
Abstract
Background:
Although excessive use of social networking site (SNS) is related to undesired effects on healthy individual’s psychological well-being, there is a huge gap in studies performed with individuals who suffer from various mental disorders.
Aim:
The main goal of this study is to examine the association between problematic utilization of SNSs and depressive symptoms across patients diagnosed with major depressive disorder (MDD).
Methods:
111 patients diagnosed with MDD (diagnoses confirmed via the Structured Clinical Interview for DSM-5–Clinician Version (SCID-5/CV)) and 108 healthy controls (HCs) were recruited for the study. Montgomery–Asberg Depression Rating Scale (MADRS) and Bergen Social Media Addiction Scale (BSMAS) were administered by both MDD and HC groups. Group comparisons were estimated with multivariate analysis of covariance (MANCOVA) analyses. To identify the relationship between SNS addiction and depressive symptoms, the Pearson correlations were performed, and finally, we computed the multiple linear regression analyses to determine whether SNS addiction predicts depressive symptoms.
Results:
The results revealed that MDD group is more addicted to SNS relative to HC. In addition, depressive symptoms were significantly predicted by ‘relapse’ subdimension and the overall score of SNS addiction in the MDD group.
Conclusion:
Our study illustrated the detrimental effects of excessive SNSs usage on depressive symptoms in MDD particularly for the individuals in ‘relapse’ state of SNS addiction. The mental health workers should consider the usage patterns of SNSs in patients diagnosed with MDD during their clinical observation and management.
Introduction
The social networking site (SNS) use patterns evolve and change simultaneously with the development of technology. However previous studies have acknowledged both adverse and beneficial effects of SNS use, there is still conflict regarding how this new concept is altering or improving an individual’s life (Pantic, 2014). SNSs have already penetrated the daily lives of human beings with over one billion subscribers worldwide (Obar & Wildman, 2015). Therefore, the identification of the pros and cons of SNSs is remarkable while administrating the psychological health of the public (Pantic, 2014). The researchers have defined SNS addiction or problematic use of SNS as: being extremely concerned about SNSs with a tough intrinsic motivation which turns out impairments in social functionality and psychological well-being (Andreassen, 2015). SNS addiction is not classified as a mental disorder in DSM-5; nonetheless, it was remarked as a potential mental health problem that is associated with the disturbances in interpersonal relationships, academic and occupational achievements (Andreassen & Pallesen, 2014; Kirschner & Karpinski, 2010; Kuss & Griffiths, 2011). Moreover, it was claimed that SNS addiction may aggravate depression, anxiety and insomnia. Therefore, it may decrease life satisfaction and may yield negative consequences on mental well-being (Pantic, 2014).
The depressive symptomatology is well-studied in addictions related to technology use (Baker & Algorta, 2016). The previous studies distinctly revealed the associations between depressive symptoms and SNS addiction (Andreassen et al., 2016; Błachnio et al., 2015; Davila et al., 2012; Giota & Kleftaras, 2013). These studies have reported that the vulnerable individuals who are exposed to SNS for a longer period may refrain themselves from engaging in social, occupational and daily life activities. Consequently, this withdrawal may cause depressive symptoms. However, there are contradictory findings in the growing literature which showed the beneficial effects of SNS utilization among different parts of society. In these studies, neither SNS addiction nor excessive use of it was found to be liable for depressive symptoms (Jelenchick et al., 2013); on the contrary, the researchers highlighted the advantageous arguments of SNS use in alleviating depressive symptomatology (Moreno et al., 2011).
The presence of the diversity in SNS effects on an individual’s mental well-being might have arisen from several factors. One of the factors which cause complexity in this relationship might be usage/user dependent variables (e.g. SNS type, frequency, gender, quality, personality, social factors and economic status), which can moderate or mediate the associations between SNS addiction and depressive symptoms (Błachnio et al., 2015; Davila et al., 2012; Feinstein et al., 2013; Hanprathet et al., 2015; Moberg & Anestis, 2015; Nikčević et al., 2017; Wegmann et al., 2015). Thus, these confounding factors should be controlled while assessing the interaction between depression and SNS addiction to ascertain the boundaries. The second potential reason for the inconsistent reports might be related to the sample characteristics. The vast majority of the above-cited studies recruited student populations and the diagnoses of the participants were unclear or based on their self-reports. Therefore, the diagnosis of depression among these studies might fail in representing the population who suffer from genuine depressive symptomatology. As depression and SNS addiction are affected by a pile of variables, accurate interpretation of this relationship is essential to provide mental health workers more clear sight during their observation of the potential effects of SNS on depression (Baker & Algorta, 2016). This study aims to specify the SNS addiction in major depressive disorder (MDD) particularly, and to reveal the possible effects of SNS addiction on depressive symptoms.
Methods
Participants
130 patients diagnosed with MDD and 110 healthy controls (HCs) were recruited with a convenience sampling method. 16 patients with MDD did not complete the given tests and three patients were excluded due to the withdrawal of consent. Two individuals from HC group did not want to involve in the study after completing the test battery. Therefore, this study was comprised of 111 patients diagnosed with MDD and 108 HCs. The MDD diagnosis was confirmed via the Structured Clinical Interview for DSM-5–Clinician Version (SCID-5/CV) (Elbir et al., 2019). The patients were recruited from the outpatient clinic of the Psychiatry Department at Near East University School of Medicine. The HC group consisted of Turkish citizens who were selected through Internet-based advertisement at the International University of Sarajevo, and they were also evaluated by SCID-5/CV to be included in the study. The inclusion criteria were as follows: (a) to be between 18 and 65 years of age; (b) to have at least one valid SNS account (e.g. Twitter, Facebook, Instagram, WhatsApp and Viber); and (c) MDD diagnosis (for the patient group, solely). The HCs’ exclusion criterion was the existence of any psychiatric disorder, mental retardation and cognitive incapacity to accomplish the given tasks. For the patient group, the individuals with any comorbid mental disorder rather than MDD were dropped from the study. All patients were taking at least one antidepressant treatment and the medication dosages were constant during the study. The study was approved by the Institutional Review Board of Near East University (YDU/2018/683-64) and permissions were also given by the International University of Sarajevo (IUS-FASS-05-693/19). All participants signed the written informed consent form.
Instruments
Montgomery–Asberg Depression Rating Scale
Montgomery–Asberg Depression Rating Scale (MADRS) was developed to assess an individual’s depression severity. The test involves 10 different items (i.e. apparent sadness, reported sadness, inner tension, reduced sleep, reduced appetite, concentration difficulties, lassitude, inability to feel, pessimistic thoughts and suicidal thoughts). The responses are scored according to the seven-point Likert-type scale ranging from 0 (not at all) to 6 (definitively). The higher scores indicate more severe depressive symptoms. The score ranges are interpreted as follows: 0 to 6 – normal/symptom absent; 7 to 19 – mild depression; 20 to 34 – moderate depression; and > 34 – severe depression (Montgomery & Åsberg, 1979; Svanborg & Åsberg, 2001). The Turkish reliability and validity study was conducted in 2001 (Ozer et al., 2001).
Bergen Social Media Addiction Scale
To evaluate the SNS addiction, Bergen Social Media Addiction Scale (BSMAS) was utilized. BSMAS consists of six items based on the theoretical framework of the addiction components of the biopsychosocial model (i.e. salience, tolerance, mood modification, relapse, withdrawal symptoms and conflict) (Andreassen et al., 2017; Griffiths, 2005). The responses are scored according to the five-point Likert-type scale (‘1 = never’ to ‘5 = always’). The higher scores in each subtest reflect more problematic use of SNSs. BSMAS was found to be valid and reliable among Turkish sample (Demirci, 2019).
Statistical analyses
Statistical analyses were performed with 219 participants (111 patients with MDD and 108 HCs). The normality test was checked with the Shapiro–Wilk tests. The χ2 tests and independent samples’ t-tests were performed to estimate the differences in the sociodemographic characteristics. The specific group differences in MADRS and BSMAS were calculated by the multivariate analysis of covariance (MANCOVA) analysis when significant main effects were found in sociodemographic variables. We used the Pearson correlations to disclose the associations between MADRS and BSMAS. As a final step, we executed multiple linear regression analyses (enter method used) to determine the predictive value of BSMAS on MADRS in the MDD group. We calculated Cohen’s f2 values for linear regression analyses to estimate the effect sizes. According to Cohen’s guidelines, f2 ⩾ .02, f2 ⩾ .15 and f2 ⩾ .35 represent small, medium and large effect sizes, respectively (Cohen, 1988). The analyses were computed with commercially available statistical analyses software (SPSS Statistics 22.0, IBM Corp., Armonk, NY, USA). The statistical significance (p) criterion was set to .05.
Results
Sociodemographic characteristics and differences in MADRS and BSMAS among groups
The employment status, tobacco/alcohol use patterns and current residential area of the groups did not differ significantly. The MDD group was older than HCs; in addition, socioeconomic status was better in HCs relative to MDD. Both HC and MDD groups involved more female individuals than male ones. The mean education duration was higher in HCs relative to the MDD group. Married individuals were abundant in the MDD group compared to HCs. Sociodemographic variables and descriptive statistics for each group were presented in Table 1. In the second step, an MANCOVA analysis was utilized to compare the scores of MADRS and BSMAS subtests of the groups. In this step, possible effects of confounding variables (i.e. age, gender, education status, marital status and socioeconomic status variables) were controlled. The multivariate statistical results were presented following the Bonferroni correction. There were no significant effects for age (F(7, 206) = 1.28; p = .26;
Sociodemographic characteristics of the groups.
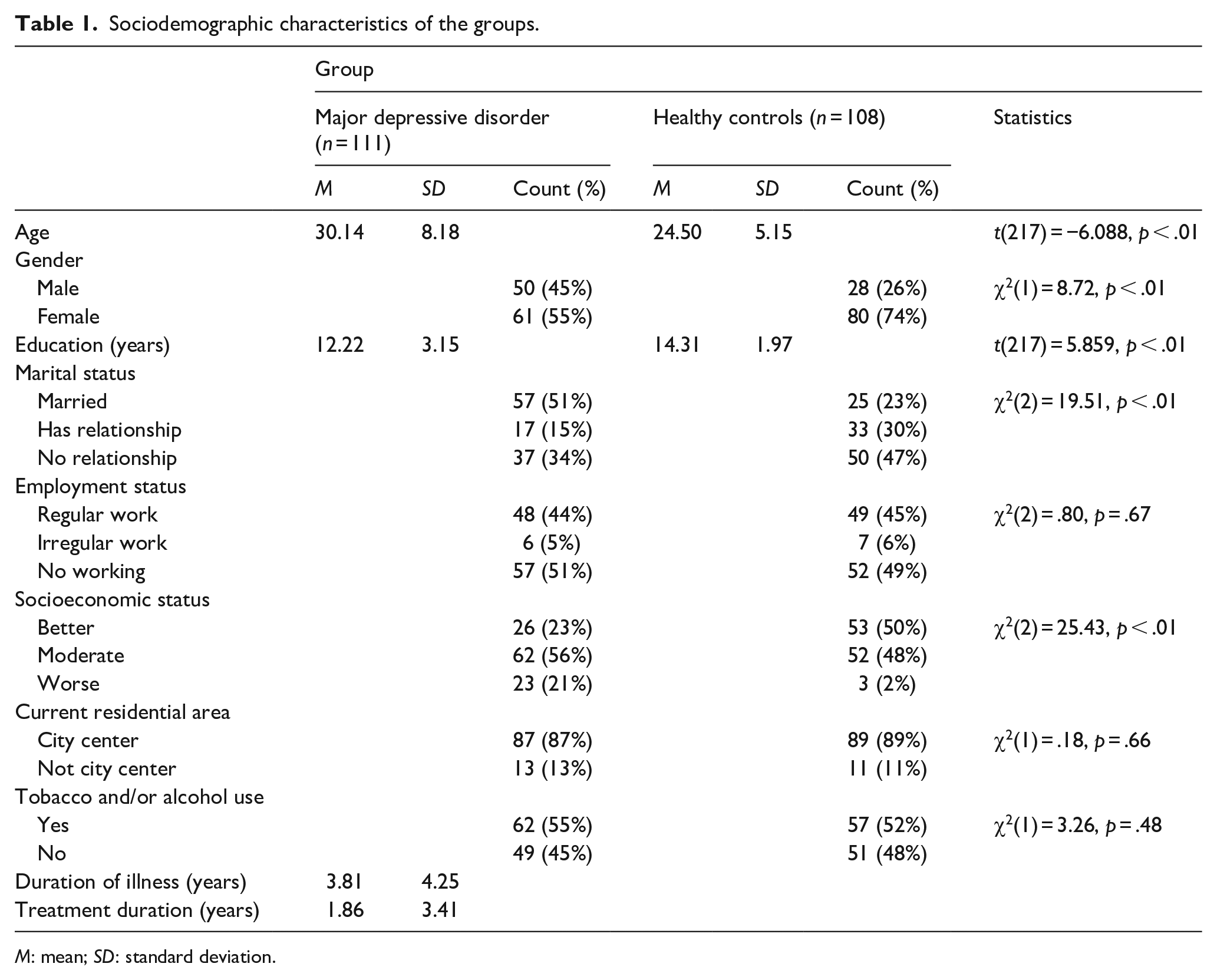
M: mean; SD: standard deviation.
Group comparison of BSMAS subtests and MADRS showing mean values and the results from an MANCOVA a analysis.
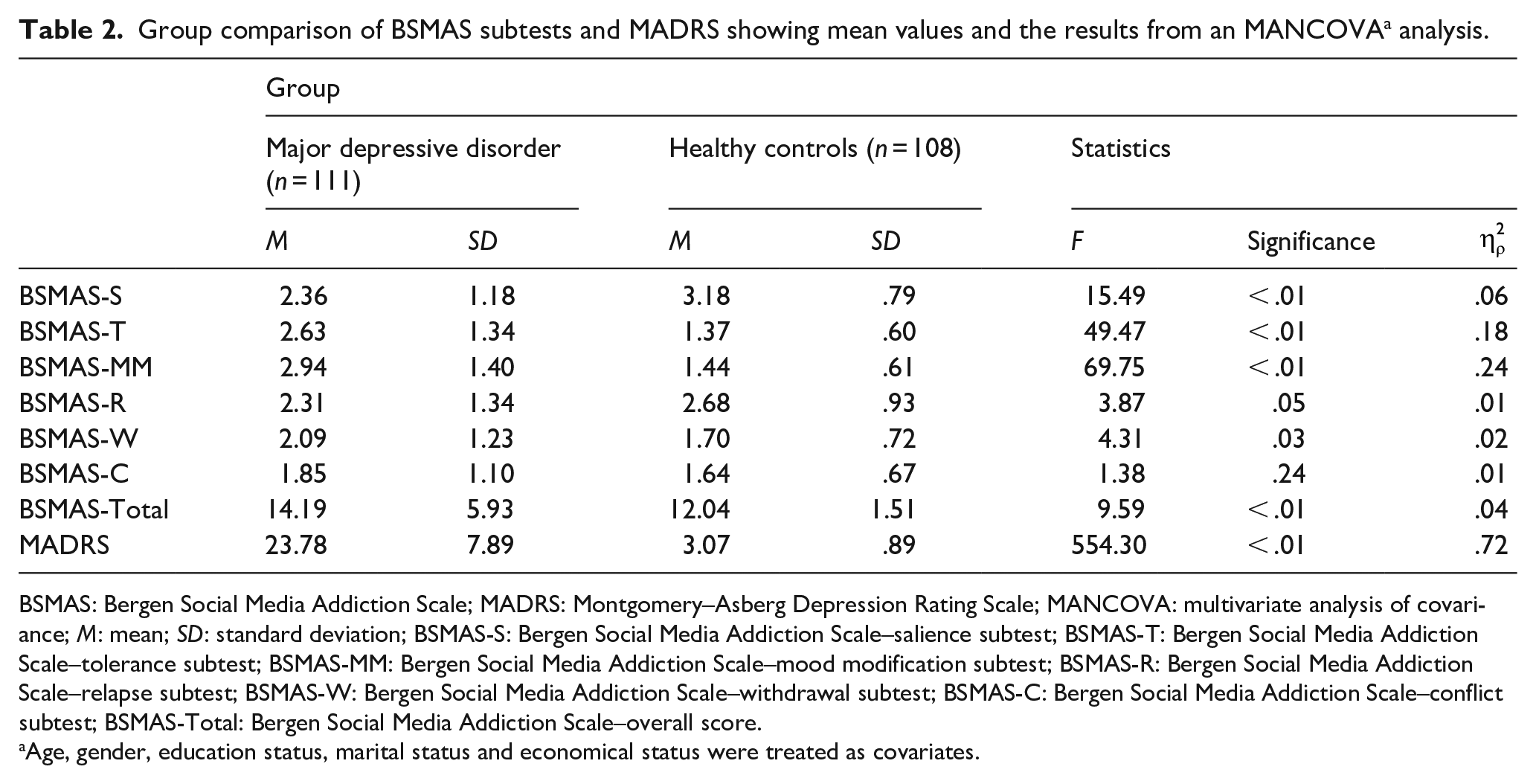
BSMAS: Bergen Social Media Addiction Scale; MADRS: Montgomery–Asberg Depression Rating Scale; MANCOVA: multivariate analysis of covariance; M: mean; SD: standard deviation; BSMAS-S: Bergen Social Media Addiction Scale–salience subtest; BSMAS-T: Bergen Social Media Addiction Scale–tolerance subtest; BSMAS-MM: Bergen Social Media Addiction Scale–mood modification subtest; BSMAS-R: Bergen Social Media Addiction Scale–relapse subtest; BSMAS-W: Bergen Social Media Addiction Scale–withdrawal subtest; BSMAS-C: Bergen Social Media Addiction Scale–conflict subtest; BSMAS-Total: Bergen Social Media Addiction Scale–overall score.
Age, gender, education status, marital status and economical status were treated as covariates.
The associations between BSMAS and MADRS in the MDD group
There was a positive correlation between MADRS and Bergen Social Media Addiction Scale–relapse subtest (BSMAS-R) (r = .33, p < .01) and Bergen Social Media Addiction Scale–overall score (BSMAS-Total) (r = .20, p = .02). However, no correlational relationships were found between MADRS and BSMAS-S (r = .16, p = .07), BSMAS-T (r = .14, p = .13), Bergen Social Media Addiction Scale–mood modification subtest (BSMAS-MM) (r = .15, p = .09), Bergen Social Media Addiction Scale–withdrawal subtest (BSMAS-W) (r = .17, p = .07) and Bergen Social Media Addiction Scale–conflict subtest (BSMAS-C) (r = −.02, p = .78). To validate the relationship between variables, BSMAS-R and BSMAS-Total were entered into the regression equation. In the MDD group, BSMAS-R (Cohen’s f2 = .49, large effect size) and BSMAS-Total (Cohen’s f2 = .25, medium effect size) were significantly predicted the MADRS. The regression results were reported in Table 3.
The multiple linear regression results between BSMAS and MADRS in major depressive disorder group.

BSMAS: Bergen Social Media Addiction Scale; MADRS: Montgomery–Asberg Depression Rating Scale; SE: standard error; BSMAS-R: Bergen Social Media Addiction Scale–relapse subtest; BSMAS-Total: Bergen Social Media Addiction Scale–overall score.
p < .05; **p < .01.
Discussion
The existing literature on SNS addiction lacks clarity regarding the diagnostic process of the samples. So far, no previous study used a structured diagnostic tool and/or clinical interview and the depressive symptoms were generally evaluated with self-report measurements. Therefore, this might limit the interpretation of the previous findings which have indicated the relationship between SNS addiction and MDD. According to our knowledge, this study is the first attempt to reveal the relationship between SNS use and depressive symptoms among individuals diagnosed with MDD. However, there was no difference found in conflict and relapse components between the groups, and the comparisons revealed that tolerance, mood modification and withdrawal aspects of SNS addiction were predominant in the patient group. On the contrary, the salience subdimension of SNS addiction was much more observed among healthy participants relative to depressive patients. When the overall SNS addiction scores were considered, the patients with MDD have shown more addictive behaviors in SNS use compared to healthy individuals. In addition, the relapse subdimension and overall score of SNS addiction were associated with depressive symptoms in MDD group.
In our study, the patients suffered from moderate depression and they exhibited higher liability in SNS addiction. In regard to subdimensions of SNS addiction, compared to healthy individuals, the patients have shown ever-increasing use of SNSs over time (tolerance), have tried to control their mood changes via excessive use of SNS (mood modification) and have exhibited undesired feelings and psychological symptoms (e.g. depression, irritability and anxiety) when SNS use is restricted (withdrawal). Several studies have explored that depressive symptoms were related to more frequent use of SNS (Jelenchick et al., 2013; Kim et al., 2006; Pantic, 2014), and our results were consistent with the previously proposed models in the development of SNS addiction. According to one of these models, the individuals suffering from depression tend to engage more in SNS in course of time (tolerance), and they can utilize SNS as a tool to escape from negative mood states (mood modification) (Caplan, 2010). When the depressed individual experiences tolerance and endeavors to modify his or her mood via SNS, he or she becomes easily agitated when the SNS use is restricted (withdrawal) (Caplan, 2010). Another model has suggested that if the depressive symptoms outweigh an individual’s life, the individual would less engage in social activities (Kupferberg et al., 2016). This may lead the patient to prefer online social communication over face-to-face interaction in real life to fulfill his or her social needs (Caplan, 2010; Satici et al., 2014). Consequently, the individual’s depression may limit the active participation in the social environment and this insufficient self-competency may result in excessive use of SNS (Turel & Serenko, 2012).
In our study, total preoccupation with SNS use (salience) was found to be lower in the MDD group. The depression refers to markedly diminished interest or pleasure in all, or almost all, activities most of the day (American Psychiatric Association, 2013); therefore, the individual shows up with decreased engagement in miscellaneous daily activities. Our study involved patients who have demonstrated moderate depressive symptoms. The individuals who exhibit this level of severity could easily withdraw themselves from daily activities. Hence, it is possible to conclude that this withdrawal might decrease the preoccupation with SNS accounts during the day. Furthermore, in this study, MDD and HC groups have demonstrated a similar pattern in regard to conflict (i.e. interpersonal problems as a result of SNS use) and relapse (i.e. recurrence of problematic SNS use after abstinence) subdimensions. It is noteworthy that healthy individuals were also found to be as vulnerable as depressive patients in terms of repetitive SNS use after discontinuation. In addition, SNS addiction may cause problems in social relationships, even the individual is healthy enough to maintain interpersonal communications.
The associations between SNS addiction and distinctive psychiatric symptoms have been examined in different psychiatric populations, such as schizophrenia (Torous & Keshavan, 2016), bipolar disorder (Rosen et al., 2013) and anxiety (Weinstein et al., 2015). Although the antecedent role of SNS addiction in MDD remains unclear (Pantic, 2014; Pantic et al., 2012; Stankovska et al., 2016), there were different approaches which state the positive (Tandoc et al., 2015) and negative (Caplan, 2010) impacts of SNS use on depression. In our study, the effect size of ‘relapse’ subdimension was large which has indicated a strong association with depressive symptoms. However, the overall score of SNS addiction has shown association with medium effect size and none of the other subdimensions of SNS addiction were related to symptom severity among patients with MDD. We acknowledged that when an individual decides to use SNSs less frequently but he or she does not manage to do so, and accordingly he or she quickly reverts to SNSs use after a period of abstinence, this may elevate the depressive symptoms. Therefore, it might be noticeable to question SNS usage pattern particularly for ‘relapse’ state of the patient during the management of the MDD. It could aid mental health workers to focus on precise behaviors of the patients during their SNS usage to maintain their psychological well-being. The lack of the associations between other subdimensions (i.e. salience, tolerance, withdrawal, conflict and mood modification) and depression might be related to the severity of SNS addiction in our sample. However, there was not any cut-off score defined for SNS addiction in BSMAS (min: 6, max: 30) (Demirci, 2019), and 19 points were recommended as a threshold for risky SNS use (Bányai et al., 2017). The MDD group scored under the risk threshold; therefore, it might cause loss of significant relationships between the variables. Indeed, the patient group scored similarly when compared with a large cross-sectional study that was consisted of 23,533 adults (Andreassen et al., 2016). Moreover, that study has also found a weak negative association between depression and SNS addiction. The individuals were not diagnosed with MDD and the symptomatology was evaluated by a self-report test which has indicated mild symptoms in the overall sample. The researchers interpreted the weakness of the association as a consequence of social withdrawal and lack of participation in all kind of SNS activities due to the negative outcomes of depression. However, one study stated the SNS use and SNS addiction as different concepts, and it emphasized that SNSs function as possible venues for individuals to explicit their existing psychopathologies. It is possible that depressive patients do not use SNSs more due to the loss of interest in participation to them, but they engage more in problematic interactions of SNS use; thus, they experience more undesired negative effects as a consequence of these interactions (Feinstein et al., 2012). In contrast to our findings, several studies have found that SNS use can mitigate depressive symptoms (Shaw & Gant, 2002; Tandoc et al., 2015). It was suggested that SNS may pose an effective role in compensation of the social deficits by increasing perceived social support; thus, it may suspend negative feelings like depression (Shaw & Gant, 2002). Furthermore, it was emphasized that the sensitivity for social rejection by peers is lower in online interactions compared to real-life encounters (Caouette & Guyer, 2016). However, these studies also did not include diagnosed patient groups.
The utilization of structured diagnostic interview and clinician-rated symptom severity measurement can be counted as strengths of this study. The lack of this methodology was cited as a major limitation in previous studies which were conducted in this field (Andreassen et al., 2016; Baker & Algorta, 2016; Bányai et al., 2017). From this point of view, our study could suggest a different perspective in estimating the effects of SNS directly on MDD. However, there were several limitations required to be addressed. The cross-sectional design may preclude conclusions in regard to causality across significant associations. Hence, the determined relationships may be present in both directions between depression and SNS addiction (Kuss et al., 2014). The relatively small sample size, the medium effect size found in the associations, the recruitment of only young adult participants and MDD group’s lower SNS addiction score limited the generalizability of the findings. Moreover, the individuals who are at different stages of the MDD and who use different types of SNSs may pose distinct relationships. Future longitudinal studies can overcome these issues.
In conclusion, our study uniquely contributed to the existing literature by revealing the association between depressive symptomatology and SNS addiction among the psychiatric sample. The findings implied that ‘relapse’ subdimension of SNS addiction might exclusively exacerbate the depressive symptoms in MDD among young adults; however, not all subdimensions of SNS addiction have contributed to the depression, and several subdimensions did not differ between patients and healthy individuals. Therefore, it is possible that SNS addiction patterns and effects on symptom severity may differ between individuals who are diagnosed with MDD and who exhibit mild depressive symptoms. Our findings could shed light on conflicting associations to better comprehend the effects of SNS addiction on MDD. With more than one billion people actively participate SNSs every day, it is prominent to evaluate whether the technology use is positively supporting public mental health or affecting it in a negative direction. Furthermore, we recommend that the mental health workers should envision certain behaviors related to SNS use to prevent the progress of depressive symptoms in risky populations.
Footnotes
Author’s note
Kuzeymen Balikçi is now affiliated with Department of Psychology, Faculty of Arts and Social Sciences, Cyprus Social Sciences University, Nicosia, Turkish Republic of Northern Cyprus.
Author contributions
O.A. and P.Ü.-A. contributed to the conceptualization of the study. K.B., F.P.Ç. and D.S.-D. contributed to the data curation of the study. O.A. contributed to formal analysis of the study. O.A. and F.P.Ç. contributed to investigation of the study. O.A. and P.Ü.-A. contributed to methodology of the study. K.B. contributed to supervision of the study. O.A. contributed to writing the original draft. P.Ü.-A contributed to writing, reviewing and editing the manuscript.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.