
Abstract
Background:
Health literacy (HL) is considered a key concept to positively address relevant decisions concerning physical and mental health. According to an integrated model of a European Consortium, the process to access, understand, appraise and apply health information is at the centre of practising HL.
Aim:
In this study, we examine HL in a population with an early onset of a mental disorder (MD).
Methods:
Results are based on a cross-sectional survey among people with MD (n = 310) who sought help at an early detection centre for MD in Cologne, Dresden or Munich. Help-seekers filled out the European Health Literacy Survey questionnaire (HLS-EU-Q) on perception-based HL, socio-demographic data and general health status. Psychopathology was assessed separately by trained specialists. Data are compared with a representative sample of the German population.
Results:
Overall, HL was lower in a sample with MD compared with the general population. Disease-specific limitations were present in accessing, appraising and applying health information, whereas understanding was perceived fairly easy. Statistical analysis of limited HL revealed correlations with the diagnosis of affective disorders and anxiety disorders, an increase of depressive symptoms as well as the presence of more than one MD. In line with these findings, low levels of HL were associated with a worse general health status.
Conclusion:
In a population with MD, accessing, appraising and applying health information seemed to be particularly challenging. Therefore, educational programmes that mainly focus on increasing knowledge might not be sufficient for improving the HL in people with MD. Further research should concentrate on context-specific HL to foster behavioural change and improve overall health.
Introduction
Mental Disorders (MDs) belong to the most common chronic conditions of Western societies. An estimated 28% of the adult population in Germany is currently affected or has been affected by at least one MD within the past 12 months (Jacobi et al., 2014, 2015). In Germany alone, the economic burden related to MDs amounted to more than 44 billion euros in 2015, which accounts for 13.1%, of all disease costs (Statistisches Bundesamt, 2017a).
Mental and physical health are closely linked: somatic and mental comorbidities are highly prevalent in individuals with MD and rates of mortality are several times higher compared with the general population (Laursen, Trine, & Gasse, 2011; Piatt, Munetz, & Ritter, 2010). MD often goes along with a decline in cognition and motivation, which can challenge the competencies to make beneficial health decisions (Kemp, Fisher, Law, Battersby, & Isaac, 2014). Studies show that only about 14% to 28% of people affected by MD seek professional advice from a doctor (Kim, Cho, Park, & Park, 2015; Oliver, Pearson, Coe, & Gunnell, 2005). Young people are disproportionately affected by mental illness (Kessler et al., 2007). At the same time, they are the most likely of any age group to delay or fail to seek help (Burgess et al., 2009).
Health literacy (HL) is regarded as key contributor to overcome barriers to prevention and to treatment, to make self-governed health decisions as well as to facilitate adherence to treatment, appointments and clinical advice (Woopen, 2015). In this study, we refer to an integrated definition by Sørensen et al. (2012), which emphasizes four steps of information processing: Health literacy is linked to literacy and entails people’s knowledge, motivation and competences to access, understand, appraise, and apply health information in order to make judgments and take decisions in everyday life concerning healthcare, disease prevention and health promotion to maintain or improve quality of life during the life course. (p. 3)
The central idea of HL can be depicted in an ongoing dynamic cycle of information processing, which should be understood as both disease- and context-specific (see Figure 1; Sørensen et al., 2012).
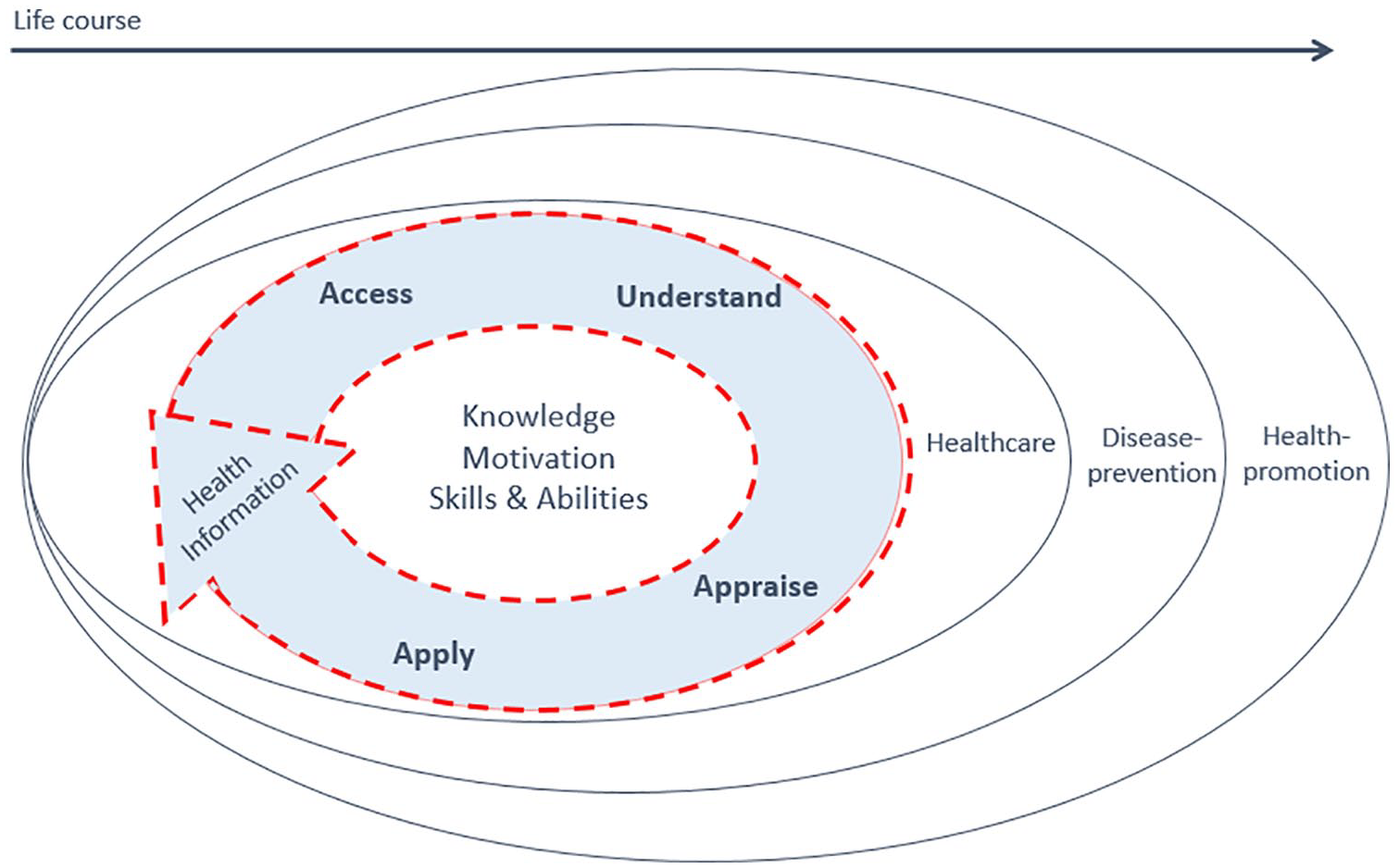
Model of health literacy.
The research from European countries (HLS-EU-Consortium, 2012), the United States (Parker, Ratzan, & Lurie, 2003) and Germany (Schaeffer, Vogt, Berens, & Hurrelmann, 2016) has shown that limited HL is related to a range of negative health outcomes and health behaviour. For instance, people with low levels of HL were less adherent to their medication, had more frequent emergency treatments and poor overall subjective health (Berkman et al., 2011; HLS-EU-Consortium, 2012; Schaeffer et al., 2016). Conversely, people with sufficient HL are more likely to navigate the various health care structures for needed services, such as receiving preventive health services and managing illness (Berkman et al., 2011).
Several studies examined the causal pathways between mental health problems and barriers as well as facilitators to mental health help seeking. One of its most important barriers was a limited mental health literacy (MHL; Bonabi et al., 2016; Gulliver, Griffiths, & Christensen, 2010). MHL is defined as the ‘knowledge and beliefs about mental disorders which aid their recognition, management or prevention’ (Jorm et al., 1997). It is closely linked to the notion of HL, although the two concepts differ in their tradition of operationalization. Thereby, MHL focusses mainly on knowledge about MD and public attitudes towards people with MD (Jorm et al., 1997) rather than on literacy-related challenges in the context of health. Thus, it is related to research on stigma towards psychiatric disorders, their early recognition and adequate treatment seeking – particularly well examined in the general population.
Less research has been conducted, however, on HL and the individually perceived difficulties in the differentiated processing steps of accessing, understanding, appraising and applying relevant health information in people suffering from MD. Overall, the available evidence indicates that the presence of psychiatric diagnoses is associated with low literacy and numeracy skills, stating that cognitive or functional impairments may affect health-related literacy of psychiatric patients (Collins, Crowley, Karlawish, & Casarett, 2004; Krishan, von Esenwein, & Druss, 2012; Lincoln et al., 2006).
Aims and scope
The study pursues the aim to present empirical evidence on HL in people with MD and to identify disease-specific difficulties in dealing with health-relevant information.
This article reports empirical results of a Health Literacy Survey (HLS) in a sample with MD (hereafter referred to as HLS-MD) within the following scope:
HL and its differentiated processing steps (access, understand, appraise, apply) and associations with socio-demographic data and psychopathological characteristics.
Comparison of HLS-MD with data of a representative sample of the German population (Health literacy Survey Germany; HLS-GER).
Methods
Data analysis is part of a cross-sectional survey among people with MD (n = 310). The study was conducted in an explorative and comparative design. The study protocol was published at the German Clinical Trials Register (No. DRKS00006260, registered on 22 December 2014).
A representative German population study on HL (HLS-GER) was considered for the comparison. The survey was conducted from 2009 to 2012 in form of computer-assisted, personal face-to-face interviews for the assessment of self-perceived challenges in dealing with health information. The study was representative with regard to age, gender and federal state (Schaeffer et al., 2016).
For better comparability of the results, we compared our sample (15–41 years) with the respective age groups (15–29 years and 30–45 years/n = 893) of the total population-based sample (N = 2,000).
Data collection
Recruitment took place at three early detection centres for psychiatric diseases in three German cities: Cologne (50.7%), Munich (38.7%) and Dresden (10.6%). Participants contacted one of the three centres over a period of 36 months. Inclusion criteria comprised a minimum age of 15 years, proficiency in German language and the capacity to give informed consent. After obtaining written informed consent, the participants filled in the questionnaire on HL independently. Psychopathology was assessed and reported separately by trained specialists of the early detection centres.
Measurements
HL was assessed by administering the German version of the HLS-EU-Q47, a questionnaire corresponding to the integrated model conducted by the European Consortium (Sørensen et al., 2012; see Figure 1). Since its development, the HLS-EU-Q has been frequently used and validated in diverse research projects all over the world (Duong et al., 2017; Huang et al., 2017; Jordan & Hoebel, 2015; Schaeffer et al., 2016; Toçi, Burazeri, Sørensen, Kamberi, & Brand, 2015). In 47 items, respondents are asked to rate the manageability of certain health-related tasks according to their perceived difficulty. Therefore, respondents have to state if they find this task ‘very easy’, ‘easy’, ‘difficult’ or ‘very difficult’ (coded from 1 to 4). (Sub-)Indices for HL were calculated in accordance with the recommendation of the European Health Literacy Survey (HLS-EU; HLS-EU-Consortium, 2012). We calculated the general HL index, which includes all 47 items, as well as sub-indices reflecting the four processing steps of HL. To simplify calculations, comparisons and interpretation between the individual indices (general HL, access, understand, appraise, apply) and the sample of HLS-GER (Schaeffer et al., 2016), they were transformed into a common metric. Mean values of each sub-index were standardized between 0 and 50 (higher values indicating higher HL) using the following formula:
Thresholds were set accordingly to HLS-GER to compare levels of HL, divided in excellent (>42–50), sufficient (>33–42), problematic (>25–33) and inadequate (0–25).
Index scores were only calculated if respondents answered at least 80% of the respective items. Socio-demographic characteristics included age, gender, migration background and educational degree. Migration background was defined as other than German nationality and/or at least one parent was born abroad.
General health status, including prevalence of chronic diseases (diseases which lasted 6 months or longer) and overall subjective health (five different categories ranging from very good to very bad), was assessed by self-report.
Diagnostic interviews were undertaken by trained specialists in the early detection centres to confirm a diagnosis according to International Statistical Classification of Diseases and Related Health Problems, 10th Revision, German Modification (ICD-10-GM).
Depressive symptomatology was recorded by the latest German version of Beck Depression Inventory (BDI-II; Hautzinger, Keller, & Kühner, 2006). The BDI is one of the widely used and validated screening instrument for measuring the severity of depressive symptoms worldwide (Beck, Steer, & Garbin, 1988; Bennett et al., 1997; Chorwe-Sungani & Chipps, 2017; Kühner, Bürger, Keller, & Hautzinger, 2007). In four self-statements, respondents are asked to rate the subjective severity of the respective symptom, for example, hopelessness or sadness. Every self-statement was assigned to a scale value (0–3) ranging in intensity. The addition of each scale value results in a total sum score reaching from 0 to 63, which were translated in four categories applying standardized thresholds for ‘No depression or remitted’ (0–13), ‘mild depression’ (14–19), ‘moderate depression’ (20–28) and ‘severe depression’ (29–63) (Kühner et al., 2007).
Statistical analysis
The statistical analysis contains two approaches. Mean comparison of the general HL index and indices of the respective processing step (scores ranging from 0 to 50) were calculated to demonstrate associations with personal variables on socio-demographic data, psychopathological characteristics and general health. The t tests and analyses of variance (ANOVAs) were performed to detect significant differences in mean values. With regard to the MD diagnosis, t tests were conducted for the three main diagnosis groups according to ICD-10.
In a further analysis step, differentiation was considered in terms of HL levels, which is revealed in the distribution of the four categories of excellent, sufficient, problematic and inadequate HL.
For comparability with data from the representative German sample (HLS-GER), both approaches served to detect differences. Because of the young average age in our sample, we compared the results with the corresponding age groups of HLS-GER (15–29 years and 30–45 years). For the analysis of general HL and the steps of information processing (access, understand, appraise, apply), the total number and means were summarized. The standard deviation (SD) was pooled according to the following calculation
Sample size differs between analyses due to different amounts of missing values among the items, which were accepted to avoid a loss of power. A two-sided p < .05 was considered significant. The p value adjustment was not conducted; therefore, the results are of explorative nature. IBM SPSS-23 was used throughout.
Results
General description of the sample
In total, 310 help-seeking individuals participated in the study, thereof 39.6% females and 60.4% males (Table 1). Ages ranged from 16 to 41 with an average age of 24.92 (SD = 5.4).
Characteristics of study participants.
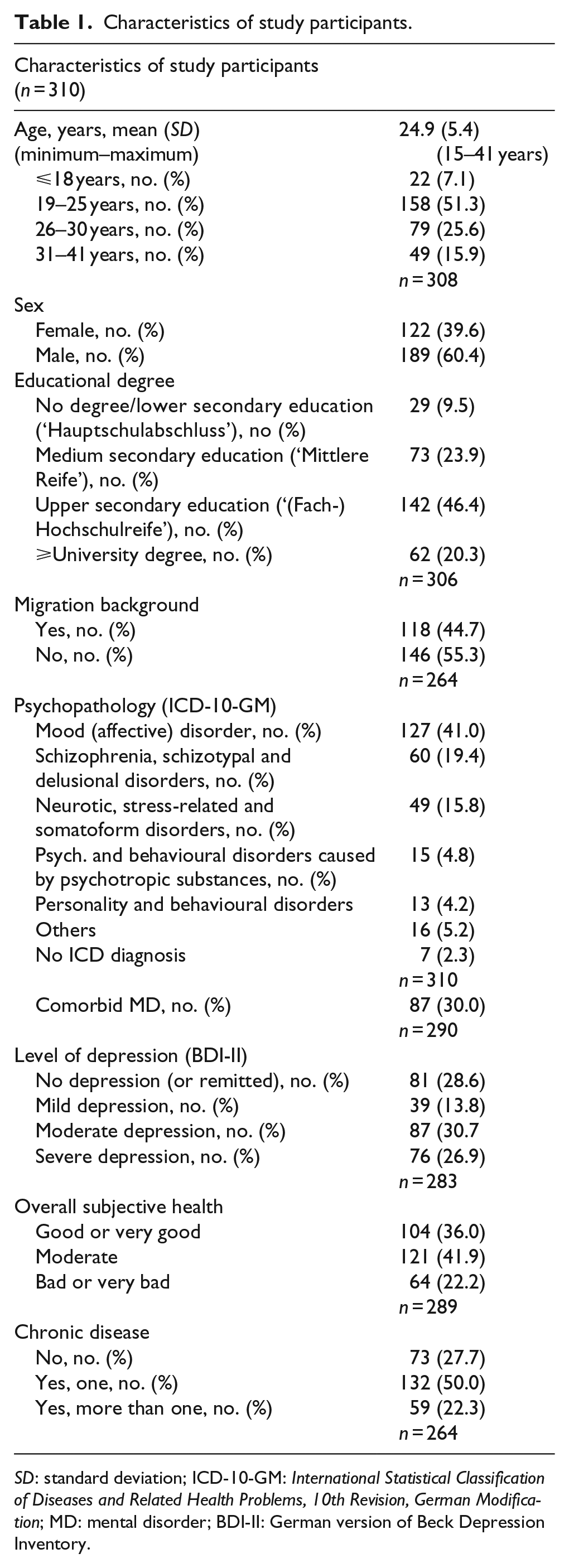
SD: standard deviation; ICD-10-GM: International Statistical Classification of Diseases and Related Health Problems, 10th Revision, German Modification; MD: mental disorder; BDI-II: German version of Beck Depression Inventory.
The study population was highly educated: up to 70% had completed upper secondary education or higher. It can be expected that a fair number of respondents was still undergoing education or training, yet attaining a higher level of education and 44.2% reported having a migration background.
The most common ICD-10 diagnosis groups were mood (affective) disorders (41.0%), followed by schizophrenia, schizotypal and delusional disorders (19.4%) and neurotic, stress-related and somatoform disorders (15.8%). In seven individuals (2.3%), no psychopathological abnormality was found according to ICD criteria. Further analysis concentrates on those with an ICD diagnosis.
In total, 30% of the participants were diagnosed with one or more comorbid MD. According to the BDI-II, 71.4% of the population showed a certain level of depressive symptoms, ranging from mild to severe symptomatology.
Self-reported chronic diseases were stated high, with 72.3% reporting to suffer from one or more diseases lasting more than 6 months and 22.2% of the people with MD rated their general subjective health as bad or very bad.
Associations of HL and personal variables
The following results show statistical correlations between HL and variables within the two domains of socio-demographic characteristics and psychopathology. Table 1 presents the results for the comparison of mean values of general HL and the respective information processing step.
Socio-demographic characteristics
Associations within socio-demographic characteristics indicated that men had higher self-assessed HL than women (p < .05). Results showed significant differences for the general HL index as well as for the processing steps access and appraise. Neither migration background nor age nor the level of education was found to have a notable effect on HL.
Psychopathology
Mean comparison of HL scores showed significant associations of HL and the prevalence of mood (affective) disorder (p < .05) and neurotic, stress-related and somatoform disorders (hereafter also referred to as anxiety disorders) (p < .05). Mood disorders were associated with limitations in general HL scores and in the processing steps of understanding and applying health information. The prevalence of anxiety disorders was significantly associated with limited HL scores in accessing health information. The diagnosis category of schizophrenia was not significantly associated with limited HL scores.
Further, statistical analysis suggested a negative association between level of depressive symptoms and HL: means of HL significantly decreased from no depression to mild, over moderate to severe depressive symptoms (p = .001). This finding became particularly noticeable for general HL and the processing step appraise.
Those with more than one MD on average had lower HL than respondents with a mental health condition limited to one diagnosis (p < .01).
Health status
Results indicated associations of HL and self-reported general health status. A decrease in HL was reflected within the downgrading from very good/good to moderate to very bad/bad overall subjective health (p < .01). This is in line with our findings on chronic diseases; HL limitations increased with the number of chronic diseases (p < .01). Correlations of HL limitations and worse general health status became particularly evident for the processing step of applying health information.
Comparison of HL: HLS-MD versus HLS-GER
Table 2 shows the distribution of mean HL scores among HLS-MD and, in comparison, the distribution in the HLS-GER sample.
Summary statistic of mean HL scores (ranging from 0 to 50).
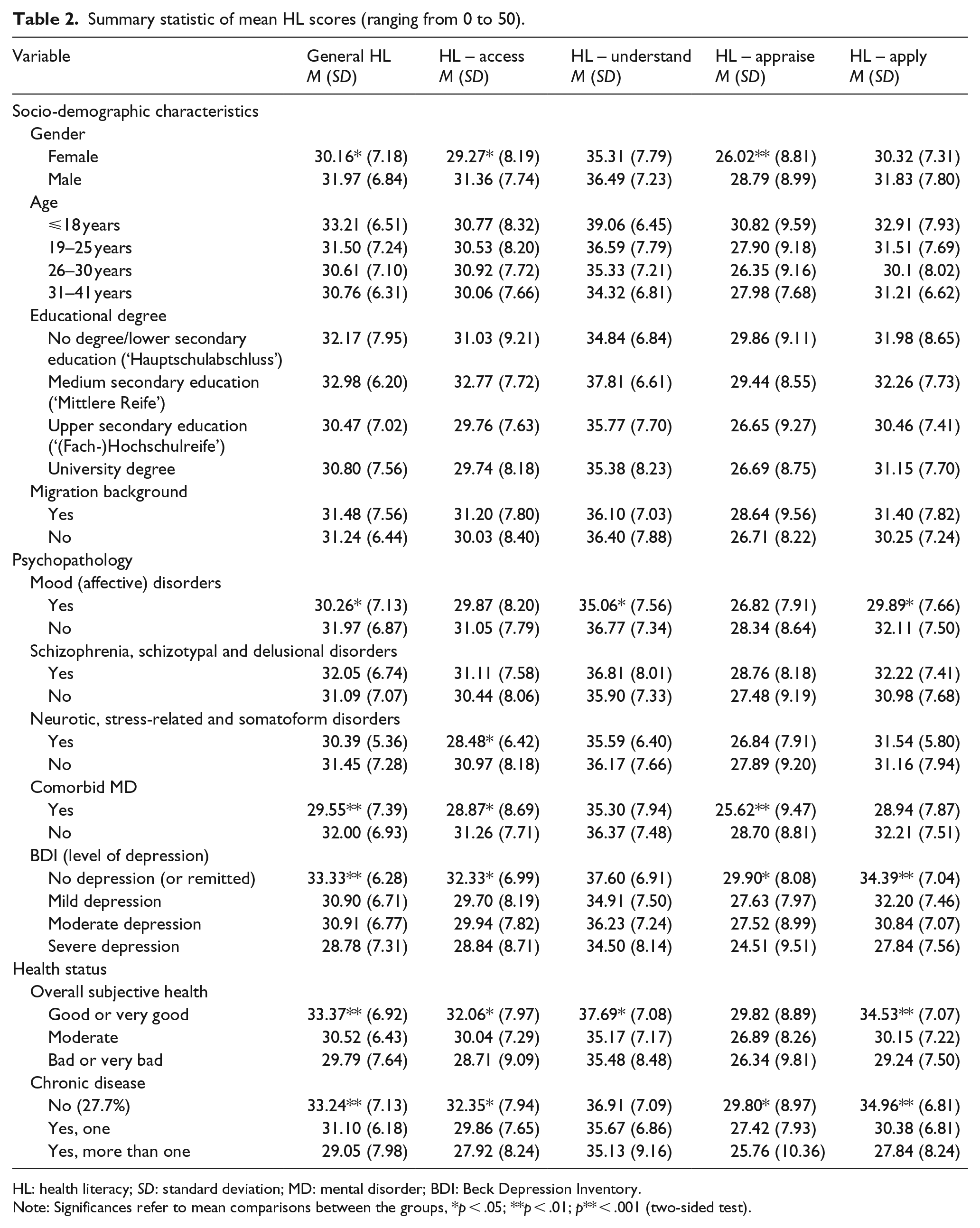
HL: health literacy; SD: standard deviation; MD: mental disorder; BDI: Beck Depression Inventory.
Note: Significances refer to mean comparisons between the groups, *p < .05; **p < .01; p** < .001 (two-sided test).
Mean comparison of HL.

HL: health literacy; SD: standard deviation; MD: mental disorder.
Note: Significances refer to mean comparisons between the groups, *p < .05; **p < .01; p** < .001 (two-sided test).
Statistical analysis revealed significant differences in the mean values of HL. By conventional criteria, this difference is considered to be extremely statistically significant for general HL as well as for the processing steps: access, appraise and apply (p < .001). Overall, HL appears to be lower in the HLS-MD compared with the HLS-GER sample, whereas understanding health information was solely perceived equally challenging with no statistically significant differences.
Further insights of peculiarities of health information processing in people with MD were elucidated in the comparison of HL levels ranging from inadequate to excellent HL.
Figures 2 and 3 show the distribution of HL in the samples of HLS-MD and HLS-GER for the general HL index as well as for the four processing steps of dealing with health information.
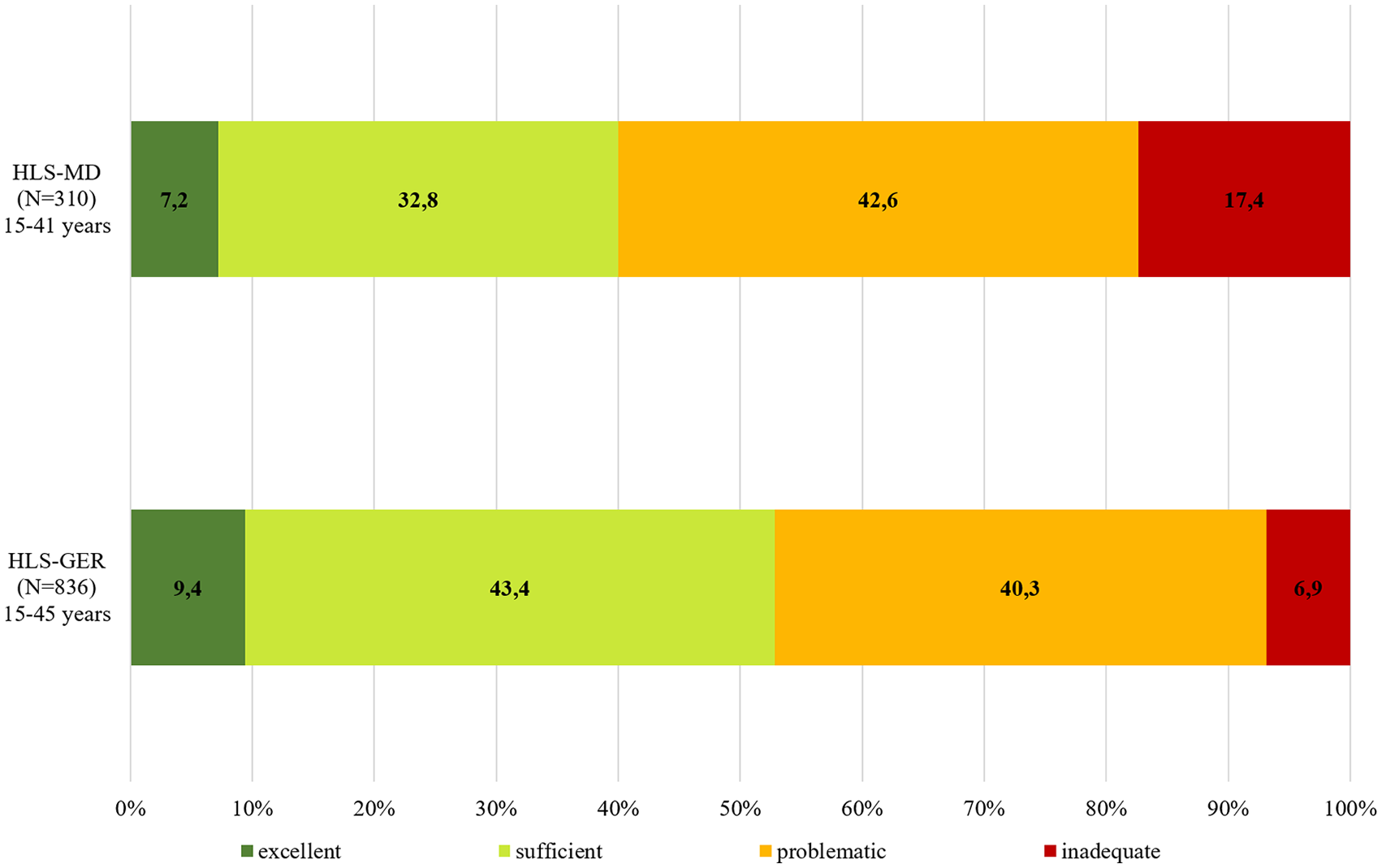
Comparison of health literacy levels: general health literacy.
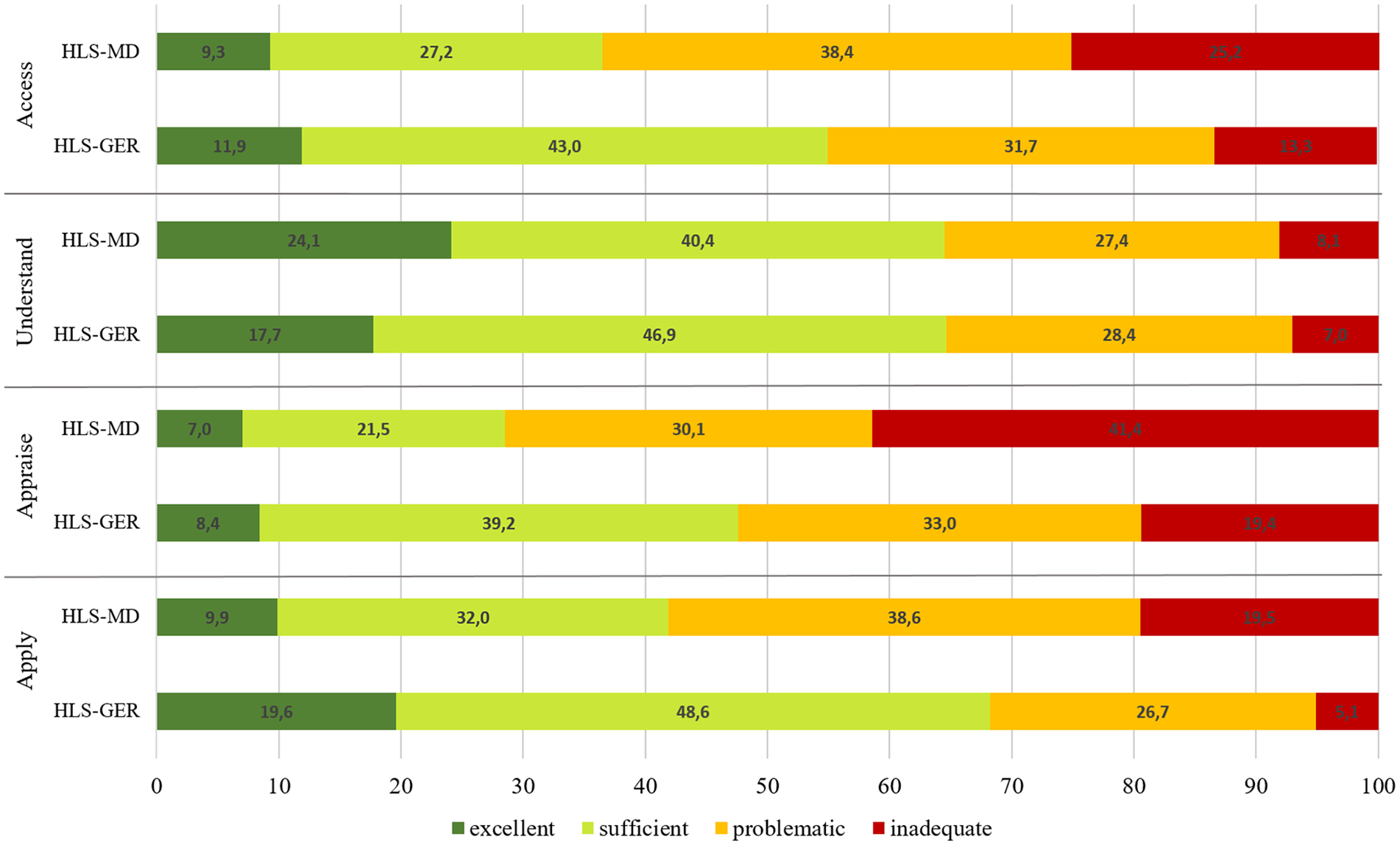
Comparison of health literacy levels: steps of information processing.
The comparison of general HL levels revealed a notably higher proportion of inadequate HL in the HLS-MD sample (17.4% vs 6.9%). In total, 60.0% of respondents had limited HL (denoted as problematic or inadequate HL), while this share was 47.2% in the respective age groups of the HLS-GER sample.
A differentiated analysis of the four processing steps allowed for a more comprehensive understanding of the perceived challenges in health information processing related to people with MD (Schaeffer et al., 2016).
While accessing health information was perceived more difficult overall, understanding them was the only processing step that was perceived equally difficult or respectively easy within the HLS-MD sample. The step of appraising health information was perceived as most difficult in the HLS-MD sample, as it was likewise in the HLS-GER sample. However, the share of people with inadequate HL was twice as high in the population with MD and in total over 70% with considerably perceived difficulties within the processing step ‘appraise’. While applying health information was experienced as easiest in the HLS-GER sample (least limited HL with a share of 31.8%; Schaeffer et al., 2016), this step was categorized almost twice as frequent as problematic or inadequate by 58.1% within the HLS-MD sample.
Discussion
The results demonstrate that the level of subjective HL is lower in people with MD than in the respective age group of the general German population. This is particularly remarkable as the HLS-MD sample is very well educated, with 66.7% of participants who completed at least upper secondary education. As a means of comparison, only 8.3% of all Germans have a university degree and 27.9% have completed upper secondary education (Statistisches Bundesamt, 2017b). Individuals with a migration background currently account for 20.6% of the total German population (Statistisches Bundesamt, 2018). In our sample, the amount of individuals with a migration background was 44.6%, which indicates an overrepresentation of this demographic factor in the HLS-MD sample.
Overall, the HLS-MD sample corresponds with those in the respective early detection centres with regard to age structure, gender and diagnosis groups. Information on education levels was not systematically assessed in the early detection centres. The low level of HL in this highly educated and young population indicates a vulnerability of people with mental health conditions with regard to perceived difficulties to manage one’s own health.
Support for our findings comes from studies on reduced problem-solving ability that may accompany the presence of MDs. It has been hypothesized that limited literacy and mental illness commonly co-occur (Currier, Sitzman, & Trenton, 2001; Kirsch, Jungeblut, Jenkins, & Kolstad, 1993). Recent studies have also suggested that cognitive and functional impairments caused by the nature of mental health problems could be contributing factors to a decreased level of HL (Krishan et al., 2012). On the contrary, Galletly, Neaves, Burton, Liu, & Denson (2012) found that HL of people with schizophrenia and depression was comparable with that of the Australian public.
Current research on HL has shown older age, low education and migration background to be risk factors for a low HL (Adams et al., 2009; HLS-EU-Consortium, 2012; Kutner, Greenberg, Jin, Paulsen, & White, 2006; Schaeffer et al., 2016; Zok, 2017). This could not be confirmed in our sample of people with MD. Interestingly, having a migration background, unlike in the total sample of the HLS-GER (Schaeffer et al., 2016), had no effect on HL in the HLS-MD sample. Support for this finding comes from another empirical study on the subjective HL of vulnerable groups in Germany, which indicated that HL in young individuals is associated with the education level of the juveniles’ parents and the familiar socioeconomic resources in general, rather than with the fact of having a migration background (Quenzel, Vogt, & Schaeffer, 2016). Low levels of education, in turn, are associated with lower educational levels of the descendants in the general German population (Federal Ministry of Education and Research, 2016). Therefore, it is reasonable to assume that our highly educated sample provided particularly good conditions for adequate HL. With regard to age structure, it has to be considered that populations of comparable studies on HL in people with MD have a broader age range, while this sample consists of mostly young people with a mean age of ~25 years. In contrast to findings from various fields in medicine, for example, in coronary heart diseases (Morrow et al., 2006) and cancer (Bauer et al., 2013), we did not find a systematic association between educational degree and level of HL. Again, this sample is rather homogeneous with regard to a high level of education.
The analyses of the HLS-MD sample showed that low HL was associated with worse general subjective health and reporting of chronic diseases. This is consistent with findings from the HLS-GER sample (Schaeffer et al., 2016) as well as other studies on subjective HL using the HLS-EU-Q (HLS-EU-Consortium, 2012; Jordan & Hoebel, 2015).
The severity of depressive symptoms was associated with HL limitations (p < .001). Depressive symptoms on various levels were a shared characteristic of the most common diagnosis groups within the sample of this study. They may serve as an explanatory variable of how MD can lead to limited HL: depressive symptoms can cause adverse effects on motivation, self-efficacy and executive functions and may therefore negatively affect a patient’s ability to engage in self-care activities (Bauer et al., 2013; Riegel et al., 2009). In addition, depressive symptoms often go along with decision-making problems, indecisiveness and a general low self-esteem (Groen & Petermann, 1998) which can be crucial for HL, especially in terms of accessing and appraising health information and translating it into healthy choices. In this respect, they might not only lead to increased barriers when dealing with health information but also to more questioning of own competences. On the contrary, a phenomenon referred to as ‘depressive realism’ (Alloy & Abramson, 1979) depicts that depressed individuals may be less biased in their ability to process information and evaluate or recall their performances than their non-depressed peers, who tend to overestimate their degree of control over a certain outcome. However, this effect appears to be rather small overall (Moore & Fresco, 2012).
The results of the comparisons of HL averages within diagnosis groups indicate that affective disorders as well as anxiety disorders tend to lead to more limitations in HL than schizophrenic disorders and other diagnosis groups. Both mentioned diagnosis groups have in common that they lead to impaired affect. Depressive and bipolar illnesses as well as anxiety disorders are associated with reduced self-esteem and self-confidence. Anxiety disorders often occur in combination with depressive symptoms within diagnosis groups (e.g. F41.2/F41.3) as well as with depression as a comorbid MD (Deutsches Institut für Medizinische Dokumentation und Information, 2017).
The analysis on the different processing steps of HL has turned out to be of explanatory power, with greatest perceived difficulties in the processing steps of accessing and especially appraising health information. Accessing health information was to be found the second most difficult processing step, which is somewhat surprising with regard to a rather young sample with potentially high affinity to the Web medium, where information is easily accessible at any time: pathways of information are getting shorter and more comfortable. According to a European survey on digital HL, 75% of the respondents felt that the Internet was a good resource for health information. (European Commission, 2014). However, while seeking information may become easier, finding health-relevant information can be very demanding. Individuals need to filter information in terms of relevance, accuracy, plausibility and practicability, which is continuously becoming more complex. With respect to the quality of online mental health information, Grohol, Slimowicz, and Granda (2014) found that the readability of mental health websites needs to be improved. In the field of mental health, it might be a particular challenge not to seek but to find suitable information within the flood of online and offline sources. This finding might point to a great awareness of challenges in getting access to appropriate information and thus adequate therapy, especially in the context of MD. The need for individual HL-adjusted health information and care is considerably reflected in the alarmingly low rate of help seeking in individuals with MD. The provision of context- and disease-adapted information represents a central task for health care organizations to respond more effectively to individual’s HL needs in future.
Appraising health information was perceived as notably more challenging for individuals with severe depressive symptomatology in comparison to non-depressed participants (mean values: 24.51 vs 29.90). In consideration of the high number of participants with depressive symptoms, the negative correlation between severity of depressive symptoms and HL can therefore partly explain the general lower levels in the processing step of appraising health information within our sample. Interestingly, the divergences between knowledge and appraisal of health-related information have been addressed in a MD-specific context: in a study on mental health-related knowledge, findings revealed that an increase in knowledge on MDs and its management is not inevitably connected with an increase in treatment-seeking behaviours of those concerned (Chamberlain, Goldney, Taylor, & Eckert, 2012). In a comparison of MHL in the Australian population over three decades, it was shown that knowledge has increased. However, there was a paucity of change in those most at risk (depressed and suicidal) in terms of their attitudes towards treatment seeking and, more importantly, their treatment-seeking behaviour (Goldney & Fisher, 2008).
This sheds light on the findings of the study by Galletly et al. (2012), who discovered no significant differences in HL between people with MDs and the general population (Galletly et al., 2012). The results are consistent with our findings that literacy skills such as understanding verbal and written health information are not per se the issue. In contrast to other studies on HL in mentally ill (Clausen, Watanabe-Galloway, Baerentzen, & Britigan, 2016), we did not find evidence for increased limitations in understanding health information. This might be partly explained by severity of the MD and level of education.
Compared with the HLS-GER sample, results suggested that MD go along with increased perceived difficulties to put health-relevant information into action (apply), which, in contrast, was perceived as easiest in the respective age group of the representative German sample. Whether health-relevant information is translated into action or not is a complex process that could not be fully grasped in this study due to the chosen methodological approach. It remains unclear whether the perceived difficulties relate to the decision-making process itself or the actual implementation of the decision.
Limitations and strengths
The research presented is explorative and builds on a limited number of cases but nevertheless provides interesting propositions for future research. Study limitations principally include the self-report nature of HL. This survey is based on a perception-based HL assessment tool to capture the complex construct of HL which is rooted in the experience of the patients. There are advantages and disadvantages of this approach discussed in the literature (Gerich & Moosbrugger, 2016; van der Heide et al., 2016). As participants already had to go through many medical examinations at their first visit to the early detection centre, there was no additional assessment of performance-based HL included. However, a low level of perception-based HL is a clear indicator for feelings of insecurity and unmet needs in making health-related decisions. It should be taken into account that participants were help-seekers who got in contact with an early detection centre for the very first time. This is important because we consider HL to be context-specific. In this vulnerable situation, feelings of doubt and general uncertainty are likely to have a significant impact on HL.
The study enables a comparison of HL in people with MD with a representative sample of the German population and thus provides information about disease-specific peculiarities in dealing with health-related information. However, comparison is somewhat limited by the divergent sample sizes (n = 310 vs n = 836) and slightly different range of ages (15–41 vs 15–45).
The HLS-MD sample was recruited from three early detection centres where young people and people with high levels of education are overrepresented. It can be expected that patients who are willing to engage with mental health services would already have a higher level of health-related competences. In addition, the questionnaire was self-administered, excluding individuals that were not able to fill in the questionnaire without external help. Therefore, a selection bias of highly educated, ‘help-seeking’ individuals should be considered when interpreting the results. Nevertheless, if we assume such biases, HL in people with MD might be even lower than the results of the analyses in this article suggest.
We defined migration background as not being of German nationality and/or having at least one parent born abroad. This is not in line with the definition of the HLS-GER, in which a migration background was defined as either oneself or at least one of the parents’ being a first generation migrant. However, despite the theoretical shortcoming, this fact did not affect our results as all of the participants with foreign nationality had at least one parent who migrated to Germany indicating a comparable group of persons for our analysis.
The study’s strengths lie in the contribution to a better understanding of HL in people with MD, including detailed insights on information processing. To the knowledge of the authors, no studies have been published on the HL assessment in consideration of the four information processing steps in this population.
Conclusion/outlook
The level of HL in young people with MD is considerably lower compared with the respective age group of the general German public and it is associated with worse overall health status, severity of depressive symptomatology and higher burden of disease. Limitations in practising HL became particularly clear in the processing steps of accessing, appraising and applying health information.
The demonstrated peculiarities of HL in the HLS-MD sample point to a need for quick responses on the health care system’s level. Especially, political decision-makers should interpret our results as a call for action, as HL is a relational construct, which is determined by individual abilities and resources as well as situational, environmental and societal conditions (Dodson, Good, & Osborne, 2015). With regard to the young age of the HLS-MD sample, it seems particularly important to point out that interventions should start at the earliest possible stage to promote health and HL effectively in young individuals at risk for MD.
Psycho-educational interventions for individuals with MD that serve the goals of treatment and rehabilitation have been successfully implemented in practice. The aim of psycho-education is to enable psychiatric patients to cope with their illness more effectively by increasing knowledge of and insights into their illness and its treatment (Pekkala & Merinder, 2002). Thus, it takes up essential elements of the concept of HL. However, against the background of the present results, educational programmes might not be sufficient for improving the HL of people with MD, since understanding health information seems not to be the issue per se. Thus, further interventions should concentrate more on the competence to access valid and relevant information, to appraise health information on the horizon of personal values and living concepts and to put this information into deliberate action (apply).
Previous research and intervention approaches focus strongly on the transfer of knowledge and the understanding of health-related information. Further research should concentrate on the connection between potentially limiting aspects such as motivation or self-efficacy and the differentiated processing steps of information processing.
Improving the individual HL at an early age has a great potential to enhance protective factors for the prevention and early intervention of physical and mental health problems.
Footnotes
Acknowledgements
This study was carried out in the context of ‘SysKomp’, a collaborative project of ethics, law, health system research and psychiatry, which was dedicated to analyse societal and individual competencies to deal with innovative approaches of risk determination in medicine. The authors would like to thank Prof. Dr Stephan Ruhrmann and team, Prof. Dr Nikolaos Koutsouleris and team and Prof. Dr Andrea Pfennig and team, who assisted in data collection for the study. They also thank Julia Däumling for assistance in data preparation.
Availability of data and material
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval and consent to participate
The ethic approval for this study was issued by the respective Ethics Committee of the medical faculty of the University of Cologne, the Ludwig-Maximilians-University of Munich and the Technical University of Dresden, which is registered as Institutional Review Board (IRB) at the Office for Human Research Protections (OHRP). All participants provided written consent before participation in this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article. This study was funded by the Federal Ministry of Education and Research (BMBF), Germany.