
Abstract
Background:
It is important to identify problem areas of parents with mentally disabled children, to support them, to address their stress sources and to effectively cope with them. The aim of this study is to evaluate the effect of training given to parents with mentally disabled children on their life satisfaction, self-stigma of seeking help, depression and stress-coping styles.
Material:
Families with disabled children who continued their education at the Special Education Centers in Sivas created the sample of this pre- and post-test study (with control group). The data were collected with the Satisfaction With Life Scale (SWLS), the Beck Depression Inventory (BDI), the Self-Stigma of Seeking Psychological Help Scale (SSPHS) and the Ways of Coping Questionnaire (WCQ). The scales were re-applied to the experimental group (n = 75) after the application of scales and 5-week training. Individuals in the control group were not given any training. The Mann–Whitney U test, t test and Kruskal–Wallis variance analysis were used in the evaluation of the data.
Results:
The mean SWLS score was 19.14 ± 7.24 (min: 3; max: 31) before the training and 21.68 ± 7.39 (min: 6; max: 35) after the training. The mean BDI score was 16.92 ± 10.84 (min: 1; max: 60) before the training and 10.24 ± 7.77 (min: 0; max: 33) after the training. The mean SSPHS score was 58.18 ± 9.96 (min: 32; max: 82) before the training and 52.65 ± 14.28 (min: 28; max: 84) after the training. The mean optimistic approach score of SSPHS was 9.73 ± 2.67 (min: 2; max: 15) before the training and 10.58 ± 2.19 (min: 4; max: 15) after the training. It was determined that the difference between mean scores of the control group before and after the training was not significant (p > .05).
Conclusion:
The training has positively affected the decrease in depression and self-stigmatization, and the increase in life satisfaction and stress-coping styles after the training. It is recommended to plan research studies to identify the need for support of parents, and to structure the trainings to be given according to the results of the educational intervention researches.
Keywords
Introduction
Mental disability is a chronic health problem that leaves persistent deficiencies in the person; requires observation, control, care, treatment and rehabilitation; and also affects the life of family members in terms of economic, social, emotional, behavioral and cognitive aspects. Having a mentally disabled child in the family is a stressor that causes an emotional burden, a stressful life experience and requires continuous coping reactions to all family members (Ayyildiz et al., 2012; Gordeles-Beser & Inci, 2014; Yildirim-Dogru & Arslan, 2008). Having a mentally disabled child is a difficult life event with the need for development of existing coping skills and increased need for social support (Brei et al., 2015; Dardas & Ahmad, 2015; Gulsen & Gok-Ozer, 2009; Konukbay & Arslan, 2015; Kucuk & Kucuk-Alemdar, 2018; Singh et al., 2015). Difficulties in the increasing care needs of children with mental disabilities, difficulties in education needs, the insecurity of the future (Brei et al., 2015; Dabrowska & Pisula, 2010; Dardas & Ahmad, 2015; Gordeles-Beser & Inci, 2014; Gulsen & Gok-Ozer, 2009; Konukbay & Arslan, 2015; Kucuk & Kucuk-Alemdar, 2018; Lu et al., 2018; Singh et al., 2015) and the difference between healthy child expectation and reality increase the pain and emotional reactions of the family (Dabrowska & Pisula, 2010; Dardas & Ahmad, 2015; Gordeles-Beser & Inci, 2014; Lu et al., 2018). At the same time, while trying to cope with the problems of children with disabilities, families are trying to fulfill the other tasks expected by the society (Ozmen & Cetinkaya, 2012).
Parents have difficulty in fulfilling the necessities of daily life in the face of this difficult situation, and there may be experienced tension in their interpersonal relationships, especially in their marital and emotional relationships. Inappropriate reactions to this traumatic situation and the feeling of guilt in the family, as well as the time, money and energy requirement for the care of the child, increase the stress experienced by parents (Gordeles-Beser & Inci, 2014; Gulsen & Gok-Ozer, 2009; Kucuk & Kucuk-Alemdar, 2018; Yildirim-Dogru & Arslan, 2008). The impact of children’s disability on the family seems to be related not only to the child’s characteristics but also to the personal, social, economic, educational and social support variables of the family (Di Giulio et al., 2014). The family with disabled child experiences anger and stress in these areas, and when they cannot cope with this situation, they can go into depression after the burnout syndrome. All these psychological processes also affect the satisfaction of family members (Bilge et al., 2014). Studies have shown that parents with mentally disabled child have lower levels of life satisfaction than other parents (Ende-Ince & Guducu-Tufekci, 2015; Ginevra et al., 2018; Kucuk & Kucuk-Alemdar, 2018; Lu et al., 2015, 2018). In a study conducted to determine the difficulties and family burden of families with mentally disabled children, it is reported that families are under a great burden in terms of physical, emotional, social and economic aspects (Balci et al., 2019). Regulations on social policies such as education, care services, employment, social services and assistance and equal opportunities have been on the agenda in Turkey since 2005, yet they are not at the desired level. The main objective of social policies for the disabled is to provide care for individuals with disabilities while they are with their families. This model is suitable for Turkish family structure and culture. However, for some reasons, different service models have been introduced for disabled people who cannot be cared for in the family (Oktar & Yildiz, 2019).
Because of nuclear family, socio-cultural and social structure of Turkey and individualized life style in the last years, taking care of a child with disabilities is considered to be the responsibility of a mother (Citil & Dogan, 2019). Therefore, as mothers undertake a great deal of responsibility for child with disabilities, they are more affected by difficulties. Mothers are usually at home due to their traditional roles and are basically responsible for the child. They may also be more sensitive to their problematic children than their spouses (Ayyildiz et al., 2012). Having an unhealthy child is thought to be the mother’s failure by the environment and causes the mother to feel more guilt, unhappiness, stigmatization, low life satisfaction and stress than other family members (Bilge et al., 2014).
Studies show that because mothers undertake a great deal of the responsibility for the disabled child’s care in the family (Oktar & Yildiz, 2019), they give up the other roles and careers they have, their participation in social activities and their life satisfaction decrease, they cannot take part in work force and their stress levels increase (Dabrowska & Pisula, 2010; Hall & Graff, 2012; Karakus & Kirlioglu, 2019; Kucuk & Kucuk-Alemdar, 2018; Olsson & Hwang, 2001; Singh et al., 2015). In a study, it was found that mothers used ineffective methods to cope with stress (Ayyildiz et al., 2012; Duymaz, 2011). Individuals are constantly trying to cope with these problems in a vicious circle, but they have difficulty in dealing with stress because they do not get professional support. In addition, families can perceive the seek for professional psychological support as a threat to self-esteem. One of the reasons that prevent the participation in the psychological support process is the stigmatization concern by the society or the self-stigmatization (Gordeles-Beser & Inci, 2014; Sezer & Gulleroglu, 2016). In a study, some families stated that because a family member gave harm around himself/herself and the communication problem, they were exposed to social pressure, they could not go out to society and they were treated very insensitively by their environment, and therefore, they experienced social exclusion (Genc, 2015). Every family can be affected in a different way from having a disabled child because of the structure of the society, its subjectivity and sources of support. Planned education can help families to cope with difficulties, adapt to the difficult situation, understand their children and accept them with their disabilities. At the same time, the necessary knowledge, skills, motivation and positive emotions may stand out with education. In the studies, it was emphasized that having positive emotion/thought and increasing compliance were supportive factors in emotional coping and quality of life (Izani-Uzair et al., 2015; Trute et al., 2012).
It is important to identify problem areas of parents with mentally disabled children, to support them, to address their stress sources and to effectively cope with them. In literature, it has been shown that the training and counseling provided to families with disabled children are useful in coping with stress and improving life satisfaction, in decreasing stress level and in decreasing depression symptoms (Bilge et al., 2014; Ginevra et al., 2018; Gordeles-Beser & Inci, 2014). In a study examining the effectiveness of ‘coping with stress and increasing life satisfaction’ training given to relatives of individuals with disabilities once a week for 3 weeks and in 1-hour sessions, it was found that post-training stress levels of participants decreased and their life satisfaction increased, yet there was no significant difference between them (Bilge et al., 2014). When literature is examined, the effects of stress coping and depression life satisfaction on intervention studies have been examined, and no intervention studies related to stigmatization have been found. In our study, the effect of these variables was examined together. At the same time, it is emphasized in literature that the regulations regarding the needs of families should also be made as well as people with disabilities (Di Giulio et al., 2014; Kalayci-Kirlioglu & Karakus, 2015). In this context, the aim of this study was to evaluate the effect of training given to parents with mentally disabled children on their life satisfaction, self-stigma of seeking help and stress-coping styles.
Research hypotheses
The training given to parents with mentally disabled children in the experimental and control groups has an effect on life satisfaction.
The training given to parents with mentally disabled children in the experimental and control groups has an effect on self-stigma of seeking help.
The training given to parents with mentally disabled children in the experimental and control groups has an effect on depression.
The training given to parents with mentally disabled children in the experimental and control groups has an effect on stress-coping styles.
Method
The study was designed pretest–posttest with the randomized control group. This intervention study was supported by the Scientific Research Projects Unit of Sivas Cumhuriyet University (T-710; Project date: 14 March 2017/15 December 2018).
Social policies for the disabled in Turkey were started with the approval of Law 2022, which provided for a small monthly benefit payment for disabled poor or the elderly over the age of 65 years. In 1997, the Directorate of Disability Services was established under the Prime Ministry, and it was decided to create a law that was more medical rather than social. When the demands related to the determination of the legal rights for the disabled emerged, the social policies were formed in 2005 and the problems of the disabled were placed on a legal basis. Most of the social assistance is provided by the General Directorate of Services for Persons with Disabilities of the Ministry of Family, Labour and Social Services. The aim of the services provided by the Ministry of Education and its affiliated institutions, social solidarity foundations and local governments is to increase the welfare of the people with disabilities, their families and the society and to establish inclusive social policies in accordance with the law. The main social policies for the people with disabilities are mainly formed within the framework of financial assistance, education, home care, rehabilitation, employment and accessibility services. Financial assistance is provided as salary for disability and home care fee. The main objective of social policies for the care of the people with disabilities is to provide care for the people with disabilities while they are with their families. These services provided by the General Directorate of Services for Persons with Disabilities have been categorized as residential and periodical services provided through home care services, residential care and rehabilitation centers, life centers, guest care homes, family counseling and rehabilitation centers, support for home care services and special care services. However, many of these services have not become too widespread throughout the country. In the past, people with disabilities were described as individuals who needed help, whereas the logic of assistance has now been replaced by a right-based perspective (Oktar & Yildiz, 2019). In this respect, there are Special Education Application and Rehabilitation Centers of the Ministry of Education or there are private centers in our country. The aim of these centers is to provide basic academic education in line with the needs of individuals who cannot benefit from education provided by the government, to equip them with the knowledge and skills they will use in daily life, to provide professional skills to students who are provided basic education and to ensure that individuals with disabilities are productive with social responsibility awareness. In addition, another goal is to raise self-sufficient, productive and happy individuals who can live in harmony with the environment. The schools within the scope of the research consist of special education teachers, classroom teachers and guidance and workshop teachers. Guidance teachers prepare training programs for families with mentally disabled children on behavior and communication, school adaptation and disability rights.
Research population and sample
The parents of the mentally disabled children who attended the four special education centers in Sivas created the research population, and all parents who accepted to participate in the study between 15 April and 30 May 2017 created the research sample. The subjects who volunteered to participate in the study were divided into two groups as experimental (75 individuals) and control (50 individuals) groups according to the simple random sampling method.
Data collection tools
Personal information form
There are 16 questions in this form about socio-demographic characteristics such as age, gender, education level, place of residence, income status, family structure, degree of proximity to disabled children and the number of children.
Satisfaction With Life Scale
The scale was designed by Diener et al. to measure global cognitive judgments of satisfaction with one’s life. It is a 7-point (1: strongly disagree to 7: strongly agree) Likert-type 5-item scale. It was adapted to Turkish by Yetim (1993), and Cronbach’s alpha coefficient was found to be .86. The highest possible score from the Satisfaction With Life Scale (SWLS) is 35 and the lowest score is 5. Low scores on the scale indicate that life satisfaction is low.
Beck Depression Inventory
The Turkish validity and reliability study of the scale, which was developed by Beck et al., was performed by Hisli (1989). The scale, which includes affective, cognitive, somatic and motivational symptoms in depression, aims to objectively determine the degree of depression symptoms. The scale consists of 21 items, each of which is scored between 0 and 3. The depression score is determined by summing the scores. The highest possible score is 63, and the cut-off point is 17. It is stated that individuals having a score more than the cut-off point show depressive symptoms, and depression symptom severity increases as the score obtained from the scale increases. The Turkish version of the scale has a Cronbach’s alpha coefficient of .80.
Ways of Coping Questionnaire
The Ways of Coping Questionnaire (WCQ) developed by Folkman and Lazarus was adapted to Turkish by Sahin and Durak (1995). The scale is viewed in terms of two categories: emotion-focused coping and problem-focused coping. The scale consists of five subscales: ‘self-confident’, ‘optimistic’, ‘helpless’, ‘submissive’ and ‘seeking social support’. In this 30-item scale scored between 0 and 3, the ninth item of seeking social support is scored reverse. The total score is not calculated. In the evaluation of the scale, as scores from self-confident (a factor that emphasizes the importance of the problem and evaluate solution options; emphasizes to be planned and cautious in the solution; emphasizes active, logical and conscious efforts to change the situation), optimistic (a factor emphasizes to see the events in a tolerant and optimistic way, reflects to evaluate the problems in a more calm and realistic way) and seeking social support approaches (including two subscales of the problem and emotions of seeking social support, such as asking for help from others for solution and sharing problems with others) increase, coping with stress is effective; as scores from helpless (a factor focuses on emotions and other sources, not to solve the problem) and submissive approaches (a factor emphasizes to feel helpless in a fatalistic approach and to seek solutions in supernatural powers) increase, it shows that ineffective methods are used in coping (Sahin & Durak, 1995).
Self-Stigma of Seeking Psychological Help Scale
This 10-item scale was designed by Vogel et al. (2006). Its validity and reliability study was carried out by Sezer and Kezer (2013) in Turkey. The scale has 23 items and is a 5-point Likert-type scale with strongly disagree (1 point) and strongly agree (5 points). Items 3, 5, 8, 9, 12, 14 and 16 of the scale are scored reverse. The high score from the scale indicates that the self-stigma score is high. The Cronbach’s alpha coefficient for the whole scale is .90. The highest possible score is 115, and the lowest possible score is 23.
Application
Family members with disabled children registered to four special education centers in Sivas Center were contacted by phone and invited to the school. The subjects were divided into two groups as experimental and control groups. They were asked to write a pseudonym on the forms.
A total of 5 weeks of training was given to parents in the experimental group with an interactive learning method for 45–60 minutes once a week. Each session was carried out based on a semi-structured subject. After the training, the questionnaires were applied to the experimental group once again. In the first and fifth week, only the questionnaire forms were applied to the control group and no training was given.
Content of the training
The content of the first session of the program, which was prepared with an interactive learning method to enable the parents to know each other, cooperate and learn the purpose and rules of the group, is as follows:
General information about the research, determining the purpose of the training and meeting
Determining group rules and sharing expectations
Sharing the feelings and thoughts of group members and expressing how they feel
Application of the Personal Information Form, SWLS, Beck Depression Inventory (BDI), Self-Stigma of Seeking Psychological Help Scale (SSPHS) and WCQ
The content of the second session of the program, which was prepared to enable the members to think about their own situations, their emotions, thoughts and behaviors in these situations, is as follows:
Problems of mental disability and having mentally disabled children, sharing of adaptation to these problems
Informing about self-stigmatization, focusing on experiences of group members
The content of the third session of the program, which was prepared to be aware of the stressful situations and how they cope with them, is as follows:
Training on stress and coping styles
Teaching respiration and muscle relaxation exercises
The content of the fourth session of the program, which was prepared to make individuals think about themselves, what behaviors they use most often in the situations they encounter, and make them think about their assertive responses, is as follows:
Self-knowledge
Recognizing the characteristics of shy, aggressive and assertive behaviors, using I language and giving assertiveness training
The content of the fifth session of the program, which was prepared to share the achievements of the members from the process and determine how much they achieved their individual goals in the first session and to share their emotions and thoughts about the training, is as follows:
Reproducing learned techniques and acquired knowledge through real life events with role-playing technique
Sharing the achievements of the members from the process, determining how much they achieved their individual goals in the first session and sharing their emotions and thoughts about the training
Interviews with psychiatrists by the participants at the end of the training.
All sessions were carried out by summarizing the previous session, reviewing homework, summarizing the day, starting the lecture with warm-up exercise and getting feedback. During the training, various games were played and stories were told about the concept to be studied in accordance with the goals. Interactive training methods, role-play, thought-stopping technique, alternative explanation technique, breathing exercise and relaxation exercise were used in the sessions. At the end of this program, the participants were expected to learn positive thinking, coping with stress, problem-solving skills, communication with I language, saying no and being able to communicate effectively.
Ethical aspects
Before the research, approval was obtained from the Cumhuriyet University Non-interventional Clinical Research Ethics Committee (Decision no.: 2016-01/29), and written permission was obtained from the institutions where the study would be conducted. The study was carried out according to the principles of the Helsinki Declaration. Informed consent was obtained from the volunteers participating in the study. Individuals in the control and experimental groups were provided therapy by the psychiatrist who was one of the researchers. At the end of the study, the control group was given the training which was given to the experimental group according to their needs.
Evaluation of the data
SPSS (version 23) program was used for statistical evaluation of the data. In the analysis of data, number and percentage distribution were used to determine socio-demographic characteristics; the chi-square test was used to determine if there was a difference between experimental and control groups in terms of socio-demographic characteristics. The Mann–Whitney U test was used to compare the two groups when the parametric test assumptions were not fulfilled, and the Kruskal–Wallis test was used to compare three or more groups. The relationship between the variables was determined by the Spearman correlation analysis and the Bonferroni test was used to determine from which group the difference originated. The paired sample t test was used to compare the mean scores of the experimental group before and after the training. Statistical significance was accepted as p < .05.
Results
Socio-demographic characteristics of the participants
The mean age of the participants in the experimental group was 42.97 ± 8.04 (min: 20; max: 62), 56% of them was at the 36- to 45-year age group, 78.7% of them were female and 84% of them were primary school graduates. 73.3% of the participants lived in the city center, 74.7% of them perceived their income status as moderate and 64.0% of them lived in the nuclear family. 77.3% of the participants were mothers of disabled children and 10.7% of mothers with disabled children had two disabled children. 56.0% of participants stated that they did not have a disabled child willingly, and 53.3% stated that their child was educated in a public school (Table 1). In addition, 76% of mothers stated that they attended training on any subject related to disability.
Distribution of socio-demographic characteristics of the participants in the experimental control groups.

p > .05.
It was found that the participants in the experimental and control groups were similar in terms of their socio-demographic characteristics, and no statistically significant difference was found between the two groups as a result of the chi-square analysis (p > .05) (Table 1).
The distribution of SWLS, BDI, SSPHS and WCQ subscale mean scores of experimental and control groups before and after the training
The SWLS mean score of individuals in the experimental group before the training was 19.14 ± 7.24 (min: 3; max: 31), their BDI mean score was 16.92 ± 10.84 (min: 1; max: 60) and their SSPHS mean score was 58.18 ± 9.96 (min: 32; max: 82). From WCQ subscales, the self-confident approach mean score of individuals in the experimental group before the training was 14.20 ± 4.26 (min: 1; max: 21), optimistic approach was 9.73 ± 2.67 (min: 2; max: 15), helpless approach was 11.96 ± 4.75 (min: 0; max: 22), submissive approach was 9.49 ± 3.19 (min: 2; max: 16) and seeking social support approach was 6.82 ± 2.00 (min: 1; max: 12). The SWLS mean score of individuals in the experimental group after the training was 21.68 ± 7.39 (min: 6; max: 35), the BDI mean score was 10.24 ± 7.77 (min: 0; max: 33) and the SSPHS mean score was 52.65 ± 14.28 (min: 28; max: 84). From WCQ subscales, self-confident approach mean score of individuals in the experimental group after the training was 15.05 ± 3.14 (min: 7; max: 21), optimistic approach was 10.58 ± 2.19 (min: 4; max: 15), helpless approach was 11.40 ± 4.15 (min: 0; max: 21), submissive approach was 9.18 ± 2.98 (min: 3; max: 18) and seeking social support approach was 7.16 ± 1.80 (min: 4; max: 11). There was a statistically significant difference between the mean scores of the experimental group in terms of pre-training and post-training scores of SWLS (p = .003), BDI (p = .000), SSPHS (p = .004) and only optimistic approach of WCQ (p = .013). There was no statistically significant difference between the mean scores of the control group in terms of pre-training and post-training scores of SWLS, BDI, SSPHS and subscales of WCQ (Table 2).
SWLS, BDI, SSPHS and WCQ mean scores of experimental and control groups before and after the training.
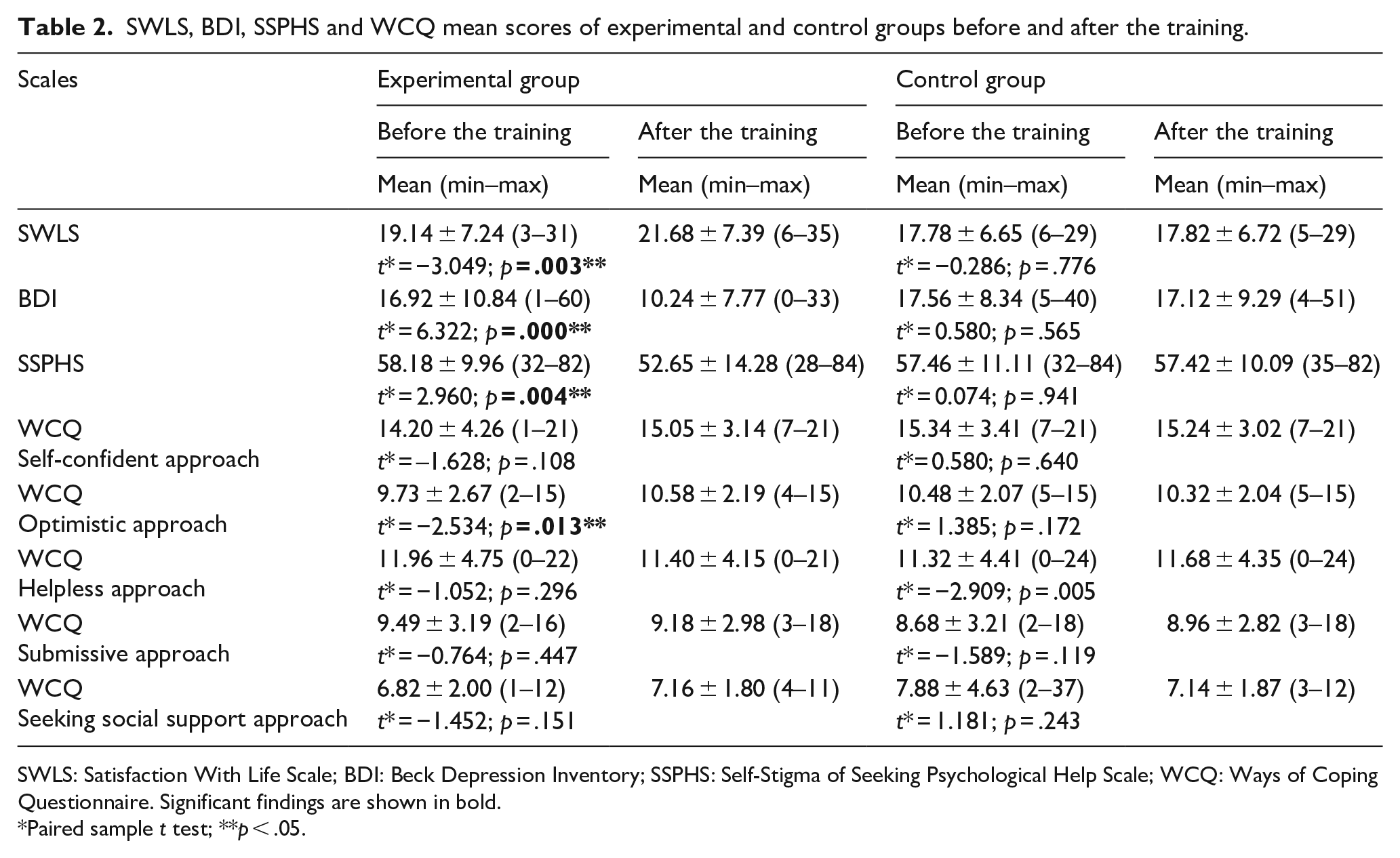
SWLS: Satisfaction With Life Scale; BDI: Beck Depression Inventory; SSPHS: Self-Stigma of Seeking Psychological Help Scale; WCQ: Ways of Coping Questionnaire. Significant findings are shown in bold.
Paired sample t test; **p < .05.
When SWLS, BDI, SSPHS and WCQ mean scores of families were compared according to experimental and control groups, a statistically significant difference was found between SWLS (p = .004), BDI (p = .001) and SSPHS (p = .031) mean scores of individuals in the experimental and control groups after the training.
Statistical evaluation of some socio-demographic characteristics of the individuals in the experimental group in terms of post-training scales and their subscale mean scores
The mean score of helpless approach subscale of WCQ was 11.4 ± 4.48 after the training in those who unwillingly had disabled child and 10.45 ± 4.61 in those who willingly had, and the difference between them was statistically significant (p = .009). The mean score of submissive approach subscale of WCQ was 10.21 ± 3.27 after the training in those who unwillingly had disabled child and 8.57 ± 2.88 in those who willingly had, and the difference between them was statistically significant (p = .019). The helpless approach mean score of those with good income status was 8.22 ± 5.91, with moderate income was 12.14 ± 4.46, with bad income was 14.30 ± 3.59, and the difference between them was significant (p = .014). The helpless approach mean score of those living in the city was 11.20 ± 4.27, those living in the county/village was 11.45 ± 4.48 and the difference between them was statistically significant (p = .029). The submissive approach mean score of those having extended family was 9.18 ± 2.71, those having nuclear family was 8.66 ± 3.11 and the difference between them was statistically significant (p = .007). The submissive approach mean score of those with good income status was 7.00 ± 3.64, with moderate income was 9.51 ± 2.98, with bad income was 11.60 ± 2.54, and the difference between them was significant (p = .008). The SSPHS mean score of those with good income status was 42.88 ± 11.10, with moderate income was 53.37 ± 14.36, with bad income was 57.40 ± 13.55, and the difference between them was significant (p = .041). The SSPHS mean score of those aged 20–25 years was 48.22 ± 10.66, aged 36–45 years was 50.23 ± 15.07, aged 46–62 years was 58.54 ± 12.54, and the difference between them was significant (p = .022). The SSPHS mean score of those having disabled child willingly was 49.09 ± 12.97, those having disabled child unwillingly was 55.45 ± 14.78 and the difference between them was p = .042. The BDI mean score of those with good income status was 5.44 ± 5.27, with moderate income was 9.94 ± 6.90, with bad income was 16.20 ± 10.88, and the difference between them was significant (p = .010). The BDI mean score of those having extended family was 9.50 ± 8.13, those having nuclear family was 11.55 ± 7.05 and the difference between them was statistically significant (p = .043). The BDI mean score of those having education in state school was 12.02 ± 8.78, those having education both in private and state schools was 8.20 ± 5.93 and the difference between them was significant (p = .030).
There was no statistically significant difference between pre-training and post-training SWLS, SSPHS, BDI and WCQ mean scores in terms of some socio-demographic characteristics of the participants in the control group.
Correlation between SWLS, BDI, SSPHS and subscales of WCQ scores of individuals in the experimental group
Before the training, a positive statistically significant relationship was found between SWLS and optimistic approach (r = .347; p = .002), between SSPHS and helpless approach (r = .466; p = .000), between SSPHS and submissive approach (r = .374; p = .001), between self-confident approach and optimistic approach (r = .748; p = .000), between self-confident approach and submissive approach (r = .303; p = .009) and between helpless approach and submissive approach (r = .471; p = .000). Before the training, a negative statistically significant relationship was found between BDI and self-confident approach (r = −.381; p = .001) and between BDI and optimistic approach (r = −.313; p = .006). After the training, a positive statistically significant relationship was found between SWLS and self-confident approach (r = .341; p = .003), between SWLS and optimistic approach (r = .407; p = .000), between BDI and helpless approach (r = .251; p = .030), between SSPHS and helpless approach (r = .461; p = .000), between SSPHS and submissive approach (r = .478; p = .000), between self-confident approach and optimistic approach (r = .745; p = .000) and between helpless approach and submissive approach (r = .755; p = .000). After the training, a negative statistically significant relationship was found between SWLS and BDI (r = −.276; p = .017), between BDI and self-confident approach (r = −.288; p = .012), between BDI and optimistic approach (r = −.239; p = .039) and between BDI and seeking social support approach (r = −.283; p = .014) (Table 3).
The relationship between SWLS, BDI, SSPHS and subscales of WCQ.
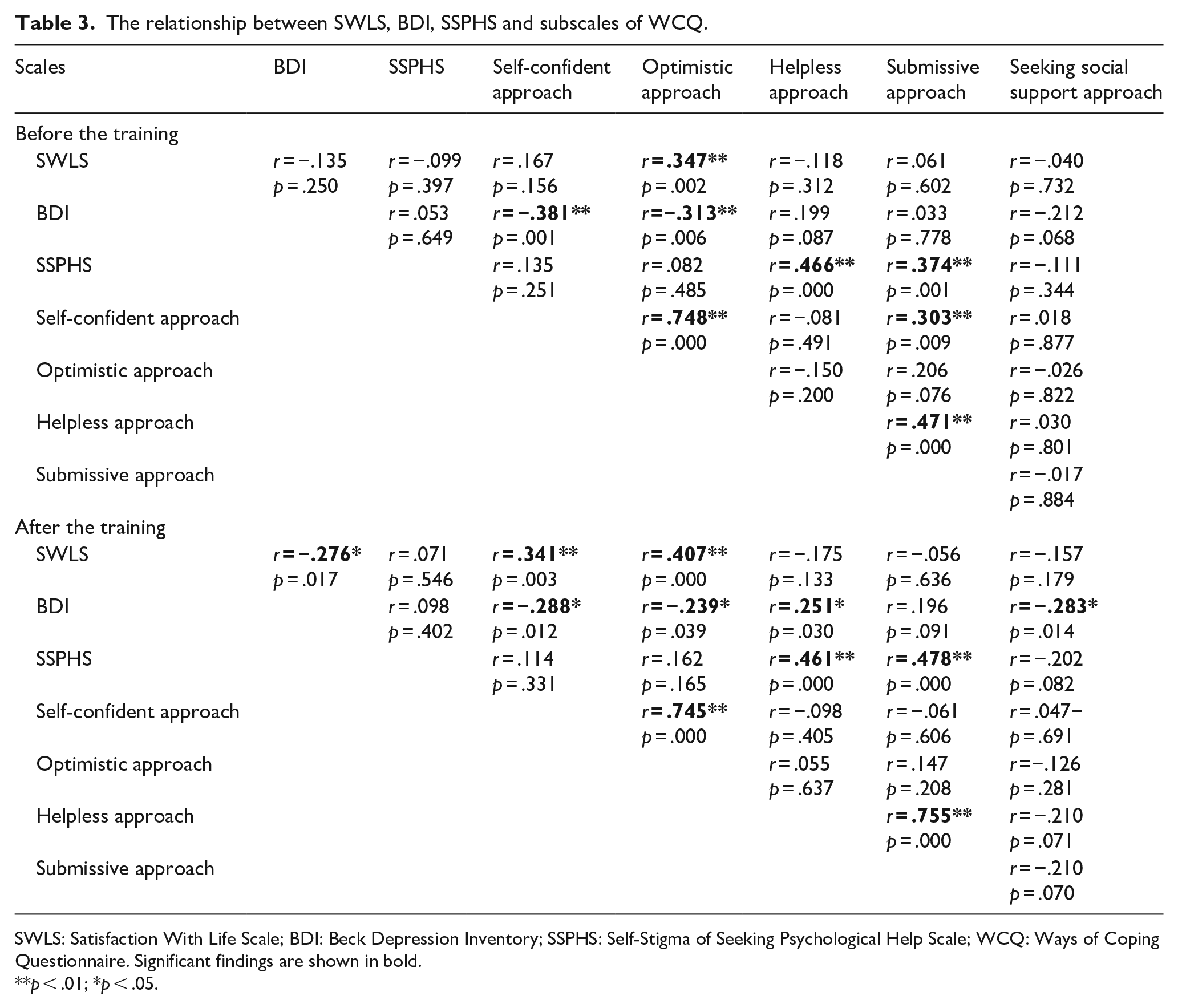
SWLS: Satisfaction With Life Scale; BDI: Beck Depression Inventory; SSPHS: Self-Stigma of Seeking Psychological Help Scale; WCQ: Ways of Coping Questionnaire. Significant findings are shown in bold.
p < .01; *p < .05.
Discussion
There was no significant difference between SWLS, BDI, SSPHS and WCQ mean scores of the control group before and after the first follow-up. However, the increase in life satisfaction of the parents in the experimental group, the decrease in depression and self-stigmatization and the increase in the optimistic approach in terms of coping with stress in post-training compared to pre-training indicate that the training is effective (p < .05). In addition, the significant difference between mean scores of SWLS, BDI, SSPHS and WCQ in post-training (p < .05) supports that the training is effective (Table 2). Creating a healthy balance by providing emotional care, understanding their emotions and thoughts about their disabled and decreasing concerns by developing a positive perspective thanks to the training can be shown among reasons of this effectiveness. In the studies, it is reported that parental education results in less stress-depression and increased life satisfaction (Ayyildiz et al., 2012; Bilge et al., 2014; Gordeles-Beser & Inci, 2014; Neece, 2014; Neff & Faso, 2014; Yildirim & Conk, 2005; Yildirim-Dogru & Arslan, 2008). The results of our study are similar to the findings of other studies, and it can be said that the training given to the relatives of the disabled has a positive effect on families. In the present study, parents’ consultation with psychiatrists might have increased the level of well-being of the participants. In a study, the findings revealed that positive emotions could balance and reduce the negative effects of chronic stress on health and relationships (Trute et al., 2012). Trainings were made by considering one or two parameters (Bilge et al., 2014). However, in our training, addressing four factors related to the problems frequently experienced by the family may have increased the effectiveness. In the education at school, it is likely that the education of the children in their care and behavior and being involved in educational activities for their own feelings and needs for the first time may have increased the effectiveness of the education.
According to the findings of our study, it is possible to state that there are no symptoms of depression in the participants, life satisfaction is not very low and parents adopt more effective methods to cope with stress but stigmatize themselves in seeking help for their problems (Table 2). It was found in a study that female caregivers tended to use problem-solving skills more (Mac Donald et al., 2006). In another study, while the families used the self-confident approach more in coping with stress, they used the optimistic approach the least (Gulsen & Gok-Ozer, 2009). In another study, unconfident approach had the highest score in coping with stress and then, self-confident approach, seeking social support approach, submissive/helpless approach and optimistic approach, respectively (Duymaz, 2011). In a study, it was determined that self-confident approach scores of mothers who were not uncomfortable with the perspective of the society to their children were high, while helpless approach scores of mothers who were uncomfortable were high (Lu et al., 2015, 2018). In literature, it was emphasized that mothers being positive were supportive in their emotional coping and that coping could increase when the family compliance increased (Trute et al., 2012).
In our study, although the stigmatization score of the participants was above the average, depression symptoms were not seen, level of satisfaction with life was not too low and so their well-being levels were not too low. This could explain the tendency of our participants to use effective methods to cope with stress. This well-being may have reduced the burden that the family felt, thus ensuring that the ineffective coping strategies in our study were not widely adopted by the participants (Yetim, 1993).
Participants educating their children at school, providing education to parents about their approaches to their children by school counseling services, mothers sparing time for themselves when their children are at school and having moderate income can be counted among the reasons of participants not too low well-being levels. At the same time, not having high-level disability in children, children being able to meet routine needs with a little support, schools gaining children control skills in their behaviors can make families feel better by reducing their burden of care responsibility. Similar to our finding, studies found that problematic behaviors of disabled child increased the stress level of the family (Dykens et al., 2014; Hall & Graff, 2012; Lu et al., 2018; Neff & Faso, 2014). In contrast to our findings, it is reported that the families of children with disabilities are depressive and psychologically distressed and they self-stigmatize themselves and prefer ineffective coping methods (Bahar et al., 2009; Charnsil & Bathia, 2010; Dabrowska & Pisula, 2010; Dave et al., 2014; Kucuk & Kucuk-Alemdar, 2018; Kvam & Loeb, 2007; Mbugua et al., 2011; Sahin & Durak, 1995; Singh et al., 2015; Yildirim & Conk, 2005).
In our study, the fact that self-stigmatization is not too high may indicate that despite the emotional pain experienced, the individual does not perceive help as a sign of weakness, failure and a bad thing, and may seek help. Research studies report that self-stigmatization may prevent individuals from seeking psychological help and a full participation in these services (Sezer & Kezer, 2013). In another study, it was found that as a result of marginalization, stigmatization and seeing children as source of shame and failure, families were exposed to social isolation (Gordeles-Beser & Inci, 2014; Sun et al., 2013). In a study, a positive high relationship was found between depressive symptoms and self-stigmatization (Sezer & Gulleroglu, 2016). As there are no depression symptoms in our study, the self-stigmatization score may be low. Similar to our finding, it is reported in literature that self-stigmatization is negatively correlated with social, emotional and physical burden. In a study conducted in China, it was found that parents of children with autism experienced higher stigmatization and self-blame (Zheng & Zheng, 2015).
That satisfaction with life is above the average in our study is similar to other studies. Moderate-level stigmatization, depression severity being very close to the cut-off point, moderate-level income and having mostly a nuclear family might have contributed to not too low satisfaction with the life score. This is because the literature reports studies showing that depression (Lu et al., 2015, 2018) and stigmatization (Acun-Kapikiran & Kapikiran, 2013) attitudes decrease the level of life satisfaction. Similarly to our findings, in another study, parents were found to be less satisfied with their life in terms of life satisfaction. In a study, parents of children with autism were found to be significantly lower in terms of social support and life satisfaction than the control group (Lu et al., 2015, 2018). Studies have shown that families with disabled children who are better able to cope with stressful care demands, who can look positively to difficulties and who have positive thinking generally have better quality of life and satisfaction (Ginevra et al., 2018; Izani-Uzair et al., 2015). When satisfaction with life is considered an important indicator of mental health (Matud et al., 2014), the absence of depression symptoms in our study may have positively affected satisfaction with the life score. As on 2005, within the scope of the principle of equality and non-discrimination, to not to perceive disability as disadvantage and instead of treating people with disabilities as if they are not disabled, practices that harmonize the existing rules, institutions and structures with differences of people with disabilities by perceiving the problems faced by the disabled as social rather than personal have started to be implemented (Oktar & Yildiz, 2019). Therefore, although this situation has delayed awareness, these developments may have affected the result positively. Facilitation of the education process of disabled people, payment of care money to caregiver family members, implementation of tax exemption for the elimination of a need for disabled people, introduction of quota system in working life, diversification of employment areas, expansion of accessibility services in local and public areas, sensitivity of the government to care services and the presence of care centers are among these developments (Genc, 2015; Oktar & Yildiz, 2019).
In this study, when some socio-demographic characteristics of individuals in the experimental group are compared with their post-training scores, those who unwillingly had disabled children, who lived in a county/village, who had a bad income level and who had extended family used ineffective methods in coping with stress more. This may be due to the limited sharing of responsibilities and experiences in the family, limited psychosocial interactions and social support. Supporting our study, it was seen that the people living in the nuclear family used the effective method more in coping with stress. This is due to the better communication of the people living in the nuclear family, the better understanding of each other and the better solutions they produce (Gulsen & Gok-Ozer, 2009). The reasons for using ineffective methods in coping with stress of those who unwillingly had disabled children can be to have less desire to cope with difficulties of disabled child, to have low likelihood of being able to get support in county and the possibility of sharing with common people, to have inadequate social facilities and transportation, not to be able to participate in decision-making mechanisms in the extended family and to be affected by domestic culture. At the same time, it is reported that almost all our participants are women and women use methods for emotions more (Sahin & Durak, 1995). Those who unwillingly had their child, who were more than 46 years of age and those who perceived their income status bad were found to stigmatize themselves more in seeking psychological help. The fact that the child was born without knowing the state of disability could have caused the result of not being ready for the family. The effect of the training given on internal control and taking responsibility of the individual about the stigmatizing situation was less than those who knew disability status of their child. Having a poor level of income may have diminished help-seeking behavior by reducing self-esteem. In addition, being in middle age and women having menopause in this age may decrease help-seeking behavior of women by increasing their physical and emotional problems. The BDI scores of those who considered the income status bad, those living in the extended family and those who went to the public school were higher. Due to the disability of their children, families spend more than other families because of various reasons, such as medical care, communication, special physical arrangements and equipment. Taking care of their children or spending more time with them affects their choice of occupation (Yildirim-Dogru & Arslan, 2008). In literature, the BDI scores of unemployed mothers were found to be higher than the scores of working mothers.
The reason for the BDI scores of unemployed mothers being higher than working mothers was due to the fact that employment increased social status, increased self-security and resulted in economic relief, and hence, women felt psychologically better (Charnsil & Bathia, 2010; Kucuk & Kucuk-Alemdar, 2018). The fact that the public school does not have support and education programs for the family’s depression may have affected the high BDI score in the family.
As a general result, the perception that they did not feel alone after the training may have positively affected the participants and the training may have been a driving force for them. The ability of the participants to overcome their problems and to produce effective solutions through training may have increased their emotional response to life (Akandere et al., 2009; Gordeles-Beser & Inci, 2014). At the same time, since the children of the participants were registered at a special education center, the school’s guidance and counseling services for child may have increased the effectiveness of training. Besides, the training that the family received from school, sharing with families having similar problems at school and the support and interactions of the family may have affected the individual positively and increased the comprehension and internalization of the given training and led them to develop an effective coping style.
When the post-training correlation between the scales was analyzed, self-confident and optimistic approach scores increased as satisfaction with life scores increased, helpless approach increased as depression scores increased, helpless and submissive approaches increased as self-stigmatization scores increased, optimistic approach increased as self-confident approach scores increased and submissive approach scores increased as helpless approach scores increased. Depression scores decreased as satisfaction with life scores increased, self-confidence, optimistic and seeking social support approach scores decreased as depression scores increased. The correlation between satisfaction with life and depression scores in our study was consistent with a study showing that there was a significant negative correlation between parental stress and satisfaction with life, which showed that high levels of parental stress were associated with low life satisfaction (Lu et al., 2015, 2018). Similarly to our study, the families of children who experienced high stress in a study were reported to have lower social support (Neece, 2014). In a study, a high positive relationship between depressive symptoms and self-stigmatization was found, but such a relationship was not found in our study (Sezer & Gulleroglu, 2016). This is because the symptom of depression in our study is below the cut-off point.
As a result, the training has positively affected the decrease in depression and self-stigmatization levels, and the increase in life satisfaction and stress-coping styles after the training. It is recommended to plan research studies to identify the need for support of parents, to structure the trainings to be given according to the results of the educational intervention research studies and to conduct qualitative studies to improve stress-coping styles for future studies.
In addition, the burden of care of the disabled child should be taken from the mother and divided into the family or to the institutions, and state care and economic support should be provided to ease the burden of the families. Efforts should be made to prevent the exclusion of disabled families and to raise public awareness. The activities carried out as a result of the social policies of the state for the disabled people should also be expanded.
Limitations
The effect of training on life satisfaction, depression, self-stigmatization and coping styles of individuals is limited with the scales applied.
Footnotes
Author’s note
This study was presented as a verbal statement in different themes at the V. International IX. National Psychiatric Nursing Congress on 20–23 November 2018 in Antalya and at the fourth International Symposium on New Trends in Social Sciences in Tallinn/Estonia on 6–7 July 2018.
Author contributions
G.Y. helped in study planning, analysis of data and writing of paper; scanned the literature; gave the approval of the final version; and helped in collection of data. She was a coauthor and helped in project writing for Scientific Research Projects Unit of Sivas Cumhuriyet. S.E.P. helped in study planning, analysis of data, scanned the literature, collection of data, training application to families and gave the approval of the final version. S.U. helped in study planning, collection of data, project writing for Scientific Research Projects Unit of Sivas Cumhuriyet, preparing the ethics committee application, scanned the literature and gave the approval of the final version. O.D.A. helped in study planning, collection of data, project writing for Scientific Research Projects Unit of Sivas Cumhuriyet and analysis of data; scanned the literature; and gave the approval of the final version. E.E.E. helped in study planning, interviewing with the individuals (psychiatrist), collection of data and gave the approval of the final version. All authors are in agreement with the content of the manuscript.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This was an intervention research (pre-test–post-test with experimental–control group) and was supported by the Scientific Research Projects Unit of Sivas Cumhuriyet University (T-710; Project date; 14 March 2017/15 December 2018).