufficient intensity of exercise or short duration of its practice (Pearsall et al., 2014).
Improvement of negative symptoms in schizophrenia has been found in all studies after add-on yoga treatment (Behere et al., 2011; Duraiswamy et al., 2007; Manjunath et al., 2013; Varambally et al., 2012). Interestingly, Varambally et al. (2012) found no improvement in positive symptoms from any intervention group (yogasana, exercise, or waitlist) but significant reduction in negative symptoms. Existing low scores for positive symptoms on PANSS due to stabilized antipsychotic treatment could be a possible explanation for no significant change in positive symptom scores for some studies (Duraiswamy et al., 2007).
Studies’ outcomes imply that yoga could be a beneficial add-on treatment for negative symptoms in antipsychotic stabilized patients with schizophrenia (Behere et al., 2011). A small number of participants required changes in their medication dosage during the studies’ duration, suggesting that yoga could be used as an intervention by patients with schizophrenia without aggravating psychotic experiences (Duraiswamy et al., 2007; Manjunath et al., 2013). Yoga programmes implemented breathing exercises like diaphragmatic breathing during various postures and an attentive component practised through meditation and relaxation. These could have an added benefit over physical movement alone. Such features of yoga are even attributed to improving social functioning (Bangalore & Varambally, 2012; Varambally et al., 2012). These studies emphasize that implementation of yoga for functional non-organic psychosis is an effective and practical approach.
Limitations of these studies involved implementation of brief yet intensive intervention designs, single-blind methodology, small sample sizes, drop-outs due to lack of interest or travel difficulties, and inconsistently kept logs by patients or caretakers (Behere et al., 2011; Duraiswamy et al., 2007; Manjunath et al., 2013; Varambally et al., 2012). Studies have found that benefits of yoga therapy are not long term after intervention is ceased and continuous treatment would be required to maintain the effects (Duraiswamy et al., 2007). In addition, patients were not deterred from participating in moderate exercise or games conducted in hospital wards and this could have affected the progress of the groups (Manjunath et al., 2013). Normal routines that involve physical activity of a nature different than that of yoga or exercise could have affected results. Since these studies could not monitor or record possible physical exertion that could be classified as physical activity, the possibility of such an influence cannot be ignored. Finally, no studies reported the effect of yoga on drug-induced extrapyramidal side effects (Behere et al., 2011; Duraiswamy et al., 2007; Manjunath et al., 2013; Varambally et al., 2012). Since antipsychotic side effects are difficult to control, this would be a significant finding if studied among Indian participants.
Future directions
In general, this review found that a majority of studies had incorporated short-term interventions of either yoga or exercise. Thus, the lasting effect of such programmes has not been studied and may not be determined until long-term follow-up is recorded. Patients reporting their participation in the programme at home could have resulted in unreliable accounts of adherence; thus, studies should find a method of overcoming this drawback by monitoring progress over a longer period of time or finding alternative methods to track progress. The lack of research from India on exercise for clinical populations may have resulted in a biased review when compared with the substantial amount of literature available on yoga programmes. In future, long-term interventions could assess the lasting effect of physical activity for mental illnesses and report whether yoga or exercise are producing significant results. Robust study methodologies to control for confounding variables may find clinically valid results. Homogeneous programmes for physical activity can improve comparisons across study populations and groups. Future studies should also find what mechanisms of exercise or yoga are significantly improving mean scores for mental illnesses. Finally, the ambiguity surrounding what constitutes physical activity could be resolved by clearly defining its threshold and classifying regular activities according to their intensity. Doing so would support research involving physical activity in the Indian context.
Conclusion
The existing literature from India has shown promising results towards the impact of physical activity in mental health disorders. However, more research is needed in the assessment and intervention of physical activity suitable to the Indian context. This review found that prevalence of mental illness coupled with physical inactivity was high among cross-sectional studies’ participants. Interventions of yoga are effective in reducing mean scores for both severe and common mental disorders. In studies using patients with schizophrenia, yoga had a more significant impact than exercise or no intervention. More studies on the effect of exercise are required to support the premise that physical activity of any kind has a positive impact on mental health.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.